
Abstract
Background
The latent tuberculosis infection (LTBI) burden is still unclear in schoolchildren and adolescents in China. Previous study and daily surveillance data indicate a LTBI detection gap. The research objective was to evaluate the LTBI burden and detection gap among schoolchildren and adolescents in China.
Methods
A cross-sectional study was conducted among 69,667 schoolchildren and adolescents in Chongqing, China between September 2022 and December 2023 implemented by Chongqing Municipal Institute of Tuberculosis using tuberculin skin test (TST) and creation tuberculin skin test (C-TST). To evaluate the LTBI detection gap, the pulmonary tuberculosis (PTB) screening data implemented by Chongqing Municipal Institute of Tuberculosis have been compared with the data in 2021 implemented by community-level medical and health care institutions.
Results
The LTBI prevalence rate using TST and C-TST implemented by Chongqing Municipal Institute of Tuberculosis was 12.8% (95%CI, 12.5-13%) and 6.4% (95%CI, 6-6.8%) respectively. The LTBI prevalence rate by Chongqing Municipal Institute of Tuberculosis was 9.6% higher than that by community-level medical and health care institutions (χ2 = 2931.9, P < 0.001).
Conclusions
The LTBI detection gap existed among schoolchildren and adolescents in Chongqing, and it also may exist in other similar countries and regions. National screening strategy needs improvement. Regular training and quality assurance could improve the performance of TST and C-TST and close the detection gap of LTBI.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Tuberculosis (TB) is the major cause of death in children and adolescents in infectious diseases worldwide. Children and adolescents with LTBI are a large reservoir for active TB, and proactive intervention of LTBI is a key part of the WHO End TB Strategy [1].
The cumulative number of children treated between 2018 and 2021 was 1.9 million, which was 54% of the five-year target of 3.5 million set at the UN high level meeting in 2018, and preventive treatment target has only been achieved by 42% [2]. LTBI is defined as a state of being infected with Mycobacterium TB without clinical evidence of active TB [3]. Sufficient detection of LTBI is the basis of TB prevention and control, especially for schoolchildren and adolescents.
China is one of the 30 high TB burden countries, and has the third largest numbers of cases accounting for 7.1% of the global total [2]. The LTBI burden is still unclear in schoolchildren and adolescents in China. Three national tuberculosis prevalence surveys done in 1990, 2000, and 2010 excluded children under 14 years [4]. A study has been conducted to estimate the LTBI burden in China in 2021, and the prevalence of LTBI in people five years old and above was 18.1% [5], but the study did not provide complete LTBI burden in schoolchildren and adolescents.
PTB is a type of TB that affects the lungs of the human body, and it is a contagious disease transmitted through the air. In China, PTB screening in schoolchildren and adolescents is widely carried out at schools. The majority of PTB screening are carried out by community-level medical and health care institutions, which have not received regular standardized training and quality control. This issue has not received adequate attention in provincial tuberculosis prevention and control policies. It was also found that there may be a LTBI detection gap from daily surveillance system and previous investigation. The LTBI burden and detection gap among schoolchildren and adolescents needs comprehensive investigations.
Methods
Study design
This was a cross-sectional study using stratified cluster random sampling, which was conducted among schoolchildren and adolescents in Chongqing, China between September 2022 and December 2023 by Chongqing Municipal Institute of Tuberculosis. A standardized quality control system for active PTB screening was developed. On this basis, we evaluated the LTBI burden and detection gap among schoolchildren and adolescents.
According to the local policy of Chongqing, Junior One, Senior One and Senior Two students should be screened for active PTB. The participants were tested using TST or novel skin tests for tuberculosis infection (TBST). TST remains the most widely used tool at a global scale. According to China national diagnostic criteria for TB [6], the results of TST are divided into four levels: negative(the induration average diameter < 5 mm), generally positive(5 mm ≤ the induration average diameter < 10 mm), moderately positive(10 mm ≤ the induration average diameter < 15 mm), and strongly positive(the induration average diameter ≥ 15 mm). Bacillus Calmette-Guérin (BCG) vaccination at birth is a national policy in China, and coverage has been at a high level, which might interfere with TST reactivity. Considering this, the TST induration cut-off point of ≥ 15 mm was used to indicate TB infection in school [7, 8].
C-TST is a type of TBST, which uses a new type of recombinant fusion protein that only contains Mycobacterium TB early secretory antigen target six (STAT-6) and culture filtrate protein ten (CFP10), and exposure to previous BCG vaccine will not interfere with the C-TST reactivity. The C-TST induration or erythema cut-off point of ≥ 5 mm has been commonly recommended for TB infection. TST or C-TST has been selected according to the wishes of local health department and schools. C-TST was approved for TB infection diagnosis in China in April 2020 by China National Medical Products Administration, and recommended in August 2020 by Chinese Anti-Tuberculosis Association.
The LTBI prevalence rate was the proportion of participants who are TST strongly positive or C-TST positive after excluding active TB.
The annual risk of tuberculous infection (ARTI) was evaluated [9] (appendix p 6).
Sample size
According to the the previous PTB screening investigation in schoolchildren and adolescents by Chongqing Municipal Institute of Tuberculosis, the LTBI prevalence rate is about 15%. The sample size was estimated at 13,401 schoolchildren and adolescents using the following formula, based on the expected LTBI prevalence rate of 15%, the allowable error of 1%, and the significance level of 5%.
Since the current TB notification rate in schoolchildren and adolescents in Chongqing is not high, which was about 15 cases per 100,000 population according to national TB surveillance system, we have assumed that the TB infection within the sampled schools was in a natural state, without the occurrence of severe clustered outbreaks that would lead to a significant increase in LTBI prevalence rate. The expected intra-cluster correlation coefficient should be close to 0. The average cluster size was about 1000, based on the local school conditions.
Considering the situation mentioned above, and given that the intra-cluster correlation coefficient should be close to 0, it would not have a significant impact on the sample size.
Randomisation and cluster selection
This study used stratified cluster random sampling. According to the division of local government, there were four regions in Chongqing including: the Central Urban Districts, New West Urban Development Districts, Northeast Districts and Southeast Districts. These regions were different in terms of socioeconomic development. Clusters were defined as middle schools located in the four districts. Each cluster had at least 500 participants registered between September 2022 and December 2023.
Study participants
The inclusion criteria were as follows: (1) participants in school at least ten years old, and (2) participants who can participate in the entire PTB screening process. The exclusion criteria were as follows: (1) participants with allergic constitution, (2) participants with acute infectious diseases or other diseases judged by doctors that TST or C-TST can not be performed, (3) participants who have been vaccinated in the last month, (4) previous TB, and (5) TST or C-TST has been implemented in the last three months.
Participants with allergic constitutions were excluded because they may be at risk of severe allergic reactions, including anaphylactic shock, due to the administration of TST or C-TST. Participants vaccinated in the last month were excluded because injecting any vaccine in the last month may interfere with the results of TST and C-TST.
According to the inclusion and exclusion criteria, participants were continuously selected from the selected clusters until they were fully enrolled.
Procedures
Standardized training was provided for all medical workers involved in this study, including public health and clinical theory, as well as TST and C-TST practical skill. The trainees were assessed, and only those who pass the assessment can implement PTB screening.
For each enrolled participant, socio-demographic information was collected, including age, gender and educational level.
PTB screening mainly includes a consultation on close contact history with PTB patients and suspicious symptoms of PTB, a TST test/C-TST test, and a chest X-ray examination.
TST and C-TST were performed according to the Mantoux technique. When performing TST (Purified Protein Derivative of Tuberculin; Xiang Rui, China or Chengdu Institute of Biology, China), 0.1 mL (5IU) purified protein derivative of tuberculin was injected on the volar surface of the left forearm intradermally. The induration was measured in millimeter after 72 h at injection sites.
When performing C-TST (Recombinant Mycobacterium Tuberculosis Fusion Protein; Zhifei Longcom Biologic Pharmacy Company, Anhui, China), 0.1 mL (5U) recombinant mycobacterium TB fusion protein was injected on the volar surface of the left forearm intradermally. The induration or erythema was measured in millimeter after 48 h at injection sites.
Digital chest radiography was performed on each participant with suspected symptoms of PTB, who was TST strong positive or C-TST positive, and who met the exclusion criteria of study participants mentioned earlier in study participants section. Those with abnormal digital chest radiography went to designated medical institutions for further examination.
The LTBI detection gap
To evaluate LTBI detection gap, we collected PTB screening data implemented by community-level medical and health care institutions in the same schools selected in this study in 2021, which have been compared with the data implemented by Chongqing Municipal Institute of Tuberculosis between September 2022 and December 2023.
The data of 2021 came from national TB surveillance system. Due to the limitations of national TB surveillance system, it was not possible to make an assessment of participants who did not participate in TST. PTB screening in 2021 has not excluded the students who undergone TST within the last three months and those who had previous TB. It has also not excluded the students who was TST positive previously.
Statistical analysis
We calculated the proportion and 95% CI for the LTBI prevalence rate, which was the proportion of schoolchildren and adolescents with LTBI excluding active PTB. Different LTBI prevalence rates were tested using chi-square test. The trend of rate was tested using chi-square test for linear trend. Some participants were unable to verify the TST or C-TST results due to leave or other reasons, resulting in missing data. To evaluate the impact of missing data, we compared the distribution of gender, grade, region and school type between participants with and without the TST or C-TST results by chi-square test. A two-sided P < 0.05 was taken as statistically significant. Statistical analyses were performed with the SPSS 22.0 software (SPSS, Inc., Chicago, IL, USA).
Results
The screening process for participants
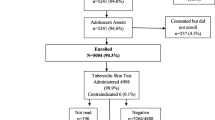
There were 69,667 participants in 51 schools in Chongqing between September 2022 and December 2023, and 4786 (6.9%) were excluded for various reasons leaving 64,881 (93.1%) participants with TST or C-TST result (Fig. 1).

Flow chart of participants screened for LTBI between September 2022 and December 2023 in Chongqing. *PTB Pulmonary Tuberculosis; TB Tuberculosis; TST Tuberculin Skin Test; C-TST Creation Tuberculin Skin Test; LTBI Latent Tuberculosis Infection
There are 41 schools using TST (48583 participants with results), and ten schools using C-TST (16298 participants with results). Participants who were unable to verify the TST or C-TST results due to leave or other reasons were excluded from statistical analysis considering that these missing data were completely random and had a low proportion of 0.4% (279/65160). In addition, there was no difference in the distribution of gender, grade, region and school type between participants with and without the TST or C-TST results (appendix p 2).
PTB screening results
The LTBI prevalence rate using TST and C-TST was 12.8% (95%CI, 12.5-13%) and 6.4% (95%CI, 6-6.8%) respectively (Tables 1 and 2). The LTBI prevalence rate using TST was significantly higher than that using C-TST (χ2 = 492.7, P < 0.001).
The detection rate of active PTB in participants using TST was 32.9 cases per 100,000 population (16/48583), and the detection rate of active PTB in participants using C-TST was 67.5 cases per 100,000 population (11/16298). There was not a significant difference in detection rate of active PTB in participants using TST or C-TST (χ2 = 3.5, P = 0.06).
The TST strongly positive rate has increased significantly from 8.3% in Junior One to 15% in Senior Two (χ2 trend = 223.6, P < 0.001) .The C-TST positive rate has also increased significantly from 4.9% in Junior One to 7% in Senior Two (χ2 trend = 8.6, P = 0.003) .
The LTBI detection gap
There were 47,320 participants with TST result in the same schools of this study in 2021. The LTBI prevalence rate using TST by community-level medical and health care institutions was 3.2% (95%CI, 3.1-3.4%) in 2021 (Table 3).
The LTBI prevalence rate using TST by Chongqing Municipal Institute of Tuberculosis was 9.6% higher than that by community-level medical and health care institutions (χ2 = 2931.9, P < 0.001), and there were also similar trends in LTBI prevalence rate in each subgroup (Fig. 2). The risk factors associated with LTBI were analyzed, and the LTBI prevalence rate in Southeast Districts by Chongqing Municipal Institute of Tuberculosis was the highest (appendix p 3). The LTBI detection gap in Southeast Districts was also the greatest, reaching 15.5%.

The LTBI detection gap of schoolchildren and adolescents using TST in Chongqing. *TST Tuberculin Skin Test; LTBI Latent Tuberculosis Infection
The ARTI of schoolchildren and adolescents
The ARTI using TST and C-TST was 0.9% (95%CI, 0.8-1%) and 0.4% (95%CI, 0.3-0.5%) respectively (appendix p 6).
Discussion
One key challenge in TB prevention and control is to accurately find students infected with TB among schoolchildren and adolescents. Through this study, we have obtained accurate LTBI burden among them in Chongqing.
In this study, the LTBI prevalence rate conducted by Chongqing Municipal Institute of Tuberculosis using TST between September 2022 and December 2023 was 9.6% higher than the results conducted by community-level medical and health care institutions in the same schools in 2021. The quality of PTB screening implemented by community-level medical and health care institutions may be poor. The reduction of the reported number of TST strong positive schoolchildren and adolescents has significantly decreased the detection of active PTB and LTBI, which may result in more community transmission. According to Statistical Bulletin on National Economic and Social Development in Chongqing of 2021, the total number of middle school students in Chongqing was 1.77 million, which may mean a LTBI detection gap of 0.17 million middle school students who were not detected and intervened timely in Chongqing.
This detection gap may not happen only in Chongqing. A study found that the TST strong positive rate was 2.69% among 16,795 freshmen in senior high schools and boarding junior high schools in 2019 in Ningbo, Zhejiang Province, China [10], and the TST strong positive rate was 1.45% among 78,102 freshmen in the same population of the same area in 2021 [11]. The PTB screening among 220,269 freshmen in senior high schools and boarding junior high schools showed that the TST strong positive rate was 1.70% from 2016 to 2020 in Liuzhou, Guangxi Province, China [12]. The TST strong positive rate was 0.36% among 20,153 students in Longgang District, Shenzhen, China in 2021 [13]. Two studies in Beijing showed that the TST strong positive rate was 2.59% among 6187 freshmen in 2018, and 1.86% among 12,562 freshmen in 2020 respectively [14, 15]. The TST strong positive rates in these studies were lower than our results, which may be due to the lower PTB burden in these regions or the existence of a LTBI detection gap. The reported incidence rate of active PTB was about 48 cases per 100,000 population in Chongqing, which currently ranks 13th among all provinces in 2023 in China according to national TB surveillance system, and the reported PTB incidence rate of the above provinces was about 23–68 cases per 100,000 population. It was unreasonable to explain such a low TST strong positive rate using the reason that the PTB burden in these regions was far lower than that in Chongqing.
Our study conducted standardized training for medical workers. During the training process, it was found that the reasons for this detection gap may include non-standard TST administration and inaccurate TST result reading, and inaccurate TST reading may have the greatest impact on this detection gap, which may be due to the reader’s incorrect understanding of the operation rules and rusty practical skills.
Research on TST quality control is rare. A study has noticed the limitations of TST quality, which included reader variability and the need for trained personnel to read the results [16]. A study has found that TST reading results vary very much between readers [17]. Although a large number of schoolchildren and adolescents underwent TST every year, the TST quality might be seriously underestimated. With the development of information technology, intelligent software for TST or TBST result reading may also be developed to improve the accuracy. Regular training and quality assurance are needed to establish, and maintaining proficiency is equally important. A study has found that mhealth approach using smartphone may be a method that could serve as a TST training and quality control tool in many settings [18].
This study used two skin test methods, TST and C-TST. However, C-TST was approved for TB diagnosis in China in 2020, and has not been widely used in China. This study obtained the LTBI prevalence rate using C-TST, and the C-TST positive rate was lower than the TST strong positive rate. BCG vaccination might have accounted for a considerable proportion of positive TST [19]. A study using C-TST showed that the positive rate was 10.14% (14/157) in 2022 in a high school in southeast of Chongqing [20]. YANG Zhen et al. [21] have found that C-TST positive rate was 9.1% among 1924 college students in 2022 in Beijing, China. MU Tingmei et al. [22] showed that C-TST positive rate was 0.97% among 7416 junior middle school students and 1.1% among 2555 high school students respectively in 2021 in Yaan City, Sichuan Province, China. There were still differences in the C-TST positive rates conducted in different regions, and there was also a possibility of LTBI detection gap.
The TST strongly positive rate and C-TST positive rate has increased significantly from Junior One to Senior Two in Chongqing. Other studies have also shown that the TST positive rate has increased with age in schoolchildren and adolescents [10,11,12, 14]. Most provinces of China do not implement PTB screening for Senior Two in high school, and it is important to add a PTB screening in Senior Two, so as to prevent students from being unable to participate in the college entrance examination because of PTB.
In 2022, the reported PTB incidence rate of schoolchildren and adolescents aged 10–19 of Chongqing was 23.77 cases per 100,000 population per year according to the national TB surveillance system, which was less than the actual incidence rate. In this study, the overall prevalence of LTBI using TST was 12.8% (95% CI, 12.5-13%) with a corresponding ARTI of 0.9% (95% CI, 0.8-1%). If we assume 5% rapid progression from recent infection to active TB [23], and 0.05% annual progression rate from remote infection to active TB [24], incidence rate can be measured: 0.9%×5%+12.8%×0.05%=51.4 cases per 100,000 population per year [9]. According to a study in Chongqing in 2021, the PTB screening proportion of freshmen in middle school is only 42.4%, indicating that there were still some PTB patients who have not been found in time [25]. Under these assumptions, the ARTI obtained in this study using TST may reflect the current situation.
Using the same method, estimated incidence rate using C-TST was 23.2 cases per 100,000 population per year. The estimated incidence rate using C-TST may be underestimated using the Styblo’s rule [23, 26]. Considering the universal vaccination of BCG in China and the lower false positive rate of C-TST, the progression rate should be higher than 5% in LTBI using C-TST [26].
This study has limitations. There were no schools in Northeast Districts that conducted C-TST. The PTB screening in schoolchildren and adolescents has not been systematically implemented before 2022, resulting in the data from routine surveillance system were limited. Lack of gender and some information in routine surveillance system before 2022 made it impossible to conduct related analysis.
This study obtained accurate LTBI burden using TST and C-TST in schoolchildren and adolescents in Chongqing, China. The LTBI detection gap existed among schoolchildren and adolescents in Chongqing, and it also may exist in other similar countries and regions, which may lead to more TB infections and morbidity. This situation must attract high attention from decision-makers. The staff of community-level medical and health care institutions need to receive regular standardized training and quality control to maintain the skill proficiency. These measures should be included in national tuberculosis prevention and control policies. Intelligent software for the result reading of TST and TBST should be developed, along with the development of mhealth systems capable of conducting quality control, which could help to enhance the PTB screening capabilities in areas with limited medical resources.
In conclusion, obtaining accurate LTBI burden in schoolchildren and adolescents is crucial to develop effective TB prevention and control policies. Taking necessary measures could significantly improve the quality of TST and TBST, and close the detection gap of LTBI.
Data availability
The PTB screening data of this study has been stored in the the provincial TB surveillance system but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the corresponding author upon reasonable request and with permission of the provincial TB surveillance system.
Abbreviations
- WHO:
-
World Health Organization
- LTBI:
-
Latent Tuberculosis Infection
- TST:
-
Tuberculin Skin Test
- C-TST:
-
Creation Tuberculin Skin Test
- TB:
-
Tuberculosis
- PTB:
-
Pulmonary Tuberculosis
- TBST:
-
Novel Skin Tests for Tuberculosis Infection
- BCG:
-
Bacillus Calmette-Guérin
- STAT-6:
-
Secretory Antigen Target Six
- CFP10:
-
Culture Filtrate Protein Ten
- ARTI:
-
The Annual Risk of Tuberculous Infection
References
Uplekar M, Weil D, Lonnroth K, Jaramillo E, Lienhardt C, Dias HM, et al. WHO’s new end TB strategy. Lancet. 2015;385(9979):1799–801.
World Health Oragnization. Global tuberculosis report 2023. Geneva, Switzerland: World Health Organization. 2023. https://www.who.int/publications/i/item/9789240083851. Accessed March 10, 2024.
World Health Organization. Latent tuberculosis infection: updated and consolidated guidelines for programmatic management. Geneva, Switzerland: World Health Organization. 2018. https://www.who.int/publications/i/item/9789241550239. Accessed March 10, 2024.
Wang L, Zhang H, Ruan YZ, Chin DP, Xia Y, Cheng S, et al. Tuberculosis prevalence in China, 1990–2010; a longitudinal analysis of national survey data. Lancet. 2014;383(9934):2057–64.
Gao L, Zhang H, Hu MG, Xu CD, Xia YY, Li T, et al. Estimation of the national burden on latent tuberculosis infection based a multi-center epidemiological survey and the space statistics model. Chin J Antituberculosis. 2022;2022(01):54–9.
National Health Commission of the People’s Republic of China. Diagnosis for pulmonary tuberculosis. Beijing, China: National Health Commission of the People’s Republic of China; 2017.
National Health Commission of the People’s Republic of China. Technical specifications for Tuberculosis Prevention and Control in China (2020 Edition). Beijing, China: National Health Commission of the People’s Republic of China; 2020.
National Health Commission of the People’s Republic of China, Ministry of Education of the People’s Republic of China. Guidelines for Tuberculosis Prevention and Control in Chinese Schools. (2020 Edition). Beijing, China: National Health Commission of the People’s Republic of China, Ministry of Education of the People’s Republic of China; 2020.
David WD, Marcel AB. Are we underestimating the annual risk of infection with Mycobacterium tuberculosis in high-burden settings? Lancet Infect Dis. 2022;22(9):e271–8.
Chen T, He TF, Yu M, Che Y, Lin X. Analysis on tuberculin skin test results in 16795 freshmen in Ningbo, Zhejiang. Disease Surveillance. 2023;38(9):1043–7.
Lin X, Yu M, He TF, Che Y, Lin L, Cheng T. Tuberculin skin test results among new middle and high school students in Ningbo in 2021. Chin Prev Med. 2023;02:135–8.
Huang BY, Wei GL. Tuberculosis screening among freshmen and incidence of tuberculosis among students in Liuzhou from 2016 to 2020. Chin Youjiang Med J. 2020;10:790–3.
Li ML, Liu JY, Zhang XQ, Qiu YH, Huang DH, Zheng TH. Analysis of tuberculosis health examination results in schools in Longgang District, Shenzhen in 2021. J Med Pest Control. 2023;05:465–9.
Ma CX, Xu W, Liang YR, Liang RY, Zhang XZ, Wang M. Tuberculosis screening results among new students in Chaoyang district of Beijing in 2020. Disease Surveillance. 2022;37(7):949–53.
Meng WL, Li SY, Wang FH, Li HY, Lang Y, Guo JL, et al. Tuberculosis screening results of freshmen in 138 primary and secondary schools. China Trop Med. 2019;19(8):781–3.
Gina G, Paola M, Francesco NL, Fabrizio P, Sayoki M, Peter M. Tuberculin skin test-outdated or still useful for latent TB infection screening? Int J Infect Dis. 2019;80S:S20–2.
Keiko N, Kiminori S, Yuko S, Akimitsu S, Hidetoshi I, Keiichi N. Problems about tuberculin skin test raised from consultations and countermeasures–influence to the interpretation of tuberculin skin test in case of the stoppage of BCG revaccination abolition and the introduction of induration measurement. Kekkaku. 2002;77(10):639–45.
Saeedeh MN, Leila B, Olivia O, Chantal V, Mei-Xin L, Jonathon RC. The mTST-An mHealth approach for training and quality assurance of tuberculin skin test administration and reading. PLoS ONE. 2019;14(4):e0215240. https://doi.org/10.1371/journal.pone.0215240.
Ben JM. Mycobacterium tuberculosis infection burden in poor urban communities. Lancet Child Adolesc Health. 2018;2(1):7–8.
Su Q, Wang QY, Zhang T, Liu Y. Comparison of recombinant Mycobacterium tuberculosis fusion protein skin test and tuberculin skin test for screening latent tuberculosis infection in school students. Chin J Infect Control. 2023;22(5):547–51.
Yang Z, Sun Q, Han L, Bao C, Wang X, Zhang ZG. Analysis of recombinant mycobacterium tuberculosis fusion protein in screening for latent tuberculosis infection in college students. Chin J Front Med Sci. 2022;14(07):51–4.
Mu TM, Hu QY, Li W, Feng Y, Wang XG. Analysis of recombinant mycobacterium tuberculosis fusion protein in screening for latent tuberculosis infection in college students. Parasitoses Infect Dis. 2022;3:166–70.
Styblo K. The relationship between the risk of tuberculous infection and the risk of developing infectious tuberculosis. Bull Int Union Tuberc Lung Dis. 1985;60:117–9.
Horsburgh CJ, O’Donnell M, Chamblee S, Moreland JL, Johnson J, Marsh BJ, et al. Revisiting rates of reactivation tuberculosis: a population-based approach. Am J Respir Crit Care Med. 2010;182:420–5.
Pang Y, Wu CG, Wang QY, Zhang T. Screening results of tuberculosis among new students in Chongqing Municipality, 2021. Practical Prev Med. 2023;30(02):165–8.
Dye C. Breaking a law: tuberculosis disobeys Styblo’s rule. Bull World Health Organ. 2008;86:4.
Acknowledgements
We thank the field workers and the study nurses Jinshan Qian, Jia Luo, Xianhui Feng, Xuemei Feng, Jin Wu, Yanping Feng, Cuimei Yue, Shanshan Liu, Huli Pan, and Yanjun Feng.
Funding
The data collection and data analysis of the study was supported by Chongqing Science and Health Joint Research Project (2023ZDXM027 and 2023MSXM143), Chongqing Health Commission Medical Science Research Project (2024WSJK08), and Chongqing Public Health Key Specialties (Disciplines) Construction Fund.
Author information
Authors and Affiliations
Contributions
JF, JYZ, BW, and YY designed the study. CGW, YLS, YL, JY, QS, ZZ, XH, and MW were involved in conducting the study. BW, YY, JY, QS and YP were involved in data analysis. BW and YY wrote the draft manuscript. BW, YY, JY, and QS had access to and verified the existence of the raw data. All authors read and approved the final manuscript before submission. JF was responsible for the decision to submit the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethics committee of Chongqing Municipal Institute of Tuberculosis (202202, 26 September 2022). As we were carrying out a data analysis based on mandatory physical examinations and all individual information was removed before analysis, the need for informed consent to participate was waived by the ethics committee of Chongqing Municipal Institute of Tuberculosis.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wu, B., Yu, Y., Wu, C. et al. Addressing the burden and detection gap of latent tuberculosis infection in schoolchildren and adolescents in China: a cross-sectional study. BMC Infect Dis 24, 984 (2024). https://doi.org/10.1186/s12879-024-09812-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09812-0