
Abstract
Background
Dissatisfaction with the intensive care unit may threaten medical care. Clarifying treatment preferences can be useful in these settings, where physician direction may influence decision making and therefore medical treatment. This study aimed to evaluate whether fast-track discharge from intensive care units affects the satisfaction of family members.
Methods
We used a single-center non-randomized trial, with all eligible family members involved. To evaluate family satisfaction, we used the Society of Critical Care Family Needs Assessment questionnaire (SCCMFNAQ). We hypothesized that those discharged within 24 h of intensive care unit admission and their families would have higher levels of satisfaction. Patients were scored using the therapeutic interventions scoring system (TISS) and additive EuroSCORE.
Results
Two-hundred fifty-five family members were enrolled. The mean patient age was 53 years, and 92 % were male. The median satisfaction level among family members was 17.9 (range 14–31). Patients were divided into two groups, one receiving fast-track discharge (116 patients), and one whose members stayed longer (139 patients). The overall satisfaction was affected significantly by quality of the delivered care and dissatisfaction increased by lack of comfort in hospital settings, including the waiting room. No significant differences were seen between the two groups for overall satisfaction (p = 0.546) and individual components of the questionnaire. Higher satisfaction was linked to higher levels of education among family members (p = 0.045) and information being relayed by a senior physician p = 0.03 (two-tailed test).
Conclusions
Fast-track discharge from intensive care did not influence family satisfaction as hypothesized. Satisfaction relied on family members’ level of education and the level of seniority of the physician relaying information.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
One of the primary initiatives to promote care for acutely ill patients is to create an outline of the patient’s treatment preferences [1]. This is particularly relevant in the intensive care unit (ICU) because the severity of a patient’s condition may limit his/her decision-making capacity [2]. Advanced directives are often neither implemented by physicians nor initiated by patients, leading to failure of clinical decision guidance [3]. The ability of patients and their families to understand treatment directions can be further complicated by physicians’ attitudes and practices, which are usually related to the achieved satisfaction level [4]. Numerous studies from the United States and Europe have documented the needs of family members of critically ill patients because they are frequently involved in psychological crises [5, 6]. Providing adequate care for patients and families has emerged as a priority for ICU physicians and nurses [5, 6].
The sensation of being cared for, along with a sense of security in families who are deeply involved in a life crisis, are related to psychological assurance from ICU physicians and nurses. Information that is provided by health care professionals needs to be clear and appropriate to engage family members in making decisions about patients. Some studies on family satisfaction in ICUs [5, 7] have suggested that information giving is one of the most effective means of communication. This should be considered a cornerstone in successful interventions for crises with families of ICU patients. Family satisfaction is improved by clear information, but provision of reassurance and professional closeness to the patient is as important as the need for communication [5–9].
Few studies have been carried out in the Middle East to measure satisfaction of family members of ICU patients [10, 11] and none have been carried out in Qatar. Qatar is a multinational community, with more than 50 nationalities receiving treatment at Hamad Medical Corporation. Therefore, communication between health care professionals and the patients’ families can be complicated. Arab people are highly dependent on their family members to make surrogate decisions related to treatment options. Keeping family members informed regarding the patient’s condition and talking to the family member in confidence are important [12].
Klingele et al. defined “fast-track discharge” from the ICU as discharge within 24 h of initial admission [10]. We hypothesize that fast-track discharge from the ICU has a positive effect on overall family satisfaction.
The study aimed to evaluate the satisfaction of family members of patients in a Qatari ICU, and to assess determinants of satisfaction, particularly the relationship with fast-track discharge from the ICU. We also aimed to determine if family satisfaction could be improved through an effective assessment and communication plan.
Methods
This was a prospective, single-center survey with purposive sampling of patients’ family members. The survey was conducted in a 12-bed, post-cardiac-surgery ICU of Heart Hospital, Hamad Medical Corporation. This ICU admits approximately 300 patients annually with an average daily turnover of two patients who have an average age of 40 years. Staff included six consultants and 15 specialists. We included family members who were older than 18 years, adult patients older than 16 years, and family members and patients who were available and agreed to participate in the study. We excluded families who could not be traced or refused to participate, and in cases of poor understanding of the questionnaires.
There were 321 patients whose family members were eligible, of whom 15 family members refused to participate, and a further 51 could not be traced. The remaining 255 patients were included in the study. The study was conducted from September 2012 to October 2013 after approval by the ethics committee (Hamad Medical Corporation-Institution review board: reference number 13244/13), which waived the requirement for informed consent. Questionnaires were provided to family members after the daily round, which included the list of problems and plan of management. A physician met the family members of each patient in the ICU, and asked them to complete the form.
The following information was recorded for each patient: age, sex, marital status, diagnosis, length of stay in the ICU, European System for Cardiac Operative Risk Evaluation (EuroSCORE) to assess the effect of variations in patients’ risk profiles [13], the Therapeutic Intervention Scoring System (TISS) score on the day of the interview [14], use of mechanical ventilation, number of patients in the ICU at the time of interview, and the nurse-to-patient ratio. Demographic information for each family member included the following: age, sex, nationality, relationship with the patient, occupation, level of education, commuting time to the ICU per day, and whether information had been provided by a senior or junior ICU physician. Family members were defined as all individuals (relatives or friends) who visited the patient in the ICU, regardless of their relationship to the patient [5].
Satisfactory understanding of the diagnosis was defined as having knowledge of the diagnosis before admission. Comprehension of the treatment was defined as knowledge of the most important treatments performed on admission [15]. Finally, satisfactory comprehension of prognosis was considered as knowing whether the patient was expected to survive [16].
We used the Society of Critical Care Medicine’s family needs assessment questionnaire (SCCMFNAQ), validated by Johnson et al. to assess family satisfaction [5]. This instrument consists of 14 items, each rated on a four-point self-report Likert scale, ranging from 1 (extreme satisfaction) to 4 (extreme dissatisfaction). The final satisfaction score is calculated as the sum of the scores of all 14 items. Therefore, the smallest possible score is 14, indicating total satisfaction and the highest possible score is 56, indicating extreme dissatisfaction. Because of the multicultural atmosphere, Arabic, English, Hindi, and Urdu versions of the SCCMFNAQ were made available. The questionnaire was slightly reworded based on family members’ suggestions. A physician was available in case of questions during the discussion.
Immediately after the daily visit to the ICU, a researcher approached every family representative and provided verbal information on the purpose and procedures of the study. The visitors were asked to anonymously complete the SCCMFNAQ. The questionnaire was provided to family members 2 or 3 days postoperatively. The form was recovered immediately after completion and family members were not allowed to take the questionnaires home. The effect of the information provided by nurses and paramedics was not evaluated. We compared the individual components of the SCCMFNAQ score with the mean SCCMFNAQ score (total SCCMFNAQ score divided by 14). A pilot group of 20 family members was used to test the validity and reliability of the questionnaires, and this was not included in the final sample.
The TISS is a scoring system denoting the intensity of interventions carried out on the patient. The total maximum score is 78. Interventions are allocated scores ranging from 1–4, depending on the severity. The severity of intervention is assigned to one of the four classes depending on the severity [17].
Normally distributed continuous variables are reported as mean ± SD and non-normally distributed continuous variables are shown as median and range. Categorical variables are reported as frequency and percentage. Normally and non-normally distributed continuous variables were compared using the Student’s t-test and Mann–Whitney U test, respectively. Categorical variables were compared using the chi-squared test. A two-sided p value < 0.05 was considered statistically significant. The reliability of the translated version of the SCCMFNAQ was addressed using Cronbach’s alpha coefficient. A coefficient of ≥ 0.70 suggests that the items within the scale measure the same construct, which strengthens the construct validity [18]. All statistical analyses were carried out using SPSS for Mac 22.0 (SPSS, USA).
Results
Completed questionnaires were collected from 255 family members of patients and included in this study. The patients were predominantly male. Detailed demographic and surgical characteristics are shown in Table 1. Intraoperative and ICU details, including the severity of illness scoring, are shown in Table 2. Demographic characteristics of relatives and the details of administration of SCCMFNAQ scores are shown in Table 3.
Figure 1 shows the mean satisfaction scores of SCCMFNAQ individual variables in family members. Most of the relatives expressed extreme satisfaction for most of the variables in the questionnaire. Compared with the mean SCCMFNAQ score, family members were significantly more satisfied about delivery of the best possible care, the care of the patient by hospital staff, staff courtesy, and the expectation that they would call if there was a change in the patient’s condition. However, they were significantly more dissatisfied with the explanation of the equipment used, the comfort of the waiting room, and feeling isolated while waiting (Fig. 2).

Satisfaction level of patients’ families

Individual satisfaction mean scores vs mean SCCMFNAQ score
The patients were divided into subgroups: group 1 stayed one day or less in the ICU (116 patients) and group 2 stayed longer than 1 day (139 patients). There was no significant correlation between the length of stay and family satisfaction (Table 4). There were also no significant differences in satisfaction of the individual variables of the SCCMFNAQ score between the two groups.
Further analysis showed that certain patients’ characteristics, such as prolonged ventilation, the need for further operations, being confused, renal failure, having an intra-aortic balloon pump, and infectious complications were associated with a prolonged ICU stay (Table 5). Re-admission to the ICU was the same in both groups (three times in each group) Similarly, a low baseline ejection fraction, increased bleeding and transfusion rates, a high TISS score, a high pre-operative EuroSCORE, and prolonged bypass were associated with a prolonged stay (Table 6), but none of these parameters affected the satisfaction levels (Table 7).
Discussion
To the best of our knowledge, this is the first Middle Eastern study to evaluate the effect of information provided to family members of ICU patients. The main findings of our study were that family members tended to be dissatisfied with their own comfort levels while visiting, especially the comfort of the waiting room and the fact that they felt isolated there. Satisfaction was increased by feeling that the patient was obtaining the best possible care and that hospital personnel were taking care of them, staff courtesy, the expectation that they would be called if there was a change in the patient’s condition, and comfort when they visited the patient (the first six items in the questionnaires, Fig. 2). Fast-track discharge did not affect the level of satisfaction (Table 4). Satisfaction measured by questionnaires was significantly related to the level of education and whether information was provided by a senior or junior physician.
Most previous studies on family satisfaction were multicenter or limited to medical or mixed ICUs. Our study was performed in a cardiothoracic surgical ICU setting, which makes it unique. The unpredictability of complex open heart surgery might have an effect on family satisfaction.
Satisfaction in critically ill patients is a complex emotion, and is affected by the interaction between perception and expectations [19]. Satisfying patients’ family members is also a fundamental part of the ICU physicians’ responsibilities because family members need clarification about the patient’s treatment and interventional preferences [19]. We hypothesized that fast-track discharge has a positive effect on family satisfaction which was not substantiated in our study.
Family needs have been evaluated in many studies in Western countries [15, 16, 20] and in a few studies in Arab countries [21]. The median score of the SCCMFNAQ was 17 in our study, highlighting higher satisfaction than in previous studies. We found that the satisfaction was significantly increased for questions 1, 2, 6, 10, 8, and 12. Similarly, Roberti and Fitzpatrick [22] found that the given variables significantly affected satisfaction. However, Neves et al. [23] found that communication and satisfaction with medical care positively influenced overall satisfaction.
Factors significantly affecting dissatisfaction in our study were those in questions 9, 13, and 14, which is similar to the findings of Damghi et al. [21]. Discomfort related to the waiting area was found to affect satisfaction in other studies where relatives experienced “the emotional hell of waiting” [24–26]. In our hospital, the waiting area is a long way from the cardiothoracic ICU. This area is also small and shared with those visiting the coronary care, catheterization, and high-dependency units. Because of the high number of day-case procedures, waiting is often busy during the day.
Demographic and cultural variables
Qatar’s population is multinational, and was estimated to be approximately 1.6 million in June 2010. Major ethnic groups include Arabs, those from the Indian subcontinent, and also the Philippines. Major religions include Islam, Christianity, Hinduism, and Buddhism. The majority of the Qatari population is Muslim, a tradition in which family is the basic subunit, with close relations between family members. Islamic traditions encourage supporting and visiting those who are sick. Muslims believe that critical illness and death are God’s will, and that family prayers can help overcome these life crises [21]. No single authority exists in the culture of the Indian sub-continent, and diverse opinions and actions are observed. The ideal of longevity is a motive for families to demand life-supporting measures. Many Eastern religions support reverence for the deceased and accept death as a natural event. Compassion is a biphasic act between families and patients in these cultures [27]. Cultural and religious norms suggest lower demands by families of patients in the ICU because acute illness is perceived as predestined and not the caregiver’s fault [28].
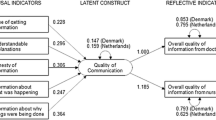
In the current study, clinical variables that significantly increased the ICU stay were the need for a further operation, renal failure, infective complications, intra-aortic balloon pump use, and the duration of mechanical ventilation (Table 5). Other factors that differed between the two groups of patients included lower ejection fraction, and higher total blood loss, transfusion of blood products, bypass time, additive EuroSCORE, and TISS in more than 1 day stay in ICU group. There was no mortality in our study patients. We hypothesized that satisfaction is affected by the length of ICU stay because of the comorbid condition of the patients. However, our results failed to substantiate this hypothesis. Our finding is in agreement with previous studies. Hunziker et al. [25] found that the length of ventilation, but not the total length of stay, affected satisfaction. Heyland et al. [29] also observed that satisfaction scores were better in patients who were ventilated for more than 48 h, the authors had further provided a conceptual framework of a patient–physician interaction (Fig. 3). Neither the length of ventilation nor the total length of stay affected satisfaction in another study [21]. Families of patients who died while in the ICU were more satisfied than the families of survivors. The centered aspect of care is highly rated, and those who die also stay longer [30]. Azoulay et al. [31] found no relation between satisfaction and severity of illness, the length of hospital stay, or mortality. Another study [32] showed that written admission and discharge criteria were associated with dissatisfaction among family members, which is not consistent with our results.

Conceptual framework of a patient–physician interaction. Adopted from Heyland et al. [29]
Participants’ characteristics
In our study, the SCCMFNAQ was nor correlated with individual variables, but increased satisfaction was significantly related to a higher level of education and information being provided by a senior physician (Table 7). Sundararajan et al. [33] reported that dissatisfaction with care is more frequently found in non-graduates. However, another study showed that better education may be related to a lower level of satisfaction [31]. Lower levels of education in family members were also associated with increased family satisfaction in other studies [23, 34]. Our finding on education level is similar to that by Verhaeghe et al. [35], who showed that a higher education level was associated with increased satisfaction in multivariate analysis.
In a multicenter study by Azoulay et al. [31], the effect of whether information was delivered by a senior or junior physician was investigated. Family members were found to prioritize receiving information from one person, regardless of whether they were senior or junior, rather than from multiple practitioners, because they found it resulted in less contradictory information. Other investigators found that family satisfaction tended to increase in those with lower education levels when information was provided by a senior physician. Developing structured communication programs by health care professionals could be an option to improve satisfaction [34].
We found that information being delivered by a senior physician significantly increased satisfaction (Table 7). This finding might be because Arabs and Asians tend to trust and respect older physicians more than younger physicians. This is consistent with a Moroccan study where families’ preferences were for a senior physician to provide information, and this tended to increase satisfaction [21]. A multicenter French study concluded that junior physicians might lack the time to effectively provide information [29]. Families want daily information on ongoing care, treatment, and interventions provided. Additionally, communication skills and awareness are required, which develop as physicians mature. Junior doctors may be perceived as less proficient. Finally, families’ perceptions might be more negative when information is provided by junior doctors [36].
Strengths and limitations
A strength of our study is that, to the best of our knowledge, this was the first study to address family satisfaction in a multicultural community, with variable languages and religions. Additionally, this was the first study to use questionnaires in four languages. In contrast to our hypothesis, we found that family satisfaction was not affected by fast-track discharge in the ICU, but rather by high quality care and improved hospital facilities. This study was limited by being performed at a single center, and restricted to a cardiothoracic ICU.
Conclusions
Fast-track discharge from ICU does not affect family satisfaction. Family satisfaction is dependent on the family member’s level of education and the seniority level of the physician providing information.
Recommendations and future directions
-
1)
Senior physicians should relay information to families to maximize satisfaction levels.
-
2)
The family member’s level of education should be considered in assessing their satisfaction.
-
3)
Improving the quality of care and the comfort of waiting areas is important.
-
4)
Hospitals should consider establishing a structured communication program for family members of ICU patients, including education of junior physicians.
-
5)
We recommend that management recognizes the importance of care environments in assessing patient and family satisfaction with services.
Abbreviations
- ACC:
-
Aortic cross clamp
- AKI:
-
Acute kidney injury
- CABG:
-
Coronary artery bypass graft
- CPB:
-
Cardiopulmonary bypass
- SCCMFNAQ:
-
Society of Critical Care Medicine Family Needs Assessment questionnaire
- TISS:
-
Therapeutic Intervention Scoring System
References
Nelson JE, Danis M. End-of-life care in the intensive care unit: Where are we now? Crit Care Med. 2001;29(2 Suppl):N2–9.
Alpert HR, Emanuel L. Comparing utilization of life-sustaining treatments with patient and public preferences. J Gen Intern Med. 1998;13:175–81.
Teno JM, Licks S, Lynn J, Wenger N, Connors Jr AF, Phillips RS, et al. Do advance directives provide instructions that direct care? SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. J Am Geriatr Soc. 1997;45:508–12.
Teno JM, Hakim RB, Knaus WA, Wenger NS, Phillips RS, Wu AW, et al. Preferences for cardiopulmonary resuscitation. J Gen Int Med. 1997;10(4):179–86.
Johnson D, Wilson M, Cavanaugh B, Bryden C, Gudmundson D, Moodley O. Measuring the ability to meet family needs in an intensive care unit. Crit Care Med. 1998;26:266–71.
Harvey M, Lent M. Volunteers in the critical care waiting room. Dimen Crit Care Nurse. 1994;13(4):201.
Foss KR, Tenholder MF. Expectations and needs of persons with family members in an ICU as opposed to a general ward. South Med J. 1993;86:380–4.
Henneman EA, McKenzie JB, Dewa CS. An evaluation for meeting the information needs of families of critically ill patients. Am J Crit Care. 1992;1:85–93.
Kiessling AH, Huneke P, Reyher C, Bingold T, Zierer A, Moritz A. Risk factor analysis for fast track protocol failure. J Cardiothorac Surg. 2013;8(1):47.
Rego Lins Fumis R, Nishimoto IN, Deheinzelin D. Measuring satisfaction in family members of critically ill cancer patients in Brazil. Intensive Care Med. 2006;32:124–8.
Lee LY, Lau YL. Immediate needs of adult family members of adult intensive care patients in Hong Kong. J Clin Nurse. 2003;12:490–500.
Aboul-Enein BH, Aboul-Enein FH. The cultural gap delivering health care services to Arab American Populations in the United States. J Cult Divers. 2010;17(1):20–3.
Nashef SA, Roques F, Michel P, Gauducheau E, Lemeshow S, Salamon R. European system for cardiac operative risk evaluation (EuroSCORE). Eur J Vasc Endovasc Surg. 1999;16(1):9–13.
Keene AR, Cullen DJ. Therapeutic Intervention Scoring System: Update 1983. Crit Care Med. 1983;11:1–3.
Azoulay E, Chevret S, Leleu G, Pochard F, Barboteu M, Adrie C, et al. Half the families of intensive care unit patients experience inadequate communication with physicians. Crit Care Med. 2000;28(8):3044–9.
Azoulay É, Sprung CL. Family-physician interactions in the intensive care unit. Crit Care Med. 2004;32(11):2323–8.
Cullen DJ, Civetta JM, Briggs BA, Ferrara LC. Therapeutic intervention scoring system: a method for quantitative comparison of patient care. Critical Care Med. 1974;2(2):57–60.
Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16:297–334.
Burns JP, Mello MM, Studdert DM, Puopolo AL, Truog RD, Brennan TA. Results of a clinical trial on care improvement for the critically ill. Crit Care Med. 2003;31(8):2107–17.
Stapleton RD, Engelberg RA, Wenrich MD, Goss CH, Curtis JR. Clinician statements and family satisfaction with family conferences in the intensive care unit*. Crit Care Med. 2006;34(6):1679–85.
Damghi N, Khoudri I, Oualili L, Abidi K, Madani N, Zeggwagh AA, et al. Measuring the satisfaction of intensive care unit patient families in Morocco: a regression tree analysis*. Crit Care Med. 2008;36(7):2084–91.
Roberti SM, Fitzpatrick JJ. Assessing family satisfaction with care of critically ill patients: a pilot study. Crit Care Nurs. 2010;30(6):18–26.
Neves FBCS, Dantas MP, Bitencourt AGV, Vieira PS, Magalhães LT, Teles JMM, et al. Análise da satisfação dos familiares em unidade de terapia intensiva; analysis of family satisfaction in intensive care unit. Rev Bras Ter Intensive. 2009;21(1):32–7.
Bournes DA, Mitchell GJ. Waiting: the experience of persons in a critical care waiting room. Res Nurs Health. 2002;25:58–67.
Hunziker S, McHugh W, Sarnoff-Lee B, Cannistraro S, Ngo L, Marcantonio E, et al. Predictors and correlates of dissatisfaction with intensive care. Crit Care Med. 2012;40(5):1554.
Desai PN. Medical ethics in India. J Med Phil. 1988;13:231–55.
Berger JT. Culture and ethnicity in clinical care. Arch Int Med. 1998;158(19):2085–90.
Dhainaut JF, Schlemmer B. Meeting the needs of intensive care unit patient families. Am J Respir Crit Care Med. 2001;163:135–9.
Heyland DK, Rocker GM, Dodek PM, Kutsogiannis DJ, Konopad E, Cook DJ, et al. Family satisfaction with care in the intensive care unit: Results of a multiple center study*. Critical Care Med. 2002;30(7):1413–8.
Wall RJ, Curtis JR, Cooke CR, Engelberg RA. Family satisfaction in the ICU: differences between families of survivors and nonsurvivors. Chest. 2007;132(5):1425–33.
Azoulay E, Pochard F, Chevret S, Lemaire F, Mokhtari M, Le Gall JR, et al. Meeting the needs of intensive care unit patient families: a multicenter study. Am J Respir Crit Care Med. 2001;163(1):135–9.
Kay HS, Oliver K, Kurt S, Marcel Z, Ulrike M, Hans UR. Family satisfaction in the intensive care unit: what makes the difference? Intensive Care Med. 2009;35:2051–9.
Sundararajan K, Sullivan TR, Sullivan TS, Chapman M. Determinants of family satisfaction in the intensive care unit. Anaesth Intensive Care. 2012;40(1):159–65.
Huffines M, Johnson KL, Naranjo LLS, Lissauer M, Fishel MAM, Howes SMA, et al. Improving family satisfaction and participation in decision making in an intensive care unit. Critical Care Nurse. 2013;33(5):56–69.
Verhaeghe S, Defloor T, Van Zuuren F, Duijnstee M, Grypdonck M. The needs and experiences of family members of adult patients in an intensive care unit: a review of the literature. J Clinic Nurs. 2005;14(4):501–9.
Moreau D, Goldgran-Toledano D, Alberti C, Jourdain M, Adrie C, Annane D, et al. Junior versus senior physicians for informing families of intensive care unit patients. Am J Respir Crit Care Med. 2004;169(4):512–7.
Acknowledgements
This work would not have been possible without the kind assistance of many individuals and our organization. We thank the head of department and members of the Cardiothoracic Surgery Department, Heart Hospital, Hamad Medical Corporation, Qatar, for providing unlimited support and all the necessary information for the project. We are also grateful to the members of the Medical Research Department of Hamad Medical Corporation for their support throughout this project.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
ASO wrote the manuscript, designed the study, and submitted the manuscript. PS was responsible for data collection and management, and provided support in the initial study design and in writing the manuscript. MG and RT were responsible for data collection and conception of the study. AKT, as chair of the intensive care unit, provided general support, and contribute to the design of the study. All authors approved the final manuscript after reading.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Omar, A.S., Sivadasan, P.C., Gul, M. et al. Impact of fast-track discharge from cardiothoracic intensive care on family satisfaction. BMC Anesthesiol 15, 78 (2015). https://doi.org/10.1186/s12871-015-0060-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-015-0060-6