
Abstract
Background
This study aims to comprehend the levels of dry mouth and thirst in patients after general anesthesia, and to identify the factors influencing them.
Methods
The study included all patients transferred to the Post Anesthesia Care Unit (PACU) at the Second Affiliated Hospital of Dalian Medical University between August 2021 and November 2021 after undergoing general anesthesia. A thirst numeric rating scale was utilized to conduct surveys, enabling the assessment of thirst incidence and intensity. Statistical analysis was performed to explore patient thirst levels and the associated factors.
Results
The study revealed a thirst incidence rate of 50.8%. Among the thirst intensity ratings, 71.4% of patients experienced mild thirst, 23.0% reported moderate thirst, and 5.6% expressed severe thirst. Single-factor statistical analysis of potential risk factors among the enrolled cases indicated that gender, history of coronary heart disease, surgical duration, intraoperative fluid volume, intraoperative blood loss, intraoperative urine output, and different surgical departments were linked to post-anesthetic thirst in patients undergoing general anesthesia. Multifactorial Logistic regression analysis highlighted age, gender, history of coronary heart disease, fasting duration, and intraoperative fluid volume as independent risk factors for post-anesthetic thirst in patients undergoing general anesthesia. Moreover, age, gender, history of coronary heart disease, and intraoperative fluid volume were also identified as risk factors for varying degrees of thirst.
Conclusion
The incidence and intensity of post-anesthetic thirst after general anesthesia are relatively high. Their occurrence is closely associated with age, gender, history of coronary heart disease, fasting duration, and intraoperative fluid volume.
Similar content being viewed by others

Background
As society progresses and medical capabilities improve, doctors are not only focused on curing patients’ illnesses but also on providing them with a more comfortable medical experience. The recovery period after general anesthesia is crucial for the restoration of various bodily functions in patients. Due to factors like pre-operative fasting, mechanical ventilation during surgery, and the effects of anesthesia drugs, patients in The Post Anesthesia Care Unit (PACU) often experience varying degrees of discomfort, including dry mouth, thirst, throat discomfort, pain, anxiety, and fear [1, 2]. Thirst is the most intense symptom experienced by patients after extubation during the recovery period following general anesthesia [3], with an incidence rate as high as 67.7% [4]. Thirst not only increases the risk of oral infections but also hinders the recovery of gastrointestinal function and reduces the secretion capacity of digestive glands. It can also lead to significant anxiety and stress, thereby increasing oxygen consumption and the metabolic burden on organs [5,6,7]. In severe cases, it might even induce delirium [8], consequently impacting postoperative recovery [9,10,11,12]. Inadequate attention postoperatively, lack of standardized assessment methods, and incomplete treatment strategies [13] have led to clinical doctors lacking a systematic identification and evidence-based management of thirst.
Surgical patients often experience thirst during the perioperative period due to increased osmotic pressure or decreased plasma volume. Some studies attribute thirst to excessively long preoperative fasting periods. Consequently, shortening these fasting periods has emerged as a promising avenue of research. However, this largely overlooks patients’ underlying risk factors. Existing research mostly focuses on specific surgeries, such as laparoscopic cholecystectomy [14], or specific populations, like children [15]. Children, distinct from adults due to their lower tolerance for thirst and lesser self-control, are a common subject of such research [16]. Therefore, this study incorporates various surgical departments, as well as factors like gender and age, to investigate the incidence and risk factors of postoperative thirst. This research aims to improve perioperative diagnostic and treatment approaches, offer personalized support, and ultimately enhance patients’ perioperative experiences.
Materials and methods
Participants
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Dalian Medical University (IRB 2021 − 113), and written informed consent was obtained from all subjects participating in the trial. The trial was registered prior to patient enrollment at the China Clinical Trial Registry (ChiCTR) – a primary registration agency of the World Health Organization International Clinical Trials Registry Platform (chictr.org.cn) (Registration number: ChiCTR2100049748, The Second Affiliated Hospital of Dalian Medical University, Principal investigator: Zhaoyang Xiao, Date of registration: 2021-08-09). This manuscript adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
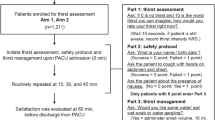
The study utilized a cross-sectional design, with samples collected from all patients transferred to the Post Anesthesia Care Unit (PACU) of the Second Affiliated Hospital of Dalian Medical University between August 2021 and November 2021 after undergoing general anesthesia. Informed consent was obtained from both patients and their families. The first patient was enrolled on August 14, 2021. Inclusion criteria: Patients in PACU recovering from general anesthesia without a history of oral or head and neck radiotherapy, without kidney dysfunction necessitating hemodialysis, and not on long-term secretion-suppressing medication. Exclusion criteria: Patients under 18 years old; patients who, due to various reasons, are unable to communicate effectively after regaining consciousness; neurosurgical patients whose autonomous breathing has recovered but consciousness has not; emergency cases; patients transferred unexpectedly from PACU to the Intensive Care Unit (ICU) (Fig. 1).

Flowchart of drainage and narcotics
Outcome ascertainment
The primary outcome was the occurrence of post-anesthetic emergence thirst in PACU after endotracheal extubation. The secondary outcomes included the level of thirst intensity and the subjective willingness of patients to drink proactively.
Exposure measurement
Thirst Assessment: We evaluated patient thirst using the Visual Analog Scale (VAS) developed by the National Institutes of Health in the United States. Patients were asked to indicate their subjective intensity of thirst by selecting a point on a numerical assessment scale (VAS), divided into 10 equal segments [17]. The VAS scale ranged from 0 to 10, where scores of 1–3 represented mild thirst, 4–6 indicated moderate thirst, and 7–10 indicated severe thirst [18]. After providing relevant training to the PACU staff, we conducted the assessments following a standardized procedure (as illustrated in Supplementary Material) to eliminate variations caused by differing questioning techniques [19]. We then recorded both the presence of thirst and the thirst intensity VAS score (VAS score 0–10) reported by the patients.
Covariate assessment
Covariate selection was on the basis of previous investigations and clinical experience. the following variables was included: demographic information (age, gender, body mass index, medical history), preoperative fasting duration, ASA classification, administration of anticholinergic drugs (such as atropine, scopolamine), duration of surgery and anesthesia, intraoperative fluid intake, blood loss, and urine output.
Statistical methods
SPSS 24.0 software was employed to analyze post-anesthetic emergence thirst and the corresponding scores among extubated patients. Patient characteristics were summarized, with mean ± standard deviation employed to present normally distributed continuous variables. Inter-group comparisons were conducted using independent sample t-tests, while repeated measures analysis of variance was used for within-group comparisons of normally distributed continuous variables. Non-normally distributed continuous variables were presented as median (M) and interquartile range (IQR), with inter-group comparisons being performed through the Mann-Whitney U test. Categorical data were expressed as proportions (%), and inter-group comparisons were carried out using the chi-squared test. Variables exhibiting a p-value of < 0.2 in univariate analysis were incorporated as covariates in the subsequent multivariate analysis. Collinearity among variables was assessed utilizing VIF, and post the removal of variables exhibiting high correlations, the remaining variables were included in multivariate binary logistic regression analysis to determine independent predictors of thirst. An ordinal logistic regression analysis was conducted using varying levels of thirst as the dependent variable, with statistical significance being denoted by a P-value < 0.05.
Results
Among the included sample of 2695 cases, the mean age was 51.82 years, with females accounting for 60.1% of the sample. The average BMI was 24.29 kg/m². ASA Class II (86.6%) was predominant, with an average surgery duration of 101 min. Patients with comorbidities of hypertension, diabetes, and coronary heart disease constituted 18.9%, 8.1%, and 3.2%, respectively (Table 1). When compared with non-thirsty patients, those experiencing thirst had a lower average age, a higher proportion of coronary heart disease, longer preoperative fasting and surgery durations, increased intraoperative fluid balance, and gynecological surgeries were the most frequent among various categories of procedures.
Univariate analysis of suspected risk variables revealed that gender, history of coronary heart disease, surgery duration, intraoperative fluid infusion volume, intraoperative blood loss, intraoperative urine output, and different surgical departments (P < 0.05) were correlated factors for post-anesthetic emergence thirst in general anesthesia patients (Table 1). In order to control for confounding effects, variables with p-values < 0.2 from the univariate analysis were utilized as covariates. Collinearity between variables was assessed using VIF, and highly correlated variables were removed before entering the remaining variables into a multivariate analysis as independent variable set X. Using post-anesthetic emergence thirst as dependent variable Y, a binary logistic regression was performed using forward stepwise analysis (Table 2). The results indicated independent risk factors for post-anesthetic emergence thirst in general anesthesia patients: age, gender, history of coronary heart disease, preoperative fasting duration, and intraoperative fluid infusion volume (Table 2). Moreover, the occurrence rate of post-anesthetic emergence thirst was higher in males than in females, with males having a 1.26-fold increased risk (OR: 1.261, 95% CI 1.077 ∼ 1.476). Patients with a history of coronary heart disease had a 1.7-fold increased risk (OR: 1.704, 95% CI 1.071 ∼ 2.686). Each additional hour of preoperative fasting increased the risk by 1.034-fold (OR: 1.034, 95% CI 1.004 ∼ 1.066). For each additional liter of intraoperative fluid infusion, the risk increased by 1.469-fold (OR: 1.469, 95% CI 1.264 ∼ 1.707). Age demonstrated a significant negative relationship with thirst; the older the age, the lower the risk of post-anesthetic emergence thirst (OR: 0.994, 95% CI 0.989 ∼ 0.999).
Among these patients experiencing post-anesthetic emergence thirst, 71.4% had mild thirst, 23.0% had moderate thirst, and 5.6% had severe thirst (Fig. 2a). Among them, 4.2% stated no desire to drink water, 19.9% expressed indifference towards drinking water, 69.0% expressed a desire to drink water, and 7.0% strongly expressed the desire to drink water (Fig. 2b). Employing different levels of thirst as the dependent variable, ordinal logistic regression analysis identified age, gender, history of coronary heart disease, and intraoperative fluid infusion volume as risk factors for varying degrees of thirst (Table 3).

Proportion of Different Thirst Levels (a) and Drinking Preferences (b)
Discussion
This study represents the inaugural exploration into the occurrence rate and risk factors of post-extubation thirst among general anesthesia patients. Due to increased osmolarity or decreased plasma volume, surgical patients often experience thirst during the perioperative period. In this study, the occurrence rate of thirst following extubation in general anesthesia patients was found to be 50.9%. Among the graded levels of thirst, 71.4% of patients reported mild thirst, 23.0% moderate thirst, and 5.6% severe thirst. Statistical analysis was conducted on suspected risk factors among the enrolled cases. Univariate analysis identified 7 factors that influence the occurrence of post-extubation thirst in general anesthesia patients, namely, gender, history of coronary heart disease, surgery duration, intraoperative fluid infusion volume, intraoperative blood loss, intraoperative urine output, and different surgical departments. Binary logistic regression analysis revealed that age, gender, history of coronary heart disease, preoperative fasting duration, and intraoperative fluid infusion volume were independent risk factors for post-extubation thirst in general anesthesia patients. Among these, age, gender, history of coronary heart disease, and intraoperative fluid infusion volume were also identified as risk factors for different levels of thirst.
a physiological perspective, the sensation of thirst primarily arises due to decreased fluid volume and increased concentration of osmotically active particles (osmolarity) [20]. An elevation in the concentration of solutes, including sodium, glucose, and other small particles, increases osmolarity. In males, the stimulation of red blood cell growth and development by male hormones leads to a higher red blood cell count and higher hematocrit compared to females, indirectly affecting blood viscosity and resulting in higher blood viscosity indices in males than in females. Hence, it is worth investigating whether male patients are relatively osmotically active compared to female patients. Currently, there is no relevant research on this, warranting further exploration of the relationship between the two. Cardiovascular diseases often entail changes in hemodynamics and hemorheological parameters (plasma viscosity, whole blood high shear viscosity, whole blood low shear viscosity, hematocrit, fibrinogen). Among these, blood viscosity is a crucial hemorheological parameter. Patients with cardiovascular diseases experience changes due to long-term accumulation of pathological characteristics, necessitating reductions in cardiac circulatory load, constraints on fluid intake, and maintenance of negative fluid balance, ultimately leading to increased plasma osmolarity. When plasma osmolarity rises, cells undergo dehydration, which subsequently raises blood viscosity and frequently exacerbates symptoms of thirst and dry mouth.
High osmolarity and low blood volume result from pathological and physiological factors, preoperative fasting, and perioperative fluid loss. Fasting stimulates hypothalamic osmoreceptors and the thirst center through mechanisms including water loss, reduced blood glucose levels, and depletion of extracellular fluid. Thirst arises when stimulation of the hypothalamic satiety center decreases while stimulation of the feeding center increases [21]. Dilmen et al.‘s study [22] found that preoperative carbohydrate intake, which shortens fasting time, had a positive effect on postoperative thirst, aligning with the conclusions of this study.
Fitzsimons’ study [23] revealed that experimental animals consumed more water when subjected to peritoneal dialysis or blood withdrawal, reducing fluid volume without altering plasma osmolarity. This indicates that decreased plasma volume stimulates the thirst center, generating a sense of thirst and prompting increased water intake [24]. Clinically, hemodynamically unstable patients are often characterized by low blood volume [25]. A meta-analysis [26] concerning the use of hydroxyethyl starch in surgery demonstrated that compared to crystalloids alone, the use of hydroxyethyl starch improved hemodynamic stability and reduced the need for vasopressors (P < 0.001). This implies that hydroxyethyl starch compensates for hemodynamic instability due to low blood volume. Consequently, the higher risk of thirst occurrence associated with supplementing patients with crystalloids and colloids in our study may be attributed to the possible hemodynamic instability induced by colloids. These patients might have experienced insufficient blood volume before surgery. Of course, this conjecture necessitates the exclusion of premises such as the presence of preoperative hypertension and poor vascular elasticity to definitively establish that insufficient blood volume causes hemodynamic instability in patients.
Over the past 20 years, the concept of Enhanced Recovery After Surgery (ERAS) has rapidly and comprehensively developed since its introduction [27]. ERAS aims to apply evidence-based, multi-modal optimization protocols through interdisciplinary collaboration, with innovative minimally invasive surgical techniques as the core, to reduce perioperative futile and ineffective medical interventions, stress responses, organ dysfunction, and related complications. We now anticipate not only successful surgery, reduced operation time, minimal incisions, and postoperative pain, but also a more comfortable perioperative experience based on ERAS principles. Shortening patient recovery time, increasing bed turnover rate, improving medical resource utilization efficiency, and alleviating the burden on healthcare insurance are the ultimate goals [28,29,30].
Up to now, most research on alleviating postoperative thirst has occurred abroad, with relatively little attention in China. The related interventions are relatively simple and non-invasive. It is necessary to intervene in controllable risk factors to reduce the occurrence of postoperative thirst. This study employs thirst as a diagnostic label, aiming to raise awareness among scholars about the high incidence of postoperative thirst and its significant impact on postoperative complications. The goal is to shift the focus towards solving the issue of postoperative thirst and devising relief strategies for high-risk patients.
However, this study has certain limitations. Firstly, the assessment of thirst primarily relies on patients’ subjective feelings without supplementation from relevant scales such as resting salivary flow rate, leading to a positive bias. Secondly, the lack of physiological data such as central venous pressure (CVP) and osmolarity may have affected the accuracy of the analysis. Thirdly, the study subjects were all from the same tertiary comprehensive hospital, lacking external validation. Future research should incorporate data from multiple centers to obtain a more representative sample, thus addressing the root cause to alleviate the degree of thirst and improve postoperative complications.
Conclusion
The occurrence rate of postoperative thirst after general anesthesia is high. Statistical analysis of the enrolled cases indicates that age, gender, history of coronary heart disease, preoperative fasting duration, and intraoperative fluid infusion volume are independent risk factors for postoperative thirst after general anesthesia.
Data availability
All data generated or analysed during this study are included in this published article.
References
Yang HL, Liu FC, Tsay PK, Chou AH, Lin CC, Yu HP, et al. Use of Transcutaneous Electrical Nerve Stimulation to Alleviate Thirst after surgery: a Randomized Controlled Trial. J Perianesthesia Nursing: Official J Am Soc PeriAnesthesia Nurses. 2023;38(2):291–6.
Lee CW, Liu ST, Cheng YJ, Chiu CT, Hsu YF, Chao A. Prevalence, risk factors, and optimized management of moderate-to-severe thirst in the post-anesthesia care unit. Sci Rep. 2020;10(1):16183.
Nascimento LA, Fonseca LF, Rosseto EG, Santos CB. [Development of a safety protocol for management thirst in the immediate postoperative period]. Volume 48. Revista da Escola de Enfermagem da U S P; 2014. pp. 834–43. 5.
Motta NH, do Nascimento LA, Pierotti I, Conchon MF, Fonseca LF. Evaluation of a Safety Protocol for the management of Thirst in the postoperative period. J Perianesthesia Nursing: Official J Am Soc PeriAnesthesia Nurses. 2020;35(2):193–7.
Kjeldsen CL, Hansen MS, Jensen K, Holm A, Haahr A, Dreyer P. Patients’ experience of thirst while being conscious and mechanically ventilated in the intensive care unit. Nurs Crit Care. 2018;23(2):75–81.
Puntillo KA, Arai S, Cohen NH, Gropper MA, Neuhaus J, Paul SM, et al. Symptoms experienced by intensive care unit patients at high risk of dying. Crit Care Med. 2010;38(11):2155–60.
Lin R, Chen H, Chen L, Lin X, He J, Li H. Effects of a spray-based oropharyngeal moisturising programme for patients following endotracheal extubation after cardiac surgery: a randomised, controlled three-arm trial. Int J Nurs Stud. 2022;130:104214.
Sato K, Okajima M, Taniguchi T. Association of persistent intense thirst with Delirium among critically ill patients: a cross-sectional study. J Pain Symptom Manag. 2019;57(6):1114–20.
Nascimento LAD, Garcia AKA, Conchon MF, Aroni P, Pierotti I, Martins PR, et al. Advances in the management of Perioperative patients’ Thirst. AORN J. 2020;111(2):165–79.
IFL. F IP. LF. F, PJEAN. A. Evaluación de la intensidad e incomodidad de la sed perioperatoria. 2018;22.
AP. R RPJS, N L. LFJRBE. F. Discomfort patients expect and experience in the immediate postoperative period. 2018;32:e26070.
Lin R, Li H, Chen L, He J. Prevalence of and risk factors for thirst in the intensive care unit: an observational study. J Clin Nurs. 2023;32(3–4):465–76.
Arai S, Stotts N, Puntillo K. Thirst in critically ill patients: from physiology to sensation. American journal of critical care: an official publication. Am Association Critical-Care Nurses. 2013;22(4):328–35.
Wu M, Yang L, Zeng X, Wang T, Jia A, Zuo Y, et al. Safety and feasibility of early oral hydration in the Postanesthesia Care Unit after laparoscopic cholecystectomy: a prospective, randomized, and controlled study. J Perianesthesia Nursing: Official J Am Soc PeriAnesthesia Nurses. 2019;34(2):425–30.
Chauvin C, Schalber-Geyer AS, Lefebvre F, Bopp C, Carrenard G, Marcoux L, et al. Early postoperative oral fluid intake in paediatric day case surgery influences the need for opioids and postoperative vomiting: a controlled randomized trial†. Br J Anaesth. 2017;118(3):407–14.
Sada F, Krasniqi A, Hamza A, Gecaj-Gashi A, Bicaj B, Kavaja F. A randomized trial of preoperative oral carbohydrates in abdominal surgery. BMC Anesthesiol. 2014;14:93.
Hirschfeld G, Zernikow B. Cut points for mild, moderate, and severe pain on the VAS for children and adolescents: what can be learned from 10 million ANOVAs? Pain. 2013;154(12):2626–32.
Oldenmenger WH, de Raaf PJ, de Klerk C, van der Rijt CC. Cut points on 0–10 numeric rating scales for symptoms included in the Edmonton Symptom Assessment Scale in cancer patients: a systematic review. J Pain Symptom Manag. 2013;45(6):1083–93.
Al-Robeye AM, Barnard AN, Bew S. Thirsty work: exploring children’s experiences of preoperative fasting. Paediatr Anaesth. 2020;30(1):43–9.
Stanhewicz AE, Kenney WL. Determinants of water and sodium intake and output. Nutr Rev. 2015;73(Suppl 2):73–82.
Qi L, Wu Y, Shan L, Dong Y, Mao G, Liang G, et al. A clinical study of preoperative carbohydrate administration to improve insulin resistance in patients with multiple injuries. Annals Palliat Med. 2020;9(5):3278–87.
Dilmen OK, Yentur E, Tunali Y, Balci H, Bahar M. Does preoperative oral carbohydrate treatment reduce the postoperative surgical stress response in lumbar disc surgery? Clin Neurol Neurosurg. 2017;153:82–6.
Fitzsimons JT. Drinking by rats depleted of body fluid without increase in osmotic pressure. J Physiol. 1961;159(2):297–309.
Zimmerman CA, Leib DE, Knight ZA. Neural circuits underlying thirst and fluid homeostasis. Nat Rev Neurosci. 2017;18(8):459–69.
Bentzer P, Griesdale DE, Boyd J, MacLean K, Sirounis D, Ayas NT. Will this hemodynamically unstable patient respond to a Bolus of Intravenous. Fluids? Jama. 2016;316(12):1298–309.
Chappell D, van der Linden P, Ripollés-Melchor J, James MFM. Safety and efficacy of tetrastarches in surgery and trauma: a systematic review and meta-analysis of randomised controlled trials. Br J Anaesth. 2021;127(4):556–68.
Chen X, Li K, Yang K, Hu J, Yang J, Feng J, et al. Effects of preoperative oral single-dose and double-dose carbohydrates on insulin resistance in patients undergoing gastrectomy:a prospective randomized controlled trial. Clin Nutr. 2021;40(4):1596–603.
Mortensen K, Nilsson M, Slim K, Schäfer M, Mariette C, Braga M, et al. Consensus guidelines for enhanced recovery after gastrectomy: enhanced recovery after surgery (ERAS®) Society recommendations. Br J Surg. 2014;101(10):1209–29.
Thanh NX, Chuck AW, Wasylak T, Lawrence J, Faris P, Ljungqvist O, et al. An economic evaluation of the enhanced recovery after surgery (ERAS) multisite implementation program for colorectal surgery in Alberta. Can J Surg J canadien de chirurgie. 2016;59(6):415–21.
Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. 2017;152(3):292–8.
Acknowledgements
None.
Funding
The study was financed from the National Natural Science Foundation of China (Beijing, People’s Republic of China), Grant No: 81471373, and the Foundation of Liaoning Province Education Administration (Liaoning, The People’s Government of Liaoning Province), Grant No: LJKZ0865, both grants awarded to Professor Dr. Zhaoyang Xiao.
Author information
Authors and Affiliations
Contributions
Zhihe Zeng and Xinge Lu carried out the studies, participated in collecting data, and drafted the manuscript. Zhihe Zeng and Ye Sun performed the statistical analysis and participated in its design. Ye Sun and Zhaoyang Xiao participated in acquisition, analysis, or interpretation of data and draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. This study was approved by the Ethics Committee of the Second Affiliated Hospital of Dalian Medical University (IRB 2021 − 113). Written informed consent was obtained from both patients and their families. The study was carried out in accordance with the applicable guidelines and regulations.
Consent for publication
Not Applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zeng, Z., Lu, X., Sun, Y. et al. Exploring thirst incidence and risk factors in patients undergoing general anesthesia after extubation based on ERAS principles: a cross sectional study. BMC Anesthesiol 24, 287 (2024). https://doi.org/10.1186/s12871-024-02676-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-024-02676-6