
Abstract
Background
The prevalence of low birth weight (LBW) has stagnated at approximately 12% for the past 15 years in Nepal, significantly impacting newborn survival. While antenatal care (ANC) visits and iron-folic acid supplementation are recognised as important interventions to reduce LBW, there is a lack of evidence regarding their combined effect. This study aimed to explore the potential synergistic impact of ANC and iron-folic acid supplementation on LBW in Nepal by analyzing data from two national surveys.
Methods
The nationally representative Nepal Demographic and Health Surveys of 2016 and 2022 were used, and the pooled dataset was analysed. Birth weight and the prevalence of LBW (i.e. birthweight < 2500 g) were reported using descriptive statistics. The associations among LBW, ANC visits, and iron-folic acid supplementation were examined using logistic regression analyses.
Results
The mean birth weight was 3011 g, with an LBW prevalence of 11.2%. Not attending ANC (Adjusted Odds Ratio (AOR): 1.49; 95% Confidence Interval (CI): 1.14, 1.95) and not consuming iron-folic acid supplements (AOR: 1.43; 95% CI: 1.11, 1.84) were independently associated with a higher likelihood of having LBW. Furthermore, when considering both factors together, mothers who attended less than four ANC visits and consumed iron-folic acid for ≤ 90 days had the higher likelihood of having LBW (AOR: 1.99; 95% CI: 1.35, 2.60) compared to those who did not.
Conclusions
This study highlights that the individual and joint influence of ANC visits and iron-folic acid supplementation on having LBW. These findings underscore the significance of ANC attendance and iron-folic acid supplementation in preventing LBW. Traditionally, these two interventions were primarily considered as maternal survival strategies. However, our findings indicate that these existing interventions could be utilised further for both maternal and newborn survival. Given that these services are offered free of cost and are available near people’s homes through the National Safe Motherhood Programme in Nepal, efforts to increase the uptake of these services should be strengthened while emphasising their role in preventing LBW.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Low Birth Weight (LBW) is defined as a birth weight of less than 2500 g regardless of gestational age [1]. LBW is a significant global public health issue, which has both immediate and long-term impacts on child’s health [2], and developmental outcomes [3, 4]. Infants born LBW have higher risk of mortality in neonatal and post neonatal phase [4]. These children also have stunted growth, low IQ, and problem in catching up with height and weight [5, 6]. These children are subjected to long-term non-communicable diseases risk such as higher body mass index, abdominal obesity, increased cholesterol level, pre-diabetes, and metabolic syndrome [6,7,8].
Annually, an estimated 19.8 million babies are born LBW globally, with nearly 91% reported in low- and middle-income countries [6]. This has significant implications for achieving the Sustainable Development Goals (SDGs) to “leave no one behind” [1, 9]. Therefore, the World Health Assembly (WHA) targets to reduce LBW by 30% by 2025 from the level of 2012 [10].
Nepal is a land locked country, located in South Asia and is bordered by China to the north and India to the south, east, and west with a population of about 30 million as of 2021 [10, 11]. Nepal is administratively divided into seven provinces (i.e. states). The three ecological regions include the Terai, Hills, and Mountains, each characterized by distinct geography, climate, and biodiversity [11]. These administrative divisions and ecological regions play a significant role in shaping the accessibility to essential services, livelihood opportunities and cultural practices of the people in Nepal [12].
Despite Nepal’s commitment to reduce the prevalence of LBW by 30% by 2025 as part of Global Nutrition Targets [4, 13], the prevalence of LBW has remained stagnant at around 12% from 2011 to 2016, with a concerning 3 percentage point increase in 2023 [14,15,16]. In 2018, a joint report by UNICEF and World Health Organization (WHO) revealed [13], that approximately 2.5 million newborns worldwide died within the first 28 days of life. According to the WHO 2018 report, around 80% of these deaths were among LBW infants, two-thirds of whom were born prematurely [13]. Although newborn mortality in Nepal declined from 50 to 21 deaths per 1,000 live births between 1996 and 2016, it remained at 21 deaths per 1,000 during the 2022 survey [12, 17], indicating the urgency of addressing this issue.
Various socioeconomic, pregnancy and maternal, service-related, and infant-related factors have been linked to LBW [3, 9, 18]. A recent study including data from six South Asian countries indicated that LBW is more prevalent in the socioeconomically disadvantaged sections of society [19]. While addressing socioeconomic disparities and incorporating equity into health service delivery is a long-term solution [20], mid and short-term solutions are also essential for immediate improvements, considering the urgency of this issue. Several interventions such as folic acid, calcium, iron, vitamin D, and zinc supplementation, have been studied for their impact on reducing LBW [21, 22]. Although some studies have suggested the effectiveness of specific interventions, the overall evidence on what effectively reduces LBW is not conclusive. For example, some systematic reviews and meta-analysis suggested that calcium and zinc supplementation were effective in reducing LBW [21, 22]. Other observational studies have suggested improving access to and compliance with iron supplementation as a simple recommended therapy [23, 24]. Conversely, da Silva et al. [21] found little effect of nutrition education (within ANC visits) and iron supplementation (with or without folic acid). ANC visits can provide an opportunity for health services to implement health promotion and additional supplementation activities. The potential of antenatal visits and iron-folic acid supplementation in addressing LBW, which are already part of the Nepal’s national safe motherhood programme, still needs to be explored [15, 25].
To the best of our knowledge, there has been insufficient contextual evidence to guide decision-makers in preventing LBW in Nepal. The existing literature on the impact of iron-folic acid supplementation and ANC visits on LBW in Nepal is inconclusive [21, 23]. A recent study [19], which included the demographic and health surveys of six South Asian countries conducted between 2015 and 2022, revealed an association between iron-folic acid supplementation and LBW. However, the study did not report country-specific analyses. Inter-country and intra-country contextual factors may influence such associations due to significant differences in culture, health systems, social services, and access to maternal health services. Therefore, this study aimed to investigate the combined effect of ANC visits and iron-folic acid supplementation on LBW in Nepal, using pooled data from nationally representative surveys conducted in 2016 and 2022. The findings of this study could provide valuable insights for policymakers to develop evidence-based strategies for reducing LBW in Nepal.
Methods
Data source
We used datasets from the nationally representative Nepal Demographic and Health Surveys (NDHS) of 2016 and 2022 [12, 17]. The NDHS is conducted every five years based on globally validated and locally adapted methodology. The pooled data for our analysis covered the two survey periods spanning ten years (2012–2021).
Details of the sampling process have been published in the official survey reports [12, 17]. The NDHS is a multi-stage cluster survey. In the first stage, primary sampling units are selected. In the second stage, households are selected by random sampling of households from the primary units. The respondents are women and men from the households. Household (family) and individual-level data are then collected during the surveys. Mothers reported for themselves and their children. We used the ‘Children dataset (KR)’ based on the Guide to DHS statistics [26]. This dataset contained information on birth weight based on interviews with mothers. The response rates were 98.5% for the 2016 survey [17] and 99.7% for the 2022 survey [12], respectively.
Variables
Outcome variable
Birth weights were retrieved based on the mother’s recall and/or from a birth card, excluding missing values. The continuous birth weight variable was then dichotomized as LBW if < 2500 g and ‘non-LBW’ if otherwise, in accordance with the global standard [2, 27]. We only included singleton births and last-born children for the binary outcome variable. Multiple pregnancy is a known risk factor of LBW and is likely to mask the effect of other variables [28, 29].We chose to include only last-born children for several reasons: first, information about the most recent birth is likely to be more accurate and less subject to recall bias compared to earlier births; second, including more than one birth from one mother would have included maternal and household variables more than once, potentially biasing the results towards families with multiple children, and third, the circumstances surrounding the last birth are more likely to reflect the current socioeconomic status of the household.
Factors
Although many socioeconomic and health services utilization factors have been linked to LBW in the literature, their inclusion in the present study was guided by our extensive literature review, study objective in the Nepal context, and availability in the NDHS report. The two independent variables of interest were ANC visits and the number of days of iron-folic acid consumption, which were the key services provided during pregnancy. The Ministry of Health and Population [Nepal] recommended that a pregnant woman attends four or more ANC visits, and they start taking iron-folic supplements from the second trimester till childbirth and 45 days of postpartum. Although the WHO has recently revised their recommendations for ANC visit to eight visits [30], in Nepal, this recommendation came into place after NDHS 2016 was conducted and was not fully implemented during the data collection phase of NDHS 2022. Therefore, we included four or more ANC visits as the recommended number of visits [17]. The discrete ANC variable was dichotomized as either ‘≥ 4 visits’ or ‘< 4 visits’ based on the widely practiced recommendations of four or more ANC visits prior to 2016 [31]. The number of days of taking iron-folic acid supplements, as reported by the mothers, was categorized into ‘≤ 90 days’ and ‘> 90 days’ [16]. To ascertain their synergistic association with LBW, these two binary variables were also combined into a new variable with the following categories:
-
≥ 4 ANC visits and > 90 days of taking iron-folic acid.
-
≥ 4 ANC visits and ≤ 90 days of taking iron-folic acid.
-
< 4 ANC visits and > 90 days of taking iron-folic acid.
-
< 4 ANC visits and ≤ 90 days of taking iron-folic acid.
Key confounding factors were also considered based on the available literature, and data in the dataset, including the timing of antenatal visit (early initiation: within the first trimester; late: four months or later [31]), infant sex (male; female), maternal age (15–19 years; 20–34 years; ≥ 35 years), maternal education and paternal education (no formal education; primary; secondary; higher), place of residence (urban; rural), maternal smoking (yes; no), and birth order (primipara; multipara). In addition, the type of cooking fuel was categorized as either polluting (kerosene, coal, lignite, charcoal, wood, straw, agricultural crop, animal dung) or non-polluting (biogas, electricity, natural gases, LPG), while household wealth was classified according to family possession of assets (poorest; poor; middle; richer; richest).
Statistical analysis
The mean birth weights (SD) and the prevalence of LBW (percentages), along with their 95% confidence intervals (CIs) were reported using descriptive statistics. The univariate association between each independent variable and LBW was first assessed by the Chi-square test (χ2). Adjusted odds ratios (AORs), together with their corresponding 95% CIs from the fitted multivariate models, are reported in Table 3 and supplementary Table 1.
For the two key independent variables of interest, namely ANC visits and iron-folic acid consumption, their individual, as well as joint associations with LBW, were estimated in separate models, adjusting for all independent variables included in the study. All statistical analyses were performed using Statistical Package for Social Sciences (IBM Corp version 28.0, Armonk, NY, USA) after accounting for the sampling weight of the pooled data.
Results
Birth weight and LBW prevalence
Table 1 presents the descriptive statistics of the outcome variable. Pooled data showed that the mean birth weight was 3011 g, with an LBW prevalence of 11.2%. The prevalence of LBW was almost the same between the two surveys. Among the reported birth weights (n = 4935), 17.8% were extracted from the card, and 82.2% were based on the mother’s recall. Almost one in three mothers (28.5%) reported that their babies were either not weighed or they did not know the birth weight.
Characteristics of participants
Table 2 presents the characteristics of the participants, the majority of whom were between 20 and 34 years old (84.5%). Slightly more than half of the infants were male (54.3%), with a small proportion of mothers (14.7%) and fathers (17.3%) reporting attaining higher education. About a third of the households were located in rural areas (34.7%) and used non-polluting cooking fuel (35.7%), whereas only about 4% of participants smoked cigarette or tobacco. Almost one-quarter of women still initiated their antenatal visits after the first trimester. However, the majority attended four or more ANC visits (84%) and consumed iron-folic acid supplements for more than 90 days (79.4%). Table 2 also shows that infant sex, maternal age, paternal education, birth order, and type of cooking fuel were associated with LBW based on Chi-square tests, in addition to ANC visits and iron-folic acid consumption.
ANC visits, iron-folic acid consumption, and low birth weight
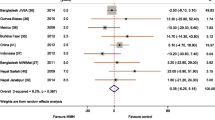
Table 3 summarizes the results from logistic regression analyses. Both ANC visits (AOR: 1.49; 95% CI: 1.14, 1.95) and iron-folic acid consumption (AOR: 1.43; 95% CI: 1.11, 1.84) remained significantly and inversely associated with LBW after adjusting for infant sex, birth order, maternal age, maternal education, paternal education, household wealth, place of residence, type of cooking fuel, and maternal smoking (Table 3; Model a). Figure 1 shows the distribution of LBW prevalence by combined variables of ANC visits and iron-folic acid consumption by mothers. The LBW prevalence was 16.4% among mothers who had less than 4 ANC visits and ≤ 90 days of iron-folic acid supplementation, compared to only 9.5% among those with four or more ANC visits and more than 90 days of iron-folic acid consumption. Furthermore, as shown in Table 1 (Model b), mothers who attended less than four ANC visits and consumed ≤ 90 days of iron-folic acid supplements (AOR: 1.88; 95% CI: 1.35, 2.60) sustained the highest likelihood of giving birth to LBW infants, when compared to their counterparts with four or more ANC visits and more than 90 days of iron-folic acid consumption. Full results of these two models, including significant and non-significant factors, are included in supplementary Table 1.

Prevalence of low birth weight by joint ANC visit and iron-folic acid consumption in Nepal using Demographic and Health Survey Data
Discussion
The study found that adhering to at least four ANC visits and consuming iron-folic acid for 90 days was protective against LBW compared to when adherence to both was not met. These findings are consistent with previous studies from Nepal and other low- and middle-income countries [23, 24, 32]. Similar studies in Nepal, India, and Bangladesh have also reported higher risks of LBW among mothers who attended less than the recommended number of ANC visits [24, 33,34,35].
The evidence regarding the association with iron-folic acid supplementation has been diverse. Previous studies from Nepal [24], India [23], and a systematic review of 49 trials from the Cochrane Database [36] evaluating the effect of supplementation with iron or iron and folic acid during pregnancy have reported positive associations between iron-folic acid supplementation and birth weight. Another systematic review and meta-analysis [22] analysed 132 articles from 101 trials, primarily conducted in Southeast Asian (n = 38) and African (n = 26) countries. This review focused on interventions for pregnant women in low- and middle-income countries and examined the impact of various interventions on outcomes such as preterm birth (< 37 weeks of gestational age), low birth weight (< 2500 g), and birth weight [22]. The findings indicated that the consumption of iron-folic acid was associated with a higher birth weight, showing a mean difference of 0.18 kg (95% CI: 0.00, 0.36 kg). Additionally, it also suggested a lower likelihood of LBW with a relative risk of 0.85 (95% CI: 0.58, 1.38) among those women who had consumed iron-folic acid. A 2015 Cochrane review including 15 randomized controlled trials among 18, 590 participants also summarized that there was an increase in mean birth weight by 23.75 g (95% CI: 3.02, 50.51) among the intervention group (taking iron) compared to those taking placebo or no iron [37].
Several causal mechanisms can explain the results of our study that adhering to at least four ANC visits or consuming iron-folic acid for 90 days or both was protective against LBW. Firstly, ANC visits provide opportunities for health promotion, screening, and early intervention, ultimately improving maternal and neonatal outcomes. In Nepal, pregnant women during ANC visits typically receive iron-folic acid supplements, tetanus and diphtheria immunization, deworming tablets, as well as advice on self-care (nutrition, rest, no smoking and drinking alcohol) during pregnancy [31, 38, 39] and post-partum; together with identification and prompt care-seeking for danger signs during pregnancy, childbirth, and the postpartum period [31, 40]. These interventions are crucial to improving their general health, well-being, and pregnancy outcomes, potentially contributing to foetal growth.
Iron-folic acid supplementation during pregnancy can help reduce oxidative stress on the foetus. Inadequate iron intake during pregnancy impedes the hormonal and neuronal regulation of pregnancy as well as fetal oxygenation [22]. Iron deficiency anaemia can lead to changes in stress-related hormones, including norepinephrine, cortisol, and corticotropin, resulting in oxidative stress and foetal growth restriction. Iron supplementation helps reverse such stress [41]. Moreover, iron-folic acid supplementation can increase the mother’s appetite [42] which is a crucial factor during pregnancy. A good appetite can lead to a better intake of food, improved nutritional status and, consequently, an improved foetal outcome. For instance, a systematic review found that intake of local food of 1500 kcal per day was associated with a reduced likelihood of LBW (RR: 0.17; 95% CI: 0.09, 0.29) [22].
The study’s strengths lie in its utilisation of pooled data from nationally representative samples, using internationally standardized methodology and locally validated questionnaires, and having a high response rate. However, several limitations must be acknowledged. Missing values were present for the birth weight outcome. For instance, as noted earlier, 28.5% of mothers could not report birth weight. For those whose birth weight was reported, they were subject to recall bias by the mothers. The maternal recall of number of antenatal visits [43], birth weight [44, 45], and their consumption of iron-folic acid [46] is subject to recall bias. We do not have further data to report the sensitivity and specificity of such recall in our study, but former studies from Nepal [44, 46] have demonstrated inaccuracies due to recall bias. However, in resource-poor settings such as Nepal, there are limited studies which can report better data. Therefore, this data collection method is still employed in the country. As mentioned in the methods section, other plausible confounding factors were omitted in our analyses. Firstly, we aimed to ascertain the joint association of ANC visits and iron-folic acid consumption with the LBW prevalence, accounting for the effects of established influencing factors. Secondly, being part of a broad national demographic and health survey, many specific pieces of information on pregnancy and lifestyle, e.g., maternal morbidity, gestational diabetes, previous history of preterm birth, dietary intake, iron-folic acid tolerance during pregnancy, air pollution, maternal stress factors, were not collected that would otherwise have been useful for inclusion in analyses. Thirdly, causal relationships could not be determined due to the cross-sectional nature of the NDHS.
Notwithstanding these limitations, the findings suggest an opportunity within the existing service delivery system to curtail the LBW problem by further promoting the benefits of ANC visits and iron-folic acid supplementation and strengthening their joint implementation. Likewise, building on the findings from another systematic review [22], additional supplements such as calcium, which have been reported useful in reducing the LBW burden, can be added as packaged interventions along with the existing ANC and iron-folic acid supplementations. Further longitudinal and life course research is needed to explore the causal mechanisms underpinning the higher incidence of LBW in Nepal and other low- and middle-income countries.
Conclusion
This study highlights the individual as well as joint influence of ANC visits and iron-folic acid supplementation on the prevalence of LBW. These interventions together were associated with a lower prevalence of LBW. This underscores the importance of strengthening the current National Safe Motherhood Programme concerning ANC and iron-folic acid supplementation. Traditionally viewed as maternal survival strategies, our findings indicate that these interventions can also enhance newborn survival. Given that these services are provided free of cost and are accessible within communities, there is a valuable opportunity for Nepal to leverage existing ANC and iron-folic acid supplementation activities in a more assertive way to improve birth outcomes. Efforts to increase the uptake of these services should be intensified, along with raising awareness of their critical role in preventing LBW. Further research should examine the opportunity to address modifiable risk factors such as the quality of services received during the ANC period and food security of pregnant women. It should also examine the potential for incorporating additional supplementations and interventions to better support mothers and families during pregnancy.
Data availability
Availability of data and materials This study uses the publicly available de-identified data which can be obtained from The DHS Program (https://dhsprogram.com/data/available-datasets.cfm ).
References
Global nutrition targets 2025. Low birth weight policy brief. In. Geneva; 2023.
Preterm. and low birth weight infants [Newborn Health (who.int)].
KC A, Basel PL, Singh S. Low birth weight and its associated risk factors: Health facility-based case-control study. PLoS ONE. 2020;15(6):e0234907.
Katz J, Lee AC, Kozuki N, Lawn JE, Cousens S, Blencowe H, Ezzati M, Bhutta ZA, Marchant T, Willey BA, et al. Mortality risk in preterm and small-for-gestational-age infants in low-income and middle-income countries: a pooled country analysis. Lancet. 2013;382(9890):417–25.
Datta Gupta N, Deding M, Lausten M. The effect of low birth weight on height, weight and behavioral outcomes in the medium-run. Econ Hum Biology. 2013;11(1):42–55.
Low birthweight [https://data.unicef.org/topic/nutrition/low-birthweight/#:~:text=In%202020%2C%2019.8%20million%20newborns,year%2 C%20suffered%20from%20low%20birthweight.].
Martin A, Connelly A, Bland RM, Reilly JJ. Health impact of catch-up growth in low‐birth weight infants: systematic review, evidence appraisal, and meta‐analysis. Matern Child Nutr 2017, 13(1).
Amadou C, Ancel P-Y, Zeitlin J, Ribet C, Zins M, Charles M-A. Long-term health in individuals born preterm or with low birth weight: a cohort study. Pediatr Res 2024.
Blencowe H, Krasevec J, De Onis M, Black RE, An X, Stevens GA, Borghi E, Hayashi C, Estevez D, Cegolon L. National, regional, and worldwide estimates of low birthweight in 2015, with trends from 2000: a systematic analysis. Lancet Global Health. 2019;7(7):e849–60.
Children. in Nepal, editor [https://www.unicef.org/nepal/children-nepal]
National Statistics Office: National Population and Housing Census. 2021. In. Kathmandu: National Statistics Office, Office of the Prime Minister and Council Ministers, Government of Nepal.; 2021.
Ministry of Health and Population [Nepal]. New ERA, ICF: Nepal Demographic and Health Survey 2022. In. Kathmandu, Nepal; 2023.
WHO. UNICEF: Survive and thrive: transforming care for every small and sick newborn. Key findings. In. Geneva: World Health Organization; 2018.
Kramer MS. Determinants of low birth weight: methodological assessment and meta-analysis. Bull World Health Organ. 1987;65(5):663.
DoHS: Annual Report: 2020–2021. In. Kathmandu, Nepal Department of Health Services, Ministry of Health and Population; 2022.
Sharma SR, Giri S, Timalsina U, Bhandari SS, Basyal B, Wagle K, Shrestha L. Low birth weight at term and its determinants in a tertiary hospital of Nepal: a case-control study. PLoS ONE. 2015;10(4):e0123962.
Ministry of Health and Population, New ERA, ICF. Nepal Demographic and Health Survey 2016. In. Kathmandu, Nepal: Ministry of Health; Nepal 2017.
Kramer MS. Determinants of low birth weight: methodological assessment and meta-analysis. Bull World Health Organ. 1987;65(5):663–737.
Khanal V, Bista S, Mishra S. Synergistic associations of antenatal care visits and iron-folic acid supplementation with low birth weight: a pooled analysis of national surveys from six south Asian countries. BMC Public Health 2024.
WHO. Global nutrition targets 2025: low birth weight policy brief. In.: World Health Organization; 2014.
Katharina da Silva L, Erika O, Prakash S, Amarjargal D, Olukunmi Omobolanle B, Juan Pablo P-R, Luz Maria D-R, Rintaro M. Effects of nutrition interventions during pregnancy on low birth weight: an overview of systematic reviews. BMJ Global Health. 2017;2(3):e000389.
Park J, Harari O, Siden E, Zoratti M, Dron L, Zannat N, Lester R, Thorlund K, Mills E. Interventions to improve birth outcomes of pregnant women living in low- and middle-income countries: a systematic review and network meta-analysis [version 2; peer review: 1 approved, 2 approved with reservations]. Gates Open Research 2020, 3(1657).
Balarajan Y, Subramanian S, Fawzi WW. Maternal iron and folic acid supplementation is associated with lower risk of low birth weight in India. J Nutr. 2013;143(8):1309–15.
Khanal V, Zhao Y, Sauer K. Role of antenatal care and iron supplementation during pregnancy in preventing low birth weight in Nepal: comparison of national surveys 2006 and 2011. Archives Public Health. 2014;72(1):1–10.
Safe Motherhood Programme [mohp.gov.np].
Croft TN, Allen CK, Zachary BW. Guide to DHS Statistics. In. Rockville. Maryland, USA: ICF; 2023.
WHO. Global Nutrition Monitoring Framework: operational guidance for tracking progress in meeting targets for 2025. In. Geneva: World Health Organization; 2017.
Onyiriuka AN. Birthweight of full-term twin infants in relation to sex-pair. Genomic Med Biomarkers Health Sci. 2011;3(3–4):123–7.
Shinwell ES, Blickstein I. The risks for very low Birth Weight infants from multiple pregnancies. Clin Perinatol. 2007;34(4):587–97.
WHO. WHO recommendations on antenatal care for a positive pregnancy experience. In. Geneva,: World Health Organization, ; 2016.
Khanal V, Bista S, Mishra SR, Lee AH. Dissecting antenatal care inequalities in western Nepal: insights from a community-based cohort study. BMC Pregnancy Childbirth. 2023;23(1):521.
Malhotra N, Upadhyay RP, Bhilwar M, Choy N, Green T. The role of maternal diet and iron-folic acid supplements in influencing birth weight: evidence from India’s National Family Health Survey. J Trop Pediatr. 2014;60(6):454–60.
Mumbare SS, Maindarkar G, Darade R, Yenge S, Tolani MK, Patole K. Maternal risk factors associated with term low birth weight neonates: a matched-pair case control study. Indian Pediatr. 2012;49:25–8.
Pawar A, Kumar D. Maternal factors associated with low birth weight: a case control study in rural Kerala. Int J Community Med Public Health. 2017;4(10):3793–5.
Khan JR, Islam MM, Awan N, Muurlink O. Analysis of low birth weight and its co-variants in Bangladesh based on a sub-sample from nationally representative survey. BMC Pediatr. 2018;18(1):1–9.
Peña-Rosas JP, Viteri FE. Effects and safety of preventive oral iron or iron + folic acid supplementation for women during pregnancy. Cochrane Database Syst Reviews 2009(4).
Peña-Rosas JP, De‐Regil LM, Garcia‐Casal MN, Dowswell T. Daily oral iron supplementation during pregnancy. Cochrane Database of Systematic Reviews 2015(7).
Adhikari M, Chalise B, Bista B, Pandey AR, Upadhyaya DP. Sociodemographic correlates of antenatal care visits in Nepal: results from Nepal demographic and Health Survey 2016. BMC Pregnancy Childbirth. 2020;20(1):1–10.
Chitekwe S, Torlesse H, Aguayo VM. Nutrition in Nepal: Three decades of commitment to children and women. In., vol. 18: Wiley Online Library; 2022: e13229.
Safe Motherhood Programme. [https://mohp.gov.np/program/safe-motherhood-programme/en]
Cogswell ME, Parvanta I, Ickes L, Yip R, Brittenham GM. Iron supplementation during pregnancy, anemia, and birth weight: a randomized controlled trial. Am J Clin Nutr. 2003;78(4):773–81.
Scrimshaw NS. Iron deficiency. Sci Am. 1991;265(4):46–53.
Xie X, Munos MK, Lama TP, Bryce E, Khatry SK, LeClerq SC, Katz J. Validation of maternal recall of number of antenatal care visits attended in rural Southern Nepal: a longitudinal cohort study. BMJ open. 2023;13(12):e079029.
Chang KT, Mullany LC, Khatry SK, LeClerq SC, Munos MK, Katz J. Validation of maternal reports for low birthweight and preterm birth indicators in rural Nepal. J Glob Health. 2018;8(1):010604.
Chang KT, Carter ED, Mullany LC, Khatry SK, Cousens S, An X, Krasevec J, LeClerq SC, Munos MK, Katz J. Validation of MINORMIX Approach for Estimation of Low Birthweight Prevalence using a rural Nepal dataset. J Nutr. 2022;152(3):872–9.
Kanyangarara M, Katz J, Munos MK, Khatry SK, Mullany LC, Walker N. Validity of self-reported receipt of iron supplements during pregnancy: implications for coverage measurement. BMC Pregnancy Childbirth. 2019;19:1–10.
Acknowledgements
The authors would like to thank The DHS Program for their approval to use the de-identified data. Thanks are also due to the mothers who shared their valuable time, and information to make the NDHS happen. We also thank Dr. Sujan Karki and Dr. Shiva Raj Mishra for their suggestions in conducting complex sample analysis.
Funding
There was no funding for this study.
Author information
Authors and Affiliations
Contributions
VK designed the original research proposal and obtained approval to use the dataset. VK conducted the initial analysis in consultation with SB and AHL. VK and SB wrote the first draft. AHL confirmed the analysis and contributed to finalizing the manuscript. All authors contributed to finalize the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study used publicly available de-identified datasets made available through The DHS Program (https://dhsprogram.com/data/available-datasets.cfm ). The DHS surveys were approved by the respective ethics committees in the individual countries and by ICF Macro Institutional Review Board in Calverton, Maryland, USA. A further analysis protocol was also approved by the DHS Program prior to allowing access to the data. The individual reports from the respective countries outline the consent process that adheres to the ethical standards.
Consent for publication
Not applicable for this analysis.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Khanal, V., Bista, S. & Lee, A.H. Examining the combined effect of antenatal care visits and iron-folic acid supplementation on low birth weight: a pooled analysis of two national data sets from Nepal. BMC Pregnancy Childbirth 24, 612 (2024). https://doi.org/10.1186/s12884-024-06807-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-024-06807-2