
Abstract
Objective
To compare the optic-haptic interaction of different hydrophobic acrylic IOLs after using six preloaded injectors.
Methods
We reviewed the video-recordings of procedures on a total of 388 eyes that underwent phacoemulsification and intraocular lens (IOL) implantation. For six preloaded injectors: multiSert (Hoya Surgical Optics) [System 1], TECNIS Simplicity (Johnson & Johnson Vision) [System 2], TECNIS iTec (Johnson & Johnson Vision) [System 3], AutonoMe (Alcon, Laboratories) [System 4], Bluesert (Carl Zeiss Meditec) [System 5], and Prosert (OphthalmoPro GmbH) [System 6], we noted in each case the time of IOL delivery and made a descriptive observation of IOL insertion and optic-haptic-interaction.
Results
We defined standard haptic behavior where the haptics emerged “folded” from the injector and quickly recovered their pre-implantation appearance. The incidence where the leading haptic emerged in a deformed way for System 1 was 20%, System 2: 19%, System 3: 14%, System 4: 56%, System 5: 24% and System 6: 5%. For trailing haptic deformed behavior, the incidence was 36%, 6%, 4%, 8%, 18% and 2%, respectively for Systems 1 to 6. Optic-haptic adhesion occurred in 2% of cases for System 1, 44% for System 2, 52% for System 3, 48% for System 4, and 11% for System 6 (P < 0.05). Adhesion was not found with System 5.
Conclusions
We observed different deformed behavior for leading and trailing haptics in the six preloaded systems, some systems had as much as 52% optic-haptic adhesion.
Similar content being viewed by others


Introduction
Cataract surgery has witnessed a continuous stream of technological innovations in recent decades. A pivotal element in ensuring the safety and efficacy of such surgical procedures entails the precise placement of an intraocular lens (IOL). Within this context, the injector apparatus, its operational characteristics, and the properties of the IOL itself assume particular significance. The advancement of cataract surgery has facilitated the emergence of preloaded IOL delivery systems [1]. The move towards preloading injectors was accompanied by improvements in injector design, eliminating the necessity for manual loading of the IOL during the surgical procedure. Consequently, this has reduced procedural variability during IOL preparation and loading, ultimately contributing to a reduction in the overall duration of the surgical procedure [2,3,4].
There are, in general, two broad categories of preloaded injectors: push “syringe-style” injectors and screw injectors [5]. A recent addition to this classification involves an innovative injector system utilizing CO2 gas pressure for lens propulsion [5]. These categories diverge in cartridge and plunger design, injector system mechanics, and their respective interactions with the preloaded IOL, resulting in distinctive implantation behaviors associated with each preloaded IOL [6]. It is worth noting that preloaded IOL delivery systems have encountered challenges regarding predictability and safety [7,8,9,10]. In a study by Ong et al., only 45% of 85 cases exhibited accurate IOL delivery, necessitating additional rotational adjustments for the remaining 55% [7]. Furthermore, other problems associated with the preloaded IOL delivery system were reported, including adhesion between the haptic and the optic and inter-haptic adhesion. This phenomenon was particularly prevalent in single-piece IOLs [9,10,11,12]. While previous research has yet to address these adhesion issues extensively, their occurrence should be considered, and they may become more conspicuous, particularly with the introduction of new IOL models and injector systems. Therefore, we compared the lens delivery performances of six preloaded hydrophobic-acrylic IOL delivery systems. This analysis was conducted through a comprehensive review of recorded surgical procedures for routine cataract cases. In each case, we assessed the deformed presentation of two haptics, optic-haptic-interaction, and recorded the implantation time for placing the lens into the capsular bag.
Materials and methods
Study design and participants
Our study was an observational, retrospective study conducted at the eye clinic of Heidelberg University in Germany and a private practice, Privatklinik der Kreuzschwestern (Borkenstein & Borkenstein) in Graz, Austria. The Ethics Committees of the University of Heidelberg and Medical University Graz approved the protocol. All patients provided written informed consent, and the study followed the principles of the Declaration of Helsinki. We excluded patients requiring an intraocular lens outside the commercially available spherical power range. Critical exclusion criteria applied to each eye included pupil abnormality, corneal opacity, glaucoma, retina disease, and a history of ocular trauma or ocular surgery that was not resolved or stable.
The preloaded IOL delivery systems
We examined video recordings of surgery using six different IOLinjectors, all preloaded with the IOL by the manufacturer at the IOL manufacturing site. All are single-use injectors that claim to promote more efficient OR procedural time (avoiding the lens loading step in the OR) and improved safety since the possibility of contamination of the IOL during a loading procedure in the OR is avoided (Table 1and Fig. 1).
System 1
the multiSert (Hoya Surgical Optics, Singapore) has dual-insertion functionality that allows a choice between a two-handed screw or a one-handed syringe-style plunger enabling the surgeon to alter technique based on need or preference. It also has an adjustable insert shield for precise depth management of the injector tip.
System 2: TECNIS Simplicity and System 3: the TECNIS iTec (both from Johnson & Johnson Vision, New Jersey, USA) are screw-style injectors for implantation of the TECNIS IOL into the capsular bag. The TECNIS Simplicity is the newer-generation version that allows either ophthalmic viscosurgical device (OVD) or balanced salt solution (BSS) fill within the injector to lubricate lens movement in the injector nozzle.
System 4
the AutonoMe (Alcon Laboratories, Inc., Fort Worth, TX, USA) is a CO2-gas-powered, automated, fully preloaded system for a one-handed lens advancement using a “speed controller’ to implant the Clareon IOL.
System 5
The Bluesert (Carl Zeiss Meditec, Jena, Germany) is loaded with the CT LUCIA 621P. It features a silicone plunger that avoids damage to the IOL and advances with less force than needed.
System 6
The Prosert (OphthalmoPro GmbH, Sankt Ingbert, Germany) is a screw injector with a precision screw thread designed to facilitate a one-step “into the bag” implantation process. Additionally, its dynamic tip permits implantations with incisions ranging from 2.0 to 2.2 mm, and the injector tip boasts an outer diameter of 1.78 mm for precision.

Images of six different injector systems
Surgical procedure
All surgeries were performed by three experienced surgeons (AFB, RK, and GUA) under local or general anesthesia. A Centurion (Alcon, USA) or WhiteStar Signature (Johnson & Johnson, USA) phacoemulsification machine and a 0.9 mm 45° ABS Intrepid Balanced phaco tip with a NanoSleeve (Alcon, Fort Worth, USA) were used to allow micro-coaxial phacoemulsification at the intended incision sizes without wound size enlargement. All the side-port incision was made with a 1.0 mm paracentesis knife and the main corneal incision was placed at the superior (12 o’clock) quadrant of the cornea near the limbus. Knife sizes were 2.2 mm (System 1, 2, 3, 4, and 6) or 2.4 mm (System 5), according to the recommendations provided by the manufacturer of each delivery system. The IOL was inserted into the capsular bag using the preloaded delivery system prepared by a trained nurse or surgical assistant. The same ophthalmic viscosurgical device (OVD) (Hydroxypropylmethylcellulose [20.0 mg]) at room temperature (20–23° C) was used in all cases. Then, surgeons depressed or screwed the plunger to introduce the IOL through the injector nozzle into the capsular bag.
Video observation and data collection
Two authors (WJY and AFB) observed all the video recordings.
The main observations were: (1) deformed presentation of leading and trailing haptics, (2) optic-haptic-interaction during IOL delivery, (3) the time of each implantation step defined in seconds, calculated by adding the nozzle insertion and IOL unfolding together. Unfolding time is required for the folded IOL to recover 95% or more of its overall diameter before folding. The number of cases requiring additional manipulation with Sinskey hook, Irrigation/Aspiration (I/A) handpiece, and spatula to release the haptic adhesion was recorded. Other noncritical delivery events, including entrapment of trailing haptic, overriding of the syringe plunger over the optic, and damage to the optic edge, were also noted.
Statistical analysis
All data were recorded into an Excel spreadsheet (Microsoft Corp), from which the mean and standard deviation were calculated for each measurement. The Shapiro-Wilk test confirmed the normal distribution of the data. To statistically compare the data from the eyes of each group, one-way analysis of variance (ANOVA) with Bonferroni adjustment for post-hoc comparisons was used to compare IOL delivery and IOL power among these six groups. Statistical analysis was carried out using GraphPad (Graphpad Software, US), and a P value less than 0.05 was chosen for statistical significance.
Results
We enrolled 388 eyes of 367 patients (176 males, 212 females) in the study. 194 eyes (50%) underwent surgery by a surgeon (GUA or RK) at the eye clinic at Heidelberg University. The other 194 eyes underwent surgery in Private Practice Borkenstein & Borkenstein by one surgeon (AFB). The between-group difference in age, gender, and IOL power were not statistically significant (P > 0.05). The baseline demographics of
the study population are summarized in Table 2.
Presentation of leading and trailing haptic during the insertion
The standard performance expectation for haptics is to exhibit a “fold” during delivery. However, deviations from this ideal behavior can occur, resulting in what we classify as “straight”, “bend” and “twist” delivery behaviors when the leading or trailing haptic enters the capsular bag. The haptics exhibit a “Straight” behavior when they maintain a straight orientation along the barrel of the cartridge as they move forward within the cartridge nozzle; “Bend” occurs when the haptics fold incompletely as they travel within the cartridge nozzle or remain partially folded beneath the optic during release; “Twist” behavior indicates an incorrect orientation that requiring a 180-degree injector rotation to position the haptic properly (Fig. 2A and C).
System 1 experienced ten instances of deformed delivery behavior in the leading haptic (20%) and eighteen in the trailing haptics (36%). In System 2, there were sixteen occurrences of deformed delivery behavior in the leading haptic (19.5%) and five in the trailing haptics (6.1%). System 3 had fourteen cases of deformed delivery behavior in the leading haptic (14.1%) and five in trailing haptics (4%). In System 4, thirty-five cases displayed deformed delivery behavior in the leading haptic (55.6%), and five cases showed it in the trailing haptics (7.9%). System 5 recorded twelve cases of deformed delivery behavior in the leading haptic (24%) and nine in trailing haptics (18%). System 6 presented two cases of bend performance (4.5%) classified as deformed delivery behavior for the leading haptics and one case of bend performance (2.3%) for the trailing haptics, which we also considered as deformed delivery behavior (Fig. 2BD and Table 3).

Presentation of leading (A) and trailing (B) haptics. (From left to right: Fold, Straight, Bend and Twist). Standard and deformed rate of haptic presentation for leading and trailing haptics (B and D)
Optic-haptic adhesion
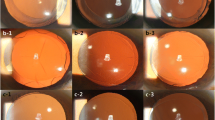
Adhesion occurred in Systems 1, 2, 3, 4, and 6 (Fig. 3A). We did not observe Adhesion in System 5. System 1 did not show any bonding between the haptics but had one case (2%) of adhesion between the haptic and optic. Thirty-six cases (43.9%) of adhesion occurred in System 2, where half (21.9%) was adhesion between two haptics and half was haptic-optic adhesion (21.9%). System 3 had fifty-two cases (52.5%) of adhesions, twenty-two cases (22.2%) between two haptics, and thirty cases (30.3%) between haptic and optic. System 4 had thirty cases (47.6%) of adhesion, with the majority (46%) occurring between haptic and optic. System 6 had five cases (11.3%) of adhesion, all haptic-to-haptic adhesion (Fig. 3B).

Adhesion Scenarios. Presentation of haptic-haptics adhesion (Left) and haptic-optic adhesion (Right) (A). Adhesion rate between the two haptics and between haptic and optic (B)
Implantation time
Figure 4 showed the results of the total implantation time. System 3 showed the longest mean delivery time (34.8 ± 9.8), whereas System 6 had the shortest (16.6 ± 4.1). Most systems had significant differences in mean total implantation time (P < 0.05). No significant differences were showed between Systems 1 and System 5, System 1 and System 6 (Fig. 4).

Total mean implantation time and mean implantation time of each phase for each delivery system. * P < 0.05
Additional manipulation
The number of cases requiring additional manipulation to release the adhesion and perform rotational adjustments to optimize the IOL’s orientation within the central of the capsular bag was: 1/50 (2%) for System 1, 23/82 (28.1%) for System 2, 32/99 (32.3%) for System 3, 32/63 (50.8%) for System 4, 12/50(24%) for System 5, and 2/44 (4.5%) for System 6.
IOL power
The IOL power exhibited a statistically significant difference in implantation time (P < 0.0087). Nonetheless, no significant differences were observed regarding adhesion occurrences between the two haptics or between haptic and optic (Fig. 5).

The correlation between IOL power and implantation time (A), occurrence of adhesion (B)
Noncritical delivery events
No cases in any systems showed the situation of entrapment of trailing haptic, overriding of the syringe plunger over the optic, and damage to the optic edge.
Discussion
We compared six preloaded injector systems by reviewing video-recorded routine cataract surgery. We took note of the presentation of leading and trailing haptics, optic-haptic-interaction, and lens delivery time. The six systems have various designs, are made of different materials, and are loaded with different lens models, all leading to patterns of lens unfolding behavior. The adhesion of the haptic and optic surfaces has been described as the “handshake phenomenon”. The strength of adhesion appears to vary according to the IOL material. Overall, System 3 has the highest adhesion rate and longest implantation time compared to the other systems.
Numerous studies have indicated that the preloaded system provides safety, reproducibility, and effectiveness during the IOL implantation [10, 11, 13]. Khoramnia et al. evaluated AutonoMe (Alcon) and iSert (Hoya) preloaded systems using video-based analysis, revealing a noteworthy absence of potentially critical events during surgery, which may be attributed to the advanced design of preloaded injectors [10]. Borkenstein et al. also examined the safety aspects of preloaded compared with non-preloaded systems, which shows that preloaded systems streamlined and enhanced the safety of IOL implantation, reducing the risk of IOL damage [13]. In regards of safety, our study did not reveal any critical complication during IOL delivery, with only minor implantation incidents observed. Most occurrences involved harmless haptic-optic adhesions or deformed presentations of the leading or trailing haptic. These resolved spontaneously or were addressed through minor adjustments by the surgeon using additional instruments. Zhang et al. compared the delivery performance of 4 injector systems in porcine cadaver eyes, including multiSert (Hoya), UltraSert (Alcon), iTec (Johnson & Johnson Vision), and RayOne (Rayner), through Miyake-Apple view videos [11]. Regarding abnormal leading haptic behaviour, they observed a single case (10%) for both multiSert and UltraSert and two cases (20%) of RayOne. However, we exhibited a higher occurrence of deformed leading haptic behavior, with 20% for multiSert and 14% for iTec. This variance may be attributed to differences in the criteria used to define deformed haptic behavior between the studies. Although these deformed haptic behaviour can occur during the insertion, they do not generally affect the IOL implantation process or cause additional damage.
Several factors contribute to the observed deformations in both leading and trailing haptic behavior during lens implantation. A recent study by Borkenstein. used computed tomography to compare the different geometric features of the optic-haptic junction (OHJ), haptic thickness and area, and OHJ volume and surface-area of five hydrophobic IOLs. The collected evidence refuted opinions that all hydrophobic acrylic one-piece IOLs with the same overall diameter are alike. The authors concluded that lens models could have considerable differences in geometry affecting the lens behavior in different capsular bag sizes [14]. The results may align well with ours, as lenses with thick OHJ and haptics unfold differently than lenses with thin OHJ when inserted through the same-sized continuous curvilinear capsulorhexis (CCC). This could explain why some lenses have specific unfolding behavior. However, to attain an objective evaluation, it is important to assess the consistency of the unfolding behavior. In our investigation, all six injector systems demonstrated notable reproducibility, with the leading and trailing haptics being predominantly introduced into the capsular bag in a standard behavior (Table 3). However, in the case of System 4, only 44.4% of the leading haptics exhibited the expected delivery performance. Deformed haptics, in particular, amplified the likelihood of interactions with the optical surface, subsequently giving rise to adhesions, some of which necessitated additional instrumental manipulation or repositioning, thereby augmenting the surgical risks. Our study showed that System 4 exhibited the second-highest occurrence of adhesion among the six systems (47.6%), with most of these cases involving interactions between the haptic and optic components. Therefore, the highest proportion requires additional surgical instruments. Consequently, reproducibility significantly contributes to safety within the operating room, allowing surgeons to concentrate on standardized procedures and minimize unforeseen complications.
Complications can occur when the IOL does not fully unfold in the bag [15]. Iwase and Tanaka reported that incomplete unfolding of the hydrophobic acrylic Hoya AF-I caused intraoperative rotation of the IOL in the capsular bag. The tendency of the unfolding and rotation can result in optical rotation and potential contact with the endothelium or inverted implantation (the implant positioned upside down) [16, 17]. Decreased implantation time could reduce the risk of complications arising from incomplete IOL unfolding. Khoramnia et al. compared the quality and duration of two preloaded injectors (AutonoMe and iSert). The implantation time included docking, injection, and unfolding [10]. Our study’s the overall implantation time included the nozzle insertion and the IOL unfolding phase. However, the surgeon could proceed with parallel surgery steps (irrigation/aspiration), and the unfolding time should not be clinically relevant. Therefore, the injection time of our study was 6.4 ± 1.9 s for System 1 and 8.0 ± 1.6 s for System 4, which showed a slightly shorter but comparable injection time compared with the study of Khoramnia et al. (8.6 ± 1.9 and 10.0 ± 2.1s). Additionally, Chung et al. comparing the performance of 5 injectors found that the IOL delivery time ranged from 14.6 ± 2.1 s with the preloaded Tecnis PCB00 to 43.2 ± 6.5 s with the manually loaded EnVista MX60 [18]. Our study only used preloaded system, showing a shorter implantation time with six different preloaded systems compared to the manually loaded injector system. Therefore, we can confirm that preloaded injectors generally reduce the time needed for IOL implantation, thereby reducing the possibility of complications.
In the past, when lenses were loaded in injectors in the OR, measures were taken to avoid unpredictable unfolding: BSS was used instead of OVD, the IOL was wetted before being placed in the injector, care was taken to align the lens within the cartridge of the injector, or OVD had to be used that had a particular temperature [19, 20]. However, the current view is that the handshake phenomenon depends on material stickiness; some haptics are slightly sticky and soluble on their own or after rinsing. In some cases, the IOL needs a secondary instrument and through-the-incision manipulation of the nozzle to release the adhesion or to aid the IOL’s centration. This additional manipulation is a recognized hazard due to the increased risk of damage to the IOL, the iris, and the ocular structure (lens capsule). It also adds to increased surgical time [18]. Acar et al. reported that ocular surface bacteria contaminate the aqueous humor in 7–43% of cataract operations [21]. Every IOL and surgical fluid in contact with a surgical instrument increases the risk of bacterial contamination from the surgical field, which is not entirely sterile [21]. In our study, System 4 (50.8%) had the highest rate requiring manipulation to release the optic-haptic adhesion during the IOL implantation. This observation is slightly better than the study by Ong et al. on the AcrySert preloaded IOL delivery system (55% required additional manipulation) [7]. Although all cases in the present study did not have an adverse outcome, it could also decrease the operating room efficiency by increasing the time required for IOL loading, particularly in high-volume cataract practices. An ideal IOL injector system should have minimal or no unfolding problems during the implantation to avoid additional manipulation, shorten the entire operation, and reduce the risk of postoperative inflammation and infection.
One limitation of the study was the absence of measurements for resistance forces during IOL ejection, which impacts the IOL implantation process. Additionally, the lack of a control group (non-preloaded injectors) restricts the ability to compare techniques. Lastly, the study used the same type of OVD in all cases, but different OVDs should be evaluated in future studies to assess their impact on adhesion scenarios.
Conclusion
In conclusion, the interaction of IOL and injector appears to be acceptable for six delivery systems. All systems showed a safe IOL implantation, and this confirmed past studies. Nevertheless, our data also emphasizes and indicates that there is still room for improving preloaded injectors, as no system shows an absence of undesired haptic behavior.
Data Availability
All related data were displayed in the manuscript. Further information regarding the data can be obtained by contacting the corresponding authors.
Abbreviations
- CCC:
-
Curvilinear capsulorhexis
- IOL:
-
Intraocular lens
- IOP:
-
Intraocular pressure
- OHJ:
-
Optic-haptic junction; OVD: ophthalmic viscosurgical device
References
Oshika T, Sasaki N. One-year multicenter evaluation of a new hydrophobic acrylic intraocular lens with hydroxyethyl methacrylate in automated preloaded delivery system. J Cataract Refract Surg 2021.
Liu J, Wolfe P, Hernandez V, Kohnen T. Comparative assessment of the corneal incision enlargement of 4 preloaded IOL delivery systems. J Cataract Refract Surg. 2020;46(7):1041–6.
Oshika T, Wolfe P. In vitro comparison of delivery performance of 4 preloaded intraocular lens injector systems for corneal and sclerocorneal incisions. J Cataract Refract Surg. 2019;45(6):840–6.
Black D, Corbett D, Roberts TV, et al. Clinical evaluation of a Novel preloaded intraocular Lens Delivery System during routine cataract Surgery. Clin Ophthalmol (Auckland NZ). 2020;14:2291–300.
Weindler JN, Naujokaitis T, Schickhardt SK, Khoramnia R, Auffarth GU. Injection time related to intraocular pressure using a CO2 driven preloaded injector: an experimental laboratory study. PLoS ONE. 2021;16(7):e0254901.
Nanavaty MA, Kubrak-Kisza M. Evaluation of preloaded intraocular lens injection systems: ex vivo study. J Cataract Refract Surg. 2017;43(4):558–63.
Ong HS, Subash M, Sandhu A, Wilkins MR. Intraocular lens delivery characteristics of the preloaded AcrySof IQ SN60WS/AcrySert injectable lens system. Am J Ophthalmol. 2013;156(1):77–81e72.
Khokhar SK, Midha N, Patil B, Nayak B, Simakurthy S. A novel technique to release sticking haptic of a single-piece hydrophobic acrylic IOL using irrigation-aspiration probe. Eur J Ophthalmol. 2016;26(3):281–2.
Yao A, Liu H. Delivery characteristics of the preloaded POB-MA 877PA intraocular Lens System: comparison of 2 incision sizes. Asia-Pacific J Ophthalmol (Philadelphia Pa). 2019;8(3):233–5.
Khoramnia R, Yildirim TM, Weindler J, Naujokaitis T, Dzhambazova M, Auffarth GU. Preloaded injectors used in a clinical study: videographic assessment and laboratory analysis of injector nozzle damage. J Cataract Refract Surg. 2021;47(10):1338–44.
Zhang L, Schickhardt S, Fang H et al. Comparison of a new intraocular lens injector system against 3 standard intraocular lens injector systems with different incision sizes: a Miyake-Apple view experimental laboratory study. J Cataract Refract Surg 2021.
Wang L, Wolfe P, Chernosky A, Paliwal S, Tjia K, Lane S. In vitro delivery performance assessment of a new preloaded intraocular lens delivery system. J Cataract Refract Surg. 2016;42(12):1814–20.
Borkenstein AF, Borkenstein EM. [Safety first - evaluation of IOL Injector systems]. Klin Monbl Augenheilkd. 2019;236(8):976–82.
Borkenstein AF, Borkenstein EM. Geometry of Acrylic, hydrophobic IOLs and changes in haptic-capsular bag relationship according to Compression and different well diameters: a Bench Study using computed tomography. Ophthalmol Therapy. 2022.
Fang H, Zhang L, Schickhardt S, et al. A laboratory evaluation of nozzle tip damage in four generations of intraocular lens injector systems using a self-developed damage scale. Sci Rep. 2022;12(1):2723.
Bhogal MS, Angunawela RI, Allan BD. Haptic misfolding during aspheric IOL insertion. J Cataract Refract Surg. 2011;37(1):208–9.
Iwase T, Tanaka N. Unfolding characteristics of a new hydrophobic acrylic intraocular lens, and possible association with Complications in triple procedures. Clin Exp Ophthalmol. 2007;35(7):635–9.
Chung B, Lee H, Choi M, Seo KY, Kim EK, Kim TI. Preloaded and non-preloaded intraocular lens delivery system and characteristics: human and porcine eyes trial. Int J Ophthalmol. 2018;11(1):6–11.
Lee HY, Choy YJ, Park JS. Comparison of OVD and BSS for maintaining the anterior chamber during IOL implantation. Korean J Ophthalmology: KJO. 2011;25(1):15–21.
van Vreeswijk H. Safe and easy way to release sticking haptic of a single-piece AcrySof intraocular lens. J Cataract Refract Surg. 2008;34(9):1611.
Acar B, Torun IM, Acar S. Evaluation of preloaded IOL Delivery System and Hydrophobic Acrylic Intraocular Lens in cataract Surgery. open Ophthalmol J. 2018;12:94–103.
Acknowledgements
We thank Donald J. Munro for his contribution to the review of the manuscript.
Funding
No funding.
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
WY, AFB, and GUA contributed to conceiving and designing the study; The data was collected by WY, AFB, RK and EMB; The data was analyzed and interpreted by WY, AFB, RK and EMB. WY and AFB draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations or declaration of Helsinki. The Ethics Committees of the University of Heidelberg and Medical University Graz approved the protocol. Informed consent was obtained from all subjects and/or their legal guardian(s).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yan, W., Borkenstein, A.F., Khoramnia, R. et al. Video analysis of optic-haptic-interaction during hydrophobic acrylic intraocular lens implantation using preloaded injectors. BMC Ophthalmol 23, 515 (2023). https://doi.org/10.1186/s12886-023-03216-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-023-03216-5