
Abstract
Background
Nasal high flow (NHF) may reduce hypoxia and hypercapnia during an endoscopic retrograde cholangiopancreatography (ERCP) procedure under sedation. The authors tested a hypothesis that NHF with room air during ERCP may prevent intraoperative hypercapnia and hypoxemia.
Methods
In the prospective, open-label, single-center, clinical trial, 75 patients undergoing ERCP performed with moderate sedation were randomized to receive NHF with room air (40 to 60 L/min, n = 37) or low-flow O2 via a nasal cannula (1 to 2 L/min, n = 38) during the procedure. Transcutaneous CO2, peripheral arterial O2 saturation, a dose of administered sedative and analgesics were measured.
Results
The primary outcome was the incidence of marked hypercapnia during an ERCP procedure under sedation observed in 1 patient (2.7%) in the NHF group and in 7 patients (18.4%) in the LFO group; statistical significance was found in the risk difference (-15.7%, 95% CI -29.1 – -2.4, p = 0.021) but not in the risk ratio (0.15, 95% CI 0.02 – 1.13, p = 0.066).
In secondary outcome analysis, the mean time-weighted total PtcCO2 was 47.2 mmHg in the NHF group and 48.2 mmHg in the LFO group, with no significant difference (-0.97, 95% CI -3.35 – 1.41, p = 0.421). The duration of hypercapnia did not differ markedly between the two groups either [median (range) in the NHF group: 7 (0 – 99); median (range) in the LFO group: 14.5 (0 – 206); p = 0.313] and the occurrence of hypoxemia during an ERCP procedure under sedation was observed in 3 patients (8.1%) in the NHF group and 2 patients (5.3%) in the LFO group, with no significant difference (p = 0.674).
Conclusions
Respiratory support by NHF with room air did not reduce marked hypercapnia during ERCP under sedation relative to LFO. There was no significant difference in the occurrence of hypoxemia between the groups that may indicate an improvement of gas exchanges by NHF.
Trial registration
The full date of first registration on jRCT: August 26, 2019.
Similar content being viewed by others


Background
For relatively invasive upper gastrointestinal endoscopy procedures, such as an endoscopic retrograde cholangiopancreatography (ERCP), moderate sedation is routinely used to reduce patient anxiety and can also improve the endoscopist’s satisfaction [1, 2]. However, it has been reported that the frequently used sedation during an ERCP is associated with the occurrence of deep sedation linked to possible respiratory depression at rates as high as 35% [3]. Respiratory complications that occur during sedation may have a higher risk of hypercapnia than hypoxemia [4,5,6,7,8]. During sedation, supplemental oxygen (O2) administered through a nasal cannula can maintain the peripheral arterial O2 saturation at a normal level; however, hypoventilation may still be sustained.
Nasal high flow (NHF) with or without supplemental O2 via a nasal cannula interface may provide respiratory support in patients under sedation. NHF is commonly used in patients with acute respiratory failure and there is a substantial interest in its use during a perioperative period and procedural sedation [9,10,11]. It improves respiratory function primarily by generating low-level positive airway pressure and reducing the re-breathing from anatomical dead space [12]. During sleep, NHF without supplemental O2 is capable of reducing the re-breathing of CO2 from anatomical dead space by 45% and lowering minute volume ventilation [13]. Several randomized controlled trials (RCTs) and a retrospective study of the application of NHF with supplemental O2 (50 to 100%) during ERCP with sedation have revealed the efficacy of NHF to preserve oxygenation and the prevention of hypercapnia [14,15,16,17].
The purpose of this clinical trial was to investigate NHF without supplemental O2 as a respiratory support during sedation in patients undergoing ERCP. Taken together, the authors hypothesized that nasal high flow (NHF) of air used during moderate sedation can improve PtcCO2 and maintain SpO2 > 90% without increasing FiO2 in the inspired gas, compared with low-flow O2 (LFO) supplementation.
Methods
The study was conducted at Nagasaki University Hospital with the approval of Nagasaki University’s Clinical Research Review Board (`7180001) and written informed consent was obtained from all subjects participating in this study. This clinical trial was registered prior to patient enrollment in the Japan Registry of Clinical Trials (jRCTs072190021; Principal investigator: Takao Ayuse; Date of registration: August 26, 2019). The authors have previously reported the aims and protocol of the current study [18], which are briefly summarized below.
Study design
The present clinical trial was a prospective, randomized, controlled, open-label, single-center investigation into the efficacy of NHF use in patients undergoing ERCP under intravenous anesthesia and was carried out and analyzed in accordance with Consolidated Standards of Reporting Trials (CONSORT) guidelines [19]. The trial comprised two groups of participants who were randomized 1:1 to receive either low-flow O2 via a nasal cannula (LFO) (1 to 2 L/min: FiO2 0.22 to 0.28) or NHF at 40 to 60 L/min of room air (FiO2 0.21) during the ERCP.
Recruitment of participants
Participants were recruited from Nagasaki University Hospital and were required to provide written informed consent. The inclusion criteria were as follows: adult patients between the ages of 20 and 85 years who gave informed consent after being fully informed of all details of this study. The exclusion criteria were: 1) continuous administration of O2 by nasal cannula (home O2 therapy), 2) inability to breathe nasally, 3) use of antithrombotic drugs that could not be reduced or discontinued on the day before ERCP, 4) history of pneumothorax, 5) deemed inappropriate as a subject, 6) positive SARS-CoV-2 PCR test.
Study protocol
All participants undergo an ERCP under sedation using midazolam (approximately 0.05 mg/kg) with pethidine hydrochloride (an initial dose of 35 mg) to maintain the appropriate level of sedation using the Ramsay scale (Ramsay score 4: patient exhibits brisk response to light glabellar tap or loud auditory stimulus; and Ramsay score 5: patient exhibits a sluggish response to light glabellar tap or loud auditory stimulus). The sedation level is evaluated by Ramsay score before the start of sedation, after administration of a sedative, before the insertion of a scope, and at regular intervals after the end of treatment. The sedation level during treatment is evaluated and recorded every 5 min in the same manner as other vital sign evaluations. The NHF is generated by the Airvo™ 2 (Fisher & Paykel Healthcare Ltd., Auckland, New Zealand) with heated humidified air at a flow rate of 40 to 60 L/min.
Sedation is performed by an endoscopist using midazolam (approximately 0.05 mg/kg) with pethidine hydrochloride (initial dose of 35 mg) under consultation with an anesthesiologist. Midazolam bolus or pethidine hydrochloride is administered when patients are suspected of experiencing excessive pain or discomfort. When additional intravenous pethidine hydrochloride is administered, the administration unit should be 17.5 mg.
Additional doses of midazolam or pethidine hydrochloride are administered at the discretion of the endoscopist, but basically pethidine hydrochloride supersedes midazolam. The depth of sedation is assessed using the Ramsay scale every 5 min, along with the total dose of sedatives and the amount of sedative drug and effective opioid analgesic drug administered and the timing of each amount.
The transcutaneous CO2 partial pressure (PtcCO2) value is continuously measured by TCM4 (Radiometer Inc., Japan) every 2 s and the measured PtcCO2 value is output and recorded on the patient’s monitor (Nihon Kohden, BSM-9101) every 1 min via a connected output cable for analog value along with vital signs data. At the same time, the endoscopist reconfirms the vital signs, drug dosage, administration time, etc. from the notes recorded by the nurses. PtcCO2 of 60 mmHg or higher is defined as marked hypercapnia. PtcCO2 of 50 mmHg or higher and lower than 60 mmHg is defined as moderate hypercapnia.
For the SpO2 as the secondary outcome, the authors use the occurrence of hypoxemia with SpO2 < 90%. Because most of the continuously measured SpO2 values in the patient’s monitor showed a normal value SpO2 of > 90%, all the values of SpO2 are not recorded on the data acquisition device (REDCap). Therefore, SpO2 < 90% is defined as an occurrence of hypoxemia during the procedure and only the exact values of the occurrence of hypoxemia with SpO2 < 90% are recorded in all cases during the procedure.
To ensure patients’ safety, rescue 50% supplemental O2 is added in the NHF group and the O2 flow rate increased to 4 to 5 L/min in the LFO group if necessary, in order to maintain an SpO2 value > 90% during an ERCP procedure under sedation in the case of the occurrence of hypoxemia, just after confirming the incident of hypoxemia as a primary outcome during the procedure.
Outcomes
The primary endpoint:
-
Incidence of marked hypercapnia with a maximum PtcCO2 of 60 mmHg or higher (equivalent to PaCO2 of 55 mmHg or higher) during ERCP with sedation.
The secondary endpoints were as follows:
-
1)
Time-weighted total PtcCO2 during ERCP with sedation (Total PtcCO2 was calculated by totaling the PtcCO2 readings per minute and dividing this by the time measured.)
-
2)
Duration of hypercapnia showing PtcCO2 of 50 mmHg or higher (equivalent to PaCO2 of 45 mmHg or higher) during ERCP with sedation
-
3)
Incidence of hypoxemia with transcutaneous O2 saturation < 90% during ERCP with sedation
-
4)
The depth of anesthesia using the Ramsay scale
-
5)
The dose of anesthetic administered.
Randomization and data management
The principal investigator or co-investigator enrolled patients using Research Electronic Data Capture (REDCap) after confirming their eligibility [20]. Participants were randomly assigned to the two groups (ratio of 1:1) using the block method. Data was collected and randomization was performed using REDCap. In line with the research plan, procedures were monitored to confirm that the study was conducted appropriately.
Statistical analysis
As the authors have not found a previous study which evaluated the effect of NHF with air on PtcCO2, they plan to perform an exploratory clinical trial based on the feasibility of such a study. It was not possible to analyze or predict the required sample size in this clinical trial, so it was based on the estimated enrolment of 80 patients at Nagasaki University Hospital where approximately 250 ERCP procedures were performed under sedation over a one-year period. These 80 ERCP cases were assigned to two groups: the NHF group (40 cases) and the LFO group (40 cases).
The analysis population for the main analyses of this study is Full Analysis Set (FAS). FAS was defined as those subjects in the intention-to-treat for whom the efficacy endpoint, transcutaneous CO2 pressure, could be measured.
For efficacy analysis, the authors estimated risk ratios and 95% confidence intervals (CIs) for the occurrence of hypercapnia or marked hypercapnia by modified Poisson regression with body weight as an adjusted variable. In addition, risk differences were calculated by generalized regression analysis using the identity function. For hypoxia, risk ratios and risk differences were calculated without adjustment for body weight from the above model, because estimation was not unstable. The mean difference between the groups for PtcCO2 per unit time was also summarized and then compared using the Welch’s t-test. The Wilcoxon rank-sum test was used to analyze the Ramsay index. To calculate the relative risk, we adjusted the initial dose of sedative for body weight. Finally, the total dose of sedative was adjusted for body weight and risk ratios were calculated using Poisson regression with a logarithm of time as the offset term.
All statistical analyses were carried out using R, version 4.1.2. All p values were two sided, with p values less than 0.05 considered significant. Because of the potential for type I error due to multiple comparisons, findings for analyses of secondary endpoints should be interpreted as exploratory.
Results
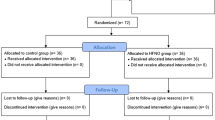
A total of 80 patients were enrolled and randomized to the NHF group (n = 40) or the LFO group (n = 40) from January 2020 to March 2021. As a result of exclusions, the number of patients analyzed in the NHF group was 37 and the number of patients analyzed in the LFO group was 38, as outlined in Fig. 1. The baseline characteristics of the patients and details of the scheduled procedures for each patient group, including the duration of the procedure and the presence of balloon-assisted enteroscopy (BAE) cases, are presented in Table 1. The duration of the procedure was 38.0 min (11–145) in the NHF group and 57.5 min (11–205) in the LFO group.

CONSORT flow chart. NHF: Nasal high flow, LFO: Low-flow oxygen via a nasal cannula, PtcCO2: Transcutaneous CO2 partial pressure
In primary outcome analysis, the incidence of marked hypercapnia during an ERCP procedure under sedation was observed in 1 patient (2.7%) in the NHF group and in 7 patients (18.4%) in the LFO group; statistical significance was found in the risk difference (risk difference: -15.7%, 95% CI -29.1 – -2.4, p = 0.021; risk ratio: 0.15, 95% CI 0.02 – 1.13, p = 0.066) (see Table 2).
In secondary outcome analysis, the mean (SD) total PtcCO2 per unit time was 47.2 mmHg (4.6) in the NHF group and 48.2 mmHg (5.7) in the LFO group, with no significant difference (-0.97, 95% CI -3.35 – 1.41, p = 0.421). The duration of hypercapnia did not differ markedly between the two groups either [median (range) in the NHF group: 7 (0 – 99); median (range) in the LFO group: 14.5 (0 – 206); p = 0.313]. Figure 2 shows the timeline sequence of PtcCO2 value for each group and suggests that although there was no statistically significant difference, this might indicate a tendency for the changes in PtcCO2 to differ between the two groups over time.

Sequence of PtcCO2 value of each group throughout this study. PtcCO2 values are presented as means. LFO: Low-flow oxygen via a nasal cannula
The incidence of hypoxemia during an ERCP procedure under sedation was observed in 3 patients (8.1%) in the NHF group and 2 patients (5.3%) in the LFO group, with no significant difference (risk difference: -2.8%, 95% CI -8.5 – 14.2; risk ratio: 1.54, 95% CI 0.27 – 8.70; p = 0.62).
The depth of sedation (Ramsay score) was not significantly different between the two groups [median (range) for the NHF group: 5 (4 – 6); median (range) for the LFO group: 5 (4 – 6); p = 0.488]. In regard to the anesthesia dose, there was no difference between the initial and total dose of midazolam and the initial dose of pethidine hydrochloride. The total dose of pethidine hydrochloride (mg) was not different in the NHF group compared with the LFO group [median (range) for the NHF group: 35 (0 – 105); median (range) for the LFO group: 70 (0 – 175); p = 0.177]. There was no occurrence of any adverse events [18].
Discussion
The main findings of this clinical trial are: 1) there was no significant difference in the incidence of marked hypercapnia with PtCO2 ≥ 60 mmHg and in the time-weighted total PtcCO2 during ERCP with sedation and in the hypoxemia with SpO2 ≦ 90% during ERCP with sedation between the NHF-with-air group and the LFO group; 2) there was no significant difference in the occurrence of hypoxemia between the groups that may indicate an improvement of gas exchange by NHF without supplemental O2.
Effect of NHF on arterial and tissue carbon dioxide
In this clinical trial, there was no significant difference in the occurrence of marked hypercapnia between the NHF group and the LFO group with limited sample size. Although there was no statistically significant difference, this might indicate a tendency for the changes in PtcCO2 to differ between the two groups over time (Table 2). This finding is consistent with a recent study of 126 adults undergoing elective cardiac implantable electronic device procedures under sedation by Conway et al. [21] which reported that the difference in PtcCO2 was 0 kPa between NHF at 50 L/min and FiO2 of 0.50 or face-mask O2 at 8 L/min. Vijitpavan A et al. [22] suggested that the use of NHF in patients undergoing endovascular surgery under deep sedation reduced desaturation events when compared with conventional O2 via nasal cannula with no difference in the level of PaCO2 in arterial blood gas analyses (42.48 in conventional nasal canula vs. 44.8 in NHF; p = 0.107). Higuchi H. et al. [23] suggested that the PaCO2 was 50.1 ± 6.0 mmHg in the standard nasal cannula group and 47.6 ± 4.8 mmHg in the NHF group (flow 40 L/min, 40% O2).
Effect of NHF on oxygenation
In this clinical trial, there was no significant difference in the incidence of hypoxemia between the two groups. NHF without supplemental O2 was chosen to verify whether the respiratory support could improve gas exchange and normalize both O2 and CO2 during hypoventilation caused by sedation. It was found that O2 saturation could be maintained with NHF with room air during an ERCP procedure under moderate sedation. Although a limited number of studies in the past have shown that hypoxemia could be attenuated with the use of NHF during endoscopy in ERCP procedures [9, 17, 24, 25], most of these studies also provided supplemental O2 (50% to 100%) and in the current study supplemental O2 was not required. Conway et al. [21] reported that the odds ratio for O2 desaturation for the NHF with 50% O2 supplement group was 1:2. Nay et al. [26] suggested that a decrease in SpO2 < 92% occurred in 9.4% for the NHF with 50% O2 supplement group and 33.5% for the standard O2 groups in 379 patients undergoing gastrointestinal endoscopy under deep sedation. Lin et al. [25] reported that NHF with 100% O2 supplement also decreased the incidence of hypoxia from 8.4% in the nasal cannula group to 0% (P < 0.001) in the NHF group. Mazzeffi MA et al. [27] reported that high-flow nasal cannula O2 significantly reduced the incidence of hypoxemia events from 33.1% to 21.2% (P = 0.03) in a recent clinical study of 262 esophagogastroduodenoscopy patients.
The study data adds to these earlier findings, suggesting that the positive airway pressure and reduction of dead space provided by NHF can be effective in maintaining oxygenation without supplemental O2 during ERCP procedures under moderate sedation compared to LFO.
Limitations
There are several limitations in this clinical trial. First, the authors’ findings should be carefully generalized because of the limited number of patients enrolled and given the heterogeneous nature of the Japanese patients taking part in this study. Although the administration of midazolam or pethidine hydrochloride was based on the arbitrary evaluation by endoscopists in a single research center, it is not possible to indicate standardized results in this study.
Second, the average BMI (kg/m2) of the enrolled Japanese patients was 22.4 (15.0 –30.6) for the NHF group and 21.9 (15.9 – 36.3) for the LFO group, which is less than 25 of the obesity criteria. However, previous studies testing the effects of NHF on obese patients have revealed that NHF cannot reduce the incidence of desaturation compared to standard nasal cannula or face mask. Riccio CA et al. [10] suggested that the desaturation rates in the high-flow nasal cannula group (n = 28, BMI: 48 kg/m2) (39.3%) and the standard nasal cannula group (n = 31, BMI: 49 kg/m2) (45.2%) were not significantly different (p = 0.79). These researchers concluded that high- and low-flow O2 supplementation groups at similar FiO2 were not significantly different for the prevention of arterial O2 desaturation in morbidly obese patients undergoing propofol sedation for colonoscopy. Thiruvenkatarajan V et al. [15] reported that in high-risk obesity patients (BMI: 28.2 to 30.0 kg/m2) undergoing an ECRP procedure, O2 therapy with high-flow nasal O2also did not reduce the rate of hypoxemia or hypercapnia, compared with combined oral and nasal low-flow O2. Therefore, the authors of the present study consider that there is a need for further work to explore the optimal flow rate with O2 supplementation using NHF in high-risk patients for respiratory functions, including obesity and any respiratory complications, such as COPD.
Third, it should be noted that this trial was performed during moderate sedation. Deep sedation using another sedative agent, such as dexmedetomidine or anesthetics propofol, is now well accepted in managing ERCP. Vijitpavan et al. [22] suggested that the use of NHF in patients undergoing endovascular surgery under deep sedation using propofol reduced desaturation events greater than the use of a traditional nasal cannula. Therefore, further RCTs would be required to confirm the effects of NHF on respiratory management during ERCP under moderate to deep sedation.
Forth, masking was not possible due to the nature of the study.
Finally, in this study pethidine hydrochloride was administered when patients were suspected of experiencing excessive pain or discomfort without evaluating analgesia quantitatively using a VAS score as had been used in a previous study [28]. It might prove helpful to investigate the distinguished role of sedation and analgesia using any kind of analgesia rating score during this procedure, because analgesic can induce the respiratory depression rate and hypercapnia [29].
Conclusion
Respiratory support by NHF with air did not reduce marked hypercapnia during ERCP under sedation relative to LFO. There was no significant difference in the occurrence of hypoxemia between the two groups that may indicate an improvement of gas exchange by NHF.
Availability of data and materials
The datasets used and/or analyzed during the current study are available on reasonable request from the author for correspondence.
Abbreviations
- BAE:
-
Balloon-assisted enteroscopy
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- CO2 :
-
Carbon dioxide
- CONSORT:
-
Consolidated Standards of Reporting Trials
- CRB:
-
Clinical Research Review Board
- DG:
-
Distal gastrectomy
- ERCP:
-
Endoscopic retrograde cholangiopancreatography
- FEV1.0%:
-
Forced expiratory volume percentage in one second
- FiO2 :
-
Fraction of inspired oxygen
- jRCT:
-
Japan Registry of Clinical Trials
- LFO:
-
Low-flow oxygen via a nasal cannula
- NHF:
-
Nasal high flow
- PaCO2 :
-
Partial pressure of arterial carbon dioxide
- PCR:
-
Polymerase chain reaction
- PD:
-
Pancreaticoduodenectomy
- PETCO2 :
-
Partial pressure of end-tidal carbon dioxide
- PtcCO2 :
-
Transcutaneous CO2 partial pressure
- RCT:
-
Randomized controlled trial
- REDCap:
-
Research Electronic Data Capture
- SD:
-
Standard deviation
- SpO2 :
-
Transcutaneous oxygen saturation
- TG:
-
Total gastrectomy
References
McQuaid KR, Laine L. A systematic review and meta-analysis of randomized, controlled trials of moderate sedation for routine endoscopic procedures. Gastrointest Endosc. 2008;67(6):910–23.
Kinugasa H, Higashi R, Miyahara K, Moritou Y, Hirao K, Ogawa T, Kunihiro M, Nakagawa M. Dexmedetomidine for conscious sedation with colorectal endoscopic submucosal dissection: a prospective double-blind randomized controlled study. Clin Transl Gastroenterol. 2018;9(7):167.
Patel S, Vargo JJ, Khandwala F, Lopez R, Trolli P, Dumot JA, Conwell DL, Zuccaro G. Deep sedation occurs frequently during elective endoscopy with meperidine and midazolam. Am J Gastroenterol. 2005;100(12):2689–95.
Kaess BM, Feurich F, Burkle G, Ehrlich JR. Midazolam addition to analgosedation for pulmonary vein isolation may increase risk of hypercapnia and acidosis. Int J Cardiol. 2018;259:100–2.
Nelson DB, Freeman ML, Silvis SE, Cass OW, Yakshe PN, Vennes J, Stahnke LL, Herman M, Hodges J. A randomized, controlled trial of transcutaneous carbon dioxide monitoring during ERCP. Gastrointest Endosc. 2000;51(3):288–95.
De Oliveira GS Jr, Fitzgerald PC, Hansen N, Ahmad S, McCarthy RJ. The effect of ketamine on hypoventilation during deep sedation with midazolam and propofol: a randomised, double-blind, placebo-controlled trial. Eur J Anaesthesiol. 2014;31(12):654–62.
Nieuwenhuijs D, Bruce J, Drummond GB, Warren PM, Wraith PK, Dahan A. Ventilatory responses after major surgery and high dependency care. Br J Anaesth. 2012;108(5):864–71.
Raiten J, Elkassabany N, Gao W, Mandel JE. Novel uses of high frequency ventilation outside the operating room. Anesth Analg. 2011;112(5):1110–3.
Douglas N, Ng I, Nazeem F, Lee K, Mezzavia P, Krieser R, Steinfort D, Irving L, Segal R. A randomised controlled trial comparing high-flow nasal oxygen with standard management for conscious sedation during bronchoscopy. Anaesthesia. 2018;73(2):169–76.
Riccio CA, Sarmiento S, Minhajuddin A, Nasir D, Fox AA. High-flow versus standard nasal cannula in morbidly obese patients during colonoscopy: a prospective, randomized clinical trial. J Clin Anesth. 2019;54:19–24.
Sago T, Watanabe K, Kawabata K, Shiiba S, Maki K, Watanabe S. A nasal high-flow system prevents upper airway obstruction and hypoxia in pediatric dental patients under intravenous sedation. J Oral Maxillofac Surg. 2021;79(3):539–45.
Pinkham MI, Domanski U, Franke KJ, Hartmann J, Schroeder M, Williams T, Nilius G, Tatkov S. Effect of respiratory rate and size of cannula on pressure and dead-space clearance during nasal high flow in patients with COPD and acute respiratory failure. J Appl Physiol (1985). 2022;132(2):553–63.
Pinkham M, Burgess R, Mundel T, Tatkov S. Nasal high flow reduces minute ventilation during sleep through a decrease of carbon dioxide rebreathing. J Appl Physiol. 2019;126(4):863–9.
Schumann R, Natov NS, Rocuts-Martinez KA, Finkelman MD, Phan TV, Hegde SR, Knapp RM. High-flow nasal oxygen availability for sedation decreases the use of general anesthesia during endoscopic retrograde cholangiopancreatography and endoscopic ultrasound. World J Gastroenterol. 2016;22(47):10398–405.
Thiruvenkatarajan V, Dharmalingam A, Arenas G, Wahba M, Liu WM, Zaw Y, Steiner R, Tran A, Currie J, collaborators. Effect of high-flow vs. low-flow nasal plus mouthguard oxygen therapy on hypoxaemia during sedation: a multicentre randomised controlled trial. Anaesthesia. 2021. https://doi.org/10.1111/anae.15527.
Cha B, Lee MJ, Park JS, Jeong S, Lee DH, Park TG. Clinical efficacy of high-flow nasal oxygen in patients undergoing ERCP under sedation. Sci Rep. 2021;11(1):350.
Kim SH, Bang S, Lee KY, Park SW, Park JY, Lee HS, Oh H, Oh YJ. Comparison of high flow nasal oxygen and conventional nasal cannula during gastrointestinal endoscopic sedation in the prone position: a randomized trial. Can J Anaesth. 2021;68(4):460–6.
Ayuse T, Sawase H, Ozawa E, Nagata K, Komatsu N, Sanuki T, Kurata S, Mishima G, Hosogaya N, Nakashima S, et al. Study on prevention of hypercapnia by nasal high flow in patients undergoing endoscopic retrograde cholangiopancreatography during intravenous anesthesia. Medicine (Baltimore). 2020;99(19):e20036.
Chan AW, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, Krleža-Jerić K, Hróbjartsson A, Mann H, Dickersin K, Berlin JA, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158(3):200–7.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81.
Conway A, Collins P, Chang K, Kamboj N, Filici AL, Lam P, Parotto M. High flow nasal oxygen during procedural sedation for cardiac implantable electronic device procedures: a randomised controlled trial. Eur J Anaesthesiol. 2021;38(8):839–49.
Vijitpavan A, Kooncharoensuk Y. High flow versus conventional nasal cannula for oxygenation and ventilation maintenance during surgery with intravenous deep sedation by propofol: a randomized controlled study. BMC Anesthesiol. 2021;21(1):214.
Higuchi H, Takaya-Ishida K, Miyake S, Fujimoto M, Nishioka Y, Maeda S, Miyawaki T. Comparison of oxygen saturation between nasal high-flow oxygen and conventional nasal cannula in obese patients undergoing dental procedures with deep sedation: a randomized crossover trial. J Oral Maxillofac Surg. 2021;79(9):1842–50.
Service JA, Bain JS, Gardner CP, McNarry AF. Prospective experience of high-flow nasal oxygen during bronchoscopy in 182 patients: a feasibility study. J Bronchology Interv Pulmonol. 2019;26(1):66–70.
Lin Y, Zhang X, Li L, Wei M, Zhao B, Wang X, Pan Z, Tian J, Yu W, Su D. High-flow nasal cannula oxygen therapy and hypoxia during gastroscopy with propofol sedation: a randomized multicenter clinical trial. Gastrointest Endosc. 2019;90(4):591–601.
Nay MA, Fromont L, Eugene A, Marcueyz JL, Mfam WS, Baert O, Remerand F, Ravry C, Auvet A, Boulain T. High-flow nasal oxygenation or standard oxygenation for gastrointestinal endoscopy with sedation in patients at risk of hypoxaemia: a multicentre randomised controlled trial (ODEPHI trial). Br J Anaesth. 2021;127(1):133–42.
Mazzeffi MA, Petrick KM, Magder L, Greenwald BD, Darwin P, Goldberg EM, Bigeleisen P, Chow JH, Anders M, Boyd CM, et al. High-flow nasal cannula oxygen in patients having anesthesia for advanced esophagogastroduodenoscopy: HIFLOW-ENDO, a randomized clinical trial. Anesth Analg. 2021;132(3):743–51.
Mauri T, Spinelli E, Pavlovsky B, Grieco DL, Ottaviani I, Basile MC, Dalla Corte F, Pintaudi G, Garofalo E, Rundo A, et al. Respiratory drive in patients with sepsis and septic shock: modulation by high-flow nasal cannula. Anesthesiology. 2021;135(6):1066–75.
Tarradell R, Pol O, Farre M, Barrera E, Puig MM. Respiratory and analgesic effects of meperidine and tramadol in patients undergoing orthopedic surgery. Methods Find Exp Clin Pharmacol. 1996;18(3):211–8.
Acknowledgements
We deeply appreciate that Mary Dobbyn has made a significant contribution for reviewing and proofreading as a professional proofreader (www.marydobbyn.co.nz).
Funding
This study is funded by the institutional budget and partly by Fisher & Paykel Healthcare Ltd., Auckland, New Zealand.
The equipment for nasal high flow was provided by Fisher & Paykel Healthcare Ltd., Auckland, New Zealand.
This study is funded by the institutional budget and partly supported by Fisher & Paykel Healthcare Ltd., Auckland, New Zealand.
M.I.P. and S.T. are employees of Fisher & Paykel Healthcare Ltd., the manufacturers of the nasal high flow (NHF) devices used in the study. T.A. has received funding and support from Fisher & Paykel Healthcare Ltd.
The study is sponsored by the Nagasaki University Graduate School of Biomedical Sciences. (The sponsor’s representative is Dr. Ayuse; tel.: + 81–95-819–7713; email: ayuse@nagasaki-u.ac.jp.)
Author information
Authors and Affiliations
Contributions
Conception and design: Hironori Sawase, Eisuke Ozawa, Takao Ayuse, Kazuhiko Nakao, Kazuto Ashizawa, Shinji Kurata, Maximilian Ichabod Pinkham, Stanislav Tatkov, Shuntaro Sato. Consulting and advice for sedation: Taiga Ichinomiya, Rintaro Yano. Data collection: Hironori Sawase, Eisuke Ozawa, Naohiro Komatsu, Kazuyoshi Nagata, Hisamitsu Miyaaki. Registration of clinical trial: Takao Ayuse. Analysis and interpretation of the data: Hiroshi Yano, Shuntaro Sato, Hironori Sawase, Eisuke Ozawa, Maximilian Ichabod Pinkham, Stanislav Tatkov, Takao Ayuse. Drafting of the article: Hiroshi Yano, Shuntaro Sato, Hironori Sawase, Eisuke Ozawa, Maximilian Ichabod Pinkham, Stanislav Tatkov, Takao Ayuse. Critical revision of the article for important intellectual content and final approval of the article: Takao Ayuse, Shinji Kurata, Hironori Sawase, Eisuke Ozawa, Hiroshi Yano, Taiga Ichinomiya, Rintaro Yano, Maximilian Ichabod Pinkham, Stanislav Tatkov, Shuntaro Sato, Naohiro Komatsu, Kazuyoshi Nagata, Kazuto Ashizawa, Kazuhiko Nakao. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted at Nagasaki University Hospital with the approval of Nagasaki University’s Clinical Research Review Board (CRB7180001) and written informed consent was obtained from all subjects participating in this study. This clinical trial was registered prior to patient enrollment in the Japan Registry of Clinical Trials (jRCTs072190021; Principal investigator: Takao Ayuse; Date of registration: August 26, 2019). All methods were carried out in accordance with relevant guidelines and regulations (Declaration of Helsinki).
Consent for publication
Not applicable
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sawase, H., Ozawa, E., Yano, H. et al. Respiratory support with nasal high flow without supplemental oxygen in patients undergoing endoscopic retrograde cholangiopancreatography under moderate sedation: a prospective, randomized, single-center clinical trial. BMC Anesthesiol 23, 156 (2023). https://doi.org/10.1186/s12871-023-02125-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-023-02125-w