
Abstract
Objectives
To observe and compare the difference in retinal perfusion using optical coherence tomography angiography (OCTA) between anisometropic amblyopia in children and fellow eyes as well as age-matched controls.
Methods
A total of 16 children with anisometropic amblyopia and 19 age-matched healthy subjects were enrolled. All participants underwent OCTA examination, with 3 mm × 3 mm and 6 mm × 6 mm scans in the macular region. Perfusion parameters of the superficial retinal layer were measured by built-in software, including the macular foveal avascular zone (FAZ) area, perimeter and circularity, as well as the vessel length density (VLD) and perfusion density (PD) of the foveal, parafoveal and perifoveal regions.
Results
Among the 16 patients with anisometropic amblyopia, the FAZ area was significantly higher in diseased eyes (P = 0.027) than in fellow eyes. The VLD and PD of the foveal average and the VLD of the nasal quadrant of the perifoveal region in anisometropic amblyopic eyes were significantly lower than those in fellow eyes (P < 0.05). The VLD of the parafoveal average, the superior, temporal, inferior and nasal quadrants of the parafoveal region, and the nasal quadrant of the perifoveal region in anisometropic amblyopic eyes were significantly lower than those in healthy controls (P < 0.05). The PD of the parafoveal average, and the inferior quadrant of the parafoveal region in anisometropic amblyopic eyes were significantly lower than those in healthy controls (P < 0.05). The VLD of the parafoveal average, the superior, inferior and nasal quadrants of the parafoveal region, and the nasal quadrant of the perifoveal region in fellow eyes were significantly lower than those in healthy controls (P < 0.05). The PD of the parafoveal average, and the inferior quadrant of the parafoveal region in fellow eyes were significantly lower than those in healthy controls (P < 0.05).
Conclusions
The macular vessel density of the superficial capillary plexus is lower in anisometropic amblyopic children than in age-matched healthy children. Compared with the fellow eye, the perfusion of the amblyopic eye in children with anisometropic amblyopia also decreases.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Amblyopia is a developmental disease of the visual system. Although there was no obvious organic disease in the eye examination, the best corrected visual acuity of one or both eyes did not develop to a normal level. It has been reported that the incidence of the disease in the general population is approximately 2%-5% [1]. Hyperopic anisometropia is one of the causes of amblyopia [2,3,4]. Amblyopia often occurs in the first 2–3 years of children's growth and development. Amblyopia is generally considered to occur during the development of neurons in the retina and cerebral cortex. It has been reported that the lateral geniculate body and visual cortex are the main affected structures in amblyopia [5,6,7]. The retina is an important tissue for visual function. The superficial capillaries provide oxygen and nutrients to the superficial retina. However, the relationship between retinal blood flow and amblyopia has not yet been elucidated. OCTA is a novel noninvasive vascular imaging technology that can perform three-dimensional imaging of retinal blood flow, clearly displaying the vascular shape, and it can perform layered quantitative analysis of retinal blood flow. It has been used in the diagnosis and follow-up of a variety of fundus diseases and to investigate the pathogenesis. there are some reports about the use of. Recently, some studies using OCTA to study the macular density and FAZ in children with amblyopia found that the macular density of capillaries increases, but the results remain inconsistent, and there have been few reports on the Chinese population [8,9,10,11,12,13,14,15]. Therefore, the current study aims to use OCTA technology to quantify and compare the blood flow density of superficial retinal capillaries in children with anisometropic amblyopia, in comparison with the fellow eye and age-matched healthy children’s macular area.
Subjects and methods
Patients recruitment
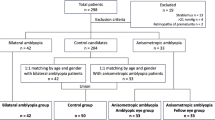
This study is a cross-sectional, case–control, noninterventional study. We recruited 16 children with anisometropic amblyopia and 19 age-matched healthy children who were regularly followed up in the Department of Pediatric Ophthalmology, Peking University First Hospital from November 2020 to May 2021. Inclusion criteria were as follows: (1) age 6–15 years old; (2) best corrected visual acuity (BCVA) ≤ 20/30 or BCVA difference of both eyes ≥ 2 line visual standard monocular amblyopic children; (3) at the first visit for patients with anisometropic amblyopia, the diopter (equivalent spherical lens) difference of both eyes is greater than 2.0 diopters (D). The exclusion criteria were as follows: (1) patients with amblyopia or nystagmus deprivation; (2) history of glaucoma, cataracts, retinopathy, optic neuropathy and other ophthalmic diseases; (3) history of eye surgery; and (4) history of preterm birth, neurological diseases or systemic diseases known to affect the retina and choroidal blood vessels such as diabetes.
Ophthalmological examinations
All subjects underwent ophthalmological examinations, including slit lamp and fundus examination, intraocular pressure, axial length (IOL Master500; Carl Zeiss Meditec, Dublin, CA), cycloplegia refraction and BCVA. Snellen BCVA was converted to logMAR for further analysis. All subjects were examined by the same skilled examiner (Cirrus HD-OCT 5000, Carl Zeiss, USA). The image quality is checked by two readers. The signal intensity is evaluated quantitatively from 1 (poor) to 10 (good), which is automatically evaluated by the machine's built-in software. When the signal strength is less than 7, and artifacts appear due to poor cooperation, such as the patient's blinking, the image quality is judged to be unqualified. Angiography scan mode was selected for the macular area scan and blood flow density parameter measurement, with the macular area as the center, scan the macular area 3 mm × 3 mm and 6 mm × 6 mm, respectively, and the scan depth is 2 mm. The software automatically stratifies the retinal tissue. The built-in AngioPlex software (version 10.0) in the system was employed to identify and measure the blood flow density parameters of the superficial retina in the macular area. The blood flow density in the FAZ, and foveal, parafoveal and perifoveal regions was analysed and measured repeatedly for three times, and the final results were averaged.
Statistical analysis
The data are first tested for normality and homogeneity of variance. The measurement data with a normal distribution are expressed as the mean ± SD, the. The comparison between the amblyopic eye group and the fellow eye group used the paired sample t test, and the comparison between the amblyopic eye group, the fellow eye group and the normal control group used the independent sample t test. The chi-square test was used to compare the two categorical variables between the two groups. One-way Covariance analysis was used to adjust the axial length and refractive power. P < 0.05 indicates that the difference is statistically significant. SPSS statistical software (IBM SPSS, USA, version 23.0) was used for statistical analysis and processing.
Results
General data of the patients
A total of 35 subjects with 51 eyes were included in the study, including 16 amblyopic eyes, 16 fellow eyes, and 19 eyes in the healthy control group. Among the patients with amblyopia, 10 were males and 6 were females, with an age of 8.19 ± 2.37 years at diagnosis. The clinical characteristics of the subjects are shown in Tables 1 and 2. Compared with the fellow eye group and the normal control group, the amblyopic eye group had a significantly shorter axial length, higher refractive power and lower LogMAR visual acuity (P < 0.05). Compared with the normal control eye group, the fellow eye group had significantly shorter axial length, higher refractive power and lower LogMAR visual acuity (P < 0.05).
FAZ area, perimeter and circularity
The mean superficial FAZ measurements (in order of amblyopic eyes, fellow eyes, control eyes, mm2) were 0.329 ± 0.163, 0.298 ± 0.132, and 0.278 ± 0.106. The area of the FAZ in the amblyopic eye group was significantly larger than that in the fellow eye group (P = 0.027). There was no significant difference in FAZ perimeter or circularity in the amblyopic eye group compared with the fellow eye and the control eye. There was no significant difference in the FAZ area, perimeter or circularity of the fellow eye compared with the control eye (P > 0.05) (Tables 3 and 4). Representative OCTA images are shown in Fig. 1.

Representative OCTA representative image of the FAZ area, perimeter and circularity measurement. The yellow area in the figure is the FAZ area. A, C and E are horizontal B-scan images passing through the central fovea in the 3 mm × 3 mm region. A and B are amblyopic eyes, C and D are contralateral eyes, and E and F are control eyes. OCTA, optical coherence tomography angiography
Vessel length density (VLD)
The VLD of the foveal average, and the nasal quadrant of the perifoveal region in anisometropic amblyopic eyes were significantly lower than those in fellow eyes (P < 0.05). The VLD of the parafoveal average and the superior, temporal, inferior, nasal quadrants of the parafoveal region and the nasal quadrant of the perifoveal region in anisometropic amblyopic eyes were significantly lower than those in control eyes (P < 0.05). The VLD of the parafoveal average, the superior, inferior, nasal quadrants of the parafoveal region, and the nasal quadrant of the perifoveal region in fellow eyes were significantly lower than those in control eyes (P < 0.05) (Tables 5 and 6). Representative OCTA images are shown in Fig. 2.

OCTA representative image of VLD. A and B are amblyopic eyes, C and D are contralateral eyes, and E and F are control eyes. The scanning range of A, C and E was 3 mm × 3 mm in the macular area. The scanning range of B, D and F was 6 mm × 6 mm in the macular area. OCTA, optical coherence tomography angiography. VLD, vessel length density
Perfusion density (PD)
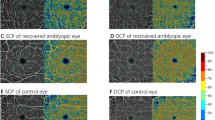
The PD of the foveal average in anisometropic amblyopic eyes was significantly lower than that in fellow eyes (P < 0.05). The PD of the parafoveal average and the inferior quadrant of the parafoveal region in anisometropic amblyopic eyes were significantly lower than those in control eyes (P < 0.05). The PD of the parafoveal average, and the inferior quadrant of the parafoveal region in fellow eyes were significantly lower than those in control eyes (P < 0.05) (Tables 7 and 8). Representative OCTA images are shown in Fig. 3.

OCTA representative image of PD. A and B are amblyopic eyes, C and D are contralateral eyes, and E and F are control eyes. The scanning range of A, C and E was 3 mm × 3 mm in the macular area. The scanning range of B, D and F was 6 mm × 6 mm in the macular area. OCTA, optical coherence tomography angiography. PD, perfusion density
Discussion
Most studies on the application of OCTA in children with anisometropic amblyopia and strabismus amblyopia found that there was no significant difference in FAZ area between amblyopic eyes and normal control eyes [8,9,10, 12, 13], which was consistent with our results. Our study found that the FAZ area of the amblyopic eye group was significantly larger than that of the fellow eye group. There was no significant difference in FAZ perimeter and circularity in the amblyopic eye group and the fellow eye compared with the control eye. FAZ is the area without perfusion in the fovea. FAZ area, perimeter and circularity are quantitative indicators measured by OCTA through automatic identification, reflecting the structure of retinal blood vessels and blood flow density. Therefore, the results of this study suggested that the retinal vascular structure in children with amblyopia is roughly normal.
In previous studies on retinal perfusion, some studies found that the blood flow density of amblyopic eyes decreased [8, 9, 12,13,14,15]. Yilmaz and colleagues included 15 patients with strabismic amblyopia (mean age, 8.2 ± 2.3 years) and 15 age-matched controls (mean age, 8.6 ± 2.2 years). They reported that the mean superficial FAZ measurements did not differ from those of the control subjects. The vessel density of the superficial capillary plexus of eyes with amblyopia is lower than that of the fellow eye and age-matched controls [8]. Lonngi et al. included 59 children with 13 amblyopic eyes (mean age, 8.0 years) and 50 control eyes (mean age, 10.3 years). They found that the vessel density in the superficial capillary plexus in patients with amblyopia was lower than that in normal controls [9]. Others reported that the blood flow density of amblyopic eyes did not change obviously [10, 11]. Demirayak et al. involved 49 eyes from 17 patients with amblyopia (mean age, 8.6 ± 2.5 years) and 21 healthy children (mean age, 9.6 ± 2.9 years). In this study, macular vessel density (VD) (%) was calculated using ImageJ software. The VD (%) was calculated using the following formula: VD (%) = vascular area (pixels) / (region of interest – FAZ area) (pixels) × 100. They found no difference between amblyopic eyes, controls, and fellow eyes of patients with unilateral amblyopia in the vessel density of the superficial capillary plexus [10]. Our study is more consistent with the former. We showed that in children with anisometropic amblyopia, the blood flow density of the macula and the surrounding retinal capillary network was reduced. Compared with the fellow eye, the blood flow density of the amblyopic eye was reduced. According to the studies, the inconsistency of the research results may be caused by the difference in the measurement method. We measured perfusion parameters of the superficial retinal layer by built-in software. Demirayak et al. calculated macular VD (%) by using ImageJ software. Different measurement methods may lead to distinct research results.
Yilmaz et al. hypothesize that decreased vessel density in amblyopic eyes may be secondary to retinal or choroid microvasculature alterations, which are secondary to underuse [8]. Lonngi et al. speculated that the decrease in blood flow density in amblyopic eyes may be related to abnormal development due to lack of normal visual experience [9]. Cheung et al. found that the decrease in blood flow density was related to short axial length in healthy children. They believed that this may also be caused by amplification errors [16]. However, other studies have reported that there is no significant correlation between the axial length and refractive power of amblyopic eyes and the related parameters of retinal blood vessels [13]. In addition, we found that the vessel density of the fellow eyes also reduced compared with healthy controls. Therefore, we believe that there is a decrease in retinal vessel density in amblyopia children, and the vessel density in the fellow eye with normal refraction is also affected to some extent. However, due to few previous studies, the specific mechanism is still unclear. Therefore, further research is expected in the future.
Our study has presented the foveal, parafoveal and perifoveal regions of the VLD and PD of the superficial retinal layer and FAZ measurements of anisometropic amblyopic, fellow, and healthy children’s eyes obtained via OCTA for the first time.
The current study also has the following limitations. First, this study is a single-center study, and only one measurement was performed. Dynamic changes in various parameters of retinal blood flow density in children with anisometropic amblyopia were not observed. In the future, large samples and longitudinal studies are still needed to further confirm that retinal blood flow density parameters can be used and whether they are an effective indicator for follow-up monitoring of the visual prognosis of children with anisometropic amblyopia. Second, limited by the current OCTA technology, considering the impact of projection artifacts on the accuracy of the quantitative analysis of the blood flow density of the deep retina and choroidal capillaries, this study only performed blood in the 3 mm × 3 mm and 6 mm × 6 mm areas of the superficial retina in the macular area. It is expected that wide-angle OCTA technology that is less affected by projection artifacts will be used in the future to conduct more in-depth research on the deep blood vessels and choroid of the whole retina in children with amblyopia.
Conclusions
In children with anisometropic amblyopia, the blood flow density of the macula and the surrounding retinal capillary network were reduced. This study provides a certain clinical basis for the future study of the pathogenesis of amblyopia and the application of OCTA technology for the diagnosis and follow-up of children with amblyopia.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author on reasonable request.
Abbreviations
- AL:
-
Axial Length
- BCVA:
-
Best Corrected Visual Acuity
- FAZ:
-
Foveal Avascular Zone
- IOP:
-
Intraocular Pressure
- LogMAR:
-
Logarithm of the Minimum Angle of Resolution
- OCTA:
-
Optical Coherence Tomography Angiography
- PD:
-
Perfusion Density
- SD:
-
Standard Deviation
- VD:
-
Vessel Density
- VLD:
-
Vessel Length Density
References
Bremond-Gignac D, Copin H, Lapillonne A, et al. Visual development in infants: physiological and pathological mechanisms[J]. Curr Opin Ophthalmol. 2011;22:S1-8.
Beck RW. Clinical research in pediatric ophthalmology: the Pediatric Eye Disease Investigator Group. Curr Opin Ophthalmol. 2002;13:337–40.
Leon A, Donahue SP, Morrison DG, Estes RL, Li C. The agedependent effect of anisometropia magnitude on anisometropic amblyopia severity. J AAPOS. 2008;12:150–6.
Shaw DE, Fielder AR, Minshull C, Rosenthal AR. Amblyopia—factors influencing age of presentation. Lancet. 1988;2:207–9.
Webber AL. Amblyopia treatment: an evidence-based approach to maximizing treatment outcome. Clin Exp Optom. 2007;90(4):250–7.
Barnes GR, Li X, Thompson B, Singh KD, Dumolin SO, Hess RF. Decreased gray matter concentration in the lateral geniculate nuclei in human amblyopes. Invest Ophthalmol Vis Sci. 2010;51:1432–8. https://doi.org/10.1167/iovs.09-3931.
Hess RF, Thompson B, Gole GA, Mullen KT. The amblyopic deficit and its relationship to geniculo-cortical processing streams. J Neurophysiol. 2010;104:475–83.
Yilmaz I, Ocak OB, Yilmaz BS, et al. Comparison of quantitative measurement of foveal avascular zone and macular vessel density in eyes of children with amblyopia and healthy controls: an optical coherence tomography angiography study[J]. J AAPOS. 2017;21(3):224–8.
Lonngi M, Velez FG, Tsui I, et al. Spectral-domain optical coherence tomographic angiography in children with amblyopia[J]. JAMA Ophthalmol. 2017;135(10):1086–91.
Demirayak B, Vural A, Onur IU, et al. Analysis of macular vessel density and foveal avascular zone using spectral-domain optical coherence tomography angiography in children with amblyopia[J]. J Pediatr Ophthalmol Strabismus. 2019;56(1):55–9.
Araki S, Miki A, Goto K, et al. Foveal avascular zone and macular vessel density after correction for magnification error in unilateral amblyopia using optical coherence tomography angiography[J]. BMC Ophthalmol. 2019;19(1):171.
Karabulut M, Karabulut S, Sabahattin Sül, et al. Microvascular changes in amblyopic eyes detected by optical coherence tomography angiography[J]. J AAPOS. 2019;23(3):155.e1-155.e4.
Doğuizi S, Yılmazoğlu M, Kızıltoprak H, et al. Quantitative analysis of retinal microcirculation in children with hyperopic anisometropic amblyopia: an optical coherence tomography angiography study[J]. J AAPOS. 2019;23(4):201.e1-201.e5.
Sobral I, Rodrigues TM, Soares M, et al. OCT angiography findings in children with amblyopia[J]. J AAPOS. 2018;22(4):286–9.
Chen W, Lou J, Thorn F, et al. Retinal Microvasculature in Amblyopic Children and the Quantitative Relationship Between Retinal Perfusion and Thickness[J]. Invest ophthalmol Vis Sci. 2019;60(4):1185–91.
Cheung CY, Li J, Yuan N, et al. Quantitative retinal microvasculature in children using swept-source optical coherence tomography: the Hong Kong Children Eye Study. Br J Ophthalmol. 2018;103(5):bjophthalmol-2018-312413.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
DHZ and CCL were responsible for the study design. XPG, PYW and YZZ examined all subjects. CCL collected the data. PYW and CCL contributed to the data analysis. CCL made major contributions to writing the manuscript. DHZ revised and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Peking University First Hospital and complied with the Declaration of Helsinki. Written informed consent was obtained from a parent or guardian for participants under 16 years old.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, C., Zhang, Y., Gu, X. et al. Optical coherence tomographic angiography in children with anisometropic amblyopia. BMC Ophthalmol 22, 269 (2022). https://doi.org/10.1186/s12886-022-02486-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-022-02486-9