
Abstract
Background
Severe hyperlactatemia (lactate level ≥ 10 mmol/L) is associated with high mortality rates in critically ill patients. However, there is limited data on emergency department (ED) patients. We aimed to investigate the clinical characteristics, etiology and outcomes of patients with severe hyperlactatemia in the ED setting.
Methods
A retrospective cohort study was conducted at a tertiary care hospital in Thailand. We included adult patients with a venous lactate sample taken in the ED within one hour. We excluded patients after out-of-hospital cardiac arrest, transferred to/from another hospital or those with missing clinical data. Mortality rates were evaluated among patients with increasing degrees of lactate elevation and among patients with severe hyperlactatemia, stratified by causative etiology.
Results
We analyzed venous lactate levels in 40,047 patients, with 26,680 included in the analysis. Among these, 1.7% had severe hyperlactatemia (lactate ≥ 10 mmol/L), 10.5% moderate (4–9.99 mmol/L), 28.8% mild (2—3.99 mmol/L), and 59.0% normal levels (< 2 mmol/L). Severe hyperlactatemia was associated with high mortality rates of 29%, 37%, and 38% at 7, 28, and 60 days respectively, significant ICU admissions and mechanical ventilation rates. Patients with severe hyperlactatemia were stratified into high (> 50% mortality), moderate (21–50%), and low (< 20%) 28-day mortality risk groups. High-risk conditions included non-septic shock, traumatic injuries/burns, and neurological issues, with mortality rates of 51.1%, 61.8%, and 57.1%, respectively. In the moderate risk group, namely infection without shock showed a high prevalence, with a mortality rate of 36%. In the low-risk group, seizures and fainting were associated with lower mortality, exhibiting mortality rates of 0%.
Conclusions
Severe hyperlactatemia is associated with higher rates of ICU admission and mortality compared to other degrees of lactate elevation in a general ED population. However, mortality rates can vary considerably, depending on the underlying etiology associated with different primary diagnoses.
Similar content being viewed by others

Background
In the emergency department (ED), lactate measurement is commonly used as a diagnostic and prognostic tool, particularly for critically ill patients [1,2,3,4,5]. Typically, normal lactate levels are considered to be less than 2 mmol/L, with values above 2 mmol/L indicative of hyperlactatemia.5 Lactate pathophysiology is complex and varies amongst different clinical scenarios. In many disease states encountered in the ED hyperlactatemia results from a combination of increased production, due to global tissue hypoxia and/or catecholamine-stimulated aerobic glycolysis, and impaired clearance, secondary to hepatic dysfunction and/or alterations in pyruvate dehydrogenase activity [6]. Elevated lactate levels have been shown to be an independent predictor of mortality in specific subtypes (sepsis, trauma, etc.) and unselected critically ill ED and intensive care unit (ICU) patients [4, 7, 8].
While the clinical utility of lactate measurement in critically ill and injured patients is undoubted, there is a lack of consensus on the classification and significance of hyperlactatemia's severity in the literature. The most commonly used cutoff values for classifying the degree of lactate elevation are greater than 4 mmol/L for moderate and greater than or equal to 10 mmol/L for severe hyperlactatemia [9,10,11]. However, some studies use alternative discriminatory values such as lactate levels > 4 mmol/L to define severe hyperlactatemia [12]. More importantly, the relatively limited available research on the prognostic significance of lactate levels ≥ 10 mmol/L suggests a drastic mortality rate (65–75%), which has led some to conclude that further resuscitation of patients with this scenario may be futile [9, 13]. Given the paucity of data underlying this assumption, it has the potential to propagate a self-fulfilling, nihilistic approach that may not truly apply to all patients with severe hyperlactatemia. Consequently, further research is needed to more accurately characterize critically ill patients with severe hyperlactatemia (hereafter defined as ≥ 10 mmol/L). Several recent studies in the ICU setting have described the etiology and outcome of such patients, but there is limited data on ED patients with marked lactate elevation [9, 10, 13]. While these ICU reports described an extremely high overall mortality, they found significant variation in outcome depending on the precipitating etiology of hyperlactatemia. The aim of this study was to investigate the characteristics, etiologies, and outcomes of patients with severe hyperlactatemia in the ED setting.
Methods
Study design, setting and population
A retrospective cohort study was conducted at Srinagarind Hospital, a tertiary care facility with approximately 60,000 annual ED visits, affiliated with Khon Kaen University. All adult (≥ 18 years old) patients admitted to our ED between January 1, 2016 to December 31, 2021 who had a venous lactate sample collected within one hour of their ED presentation were eligible for the study. We excluded patients who had an out-of-hospital cardiac arrest (due to highly different pathophysiology), patients transferred into our ED, and patients initially seen in our ED and subsequently transferred to other hospitals. Venous lactate testing was performed based on the clinical judgment of the emergency department physicians, in the context of our hospital not having a standardized protocol for ordering lactate levels.
Ethics approval and consent to participate
The study protocol was approved by the Center for Ethics in Human Research, Khon Kaen University (HE651484). The need for informed consent to participate was waived by the Center for Ethics in Human Research, Khon Kaen University due to the retrospective nature of the study, in accordance with national regulations.
Data collection and management
Eligible patients for this study were identified from the ED database (Hospital Information System) using predefined inclusion criteria. To ensure data confidentiality, patient identifiers were encrypted or anonymized. Trained data collectors, who were not blinded to the study hypothesis, systematically extracted relevant information using standardized forms. Two authors (PP and TT) validated the data for completeness and accuracy, reviewing missing parameters or outlier data and obtaining additional information through comprehensive medical record review.
The collected data included clinical parameters and laboratory results. Clinical parameters encompassed demographic information, primary ED diagnosis, Charlson Comorbidity Index, triage level, initial hemodynamic parameters, treatments received in the ED, and patient outcomes, including 48-h mortality, 7-day mortality, 28-day mortality, 60-day mortality, in-hospital mortality, and ICU admission rate. If a clinical parameter remained missing, the patient was excluded from the cohort. Missing patient outcomes were further validated through linkage with national death registries, and patients were excluded if their outcomes remained missing after this validation.
Classification of hyperlactatemia etiology
After data collection, the primary ED diagnosis for each patient was identified. This diagnosis, coded using ICD-10 codes, was assigned by the ED physician based on the presumed diagnosis before ED discharge or admission. These diagnoses were then grouped into 17 clinically relevant categories, based on the most frequent nosological classes encountered in emergency medicine and previous studies [3, 14]. Details of the 17 categories of hyperlactatemia etiology, along with examples of diagnoses, are provided in the supplementary file.
Venous lactate measurement
Lactate samples were drawn by peripheral venipuncture by a nurse during the first hour in the ED. Following collection, the venous blood samples were sent to the chemistry laboratory via a Pneumatic Tube System. We used the Cobas®-8000 machine (Roche, Basel, Switzerland) for the laboratory analysis. If a patient had several venous lactate samples collected during their stay in the ED, only the first sample was included in the study.
Data analysis
Lactate level was classified into 4 groups: normal (< 2 mmol/L), mildly elevated (2–3.99 mmol/L), moderately elevated (4–9.99 mmol/L), and severe hyperlactatemia (lactate ≥ 10 mmol/L) based upon multiple review [3, 7, 9, 10]. The baseline characteristics and clinical data of the patients were presented as the median and interquartile range (IQR) for continuous variables, and as number and percentage for categorical variables. Amongst the four lactate severity classifications, continuous variables were compared using the Kruskal–Wallis rank-sum test and categorical variables were compared using Pearson's chi-square test or Fisher's exact test. We assessed the prognostic significance of escalating lactate elevation using Kaplan–Meier analysis of 60-day mortality. Survival distributions were compared using the log-rank test. We also classified 28-day mortality rates according to the etiology of hyperlactatemia and grouped patients into low, moderate, and high mortality risk groups using cut points of 20%, 50%, and > 50% mortality. The statistical analysis was performed using R Statistical Software version 4.2.2 (www.R-project.org, R Foundation for Statistical Computing).
Results
Patient characteristics
During the study period, 394,510 patients visited the ED. 40,047 patients obtained venous lactate results. Of those, 13,367 patients were excluded due to being transferred from other hospitals (5,420 patients), transferred to other hospitals (3,021 patients), age less than 18 years (4,291 patients), missing clinical data (296 patients), and out-of-hospital cardiac arrest (339 patients). A total of 26,680 patients were included in the analysis (Fig. 1).

Study flow
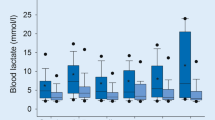
After categorizing the patients into four groups depending on lactate level, 15,735 patients had normal lactate level < 2 mmol/L, 7,680 patients had lactate 2—3.99 mmol/L, 2,799 patients had lactate 4 – 9.99 mmol/L, and 466 patients were having lactate ≥ 10 mmol/L. The patients' characteristics, including age, sex, comorbidities, hemodynamic parameters, and laboratory markers are displayed in Tables 1 and 2. Patients in the severe hyperlactatemia group exhibited a higher percentage of underlying liver disease (24%), an increased incidence of hypotension (17%), and a greater frequency of respiratory rates ≥ 22/min (80%). Additionally, these patients had a higher percentage of pulse rates > 100/min (43%), lower oxygen saturation, and more severe laboratory results, including serum creatinine and bicarbonate levels.
Outcomes and survival probabilities in patients with severe hyperlactatemia
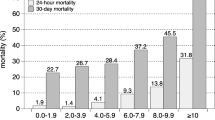
The overall mortality rates of patients with severe hyperlactatemia at 7 days, 28 days, and 60 days were 29%, 37%, and 38% respectively, as shown in Table 3. The death rate increased consistently with increasing degrees of initial hyperlactatemia. Additionally, a significant portion of the patients with severe hyperlactatemia required ICU admission (58%) or subsequent ICU transfer (67%), with a mechanical ventilation of 42%. Figure 2 shows the survival probabilities in the study cohort stratified by blood lactate levels. Individuals with lactate below 2 mmol/L had the highest 60-day survival rates, while those with levels of 10 mmol/L or above had the lowest. This observation indicates an association between elevated lactate levels and decreased survival rates.

Kaplan-Meier survival curve for lactate level categories
Etiology-based mortality risk in severe hyperlactatemia
The most common primary diagnosis among patients with severe hyperlactatemia was infection without shock, followed by non-septic shock and solid organ tumors. Additional primary diagnoses are detailed in Table 4. A wide range of mortality rates across different primary diagnoses was observed (0% for seizure – 66.7% for hematological malignancy). Patients with severe hyperlactatemia were further categorized into low, moderate, and high mortality risk groups, using cut points of 20%, 50%, and > 50% for 28-day mortality. In the high mortality risk group, the most prevalent primary diagnosis was non-septic shock, with a 28-day mortality rate of 51.1%. This was followed by traumatic injury/burns and neurological pathologies, with 28-day mortality rates of 61.8% and 57.1%, respectively. For the moderate mortality risk group, the most common conditions included infection without shock, solid organ tumor, and septic shock with corresponding 28-day mortality rates of 36.0%, 34.9%, and 46.2%. In contrast, the low mortality risk group predominantly comprised patients with seizures or fainting, toxicological causes, and renal disease. Notably, there were no recorded deaths in cases where lactate elevation was due to seizures or fainting.
Discussion
This is the first study to specifically highlight the clinical characteristics, etiology, and outcomes of severe hyperlactatemia in ED patients. Although lactate is widely recognized for its relevance in sepsis-related hyperlactatemia, our cohort study broadens its significance across a wider diagnostic spectrum in emergency medicine. We discovered that severe hyperlactatemia (lactate ≥ 10 mmol/L) was associated with significantly higher mortality compared to lesser lactate elevations (2–3.99 or 4–9.99 mmol/L). However, not all etiologies related to severe hyperlactatemia were associated with poor outcomes. This finding emphasizes the importance of rapid assessment and etiological evaluation of severe hyperlactatemia in critically ill patients.
The etiology and mortality rates of severe hyperlactatemia exhibit significant variation across different clinical settings. In previous study of surgical ICU patients, Spiegelberg et al. identified sepsis as the main etiology, accompanied by mesenteric ischemia and hemorrhagic shock, with an associated high mortality rate of 82.4%.8 Gharipour et al., analyzing critically ill patients in the MIMIC-III database, reported sepsis in 35.9% of severe hyperlactatemia cases, followed by cardiogenic shock and liver disease, with an overall ICU mortality rate of 65%.7 In the earliest study of severe hyperlactatemia, Haas et al. found the most common causes to be sepsis, cardiogenic shock, and cardiopulmonary resuscitation among a mixed ICU population. They reported that patients developing severe hyperlactatemia > 24 h after ICU admission or those without a 12-h lactate clearance < 33% exhibited 90% or greater ICU mortality [13].
In our study conducted in the context of the ED, we observed a notable contrast with a lower overall mortality rate of 37%. The most common etiologies identified were infection without shock, non-septic shock, and solid organ tumors. This disparity in overall mortality rates can be partly attributed to the broader spectrum of etiologies encountered in the ED setting. While patients in high-risk categories within our cohort exhibited significant mortality rates, those in lower-risk categories experienced substantially lower mortality rates. This variation in death rate across the patient groups culminated in an overall average mortality rate that was lower compared to the ICU population, which often comprises more uniformly high-risk cases and typically excludes milder cases by nature.
In this cohort, the highest 28-day mortality rate was observed in cases of hematologic malignancy, followed by traumatic/burns and neurological pathologies. The hyperlactatemia associated with malignancy is typically a result of Type B lactate overproduction, [15,16,17] driven by increased glucose consumption. Notably, the mortality rate we observed for hematologic malignancy aligns closely with the findings of Gharipour et al., who reported an ICU mortality rate of 71.4% for non-specific malignancies [9]. Similarly, for trauma patients, elevated blood lactate levels have been previously reported as a predictor of mortality in severe trauma cases [18].
The lowest rates of death among patients with severe hyperlactatemia occurred in the setting of tonic–clonic seizures, which are frequently encountered in ED. In this condition, lactate levels are a valuable diagnostic marker, particularly in cases of transient loss of consciousness [19]. Tonic–clonic seizures exhibit a wide range of lactate levels, from 0.5 to 17.4 mmol/L, with a median of 7.0 mmol/L [20]. Our study, which included 30 patients, found a notable incidence of seizures and accompanying severe hyperlactatemia. However, there were no fatalities among these patients.
Consistent with these data, we found that 46 patients with severe hyperlactatemia were discharged from the ED, most of whom survived at 60 days. Further analysis of their diagnoses revealed a variety of conditions, with the most common being in the lower-risk group, including seizure and fainting. The decision to discharge patients was based on multiple factors, including patient condition, preexisting medical comorbidities, and lactate clearance. This evidence indicates that severely elevated lactate levels do not necessarily predict a very poor outcome in all cases. Further studies should focus on lactate clearance and patient outcomes, particularly in low-risk groups.
Strengths and limitations
This study is based on a large dataset from a reliable electronic medical record system. Additionally, we excluded missing data to enhance data integrity. However, there were some limitations to this study. First, the retrospective nature of the study, confined to a single center, might limit its applicability to other clinical settings. Second, our analysis was based solely on initial lactate levels ordered by the treating clinicians in the ED. We have may missed patients with severe hyperlactatemia that was not clinically suspected by the treating team who did not order a venous lactate sample. Third, we did not monitor lactate levels over time or evaluate lactate clearance rates. Fourth, the determination of hyperlactatemia etiology was categorized into 17 categories based solely on the primary ED diagnosis, which may not fully reflect the complex and multifactorial nature of hyperlactatemia encountered in clinical practice. Finally, the novel etiology-based mortality risk grouping for severe hyperlactatemia used 28-day mortality for stratification. Variations in outcomes across different time frames may influence the categorization of risk groups.
Conclusions
Severe hyperlactatemia significantly correlates with high rates of ICU admission and mortality among ED patients with mortality rates varying significantly across various primary diagnoses. Patients with non-septic shock, trauma/burns, and neurological issues face the highest mortality risk. In contrast, those with renal diseases, toxicology, and seizures or fainting exhibit lower risk. Not all ED patients with lactate levels ≥ 10 mmol/l portend a grave prognosis. These patterns highlight the need for tailored resuscitation and management approaches in the ED, addressing the unique complexities of severe hyperlactatemia.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AIDS:
-
Acquired immunodeficiency syndrome
- CHF:
-
Congestive heart failure
- CKD:
-
Chronic kidney disease
- COPD:
-
Chronic obstructive pulmonary disease
- CVA:
-
Cerebrovascular accident
- ED:
-
Emergency department
- ICU:
-
Intensive care unit
- IQR:
-
Interquartile range
- MAP:
-
Mean arterial pressure
- TIA:
-
Transient ischemic attacks
- SBP:
-
Systolic blood pressure
- GCS:
-
Glasgow coma scale
References
van den Nouland DPA, Brouwers MCGJ, Stassen PM. Prognostic value of plasma lactate levels in a retrospective cohort presenting at a university hospital emergency department. BMJ Open. 2017;7(1):e011450.
Datta D, Walker C, Gray AJ, Graham C. Arterial lactate levels in an emergency department are associated with mortality: a prospective observational cohort study. Emerg Med J. 2015;32(9):673–7.
Pedersen M, Brandt VS, Holler JG, Lassen AT. Lactate level, aetiology and mortality of adult patients in an emergency department: a cohort study. Emerg Med J. 2015;32(9):678–84.
Chebl RB, Tamim H, Dagher GA, Sadat M, Enezi FA, Arabi YM. Serum Lactate as an Independent Predictor of In-Hospital Mortality in Intensive Care Patients. J Intensive Care Med. 2020;35(11):1257–64.
Kruse O, Grunnet N, Barfod C. Blood lactate as a predictor for in-hospital mortality in patients admitted acutely to hospital: a systematic review. Scand J Trauma Resusc Emerg Med. 2011;28(19):74.
Wardi G, Brice J, Correia M, Liu D, Self M, Tainter C. Demystifying Lactate in the Emergency Department. Ann Emerg Med. 2020;75(2):287–98.
Bou Chebl R, El Khuri C, Shami A, Rajha E, Faris N, Bachir R, et al. Serum lactate is an independent predictor of hospital mortality in critically ill patients in the emergency department: a retrospective study. Scand J Trauma Resusc Emerg Med. 2017;25(1):69.
Del Portal DA, Shofer F, Mikkelsen ME, Dorsey PJ Jr, Gaieski DF, Goyal M, et al. Emergency Department Lactate Is Associated with Mortality in Older Adults Admitted With and Without Infections. Acad Emerg Med. 2010;17(3):260–8.
Gharipour A, Razavi R, Gharipour M, Modarres R, Nezafati P, Mirkheshti N. The incidence and outcome of severe hyperlactatemia in critically ill patients. Intern Emerg Med. 2021;16(1):115–23.
Spiegelberg J, Lederer AK, Claus S, Runkel M, Utzolino S, Fichtner-Feigl S, et al. Severe hyperlactatemia in unselected surgical patients: retrospective analysis of prognostic outcome factors. BMC Surg. 2022;22(1):312.
Ferreruela M, Raurich JM, Ayestarán I, Llompart-Pou JA. Hyperlactatemia in ICU patients: Incidence, causes and associated mortality. J Crit Care. 2017;42:200–5.
Tuhay G, Pein MC, Masevicius FD, Kutscherauer DO, Dubin A. Severe hyperlactatemia with normal base excess: a quantitative analysis using conventional and Stewart approaches. Crit Care. 2008;12(3):R66.
Haas SA, Lange T, Saugel B, Petzoldt M, Fuhrmann V, Metschke M, et al. Severe hyperlactatemia, lactate clearance and mortality in unselected critically ill patients. Intensive Care Med. 2016;42(2):202–10.
Contenti J, Occelli C, Lemoel F, Ferrari P, Levraut J. Blood lactate measurement within the emergency department: A two-year retrospective analysis. Am J Emerg Med. 2019;37(3):401–6.
Yi HK, Yoo J, Kim SJ, Choi JY, Lee KH. Lymphoma total lesion glycolysis leads to hyperlactatemia and reduction of brain glucose utilization. Sci Rep. 2022;25(12):12639.
Wang C, Lv Z, Zhang Y. Type B lactic acidosis associated with diffuse large B-cell lymphoma and the Warburg effect. J Int Med Res. 2022;50(1):03000605211067749.
Sillos EM, Shenep JL, Burghen GA, Pui CH, Behm FG, Sandlund JT. Lactic acidosis: a metabolic complication of hematologic malignancies: case report and review of the literature. Cancer. 2001;92(9):2237–46.
Okello M, Makobore P, Wangoda R, Upoki A, Galukande M. Serum lactate as a predictor of early outcomes among trauma patients in Uganda. Int J Emerg Med. 2014;7(1):20
Matz O, Zdebik C, Zechbauer S, Bündgens L, Litmathe J, Willmes K, et al. Lactate as a diagnostic marker in transient loss of consciousness. Seizure. 2016;1(40):71–5.
Magnusson C, Herlitz J, Höglind R, Wennberg P, Edelvik Tranberg A, Axelsson C, et al. Prehospital lactate levels in blood as a seizure biomarker: A multi-center observational study. Epilepsia. 2021;62(2):408–15.
Acknowledgements
The authors would like to thank the physicians and nurses at the Srinagarind Hospital accident and emergency department and Khon Kaen University Faculty of Medicine’s Department of Emergency Medicine for their support.
Funding
This study was funded by the Khon Kaen University Faculty of Medicine in Thailand (Grant Number MN66001).
Author information
Authors and Affiliations
Contributions
TT conceived the study, designed the trial, managed the data, analyzed the results, and drafted the manuscript. BD contributed to the conceptualization and drafting of the manuscript. RD also played a key role in conceiving the study, managing the data, and drafting the manuscript. Both PK and KD were involved in drafting the manuscript. PP was instrumental in obtaining research funding and assumes full responsibility for the paper. All authors contributed significantly to the revision of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Human Research Ethics Committee of Khon Kaen University (HE651484). Informed consent has been waived by the approving ethics committee due to the retrospective nature of the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tangpaisarn, T., Drumheller, B.C., Daungjunchot, R. et al. Severe hyperlactatemia in the emergency department: clinical characteristics, etiology and mortality. BMC Emerg Med 24, 150 (2024). https://doi.org/10.1186/s12873-024-01071-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12873-024-01071-1