
Abstract
Background
Although a universal vaccine is available and Ethiopia is working outstandingly towards measles elimination, a recurrent measles outbreak has occurred each year in different parts of the country. Therefore, understanding the epidemiology of measles cases, the incidence of confirmed measles virus cases and related risk factors is crucial. Here, we conducted a systematic review and meta-analysis to summarize information regarding the epidemiology, measles incidence rate and risk factors for national measles infections occurring in the past two decades, from 2000 to 2023.
Methods
Data from electronic databases, including PubMed, African Journal Online, WHO databases and Google Scholars, were searched to identify studies describing measles outbreaks, incidence rates and associated factors in Ethiopia that occurred between 2000 and 2023. Important basic information was extracted in an Excel spreadsheet and imported into Comprehensive Meta-analysis Software version 3 to evaluate the associations between measles outbreaks and different risk factors. We pooled the odds ratios (ORs) and 95% confidence intervals (CIs) for every included risk factor to evaluate the associations with measles outbreaks.
Results
We included 36 studies involving 132,502 patients with confirmed measles cases in Ethiopia. The results of this systematic review and meta-analysis revealed that measles outbreaks were more frequently reported in the Oromia region (73,310 (33.1%)), followed by the Southern Nation Nationalities of Ethiopia region (29,057 (13.4%)). The overall pooled analysis indicated that the prevalence of measles susceptibility was 67.5% (95% CI: 67.3–67.8%), with an I2 of 99.86% and a p value for heterogeneity < 0.0001. The non-vaccinated status of the children, their contact history with measles cases, their travel history, the presence of cases in family or neighbors, and malnourished patients were identified as factors associated with the high prevalence and recurrent measles infections in Ethiopia.
Conclusion
The results of this systematic review and meta-analysis indicated that the pooled prevalence of measles infection was high, which is a public health concern in Ethiopia. Thus, strengthening healthcare services, regular vaccination campaigns, and the integration of health education activities with other services may decrease the incidence rate.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Measles is a highly contagious disease caused by the measles virus. The measles virus is an enveloped, single-stranded, negative-sense RNA virus that belongs to a member of the genus Morbillivirus in the family Paramyxoviridae [1]. The virus genome consists of six genes that encode eight viral proteins (six structural and two nonstructural proteins). The six structural proteins are the hemagglutinin (H) protein, fusion protein (F), nucleocapsid protein, phosphoprotein, matrix protein, and large protein [2]. These structural proteins, particularly the H and F proteins, are responsible for the interaction of the virus with the host cell and the fusion of the viral envelope with the plasma membrane to initiate infection [3]. After human-to-human contact via respiratory droplets, more than 90% of susceptible individuals may develop systemic infections such as fever, malaise, cough, rhinitis, conjunctivitis, and Koplik’s spots, followed by maculopapular rash [4, 5].
Prior to the introduction of the measles vaccine in 1963, this viral disease caused more than 2 million deaths and 15,000–60,000 cases of blindness worldwide [6]. Owing to its high mortality and morbidity rates, in 2001, the American Red Cross, CDC, UNICEF, and WHO launched the Measles and Rubella Initiative (MRI), with the goal of reducing measles mortality by 90% in 2010 compared with the 2000 baseline [7]. These vaccination efforts resulted in a 79% reduction in global measles deaths, from 535,000 in 2000 to 139,300 in 2010 [8]. In 2011, members of the WHO Regional Office for Africa adopted a decision to eliminate measles by 2020. Member countries developed a measles elimination strategic plan to achieve the following goals by 2020: achieve and maintain measles incidence below 1 case per million population; achieve and maintain > 95% MCV1 coverage at the national and regional levels in all regions; maintain at least ≥ 95% SIA coverage; and incorporate the second dose of measles into the routine vaccination schedule [9].
Ethiopia is a strong supporter of membership in the WHO African Regional Office and advocates for a national measles strategic plan to control and ultimately eliminate measles by 2020 [10]. The country also launched a nationwide measles catch-up campaign (SIA) in 2009 and initiated field epidemiology and laboratory training programs [11, 12]. In February 2019, Ethiopia incorporated the second dose of the measles vaccine (MCV2) into its routine vaccination schedule. However, despite these efforts, national plans to accelerate measles control by 2012 (< 5 cases per 1 million people per year) and eliminate measles by 2020 (< 1 case per 100,000 people per year) have not yet been achieved [13]. Nevertheless, measles is endemic in Ethiopia, and the annual rate of measles incidence has increased significantly. Currently, there is a high rate of measles incidence, with more than 50 cases per 1,000,000 people reported annually [14]. Ethiopia remains the 4th-leading country in the world in terms of the burden of measles cases and is experiencing an ongoing measles outbreak, with more than 6933 measles confirmed cases in 2023 [15, 16].
Although the characteristics of measles infection have been well described, previous studies have focused mainly on descriptions of single measles outbreaks, and few studies have summarized the measles immunization situation in Ethiopia. In those studies, attention has been given to summarizing measles outbreaks, incidence, and risk factors. Therefore, we conducted a systematic review and meta-analysis to summarize information regarding the outbreaks, epidemiology, incidence and risk factors for measles infection in Ethiopia from 2000 to 2023.
Methods and materials
Search strategies
Both published articles and unpublished reports were searched for primary studies through electronic databases, including PubMed, Scopus, African Journal Online, WHO, and Google Scholar, to identify studies describing measles outbreaks, incidence rates and associated factors in Ethiopia that occurred between 2000 and 2023 (Fig. 1). The selection of search terms was conducted in population, intervention, comparison, and outcome (PICO) format [17]. For the population search term “Ethiopia”, for the intervention search term “Measles risk factor”, the search terms used for comparison and outcome were “no measles” and “measles” or “measles” and “no measles”. These terms were searched individually in each database and then combined using “OR” and “AND”. We registered our protocol with the Prospero International Register of Systematic Reviews (http://www.crd.york.ac.uk/PROSPERO/) 23/11/2023 (CRD42023482250). The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist [18] was utilized to present the findings of the epidemiology of measles outbreaks, incidence and associated factors in Ethiopia.
Inclusion and exclusion criteria
Articles that reported measles epidemiology, incidence, and associated risk factors that occurred in Ethiopia were eligible for this systematic review and meta-analysis. The search was limited to articles published between January 1, 2000, and May 1, 2023. Quantitative studies with sufficient basic information (measles outbreak location and epidemiological investigation about the outbreak) and a clear diagnosis of measles were included, irrespective of whether the study was implemented in a health facility and/or in the community. The exclusion criteria were as follows: research articles describing measles outbreaks outside of Ethiopia; reports or studies that lacked key information or were not related to the aim of this study; and measles outbreaks that occurred before January 1, 2000.
Data extraction
The relevant studies were identified and merged after duplicate studies were removed via EndNote X7. The data extraction format was applied by considering all the inclusion criteria to check consistency and ensure that all the pertinent information was addressed. The format includes author name, year of publication, year of measles outbreak, country, region, study design, study period, study setting, sample size, and risk factors for measles outbreak, including the number of patients (measles cases) and controls (non-measles cases). The three reviewers (DE, WT & BT) independently assessed the articles and extracted the information from each included study according to the predefined set of inclusion criteria. Any data discrepancy among the data reviewers was resolved by referring to the original study through discussion with fourth and fifth reviewers.
Data quality assessment and risk of bias
The qualities of the data or the selected articles were assessed according to the Joanna Brigg’s Institute (JBI) critical appraisal checklist, which contains 9 checklist items [18]. On the basis of the 9 points of the JBI checklist, the three authors (DE, WT & BT) assessed the overall methodological quality and evaluated the quality of the articles as low quality (< 5 out of 9), moderate quality (5–7), or high quality (> 7) (additional file 1). The assessments revealed that more than 90% of the eligible articles included in this systematic review and meta-analysis were high-quality, and these data were compiled into a standard table (Table 1).
Data synthesis
Both descriptive and statistical data synthesis approaches were used to present the findings of this systematic review and meta-analysis. A summary table was prepared to explain the characteristics of the included articles. We described the epidemiology of measles, its incidence and associated risk factors. We performed a statistical meta-analysis for the thirty-six included articles after organizing the data on an Excel spreadsheet and imported it to Comprehensive Meta-analysis Software version 3 to evaluate the associations between measles outbreaks and different risk factors. We pooled the odds ratios (ORs) and 95% confidence intervals (CIs) for every included risk factor to evaluate the associations with measles outbreaks. We assessed the level of heterogeneity across studies via both random effects and fixed effects models, reporting heterogeneity and overall p values. An I2 value greater than 50% indicated high heterogeneity between studies; therefore, a random effects model was implemented.
Operational definition
A measles outbreak
is the occurrence of five or more reported suspected cases of measles in one month per 100 000 people living in a geographical area.
Measles-confirmed cases
suspected measles cases that were reported from the surveillance system and confirmed by laboratory serological tests.
An epidemiologically linked case
refers to a suspected case that has been linked (in person, place, and time) to a laboratory-confirmed case.
Non-measles infected case
was defined as any notified case or suspected case that was measles-specific IgM negative after testing as per established laboratory protocols.
Measle incidence
The measles incidence was calculated by dividing measles-confirmed cases by the population of the year and then multiplying by one million to compute the measles incidence per million people for a single-year period or multiple-year period.
Results
Study selection
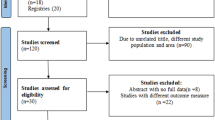
Among the 354 records identified, 211 were screened after the removal of records duplicated in more than one electronic database, and 79 records were excluded because of an unrelated title and country. Following this, 57 records were excluded because they were abstracts only, letters to editors, poster papers, or guidelines, and 39 full records or articles were excluded because of the study period and incomplete information. Finally, 36 records or articles that met the critical appraisal checklists were included in this systematic review and meta-analysis, regardless of their study design (Fig. 1).

PRISMA (flow chart of study selection for epidemiology of measles outbreaks, incidence and associated factors in Ethiopia from 2000 to 2023: a systematic review and meta-analysis)
Epidemiology of measles cases in Ethiopia
Among all the selected studies, 227,250 suspected and 149,415 (65.75%) confirmed measles cases were reported from 2000 to 2023. Among these measles-confirmed cases, 62,521 (27.51%) were laboratory-confirmed (IgM + ve), 48,887 (21.51%) were epidemiologically linked, and 38,007 (16.72%) were clinically compatible. The Oromia region is one of the most affected regions, contributing approximately 90,610 (73.42%), followed by the Southern Nation Nationalities of Ethiopia region, which accounts for more than 29,057 (70.06%) measles-confirmed cases of the overall specified regions (Table 2).
The overall pooled prevalence of measles-confirmed cases was 67.6% (95% CI: 67.3–67.8%), with an I2 of 99.86% and a p value for heterogeneity < 0.0001 (Table 3). This meta-analysis also described a subgroup analysis of the pooled prevalence of the different administrative regions of Ethiopia. The largest pooled prevalence of measles confirmed cases occurred in the Oromia region, with 72.9% (95% CI: 72.7–73.2%), followed by the Southern Nation Nationalities of Ethiopia region, with 69.3% (95% CI: 68.8–69.7%), and the Afar region, with 68.9% (66.6–71.2%). In a comparison of measles susceptibility based on investigation modalities, the prevalence of measles investigated by survey and by health facilities was 69.4% (95% CI = 69.2–69.6%; I2 = 99.78%; P < 0.0001) and 5.9% (95% CI = 5.6–6.3%; I2 = 99.82%; P < 0.0001), respectively (Table 3).
Measles incidence rate
The incidence rate of measles in Ethiopia has significantly varied between 2005 and 2023. A noticeable increase in the incidence rate started in 2008, with 42.4 cases per million people, and reached its peak in 2015, with 173.2 cases per million people. Although the incidence rate declined between 2016 and 2020, there was a surge in 2022, indicating that the incidence rate is fluctuating and not consistently declining (Fig. 2). This suggests that measures to control the disease have not been consistently effective.

Incidence rate of measles in Ethiopia (Epidemiology of measles outbreaks, incidence and associated factors in Ethiopia from 2000–2023: a systematic review and meta-analysis)
Factors associated with measles outbreaks
In our systematic review and meta-analysis, none vaccinated patients, having a contact history with measles patients, a non-educated mother, travel history to the measles site, a distance greater than 2 km from health facilities, the presence of cases in a family or neighbor, a non-ventilated house, and malnourished patients were statistically associated with measles outbreaks. However, poor knowledge of measles transmission, living in a room by more than five people, and previous measles infections were not statistically associated with measles outbreaks (Fig. 3).

Factors associated with measles cases in Ethiopia (Epidemiology of measles outbreaks, incidence and associated factors in Ethiopia from 2000–2023: a systematic review and meta-analysis)
The significant risk factors from a number of studies revealed that none vaccinated patients were 2.6 times more likely to have measles infections than were the vaccinated patients (2.63; 1.992–3.477), and a history of contact with measles patients made them nearly 3 times more likely to have measles infections (2.94; 2.198–3.928). Patients from illiterate mothers were 1.4 times more likely to have measles infections (1.38; 1.004–1.907), whereas patients with a travel history to the measles area were 1.7 times more likely to have measles infections (1.7; 1.209–2.341). On the other hand, the presence of cases in a family or neighbor makes them 2.2 times more likely to have measles infections, and taking two or more than two vaccine doses decreases the odds of contracting measles by 61% compared with those who do not take two or more vaccines (Table 4).
Discussion
This systematic review and meta-analysis focused on describing the magnitude of the measles outbreak and identifying the risk factors for measles infection in Ethiopia. This study presents the epidemiology, incidence rate, and risk factors for measles outbreaks that occurred in the past two decades between 2000 and 2023.
The overall pooled prevalence of measles-confirmed cases among all regions was 67.6% (95% CI: 67.3–67.8%); however, a difference in the pooled prevalence of measles-confirmed cases was observed among the regions in our study. The Oromia region was the most affected region, with 72.9% (95% CI: 72.7–73.2%), followed by the Southern Nation Nationalities of Ethiopia region, with 69.3% (95% CI: 68.8–69.7%), and the Afar region, with 68.9% (66.6–71.2%). The disparity may be due to differences in early detection and confirmation of measles epidemics among regions, and the highest pooled prevalence may be due to the large susceptible population, which may contribute to the spread of the virus.
The measles incidence is high and has remained above 15 cases per million populations for the past twenty years. This reveals that the country is not on the right track to attain the measles elimination goal of less than 1 case per million people by 2020 [50]. According to the present study, the highest measles incidence rate (173.2 per 1,000,000 people) occurred in 2015, and the lowest measles incidence rate (15.8 per 1,000,000 people) occurred in 2018. The variation in incidence rates from year to year could be due to differences in measles outbreak duration, low routine measles vaccine coverage, poor living and nutritional conditions, measles susceptibility accumulation, or differences in clusters of non-immune individuals [51].
Our meta-analysis revealed that the non-vaccinated status of children, contact history with measles patients, travel history to measles endemic site, the presence of measles cases in family/neighbors and malnourished patients were statistically significant risk factors for the continued high incidence rate of measles in Ethiopia. Among those risk factors, the overall pooled prevalence of non-vaccinated children in our study was 2.63 (95% CI: 1.992–3.477). Thus, the likelihood of acquiring measles infection was approximately 2.6 times greater in unvaccinated patients than in vaccinated patients. This result is in line with studies conducted in Zimbabwe (3 times) [52] and Ethiopia (5 times) [53]. This may be due to the perceptions of societies about the importance of vaccines. These factors result in low vaccination coverage and inadequate herd immunity in the community.
The pooled estimate of patients who had a history of contact with measles patients revealed a 2.9-fold greater risk of developing measles infection than did those who had no known contact history. This finding is consistent with studies performed in Japan, mainland China and Taiwan in China [54]. This is because the measles virus is highly contagious and is transmitted either by direct or indirect contact with infected patients’ respiratory droplets, which increases the spread of the virus from person to person.
In many low-income countries, including Ethiopia, malnutrition is a great challenge and leads to increased susceptibility to infectious diseases [55]. In this study, the odds of acquiring measles infection in malnourished children were 5.99 times greater among children who were not malnourished (5.99; 95% CI 3.112–11.53). The findings of this meta-analysis are in line with those of a study conducted in Yemen [56]. The association between measles and malnutrition has been described, in that malnourished children are more likely to contract the measles virus than are well-nourished children. In temperate regions, virus transmission peaks in late winter and early spring and follows the rainy season in tropical regions [57]. However, in this study, knowledge about measles transmission was not statistically associated with measles outbreaks.
Conclusion
Although; considerable improvement was practiced to eliminate Measles in Ethiopia, the outbreaks is continue to occur in many parts of the country and becomes a cause of significant number of death. In this study, the pooled prevalence of measles infection was high (67.6%), which is a public health concern in Ethiopia. The Oromia region was the most affected region, followed by the Southern Nation Nationalities of Ethiopia region and the Afar region. The result of our study also shows a significant association in terms non-vaccinated status of the children, having a history of contact with measles cases, travel history, the presence of cases in families/neighbors and malnourished patients. Those risk factors were identified as factors associated with the high prevalence and recurrent measles infections in the country.
Thus, major efforts will be needed to strengthening healthcare services, regular vaccination campaigns, and the integration of health education activities with other services to reduce measles incidence rate.
Limitations
Our study had several limitations. First, since our systematic review and meta-analysis were based on reported or published papers, some measles outbreaks may not have been recorded. Therefore, the actual number of measles cases associated with these outbreaks was possibly greater than recorded. Second, measles is self-limiting, and most infections are asymptomatic; thus, some measles patients may become unidentified during measles outbreaks. Despite these limitations, we believe that our systematic review and meta-analysis provide useful information regarding the national epidemiology of measles outbreaks, incidence and important risk factors.
Data availability
The authors confirm that all relevant data were included in the manuscript and that we do not have any research data outside the submitted manuscript file.
Abbreviations
- CDC:
-
Centers for Disease Control
- CI:
-
Confidence interval
- F-protein:
-
Fusion protein
- H-protein:
-
Hemagglutinin protein
- MRI:
-
Measles and Rubella Initiative
- MCV:
-
Measles vaccine
- MV:
-
Measles virus
- RNA:
-
Ribonucleic acid
- WHO:
-
World health origination
References
Laksono BM, de Vries RD, McQuaid S, Duprex WP, de Swart RL. Measles virus host invasion and pathogenesis. Viruses. (2016) 8:210. doi: https://doi.org/10.3390/v8080210
Leung AK, Hon KL, Leong KF, Sergi CM: Measles: a disease often forgotten but not gone. Hong Kong Med J. 2018, 24:512–520. https://doi.org/10.12809/hkmj187470
Griffin DE. Measles virus-induced suppression of immune responses. Immunol Rev 2010; 236:176 − 89.
de Vries RD, Duprex WP, de Swart RL. Morbilli virus infections: an introduction. Viruses. (2015) 7:699–706. doi: https://doi.org/10.3390/v7020699
World Health Organization. Global vaccine-preventable diseases standards measles guide line. 2018:1–30.
World Health Organization Global Measles and Rubella Strategic plan: 2012-20, Geneva.,http://www.who.int/immunization/newsroom/Measles Rubella Strategic Plan 2012 2020. pdf.; 2012.
Measles Rubella Initiative Accessed 17 October 2016.
World Health Organization, Surveillance Guidelines for Measles, Rubella and Congenital Rubella Syndrome in the WHO European Region. Copenhagen, December 2012.
Nshimirimana D, Roungou JB. The Effort to Attain Measles Preelimination Targets by 2012 and to Eliminate Measles In the African Region by 2020. Brazzaville, Republic of Congo: WHO African Regional Office, 2010. Accessed 24 November 2016
Federal Ministry of Health. Measles elimination strategic plan, Ethiopia, 2012–2020. October 2012, Addis Ababa.
Goodson JL, Masresha BG, Wannemuehler K, Uzicanin A, Cochi S. Changing Epidemiology of Measles in Africa. Journal of Infectious Diseases. 2011;204 (suppl 1):S205-S14.
Desta TK, Lemango ET, Wayess JD, Masresha BG. Measles Epidemiology in Ethiopia from 2006–2016: Predictors of High Measles Incidence from Surveillance Data Analysis. J Immunol Sci (2018); S (018): 122–129
World Health Organization. Global Health Observatory (GHO) data > measles-containing vaccine first dose (MCV1) immunization coverage among 1-year-olds. 2017.
WHO. WHO-GAVI Joint Statement: Ethiopia Launches Measles Vaccine’s Second Dose on 11th February 2019. Addis Ababa, Ethiopia; 2012. [Google Scholar]
CDC. Outbreak investigation [Available from: https://www.cdc.gov/csels/dsepd/ss1978/lesson6/Sect.2.html.
WHO Ethiopia World Health Organization. Measles - Ethiopia 4 May 2023.
Pollock, A. and Berge, E. How to do a Systematic Review. International Journal of Stroke. 2018; 13(2), pp.138–156.
Institute J. The Joanna Briggs Institute Critical Appraisal Tools for Use in JBI Systematic Reviews Checklist for Analytical Cross-Sectional Studies. The Joanna Briggs Institute North Adelaide, Australia; 2017
Hassen MN, Woyessa AB, Getahun M, Beyene B, Buluanger L, Ademe A, Bekele A, Addissie A, Kebede A. and Jima D. Epidemiology of measles in the metropolitan setting, Addis Ababa, Ethiopia, 2005–2014: a retrospective descriptive surveillance data analysis. BMC Infectious Diseases (2018) 18:400 https://doi.org/10.1186/s12879-018-3305-4
Duressa TE., Worku A. and Boulanger L. Ethiopia Field Epidemiology Training Program (EFETP) Compiled Body of Works in Field EpidemiologyAddis Ababa: Ethiopia; 2015.
Beyene BB., G/Selassie GG., Tegegne AA., Wayessa DJ., and Enqueselassie F. National measles surveillance data analysis, 2005 to 2009, Ethiopia Journal of Public Health and Epidemiology Vol. 8(3), pp. 27–37, March 2016 DOI: 10.5897/JPHE2015.0711 Article Number: D3AB 33657063 ISSN 2141–2316
Biru M, Geleta T., Assefa E, Alayu M., Tayachew A, and Wossen M. Analysis of measles case-based surveillance data in Afar Regional State, Ethiopia, from 2013 to 2017African Journal of Health Sciences and Technology. Vol. 4(1), pp. 1–8, September 2022 DOI: 10.5897/ AJHST 2022.0016 Article Number: C7C410A69674 ISSN 2805–4202
Wolde Melese Ayele. Malnutrition Precipitated Measles Outbreak in Gewane District, Afar Regional State, Northeastern Ethiopia, 2016 Research square DOI: https://doi.org/10.21203/rs.3.rs-32423/v1
Andualem T., Awoke S., Getnet S., Sied Y., Melese A. and Genet Ch. Measles outbreak investigation in Basso Liben District, Amhara Region, Ethiopia 2017. Journal of Infectious Diseases and Immunity. Vol. 13(1) pp. 1–6, January-June 2021 DOI: 10.5897/JIDI2017.0171 Article Number: 147478465746 ISSN: 2141–2375
Girmay A. and Dadi AF. Being unvaccinated and having a contact history increased the risk of measles infection during an outbreak: a finding from measles outbreak investigation in rural district of EthiopiaBMC Infectious Diseases (2019) 19:345 https://doi.org/10.1186/s12879-019-3973-8
Tariku MK. and Misikir SW. Measles outbreak investigation in Artuma Fursi Woreda, Oromia Zone, Amhara Region, Ethiopia, 2018: a case control study BMC Res Notes (2019) 12:765 https://doi.org/10.1186/s13104-019-4806-y
Mer’Awi A, Tesfaye T. Measles outbreak in Simada District, South Gondar Zone, Amhara Region, May - June 2009: Immediate need for strengthened routine and supplemental immunization activities (SIAs). Ethiop J Health Dev. 2012;26(2):115–118
Getahun M., Beyene B., Ademe A., Teshome B, Tefera M., Asha A, Afework A., HaileMariyam Y., Assefa E. and Gallagher K Epidemiology of laboratory confirmed measles virus cases in Amhara Regional State of Ethiopia, 2004–2014 BMC Infectious Diseases (2016) 16:133. DOI: https://doi.org/10.1186/s12879-016-1457-7
Ayalew A., Enquoselassie F and Workineh A. Ethiopia Field Epidemiology Training Program (EFETP) Compiled Body of Works in Field EpidemiologyAddis Ababa: Ethiopia; 2015.
Tsegaye G., Gezahegn Y, Tesfaye A, Mulatu G, Bulcha GG., Berhanu N. Measles Outbreak Investigation in Guradamole District of Bale Zone, South Eastern Ethiopia, 2021. Infection and Drug Resistance 2022:15https://doi.org/10.2147/IDR.S343270
Tsegaye G., Gezahagn Y., Bedada Sh., Berhanu N., Gudina G., Mulatu G. Epidemiology of Measles in Bale Zone, Southeast Ethiopia: Analysis of Surveillance Data from 2013 to 2019. Infection and Drug Resistance 2022:15 669–683 https://doi.org/10.2147/IDR.S343270
Belda K., Tegegne AA., Mersha AM., Bayenessagne MG., Hussein I., Bezabeh B. Measles outbreak investigation in Guji zone of Oromia Region, Ethiopia. The Pan African Medical Journal. 2017;27 (Supp 2):9. DOI: 10.11604/pamj. supp. 2017.27. 2. 10705
Kalil1 FS., Gemeda DH., Bedaso MH., Wario SK. Measles outbreak investigation in Ginnir district of Bale zone, Oromia region, Southeast Ethiopia, May 2019. Pan African Medical Journal (ISSN: 1937–8688). Volume 36, Article 20, 14 May 2020 |. https://doi.org/10.11604/pamj.2020.36.20.21169
Milkessa Mebrate M., Hailu Ch. and Alemu S. Measles outbreak investigation in Kasoshekumer kebele, Sinana district, SouthEastern Oromia, Ethiopia: A case–control study. SAGE Open Medicine Volume 11: 1–11 DOI: https://doi.org/10.1177/20503121231169182
Geatchew Abichu. Investigation of Measles Outbreak in Mieso District, Oromia Regional State, Eastern Ethiopia, December 2018GSJ: Volume 10, Issue 6, June 2022, Online: ISSN 2320–9186 www.globalscientificjournal.com
Kaba Babure Z, Fikadu Tufa A, Mohammed Ahmed Y. A Retrospective Assessment of Measles Outbreak Response Activities and Determinant Factors at Nunukumba District, East Wollega Zone, Oromia Regional State, Western Ethiopia, May 2020. Int J Pediatr 2021; 9(6): 13781-801. DOI: https://doi.org/10.22038/IJP.2020.49135.3935
Yitbarek K, Tilahun T, Debela T, Abdena D, Girma T. Measles epidemiology and vaccination coverage in Oromia Region, Ethiopia: Evidence from surveillance, 2011–2018. Vaccine 39 (2021) 4351–4358. https://doi.org/10.1016/j.vaccine.2021.06.015
Mulugeta Asefa Gutu et al. Epidemiology of measles in Oromia region, Ethiopia, 2007–2016. Pan African Medical Journal. 2020;37(171). https://doi.org/10.11604/pamj.2020.37.171.23543
Poletti1P, Parlamento S, Fayyisaa T, Feyyiss R, Lusiani M, Tsegaye A, Segafredo G, Putoto G, Manenti F. and Merler S. The hidden burden of measles in Ethiopia: how distance to hospital shapes the disease mortality rate. BMC Medicine (2018) 16:177. https://doi.org/10.1186/s12916-018-1171-y
Kassahun Mitiku, Wendemagegn Kegne. Measles outbreak investigation in west Hararghie zone of Oromia region, Ethiopia, 2007. VOL 7 NO 7 (2011): Ethiopia journal of pediatrics and child health.
Bukuno S, Asholie A, Girma Z, Haji Y. Measles Outbreak Investigation in Garda Marta District, Southwestern Ethiopia, 2022: Community-Based Case-Control Study Infection and Drug Resistance 2023:16 2681–2694
Fekede W/Kidan, Dawit Getachew, Besufekad Mekonnen & Workineh Woldeselassie Hammeso (2021) Risk Factors of Measles Outbreak Among Students of MizanTepi University, Tepi Campus, Southwest Ethiopia, Infection and Drug Resistance,, 963–970, DOI: https://doi.org/10.2147/IDR.S296928
A.B. Woyessa, A.A. Said. Measles outbreak investigation - Keffa zone, SNNP regional state, Ethiopia, January 2012 DOI: https://doi.org/10.1016/j.ijid.2012.05.461
Getahun M, Beyene B, Ademe A, Teshome B, Tefera M, Afework A, HaileMariam Y, Assefa E, Hailegiorgis Y. and Asha A. Epidemiology of laboratory confirmed measles virus cases in the southern nations of Ethiopia, 2007–2014. BMC Infectious Diseases (2017) 17:87 DOI: https://doi.org/10.1186/s12879-017-2183-5
Degefa G.,&, Gebremeriam K., Juru T., Jackson R. Magnitude and Trends of Measles in North West of Tigray Region, Ethiopia - A Four-year Surveillance Data Analysis, 2012–2015. J Interval Epidemiol Public Health. 2019 March; 2(1):2 https://doi.org/10.37432/JIEPH.2019.2.1.13
Mohammed A.D, Bizuneh H, Assefa Z, (2022). Measles Case-Based Surveillance Data Analysis Report in Tigray Region, From September 2013 to August 2017, J Nur Healthcare, 7(4), 01–07.
Yusuf Mohammed and Ayalew Niguse. Measles Outbreak Investigation and Response in Jarar Zone of Ethiopian Somali Regional State, Eastern Ethiopia. International Journal of Microbiological Research 8 (3): 86–91, 2017 ISSN 2079–2093 DOI: 10.5829/ idosi. ijmr. 2017. 86.91
Abibakar Sheikaden Ismail, Mowlid Akil Aden, Abdiaziz Abdulahi Abdikarim, and Abdikaid Ahmed Yusuf, “Risk Factors for Measles Outbreak: An Unmatched Case Control Study in Kabridahar District, Somali Regional State, Ethiopia.” American Journal of Epidemiology and Infectious Disease, vol. 7, no.1 (2019): 1–5. doi: https://doi.org/10.12691/ajeid-7-1-1.
Abdisalam. Ali, Mohammed A. Maalin. The risk factors of measles outbreak in Dollo zone Somali region, Ethiopia. International Journal of Community Medicine and Public Health Int J Community Med Public Health. 2021 Nov;8(11):5179–5183 http://www.ijcmph.com pISSN 2394–6032 | eISSN 2394–6040. DOI: https://dx.doi.org/10.18203/2394-6040ijcmph20214246
World Health Organization. Global Measles and Rubella strategic plan 2012–2020. 2012 Switzerland.
Tariku et al. BMC Infectious Diseases (2023) 23:756. https://doi.org/10.1186/s12879-023-08757-0
Pomerai KW, Mudyiradima RF, Gombe NT. Measles outbreak investigation in Zaka, Masvingo province, Zimbabwe, 2010. BMC Res Notes. 2012;5 (1):1–6. doi: https://doi.org/10.1186/1756-0500-5-687
EPHTI Hailu D, Alano A, G/Mariam A, Abicho T. Measles; for the Ethiopian health center team; 2005. Ethiopia public health training initiative, the carter center, the Ethiopia ministry of health, and the Ethiopia ministry of education. Available from: https://www.cartercenter.org/resources/pdfs/health/ephti/library/modules/degree/modmeasles_final.pdf. Accessed May 12, 2022
Shimizu K, Kinoshita R, Yoshii K, Akhmetzhanov AR, Jung S, Lee H, et al. An investigation of a Measles outbreak in Japan and China, Taiwan, China, March-May 2018. Western Pacific surveillance and response journal.WPSAR. 2018;9(3):25–31.
Schaible UE, Kaufmann SH. Malnutrition and infection: complex mechanisms and global impacts. PLoS Med. 2007;4(5):e115. doi: https://doi.org/10.1371/journal.pmed.0040115
Nassar AAH, Al Amad MA, Qasim M, Dureab F. Risk factors for measles outbreak in Ataq and Habban districts, Shabwah governorate, Yemen, February to May 2018. BMC Infect Dis. 2021;21(1):551. doi: https://doi.org/10.1186/s12879-021-06207-3
World Health Organization. Measles and rubella regional progress updates. 2015.
Acknowledgements
We would like to acknowledge the Authors of each article included in this manuscript. We would also like to thank JBI for using their systemic review and meta-analysis guidance.
Funding
There was no funding or sponsoring organization for this study.
Author information
Authors and Affiliations
Contributions
DE, WT and BT. conceived, designed the study and led the protocol design, study design, the data acquisition and data extraction. DE. conducted the statistical analysis and wrote the draft. GB. and AM. critically revised and modify the manuscript for important intellectual content. All the authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Eshetu, D., Tosisa, W., Regassa, B.T. et al. Epidemiology of measles outbreaks, incidence and associated risk factors in Ethiopia from 2000 to 2023: a systematic review and meta-analysis. BMC Infect Dis 24, 914 (2024). https://doi.org/10.1186/s12879-024-09828-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09828-6