
Abstract
Background
In older individuals, the role of low serum uric acid (SUA) as risk factor for mortality is debated. We therefore studied whether SUA levels, particularly low SUA concentrations, are associated with all-cause and cardiovascular (CV) mortality in older population, and to clarify potential effect modification of kidney function.
Methods
We identified 14,005 older people in National Health and Nutrition Examination Survey (NHANES) data from 1999 to 2018. SUA was measured only at baseline. The relationship between SUA and mortality was assessed using Cox proportional hazards models and restricted cubic spline Cox regression stratified by the estimated glomerular filtration rate (eGFR).
Results
During mean 8.3 years of follow-up, 4852 all-cause death and 1602 CV death were recorded. A significant U-shaped association was observed between SUA with all-cause mortality, with the lowest risk concentration of 5.5 mg/dL. Comparing to the reference group (5 to 7 mg/dL), the HR of 2 to < 5 mg/dL group was 1.11 (1.03–1.21) and 1.14 (1.00–1.30). This relationship was more pronounced in participants with an eGFR ≥ 60 ml/min/1.73m2 (HR, 1.16; 95%CI, 1.06—1.28). This situation similarly occurred in Urine protein negative group (HR, 1.14; 95%CI, 1.04—1.25).
Conclusions
Low SUA concentrations are associated with an increased risk in all-cause and CV mortality among older participants. Extremely low SUA concentrations are especially undesirable, especially in the older adults with normal kidney function.
Similar content being viewed by others

Introduction
With population ageing, the health problem of the older people is more prominent. Cardiovascular (CV) disease is the leading cause of death in older people and increases exponentially with age. Exploring modifiable risk factors can help promote health and longevity in older adults.
Serum uric acid (SUA) has gained increasing attention as a CV risk factor [1]. A wealth of researches have focused on an elevated SUA level with higher risk of death from any causes and CV disease in adults [2, 3], while the relationship of low SUA in older people are inconclusive [4, 5]. Recently, there is some evidence suggesting a link between low uric acid levels and poor survival outcomes in elderly individuals [6], more research is needed to fully evaluate this relationship.
The prevalence of Chronic kidney disease (CKD) in older population increased, and this condition often affects SUA levels, due to the insufficient excretion of uric acid [7, 8]. There are some evidence that the presence of CKD attenuates the strength of association between SUA and mortality compared to that observed among persons without CKD [9].
In older adults, concomitant conditions such as multimorbidity, frailty, disability and appetite regulation may confound the association between CV risk factors and adverse outcomes, leading to risk factor reversal [10]. Thus, the SUA intervention threshold identified in younger individuals may not apply to these older ones. We therefore studied whether SUA levels, particularly low SUA concentrations, are associated with all-cause and CV mortality in older population, and to clarify potential effect modification of reduced kidney function.
Methods
Study population
In order to monitor the health and nutritional status of the US civilian non-institutionalized population, the National Health and Nutrition Examination Survey (NHANES) as a largescale, multistage and ongoing was performed by the National Center for Health Statistics of the Centers for Disease Control and Prevention (CDC). To produce reliable statistics, NHANES over-samples persons 60 and older, and the older the individual, the more extensive the examination [11].
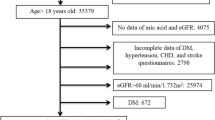
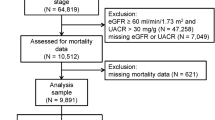
We used of ten cycles of NHANES data from 1999 to 2018. There are 19,056 individuals aged 60 years or older for whom follow-up data were eligible. We excluded participants who present of gout (n = 1136), dialysis in the previous 12 months (n = 96), with missing information and abnormal value on age, sex, race, education, BMI, biochemical test, comorbidities, co-medications (n = 3748), died or lose follow-up within 6 months (n = 71). Therefore, a total of 14,005 participants entered in our present analysis.
Outcomes
Study outcomes included any cause (all-cause) mortality and CV mortality. Every participant was follow up to 31 December 2019 or death, which one came first.
The causes of death was ascertained by matching to the National Death Index (NDI), a database of all deaths in the United States. CV mortality was defined as the primary cause of death being any disease of the circulatory system (ICD-10 codes I00-I09, I11, I13, I20-I51, or I60–I69).
Assessment of variates
Information on age, sex, race/ethnicity, education levels, smoking status, comorbidities, and medication use was collected from household interviews using standardized questionnaires. Body weight and height were obtained when people participated in the physical examinations at a mobile examination center. BMI was calculated as weight in kilograms divided by height in meters squared. Race/ethnicity was classified as non-Hispanic White, non-Hispanic Black, Mexican American, or other. Education level was categorized as low than high school, high school or equivalent, or college or above. Serum uric acid, creatinine, triglycerides, total cholesterol, high density lipoprotein cholesterol, urine albumin and creatinine concentrations were measured at baseline when the participants provided their blood and urine samples. Urinary albumin and creatinine concentrations were measured by solid phase fluorescence immunoassay and Jaffe rate reaction, respectively, in random single urine samples. urinary albumin-creatinine ratio (UACR) was calculated by urinary albumin divided by urinary creatinine. eGFR value was calculated using the creatinine equation developed by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) [12].
Diabetes was defined as self-reported doctor diagnosis of diabetes, use of insulin or oral hypoglycemic medication, fasting glucose ≥ 7.0 mmol/L, random glucose ≥ 11.1 mmol/L, or glycated hemoglobin A1c (HbA1c) ≥ 6.5%. Hypertension status was obtained from self-report, or systolic blood pressure ≥ 140 mm Hg or diastolic blood pressure ≥ 90 mm Hg. ASCVD risk was calculated according ACC/AHA Guideline [3]. CCI was calculated based on the literature published in 1997 [4].
Statistical analyses
Sample weights, clustering, and stratification were incorporated in all analyses because of the complex sampling design of the NHANES, as required to analyze the NHANES data [11]. Participants was followed to the date 31 December 2019 or death, whichever came first.
The study participants were categorized into three groups as 2 to < 5, 5 to < 7, and ≥ 7 mg/dL. Baseline characteristics are summarized as means (standard error) for continuous variables and numbers (percentages) for categorical variables.
Relationships between SUA concentrations and the risk of outcomes were evaluated on a continuous scale with restricted cubic spline (RCS) curves with 3 knots (the smallest Akaike information criterion) based on Cox proportional hazards regression models with adjustment for age, sex, race, education, smoke status, BMI, WBC count, hemoglobin, serum albumin, total cholesterol, triglycerides, urine albumin to creatinine ratio, eGFR, ASCVD risk, comorbidities (hypertension, diabetes, CV disease, CCI), and co-medications (anti-hypertension, lipid-lowering drugs, hypoglycemic, urate-lowing agents).
Associations of SUA level with all-cause and CV mortality were investigated using Cox proportional hazards regression models, with adjustment for confounders, age, sex, race, education, smoke status, BMI, laboratory test results, ASCVD risk, comorbidities, and co-medications. Hazard ratios (HR) and 95% confidence intervals (CI) were estimated for each SUA category.
We further performed subgroup analysis stratified by baseline characteristics including eGFR (< 60 and ≥ 60 ml/min/1.73 m2), UACR(< 30 and ≥ 30 mg/g), with or without CV disease and obesity (BMI ≥ 30 kg/m2).
Additional sensitivity analysis was conducted to verify the robustness of the results: considering the different survey years may affect the treatment strategies, we performed another analysis with adjusting survey years (survey cycles).
All analyses were carried out with R (package survey, version 4.2.0), a two-sided p value of less than 0.05 was considered as statistically significance.
Results
After applying all exclusion criteria, a total of 14,005 eligible participants were included in the present study, representing 44 million old people in the United States. The baseline characteristics of the study cohort stratified by the SUA concentration are presented in Table 1. The population had a mean age of 69.8 years, included 7181 (51.3%) females. The SUA concentrations were mainly found to be between 5 and 7 mg/dL (49.9%) in the data set. A total of 69.8%, 30%, and 22.7% of the participants had hypertension, diabetes mellitus, and CV disease, respectively. Compared with the lowest SUA level (2 to < 5 mg/dL), patients with higher SUA levels were more likely to be male, black, former or current smoker, obesity (BMI ≥ 30 kg/m2), had increased WBC count, UACR, triglycerides, and prevalence of comorbidities (hypertension, diabetes, CV disease and CCI count); however, patients with higher SUA concentrations had a lower eGFR and a reduced total cholesterol level, for all these comparisons (P < 0.001).
During mean 8.3 years of follow-up, 4852 all-cause death (including 1602 CV death) were observed in this cohort, which included 1458 (28.2%) patients in the SUA 2 to < 5 mg/dL group, 2307(28.6%) patients in the SUA 5 to < 7 mg/dL group, and 1087(41.9%) patients in the SUA ≥ 7 mg/dL group, respectively. After multivariable adjustment, a significant U-shaped association was observed between SUA with all-cause and CV mortality, with the lowest risk concentration of 5.5 mg/dL and 5.6 mg/dL (Fig. 1). This relationship still obvious in participants with eGFR ≥ 60 ml/min/1.73m2, but not with eGFR < 60 ml/min/1.73m2.

Relation of SUA with all-cause and CV mortality stratified by eGFR. Hazard ratio (HR) was adjusted for age, sex, race, education, smoke status, BMI, WBC count, hemoglobin, serum albumin, total cholesterol, triglycerides, urine albumin to creatinine ratio, eGFR, ASCVD risk, comorbidities (hypertension, diabetes, CV disease, CCI), and co-medications (anti-hypertension, lipid-lowering drugs, hypoglycemic, urate-lowing agents). Abbreviation: CV, Cardiovascular
Comparing with the reference group (5 to < 7 mg/dL), there was a higher risk of both all-cause and CV mortality when the SUA exceeded 7 mg/dL, the HR was 1.25 (1.13—1.38) and 1.25 (1.08—1.44). Notably, the risk of all-cause and CV morality also increased when the SUA was lower than 5 mg/dL, the HR was 1.11 (1.03—1.21) and 1.14 (1.00—1.30), further confirming the non-linear relationship between SUA concentration and mortality risk (Table 2).
Effect modification by eGFR (< 60 and ≥ 60 ml/min/1.73m2) was observed (p for interaction 0.048). Among participants with normal kidney function, the association of SUA and all-cause mortality were remained U-shaped: compared with levels of 5 to 7 mg/dL, HR was 1.16 (1.06–1.28) in the 2 to 5 mg/dL group and 1.30(1.13–1.50) in the ≥ 7 mg/dL group, respectively. But in elders with CKD, this U-shaped association changed, the 2 to < 5 group was no longer associated with an increased risk of death (HR 0.94, 95%CI 0.80—1.10). This situation similarly occurred in UACR subgroup (< 30 and ≥ 30 mg/g), while UACR more than 30 mg/g, the association of 2 to < 5 level and mortality was attenuated to 0.99 (0.85–1.16).
The U-shaped association between SUA concentration and all-cause mortality was consistent with or without CV disease and obesity (Fig. 2).

The association between SUA levels and all-cause mortality in various subgroups. Hazard ratio (HR) was adjusted for age, sex, race, education, smoke status, BMI, WBC count, hemoglobin, serum albumin, total cholesterol, triglycerides, urine albumin to creatinine ratio, eGFR, ASCVD risk, comorbidities (hypertension, diabetes, CV disease, CCI), and co-medications (anti-hypertension, lipid-lowering drugs, hypoglycemic, urate-lowing agents). Abbreviations: eGFR, estimated glomerular filtration rate; CV, Cardiovascular; UACR, urine albumin to creatinine ratio
We have performed another analysis with adjusting survey years (survey cycles). The results still supported the conclusions of this study. After multivariable adjustment, a significant U-shaped association was observed between SUA with all-cause and CV mortality.
Discussion
This study showed a significant U-shaped association between SUA concentration with all-cause and CV mortality, with the lowest mortality rate occurring in individuals with SUA concentrations ranging from 5 to 7 mg/dL (included 49.9% individuals), while revealing considerable eGFR-related differences (< 60 and ≥ 60 ml/min/1.73m2): the positive association of high uric acid levels (≥ 7 mg/dL) with all-cause mortality were strong and consistent, however the relationship of low uric acid levels (2 to < 5 mg/dL) with mortality was disappeared in elders combined with eGFR < 60 ml/min/1.73m2.
Previous studies on the association of SUA with mortality in the older people are limited and inconclusive. Some studies have suggested that SUA at the top quantile or > 7.0 mg/dL is associated with a higher risk for CV mortality in older adults [4, 13]. However, these data failed to find an increased risk of death in older adults at low concentrations of SUA [4, 13]. In some studies of older adults, SUA has not even been proven as a risk factor for cardiovascular disease [14]. Only few investigations came to know a slight increased risk of mortality in older patients with low SUA level, among those special individuals, such as diabetes [15] and malnutrition [6].
Our study found that an SUA level 2 to < 5 mg/dL was associated with greater mortality risks in the elderly population. This finding is particularly important because current guidelines do not provide an optimal lower limit for SUA concentrations [16, 17]. The URRAH study [18] even confirm that SUA levels are linearly associated with an increased risk of all-cause and CV mortality, independently from common cardiovascular risk factors, with the threshold for increasing the risk of total and CV mortality are 4.7 mg/dL and 5.6 mg/dL, significantly lower than those used for the definition of hyperuricemia in current clinical practice, this may not apply to elders. Low SUA concentration could reflect weakness and malnutrition, so the present analysis excluded patients who had died within 6 months of follow-up, and adjusted for indicators of nutritional status (e.g., BMI, total cholesterol, hemoglobin, and serum albumin) and comorbidities (hypertension, diabetes, CV disease, CCI) to make the results more reliable. This association was more pronounced in the older adults with normal kidney function or proteinuria, suggesting that low SUA acts as an independent biological indicator of CV disease in the absence of kidney decline. While CKD itself is an independent risk factor for CV disease [19], SUA is more likely to be a biological indicator of kidney function when combined with CKD. In addition, our study further provide definitive evidence for the association between asymptomatic hyperuricemia (without gout) and mortality in older people, and that was not attenuated after adjusting for kidney function and other CV disease risk factors.
Our study is suggestive of the two important but opposing properties of SUA. The putative toxic mechanism of hyperuricemia is now largely accepted to include stimulation of inflammation [20], induction of endothelial cell dysfunction [21], stimulation of vascular smooth muscle proliferation [22], and increasing oxidative stress [23], which may contribute to a substantially higher CV disease risk in these patients. A previous study reported that uric acid crystals are present in the aorta and coronary vessels of subjects, and that many uric acid deposits correspond to sites of vascular calcification and plaque formation [24], which may contribute to a substantially higher CV disease risk in these patients. However, uric acid also exerts antioxidant actions in human plasma and plays a protective role for vascular cells, including stabilization of endothelial nitric oxide synthase activity [25]. SUA may protect against various neurodegenerative diseases such as Parkinson’s disease, Alzheimer’s disease, and amyotrophic lateral sclerosis [26, 27]. The activity of enzymatic antioxidants decreases with age [28], hence, older adults are more likely to rely on non-enzymatic compounds, primarily uric acid (UA), for antioxidant action. Our results suggest that dichotomous classification of the SUA concentration is not appropriate because the mortality risk posed by an extremely low SUA concentration may be masked by this classification in future studies.
This is a prospective study design, a relatively large sample size, and a nationally representative sample of older people, which facilitates generalization. Moreover, by using 1 mg/dL increments to stratify patients according to SUA concentration rather than using quantiles, our findings make it easier for patients and physicians to standardize individual values. Finally, we adjusted for multiple potential confounders based on the understanding of elderly population, that improved the validity and robustness of our conclusions.
Several potential limitations of this study should be acknowledged. First, because it was an observational study, residual confounding factors are possible. Second, this study was conducted based on a database of only US patients; therefore, caution should be taken when generalizing the finding to other ethnicities. Third, SUA concentrations were measured only once, which may underestimate the true association of interest [29]. Finally, following the recognition that SUA concentration plays an important role in older people, controlling uric acid to an appropriate range is expected to reduce the burden of these patients; however, our study design cannot shed further light on this issue.
Conclusions
Our analyses suggested that both low and high SUA concentrations are associated with an increased risk in all-cause and CV mortality among older people. Extremely low SUA concentrations are especially undesirable, especially in those with normal kidney function.
Availability of data and materials
The datasets generated and analyzed in the current study are available at NHANES website: https://www.cdc.gov/nchs/nhanes/index.htm.
References
Williams B, Mancia G, Spiering W, et al. Linee guida ESC/ESH 2018 per la diagnosi e il trattamento dell’ipertensione arteriosa. Task Force per la Diagnosi e il Trattamento dell’Ipertensione Arteriosa della Società Europea di Cardiologia (ESC) e della Società Europea dell’Ipertensione Arteriosa (ESH) [2018 ESC/ESH Guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH)]. G Ital Cardiol (Rome). 2018;19(11 Suppl 1):3S-73S. https://doi.org/10.1714/3026.30245.
Li B, Chen L, Hu X, et al. Association of serum uric acid with all-cause and cardiovascular mortality in diabetes. Diabetes Care. 2023;46(2):425–33. https://doi.org/10.2337/dc22-1339.
Kuo CF, See LC, Yu KH, Chou IJ, Chiou MJ, Luo SF. Significance of serum uric acid levels on the risk of all-cause and cardiovascular mortality. Rheumatology (Oxford). 2013;52(1):127–34. https://doi.org/10.1093/rheumatology/kes223.
Dutta A, Henley W, Pilling LC, Wallace RB, Melzer D. Uric acid measurement improves prediction of cardiovascular mortality in later life. J Am Geriatr Soc. 2013;61(3):319–26. https://doi.org/10.1111/jgs.12149.
Ong G, Davis WA, Davis TM. Serum uric acid does not predict cardiovascular or all-cause mortality in type 2 diabetes: the Fremantle Diabetes Study. Diabetologia. 2010;53(7):1288–94. https://doi.org/10.1007/s00125-010-1735-7.
Tseng WC, Chen YT, Ou SM, Shih CJ, Tarng DC, Taiwan Geriatric Kidney Disease (TGKD) Research Group. U-shaped association between serum uric acid levels with cardiovascular and all-cause mortality in the elderly: the role of malnourishment. J Am Heart Assoc. 2018;7(4):e007523. https://doi.org/10.1161/JAHA.117.007523. Published 2018 Feb 10.
Kumar AUA, Browne LD, Li X, et al. Temporal trends in hyperuricaemia in the Irish health system from 2006–2014: A cohort study. PLoS ONE. 2018;13(5):e0198197. https://doi.org/10.1371/journal.pone.0198197. Published 2018 May 31.
Jing J, Kielstein JT, Schultheiss UT, et al. Prevalence and correlates of gout in a large cohort of patients with chronic kidney disease: the German Chronic Kidney Disease (GCKD) study. Nephrol Dial Transplant. 2015;30(4):613–21. https://doi.org/10.1093/ndt/gfu352.
Odden MC, Amadu AR, Smit E, Lo L, Peralta CA. Uric acid levels, kidney function, and cardiovascular mortality in US adults: National Health and Nutrition Examination Survey (NHANES) 1988–1994 and 1999–2002. Am J Kidney Dis. 2014;64(4):550–7. https://doi.org/10.1053/j.ajkd.2014.04.024.
Ahmadi SF, Streja E, Zahmatkesh G, et al. Reverse epidemiology of traditional cardiovascular risk factors in the geriatric population. J Am Med Dir Assoc. 2015;16(11):933–9. https://doi.org/10.1016/j.jamda.2015.07.014.
CDC. NHANES Survey Methods and Analytic Guidelines. https://wwwn.cdc.gov/Nchs/Nhanes/AnalyticGuidelines.aspx. Accessed 14 Jan 2023.
Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate [published correction appears in Ann Intern Med. 2011 Sep 20;155(6):408]. Ann Intern Med. 2009;150(9):604–12. https://doi.org/10.7326/0003-4819-150-9-200905050-00006.
Strasak AM, Kelleher CC, Brant LJ, et al. Serum uric acid is an independent predictor for all major forms of cardiovascular death in 28,613 elderly women: a prospective 21-year follow-up study. Int J Cardiol. 2008;125(2):232–9. https://doi.org/10.1016/j.ijcard.2007.11.094.
Hu P, Seeman TE, Harris TB, Reuben DB. Is serum uric acid level associated with all-cause mortality in high-functioning older persons: MacArthur studies of successful aging? J Am Geriatr Soc. 2001;49(12):1679–84.
Mazza A, Zamboni S, Rizzato E, et al. Serum uric acid shows a J-shaped trend with coronary mortality in non-insulin-dependent diabetic elderly people. The CArdiovascular STudy in the ELderly (CASTEL). Acta Diabetol. 2007;44(3):99–105. https://doi.org/10.1007/s00592-007-0249-3.
Fitz Gerald JD, Dalbeth N, Mikuls T, et al. 2020 American College of Rheumatology Guideline for the Management of Gout [published correction appears in Arthritis Rheumatol. 2021 Mar; 73(3):413]. Arthritis Rheumatol. 2020;72(6):879–95. https://doi.org/10.1002/art.41247.
Gout: diagnosis and management. London: National Institute for Health and Care Excellence (NICE); June 9, 2022.
Virdis A, Masi S, Casiglia E, et al. Identification of the uric acid thresholds predicting an increased total and cardiovascular mortality over 20 years. Hypertension. 2020;75(2):302–8. https://doi.org/10.1161/HYPERTENSIONAHA.119.13643.
Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization [published correction appears in N Engl J Med. 2008;18(4):4]. N Engl J Med. 2004;351(13):1296–305. https://doi.org/10.1056/NEJMoa04103.
Xiao J, Zhang XL, Fu C, et al. Soluble uric acid increases NALP3 inflammasome and interleukin-1β expression in human primary renal proximal tubule epithelial cells through the Toll-like receptor 4-mediated pathway. Int J Mol Med. 2015;35(5):1347–54. https://doi.org/10.3892/ijmm.2015.2148.
Khosla UM, Zharikov S, Finch JL, et al. Hyperuricemia induces endothelial dysfunction. Kidney Int. 2005;67(5):1739–42. https://doi.org/10.1111/j.1523-1755.2005.00273.x.
Yu MA, Sánchez-Lozada LG, Johnson RJ, Kang DH. Oxidative stress with an activation of the renin-angiotensin system in human vascular endothelial cells as a novel mechanism of uric acid-induced endothelial dysfunction. J Hypertens. 2010;28(6):1234–42.
Sánchez-Lozada LG, Lanaspa MA, Cristóbal-García M, et al. Uric acid-induced endothelial dysfunction is associated with mitochondrial alterations and decreased intracellular ATP concentrations. Nephron Exp Nephrol. 2012;121(3–4):e71–8. https://doi.org/10.1159/000345509.
Klauser AS, Halpern EJ, Strobl S, et al. Dual-energy computed tomography detection of cardiovascular monosodium urate deposits in patients with gout. JAMA Cardiol. 2019;4(10):1019–28. https://doi.org/10.1001/jamacardio.2019.3201.
Ames BN, Cathcart R, Schwiers E, Hochstein P. Uric acid provides an antioxidant defense in humans against oxidant- and radical-caused aging and cancer: a hypothesis. Proc Natl Acad Sci U S A. 1981;78(11):6858–62. https://doi.org/10.1073/pnas.78.11.6858.
Chen H, Mosley TH, Alonso A, Huang X. Plasma urate and Parkinson’s disease in the Atherosclerosis Risk in Communities (ARIC) study. Am J Epidemiol. 2009;169(9):1064–9. https://doi.org/10.1093/aje/kwp033.
Abraham A, Drory VE. Influence of serum uric acid levels on prognosis and survival in amyotrophic lateral sclerosis: a meta-analysis. J Neurol. 2014;261:1133–8.
Wei YH, Lee HC. Oxidative stress, mitochondrial DNA mutation, and impairment of antioxidant enzymes in aging. Exp Biol Med (Maywood). 2002;227(9):671–82. https://doi.org/10.1177/153537020222700901.
Clarke R, Shipley M, Lewington S, et al. Underestimation of risk associations due to regression dilution in long-term follow-up of prospective studies. Am J Epidemiol. 1999;150(4):341–53. https://doi.org/10.1093/oxfordjournals.aje.a010013.
Acknowledgements
The authors thank to the participants of the NHANES databases.
Funding
None.
Author information
Authors and Affiliations
Contributions
Concept and design: Yang Li. Acquisition, analysis and interpretation of the data: Yang Li, Zhongcheng Fan, Zhongju Li. Drafting of the manuscript: Yang Li. Statistical analysis: Zhongcheng Fan, Zhongju Li, Aixin Guo. Critical revision of the manuscript for important intellectual content: All authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Study protocols for NHANES were approved by the NCHS Ethnics Review Board (ERB) (Protocol #98–12, #2006–06, #2011–17 and #2018–01, https://www.cdc.gov/nchs/nhanes/irba98.htm). All participants signed the informed consent before participating in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fan, Z., Li, Z., Guo, A. et al. The association of low serum uric acid with mortality in older people is modified by kidney function: National Health and Nutrition Examination Survey (NHANES) 1999–2018. BMC Nephrol 25, 108 (2024). https://doi.org/10.1186/s12882-024-03546-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-024-03546-6