
Abstract
Purpose
To compare the biometric measurements obtained from the Pentacam AXL Wave, IOLMaster 700, and ANTERION and calculate the recommended intraocular lens power using the Barrett Formulae.
Methods
This was a retrospective cross-sectional study of patients who underwent biometry using the Pentacam AXL Wave, IOLMaster 700, and ANTERION. Flat keratometry (K1), steep keratometry (K2), anterior chamber depth (ACD), and axial length (AL) from each device were measured and compared. These parameters were used to calculate the recommended IOL powers using the Barrett formula.
Results
The study included 252 eyes of 153 patients. The IOLMaster had the highest acquisition rate among the two biometers. The Pentacam obtained the shortest mean AL, the IOLMaster measured the highest mean keratometry values, and the ANTERION measured the highest mean ACD. In terms of pairwise comparisons, keratometry and axial length were not significantly different between the Pentacam-IOLMaster and ANTERION-IOLMaster groups, while the rest of the pairwise comparisons were statistically significant. In nontoric and toric eyes, 35–45% of patients recommended the same sphere of IOL power. In another 30–40%, the Pentacam and ANTERION recommended an IOL power one step greater than that of the IOLMaster-derived data. 50% of the study population recommended the same toric-cylinder IOL power.
Conclusions
The Pentacam AXL Wave, IOLMaster 700, and ANTERION can reliably provide data for IOL power calculations; however, these data are not interchangeable. In nontoric and toric eyes, 35–45% of cases recommended the same sphere IOL power, and in another 30–40%, the Pentacam and ANTERION recommended one-step higher IOL power than the IOLMaster-derived data. In targeting emmetropia, selecting the first plus IOL power is advisable when using the Pentacam and ANTERION to approximate the IOL power calculations recommended by the IOLMaster 700.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Cataract surgery, one of the most common surgeries globally, has made many notable advances over the years [1, 2]. At the core of these improvements is the availability of premium intraocular lenses (IOLs), which have enabled patients to become less spectacle dependent [2]. Thus, in addition to the surgical technique, precise computation of the emmetropic power of the IOL is essential for achieving this goal.
The computation of intraocular lens power involves the measurement of fundamental biometric parameters, including axial length (AL), corneal refractive power (K1 and K2), and the external anterior chamber depth (ACD). Initially, corneal refractive powers came from manual keratometers, while axial length and anterior chamber depth came from ultrasonic machines. Technology has since progressed such that a single machine can provide all the needed parameters for IOL calculation. Optical biometry technology has surpassed ultrasound technology as the clinical standard for biometric measurements [2]. The accuracy of measurements is crucial because they are the basis for the IOL power, be it generated by the biometer software itself or computed using online calculators. The final lens power is then chosen based on the desired target refraction.
The Pentacam AXL Wave (Oculus, Wetzlar, Germany) (software version 1.27r11) is the upgraded version of the Pentacam AXL, which is the first machine to have five functions, namely, wavefront aberrometry, objective refraction, retroillumination, optical biometry, and Schiempflug-based tomography. The Pentacam AXL Wave consists of a Scheimpflug tomographer that scans the eye anteriorly, producing a three-dimensional image, with the addition of a partial coherence interferometry (PCI) optical biometer (475 nm wavelength) to allow for axial length measurement [2, 3]. All biometric parameters, except for lens thickness, can be measured with an IOLMaster 700 [2]. Compared to its predecessor, the Pentacam AXL Wave added a new feature of wavefront aberrometry. Notably, this new feature does not affect its biometric features.
An IOLMaster 700 (Carl Zeiss Meditec, Jena, Germany) (software version 1.90.12.5. C87915) is the latest generation biometer in the IOLMaster series and is recognized as the first swept-source optical coherence tomography (SS-OCT) biometer [4]. It can generate b-scans using lasers with variable wavelengths (high-frequency 1,055 nm tunable laser source, a scan speed of 2000 A-scans per second, with a 22 μm in-tissue axial resolution and for axial length measurements, a scan depth range of 44 mm) to produce all the biometric data needed to calculate the IOL power [2, 5,6,7]. Parameters measured include axial length, lens thickness, central corneal thickness, keratometry, anterior chamber depth, and white-to-white [2].
The ANTERION (Heidelberg Engineering, Heidelberg, Germany) is a high-resolution swept-source optical coherence tomography biometer (1300 nm wavelength) that can capture corneal topography, tomography, anterior segment metrics, and axial length measurements and perform IOL calculations from a single scan. A variant of the ANTERION is the ACE (ACE® Advanced Corneal Explorer; software version 2.4.3 (Build 1790)), adapted by Bausch and Lomb, to be the diagnostic platform linked to the Teneo excimer laser. The ANTERION has a scan speed of up to 50,000 A-scans per second. It has an in-tissue axial resolution of 10 μm and a scan depth range of 32 mm for axial length measurements. It can scan up to 16.5 mm wide and has a scan range depth of 14 ± 0.5 mm [5, 8].
The Pentacam AXL Wave, IOLMaster 700, and ANTERION serve as biometry machines but with increased functionality due to added features unique to each device. They also have higher precision and better acquisition rates than their predecessors. Since these machines utilize different technologies, our study investigated whether the biometry values obtained by the Pentacam AXL Wave, IOLMaster 700, and ANTERION were interchangeable and whether the recommended emmetropic IOL powers differed among the biometry machines, as calculated using the Barrett Universal II Formula and the Barrett Toric Calculator.
Methods
This retrospective cross-sectional study included patients who underwent cataract screening at an ambulatory surgical center between August 2021 and July 2022. In adherence to institutional regulations concerning research involving human subjects and tenets of the Declaration of Helsinki, the Ethics Review Committee at St. Frances Cabrini Medical Center-Asian Eye Institute (SCMC-AEI) has granted approval for the study protocol. They have also waived the necessity of obtaining informed consent from participants due to the retrospective nature of the study, its minimal risk, and the utilization of anonymized data. This decision was made following a comprehensive evaluation of the study protocol and ethical considerations, prioritizing the protection of participant rights and well-being. All procedures were carried out in strict accordance with ethical standards and guidelines.
Patients who were 21 years old or older and who underwent Pentacam AXL Wave, IOLMaster 700, and ANTERION biometric examinations on the same day as the standard of care for cataract screening with satisfactory measurements were included. Patients with clinically significant corneal pathologies such as keratoconus, scars or dystrophies, previous ocular surgeries, or active ocular infection and inflammation were excluded. Both eyes were collected from each participant for biometry measurements. However, only eyes with high-quality biometry readings from all three devices were included in the final analysis. Eyes with incomplete or suboptimal measurements from any of the devices were excluded to ensure the accuracy and reliability of the comparative analysis.
Biometry measurements
The scans were performed by trained diagnostic technicians. The final analysis included only good-quality scan with the Pentacam AXL Wave results displaying a QS value of “okay” and the IOLMaster 700 results displaying no exclamation point errors and with the ANTERION with only “PASS” measurements are included.
Data collection and analysis
The axial length (AL), flat keratometry (K1), steep keratometry (K2), and external anterior chamber depth (ACD) were collected for each eye from the Pentacam AXL Wave first, then from the IOLMaster 700 afterward, and finally from the ANTERION. These data were then input into an electronic spreadsheet (Microsoft Excel 2017). Unlike the Pentacam and IOLMaster, the ANTERION biometer does not directly measure the external ACD or the distance from the corneal epithelium to the anterior surface of the crystalline lens. Instead, it provides anterior aqueous depth (AQD), which is the measurement from the corneal endothelium to the anterior surface of the crystalline lens. To account for this, AQD values were added to the central corneal thickness (CCT) measurement to approximately equate to the external ACD and automatic values were recorded and analyzed [5, 7, 9]. The eyes were classified as either toric (delta K ≥ 1.0) or nontoric (delta K < 1.0) based on the difference between the K1 and K2 readings. An eye was classified as toric if at least one machine classified it as such.
The Barrett Universal II Formula v1.05 (calc.apacrs.org/barrett_universal2105) was used to calculate the recommended emmetropic IOL power for all eyes classified in the nontoric group, while the Barrett Toric Calculator v2.0 (calc.apacrs.org/toric_calculator20/Toric%20Calculator.aspx) was used for the eyes in the toric group. The A-constant used was 119.0 for all calculations. The results for the recommended IOL spherical powers, as well as the cylinder power and axis for the toric group, were collected and manually encoded into a spreadsheet.
Statistical analysis
The biometric parameters of AL, K1, K2, and ACD per eye were compared among the three biometric machines to determine agreement and consistency. Descriptive data are presented as the mean and standard deviation. Categorical data are presented as frequencies and percentages. Paired t tests were used to test for statistical significance between the biometric parameters. A p value less than 0.05 was considered to indicate statistical significance. To assess the agreement between measurements, the intraclass correlation coefficient (ICC) was calculated [3]. Good agreement was observed if the ICC values were greater than 0.900. Bland‒Altman plots were generated to evaluate the agreement between the Pentacam AXL Wave, IOLMaster 700, and ANTERION. Statistical analysis was performed using MedCalc statistical software (version 20.01). Finally, nontoric and toric emmetropic IOL powers calculated from the raw data obtained were compared to determine interchangeability.
Results
During the study period, 380 eyes were measured with the Pentacam AXL Wave, IOLMaster 700, and ANTERION. Out of the 380 eyes, 128 were excluded because they did not meet the inclusion criteria and because of measurement errors. The Pentacam had ACD errors in 0.53% (2 eyes of 380), keratometry errors in 0.26% (1 eye of 380), and AL errors in 21.32% (81 eyes of 380) of the initial sample. The IOLMaster had keratometry errors in 0.26% (1 eye of 380) and AL errors in 2.63% (10 eyes of 380) of the initial sample. ANTERION had ACD errors in 4.74% (18 eyes of 380) and AL errors in 4.74% (18 eyes of 380) of the eyes. A total of 252 eyes (153 patients) with good-quality biometry readings from all three devices were included in the final analysis. The mean age of the patients was 61.7 years, and there were more females (65.36%, n = 100) than males (34.64%, n = 53).
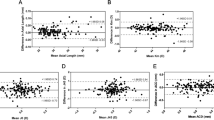
The biometric parameters investigated showed statistically significant differences in the K1, K2, ACD, and AL values obtained from the Pentacam, IOLMaster, and ANTERION (Tables 1 and 2). In terms of axial length, the Pentacam had the shortest measurements. The IOLMaster had the highest keratometry readings, while the ANTERION had the longest ACD readings. Further statistical analysis of agreeability using the intraclass correlation coefficient (ICC) showed good agreement for AL, K1, K2, and ACD among the three machines, with ICC values greater than 0.90 (Table 1). The Bland‒Altman plots, which included paired mean differences and 95% lower and upper limits of agreement, also showed good agreement between the biometric parameters of the Pentacam, IOLMaster, and ANTERION devices (Figs. 1A, 1B and 1C). The majority of the measurements of each parameter (K1, K2, ACD, and AL) were within a 95% level of agreement (Figs. 1A, 1B and 1C).

Bland-Altman plots show the agreement between Pentacam AXL Wave and IOLMaster 700 in the different biometric parameters. The bold line represents the mean and the broken lines represent the limits of agreement at 95%

Bland-Altman plots show the agreement between Pentacam AXL Wave and ANTERION in the different biometric parameters. The bold line represents the mean and the broken lines represent the limits of agreement at 95%

Bland-Altman plots show the agreement between ANTERION and IOLMaster 700 in the different biometric parameters. The bold line represents the mean and the broken lines represent the limits of agreement at 95%
A total of 117 eyes (46.43%) were classified as nontoric based on delta keratometry (K) values < 1.0 diopters (nontoric group). The recommended IOL power of each eye using each device targeted for nearest emmetropia was calculated using the Barrett Universal II Formulav1.05 and compared (Fig. 2). The mean IOL power recommended for achieving non-toric emmetropia was 19.50 ± 3.32 D when measured by the Pentacam AXL, 19.29 ± 3.44 D as measured by the IOLMaster 700, and 19.53 ± 3.47 D according to the ANTERION. In the Pentacam-IOLMaster comparison, the same IOL power was recommended for 34.19% of eyes (40 eyes). In 43.59% (51 eyes) of eyes, the IOL power recommended by the Pentacam was one step greater, or 0.50 D greater (e.g., + 20.5 D), than the IOL power recommended by the IOLMaster (e.g., + 20.0 D). In the Pentacam-ANTERION comparison, the same IOL power was recommended for 43.59% of the eyes (51 eyes). In 21.37% (25 eyes) of eyes, the IOL power recommended by the Pentacam was one step greater, or 0.50 D greater, than the IOL power recommended by the ANTERION. For ANTERION and IOLMaster, they recommended the same IOL power in 47.01% of eyes (55 eyes). In 36.75% (43 eyes) of eyes, the IOL power recommended by the ANTERION was one step greater than the IOL power recommended by the IOLMaster.

Percentage of non-toric eyes with recommended sphere intraocular lens power (IOL) similar to or different between devices (delta K < 1.0D)
Similarly, in the toric group (n = 135 eyes), the recommended sphere IOL power targeted for emmetropia was calculated and compared among the three biometric machines (Fig. 3). For toric emmetropia, the recommended IOL power was slightly lower, with the Pentacam AXL recommending 18.54 ± 4.53 D, the IOLMaster 700 suggesting 18.46 ± 4.59 D, and the ANTERION indicating 18.70 ± 4.62 D. Between the Pentacam and IOLMaster, the same IOL power was recommended for 40% of the eyes (54 eyes). In 31.11% (42 eyes) of eyes, the Pentacam recommended an IOL power one step greater or 0.50 D greater than what was recommended by the IOLMaster. Between the Pentacam and ANTERION, the same IOL power was recommended for 35.56% (48) of eyes. In 31.11% (42 eyes) of eyes, the Pentacam recommended an IOL power one step lower, or 0.50 D less than what was recommended by the ANTERION. For the ANTERION and IOLMaster groups, the same IOL power was recommended for 45.93% (62) of the eyes. In 40.74% of eyes (55 eyes), the ANTERION recommended an IOL power one step higher or 0.50 D greater than what was recommended by the IOLMaster.

Percentage of toric eyes with recommended sphere intraocular lens power (IOL) similar to or different between devices (delta K ≥ 1.0D)
In the same toric group, Pentacam and IOLMaster recommended the same cylinder IOL power in 52.59% (71 eyes) of eyes. The same cylinder IOL power was recommended for 62.96% (85) of the Pentacam and ANTERION eyes. For ANTERION and IOLMaster, they recommended the same cylinder IOL power in 50.37% (68 eyes) of eyes (Fig. 4).

Percentage of eyes with cylinder intraocular lens power (IOL) similar to or different between devices (delta K ≥ 1.0D)
The difference in the recommended axis of implantation between the Pentacam and IOLMaster was within 5 degrees in 33.33% (45 eyes), within 10 degrees in 59.26% (80 eyes), and beyond 10 degrees in 40.74% (55 eyes) (Fig. 5). Between the Pentacam and ANTERION, the difference in the recommended axis of implantation was within 5 degrees in 31.85% (43 eyes), within 10 degrees in 56.30% (76 eyes), and beyond 10 degrees in 22.22% (30 eyes). For ANTERION and IOLMaster, the difference in the recommended axis of implantation was within 5 degrees in 45.93% (62 eyes), within 10 degrees in 68.15% (92 eyes), and beyond 10 degrees in 15.56% (21 eyes).

Percentage of eyes with similar or different (within 3, 5, 10, or greater than 10 degrees) axis recommended by the Pentacam AXL Wave, IOLMaster 700, and ANTERION
Discussion
Advancements in technology and the availability of premium IOLs have elevated patient expectations of visual outcomes after phacoemulsification. Since more patients want to be less dependent on spectacles, it is imperative that we achieve the desired refractive outcomes to achieve the best performance of the IOLs implanted. Accurate biometric parameters, which include AL, K1, K2, and ACD measurements, are therefore vital because they form the basis for IOL power calculations. This study compared the raw data for these parameters from the Pentacam AXL Wave, IOLMaster 700, and ANTERION. In addition, we used a single advanced formula to calculate the IOL power targeted for emmetropia based on these four parameters obtained from each device. The goal of this additional analysis was to determine whether differences in the raw biometric data between the diagnostic machines would translate to the same or different emmetropic IOL power recommendations for each device.
Several machines capable of optical biometry have previously been compared to each other, such as the Lenstar LS 900 (Haag-Streit AG, Ko¨niz, Switzerland), IOLMaster 500 (Carl Zeiss Meditec, Jena, Germany), Aladdin (Topcon Corp., Tokyo, Japan), Pentacam AXL (Oculus Optikgeräte GmbH, Wetzlar, Germany), and the ANTERION (Heidelburg Engineering, Heidelburg, Germany) [4, 6, 10,11,12]. A recurring limitation with any optical biometer is the inability to obtain axial measurements through dense cataracts.
The IOLMaster 500, the predecessor of the IOLMaster 700, is a widely used optical biometer that uses partial coherence interferometer (PCI) technology [13]. Hirnschall et al. compared the IOLMaster 500 with the IOLMaster 700 and found that of the 23 eyes with dense cataracts that were unsuccessfully measured by the IOLMaster 500, 91.3% (21 eyes) were successfully measured by the IOLMaster 700 [14]. Akman et al. also concluded that the IOLMaster 700 was more effective than the IOLMaster 500 in measuring the biometric parameters in eyes with posterior subcapsular and dense nuclear cataracts [4].
In another study on dense cataracts, Henriquez et al. evaluated 45 eyes and reported that the IOLMaster 700 achieved the highest AL acquisition rate of 84.5%, followed by the Galilei G6, a Scheimpflug tomographer with low-coherence interferometry at 42.2%, and the Pentacam AXL at 37.7%.15 In our study, the IOLMaster 700 had the highest AL acquisition rate of 97.12%, followed by the ANTERION at 92.14% and the Pentacam at 79.06%. The higher acquisition rates in our study compared to those of Henriquez et al. can be attributed to our study population being more real-world and not limited to patients with dense cataracts only.
Hirnschall et al. and Povazay et al. addressed the inverse correlation between scattering and wavelength, called the Rayleigh scattering phenomenon. They observed that higher wavelengths lead to a greater ability to penetrate through dense media opacities [14, 15]. Since the IOLMaster 700 had a greater wavelength of 1,055 nm, it attained a higher acquisition rate than did the IOLMaster 500, which used a 780 nm wavelength, while the Pentacam AXL used a 475 nm wavelength biometer. However, despite the greater 1300 nm wavelength of the ANTERION, the IOLMaster 700 still had a higher acquisition rate. This is speculated to be due to the deeper scan range of the IOLMaster 700 at 44 mm, while that of the ANTERION was only 32 mm. Nevertheless, there will still be eyes that have cataracts that are too dense for any optical biometer to penetrate. In these situations, an immersion ultrasound (A-scan) can be used to obtain the axial length [4].
Sel et al. determined that the IOLMaster 700 produced significantly greater AL measurements (p < 0.001) than did the Pentacam AXL in the 50 eyes they studied [16]. This finding aligns with the study performed by Fisus et al., who compared 389 eyes that underwent diagnostic examination with the IOLMaster 700 and ANTERION, with the AL slightly longer for the IOLMaster 700 [5]. Muzyka-Woźniak et al. reported that the IOLMaster 500 had slightly greater AL measurements (0.01 mm) than did the Pentacam AXL in their study population of 87 eyes [3]. Kim et al. also noted a statistically significant difference in the AL between the IOLMaster 500 and the ANTERION, albeit the difference was not significant [9]. When the 3 machines were compared, as seen in Taña´-Rivero et al.’s study with a study population of 49 eyes, the Pentacam AXL produced greater values (0.013 mm) than did the IOLMaster 700. However, compared to the other 2 comparisons, namely, ANTERION with the Pentacam AXL and ANTERION with the IOLMaster 700, no significant difference was detected. Other studies previously mentioned small differences that did not alter the IOL power calculation and could be considered interchangeable [3, 9, 16]. In our study, we obtained similar results, wherein statistically significant differences between the AL measurements obtained were observed. In our study of 252 eyes, the Pentacam resulted in notably shorter axial lengths than did the other two machines. However, in the ANTERION-IOLMaster comparison, there was no statistically significant difference.
Previous studies of keratometry measurements also revealed significant differences between the IOLMaster 700 and the Pentacam AXL [5, 16, 17]. Sel et al. reported that the IOLMaster 700 had a significantly greater mean K than did the Pentacam AXL [13]. The IOLMaster 700 also showed a greater mean K than did the Pentacam HR, as presented by Ozyol et al., who investigated 62 eyes [18]. The Pentacam AXL was also observed to have lower or flatter keratometry readings, as stated by Pereira et al., than the LenStar LS 900, a biometer that uses optical low coherence reflectometry [12]. Huang et al. and Pereira et al. suggested that keratometry reading differences between machines may be due to several factors, such as microsaccades, number of readings, and tear film [12, 19]. The differences may also be due to the mechanisms used by each device [12]. Fisus et al. found a statistically significant, albeit clinically irrelevant, difference between the IOLMaster 700 and ANTERION. They noted that the ANTERION has slightly flatter keratometry values [5]. Kim et al. found that the IOLMaster 700 had markedly greater K1 values than did the ANTERION 700. The mean K2, on the other hand, was not statistically significant [9]. Taña´-Rivero et al. reported that keratometry measurements were not remarkable in their study [7]. In our study, K1 and K2 were significantly different between the Pentacam-ANTERION and ANTERION-IOLMaster comparisons. The IOLMaster was greater in the ANTERION-IOLMaster comparison, while the Pentacam was greater in the Pentacam-ANTERION comparison.
Published studies have shown varied results in anterior chamber depth. Sel et al. reported notably greater ACD measurements for the Pentacam AXL than for the IOLMaster 700 [13]. Cho et al. reported statistically significant differences in the mean ACD between the IOL Master 700 (3.16 ± 0.51 mm), Galilei G4 (3.18 ± 0.39 mm), and A-Scan (3.03 ± 0.28 mm) IOLs. In that study, Galilei G4 obtained the highest values. However, their studies also mentioned that the small differences were not significant clinically. Fisus et al. reported that there was a considerable difference in the ACD between the ANTERION and IOLMaster, where the former had a greater mean ACD of 3.20 ± 0.42 mm, while the latter had a mean of 3.13 ± 0.43 mm [5]. For Taña´-Rivero et al., comparisons of the 3 machines were statistically significant, with ANTERION having the highest mean ACD and IOLMaster 700 having the lowest [7]. In Kim et al., ANTERION had a notably greater ACD in the IOLMaster 500 and ANTERION comparisons [9]. Henriquez, Muzyka-Woźniak, Ozyol, and Nemeth et al. reported no significant differences in ACD. Our study showed statistical significance for the ACD measured by the 3 machines, which echoes studies by Taña´-Rivero et al. and Kim et al., where ANTERION acquired the highest mean ACD and IOLMaster 700 had the lowest. A summary of the studies and their corresponding results is shown in Table 3.
To assess the agreement between the measurements taken from the Pentacam, IOLMaster, and ANTERION, two methods were used. The first method, the intraclass correlation coefficient (ICC), provides a single measure of the extent of agreement. The other method, the Bland‒Altman plot, provides a quantitative estimate of how closely the values from two measurements lie. The ICC values range from 0 to 1, with 0 indicating no agreement and 1 indicating perfect agreement. The results from our study show that the Pentacam AXL Wave, IOLMaster 700, and ANTERION have excellent concordance of measurements taken from these machines for all parameters based on an ICC > 0.90. Further analysis was performed with the Bland‒Altman plot, which is a scatter plot of the mean difference between two measurements (y-axis) against the average of two measurements (x-axis). It provides a graphical display of the bias or mean difference between the two machines used with 95% limits of agreement. Our Bland‒Altman plots showed that the majority of the eyes fell within the 95% limits of agreement [20].
The acceptable limits of agreement have no uniform criterion. Ultimately, the findings that the values measured from the Pentacam AXL Wave, IOLMaster 700, and ANTERION are in agreement and interchangeable would still be based on the judgment of individual surgeons. It is highly probable that no single clinic site will have all three devices used for biometric measurements. The most crucial question to ascertain using data from our study is as follows: if a clinic had only one of these three devices, would it produce the same IOL power recommendation as the others if the same IOL formula was used? If not, is there a nomogram or adjustment factor that can be used to compensate so that, in the vast majority of cases, the IOL power would be approximately the same.
Optical biometry raw data entered into an IOL calculation formula produce IOL powers with their corresponding target refractions. Variabilities in the raw data obtained among different machines may be validated by inputting these data into the same formula and then evaluating whether the data from different machines would arrive at the same emmetropic IOL power. The Pentacam, IOLMaster, and ANTERION biometric data obtained in our study were entered into online calculators, namely, the Barrett II Universal Formulae for the nontoric group and the Barrett Toric Calculator for the toric group.
In nontoric eyes (n = 117), the IOL calculated power was the same in 34%, 44%, and 47% of cases in the Pentacam-IOLMaster, Pentacam-ANTERION, and ANTERION-IOLMaster comparisons, respectively. If you have optimized your IOL selection using the IOLMaster, the Pentacam and ANTERION may recommend a one-step increase in IOL power or result in more myopic outcomes of 43.59% and 36.75%, respectively. Therefore, we advise that the IOL power corresponding to the first plus spherical equivalent be selected when using the Pentacam and ANTERION to approximate a similar target refraction as when using the IOLMaster or to avoid a myopic outcome.
In the toric group (n = 135), the calculated sphere power was the same in 40%, 36%, and 46% of the patients in the Pentacam-IOLMaster, Pentacam-ANTERION, and ANTERION-IOLMaster comparisons, respectively. If your IOL selection is optimized for the IOLMaster, then using the Pentacam or the ANTERION would result in one-step increases in IOL sphere power of 31.11% and 40.74%, respectively. Selecting the IOL power corresponding to the first plus spherical equivalent may lessen the myopic outcomes from the Pentacam and ANTERION.
The recommended IOL cylinder power in the toric eye group was similar in 53%, 63%, and 50% of patients in the Pentacam-IOLMaster, Pentacam-ANTERION, and ANTERION-IOLMaster comparisons, respectively. The data do not show a tendency toward over- or under correction of corneal astigmatism by one device over the other. Selecting the IOL cylinder power recommended by any of the devices would seem acceptable and produce similar outcomes.
Axis wise, only 20.74–31.11% of the eyes were within 3 degrees, and 31.85–45.93% of the eyes were within 5 degrees between the 3 machines. This low percentage of consistency in axis placement could be caused either by machine differences or variance in head position during testing. When the three machines were compared, 56.3–68.15% of the eyes were within 10 degrees, and 15.56–40.74% of the eyes were beyond 10 degrees. According to Chang, an IOL rotated 10 degrees off-axis would theoretically produce an approximately one-third decrease in IOL power [21]. This would, in turn, produce unsatisfactory postoperative vision and possible IOL repositioning if the residual refractive astigmatism significantly affects uncorrected vision. Clinically, the effectiveness of cylinder correction does not solely depend on having an identical calculated toric IOL power and axis because other factors, such as the magnitude of the corneal cylinder, the contribution of the corneal incision to surgically induced astigmatism, and IOL rotation post implantation, play a role in the success of correcting corneal astigmatism with a toric IOL. When determining the axis of placement, one strategy that can be adapted is to use another device to measure keratometry and the axis, such as an automated keratometer, wherein the keratometry and the axis can be substituted in the IOL formula to provide another basis for axis placement. In the end, the surgeon needs to decide the final toric IOL axis placement based on the tools and calculations available.
Calculating the IOL power is a necessary step in preparing for cataract surgery and has a direct bearing on refractive and visual outcomes. Compared with ultrasonic measurements, optical biometers have made great advances in terms of accuracy and consistency. Each biometer has its own proprietary technology that it uses to produce data that are deemed to be the most accurate. However, these data still have to be entered into a formula to calculate the lens power. The purpose of our study was to determine whether the differences we observed in the raw data obtained by these machines would tend to produce the same IOL power. Our data suggested that the sphere power in nontoric and toric lenses was the same in approximately half of the eyes. The cylinder power was identical in approximately half to two-thirds of the included toric eyes, and the axis difference was minimal in half of these eyes. This led us to conclude that these three devices may not be interchangeable in terms of the IOL power recommended.
The Pentacam AXL Wave, IOLMaster 700, and ANTERION can perform the functions needed by a cataract practice to provide optical biometry data for calculating intraocular lens power. We made no conclusions as to which device produced the correct IOL power or was more accurate because this would need to be correlated with postsurgical refractive outcomes. It is important to keep in mind that these devices may recommend different IOL powers even when using the same Barrett formula. Therefore, customizing IOL power per diagnostic device and per type of IOL is a continuous process for improving outcomes.
Our study had several limitations. More eyes in both the non toric and toric groups are needed to produce a more consistent pattern of outcomes. Our study did not perform subgroup analysis based on the ranges of axial length and degree of astigmatism because of the inadequate sample size. Some of the eyes were very myopic or hyperopic, which possibly resulted in outliers in our population in the data analysis. To determine device accuracy, a single-surgeon prospective study with a fixed cataract surgery technique, standardized IOL, and postoperative refraction correlation is needed.
Conclusion
All three biometric devices—the Pentacam AXL Wave, IOLMaster 700, and ANTERION—can reliably provide data for IOL power calculations. The IOLMaster 700 had the highest acquisition rate compared to the Pentacam AXL and ANTERION. Although the differences in the mean axial length, keratometry, and anterior chamber depth were small, they were found to be statistically significant; therefore, the values between devices should not be interchanged. In 35–45% of patients, all three devices recommended the same IOL power in the nontoric and toric IOL groups. In another 30–40%, Pentacam and ANTERION recommended an IOL power one step higher or slightly more myopic than the IOLMaster-derived raw data. In targeting emmetropia, it may be advisable to select the IOL power corresponding to the first plus when using the Pentacam and ANTERION. An individualized nomogram to customize IOL power selection should be developed and fine-tuned based on continuous evaluation of refractive outcomes after surgery.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to compliance with the National Data Privacy Law. However, they are available from the corresponding author (rtang@asianeyeinstitute.com) upon reasonable request.
Abbreviations
- K1:
-
Flat keratometry
- K2:
-
Steep keratometry
- ACD:
-
Anterior chamber depth
- AL:
-
Axial length
- IOL:
-
Intraocular lenses
- PCI:
-
Partial coherence interferometry
- SS-OCT:
-
Swept-source optical coherence tomography
- AQD:
-
Anterior aqueous depth
- CCT:
-
Central corneal thickness
- ICC:
-
Intraclass correlation coefficient
References
Davis G. The evolution of cataract surgery. Mo Med. 2016;113(1):58–62. https://doi.org/10.1097/apo.0b013e31829df4bf
Turczynowska M, Koźlik-Nowakowska K, Gaca-Wysocka M, Grzybowski A. Effective ocular biometry and Intraocular Lens Power Calculation. Eur Ophthalmic Rev. 2016;10(02):94. https://doi.org/10.17925/eor.2016.10.02.94
Muzyka-Woźniak M, Oleszko A. Comparison of anterior segment parameters and axial length measurements performed on a Scheimpflug device with biometry function and a reference optical biometer. Int Ophthalmol. 2019;39(5):1115–22. https://doi.org/10.1007/s10792-018-0927-x
Akman A, Asena L, Güngör SG. Evaluation and comparison of the new swept source OCT-based IOLMaster 700 with the IOLMaster 500. Br J Ophthalmol. 2016;100(9):1201–5. https://doi.org/10.1136/bjophthalmol-2015-307779
Fişuş AD, Hirnschall ND, Findl O. Comparison of 2 swept-source optical coherence tomography-based biometry devices. J Cataract Refract Surg. 2021;47(1):87–92. https://doi.org/10.1097/j.jcrs.0000000000000373
Kunert KS, Peter M, Blum M, et al. Repeatability and agreement in optical biometry of a new swept-source optical coherence tomography-based biometer versus partial coherence interferometry and optical low-coherence reflectometry. J Cataract Refract Surg. 2016;42(1):76–83. https://doi.org/10.1016/j.jcrs.2015.07.039
Tañá-Rivero P, Aguilar-Córcoles S, Tello-Elordi C, Pastor-Pascual F, Montés-Micó R. Agreement between 2 swept-source OCT biometers and a Scheimpflug partial coherence interferometer. J Cataract Refract Surg. 2021;47(4):488–95. https://doi.org/10.1097/j.jcrs.0000000000000483
Schiano-Lomoriello D, Hoffer KJ, Abicca I, Savini G. Repeatability of automated measurements by a new anterior segment optical coherence tomographer and biometer and agreement with standard devices. Sci Rep. 2021;11(1):1–7. https://doi.org/10.1038/s41598-020-79674-4
Kim KY, Choi GS, Kang MS, Kim US. Comparison study of the axial length measured using the new swept-source optical coherence tomography ANTERION and the partial coherence interferometry IOL Master. PLoS ONE. 2020;15(12 12):1–11. https://doi.org/10.1371/journal.pone.0244590
Hui S, Yi L. Comparison of two optical biometers in intraocular lens power calculation. Indian J Ophthalmol. 2014;62(9):931–4. https://doi.org/10.4103/0301-4738.143930
Ortiz A, Galvis V, Tello A, et al. Comparison of three optical biometers: IOLMaster 500, Lenstar LS 900 and Aladdin. Int Ophthalmol. 2019;39(8):1809–18. https://doi.org/10.1007/s10792-018-1006-z
Pereira JMM, Neves A, Alfaiate P, Santos M, Aragão H, Sousa JC. Lenstar® LS 900 vs Pentacam®-AXL: comparative study of ocular biometric measurements and intraocular lens power calculation. Eur J Ophthalmol. 2018;28(6):645–51. https://doi.org/10.1177/1120672118771844
Shajari M, Cremonese C, Petermann K, Singh P, Müller M, Kohnen T. Comparison of axial length, corneal curvature, and Anterior Chamber depth measurements of 2 recently, Introduced devices to a known Biometer. Am J Ophthalmol. 2017;178:58–64. https://doi.org/10.1016/j.ajo.2017.02.027
Hirnschall N, Varsits R, Doeller B, Findl O. Enhanced penetration for axial length measurement of eyes with dense cataracts using swept source Optical Coherence Tomography: a consecutive observational study. Ophthalmol Ther. 2018;7(1):119–24. https://doi.org/10.1007/s40123-018-0122-1
Považay B, Hermann B, Unterhuber A, et al. Three-dimensional optical coherence tomography at 1050 nm versus 800 nm in retinal pathologies: enhanced performance and choroidal penetration in cataract patients. J Biomed Opt. 2007;12(4):041211. https://doi.org/10.1117/1.2773728
Sel S, Stange J, Kaiser D, Kiraly L. Repeatability and agreement of Scheimpflug-based and swept-source optical biometry measurements. Contact Lens Anterior Eye. 2017;40(5):318–22. https://doi.org/10.1016/j.clae.2017.03.007
Henriquez MA, Zúñiga R, Camino M, Camargo J, Ruiz-Montenegro K, Izquierdo L. Effectiveness and agreement of 3 optical biometers in measuring axial length in the eyes of patients with mature cataracts. J Cataract Refract Surg. 2020;46(9):1222–8. https://doi.org/10.1097/j.jcrs.0000000000000237
Özyol P, Özyol E. Agreement between swept-source Optical Biometry and Scheimpflug-based Topography measurements of Anterior Segment parameters. Am J Ophthalmol. 2016;169:73–8. https://doi.org/10.1016/j.ajo.2016.06.020
Huang J, Pesudovs K, Wen D, et al. Comparison of anterior segment measurements with rotating Scheimpflug photography and partial coherence reflectometry. J Cataract Refract Surg. 2011;37(2):341–8. https://doi.org/10.1016/j.jcrs.2010.08.044
Ranganathan P, Pramesh C, Aggarwal R. Common pitfalls in statistical analysis: measures of agreement. Perspect Clin Res. 2017;8(4):187–91. https://doi.org/10.4103/picr.PICR_123_17
Chang DF. Comparative rotational stability of single-piece open-loop acrylic and plate-haptic silicone toric intraocular lenses. J Cataract Refract Surg. 2008;34(11):1842–7. https://doi.org/10.1016/j.jcrs.2008.07.012
Funding
RTA (none), BLE (none), PCL (none), MNU (none), MQA (none), EMC (none).
Author information
Authors and Affiliations
Contributions
Design and conduct of the study (RTA); collection (BLE, PCL), management (RTA), analysis (RTA, BLE, PCL, MNU, MQA), interpretation of the data (RTA, BLE, PCL, MNU, MMQ, EMC); manuscript preparation (RTA, BLE, PCL, MNU, MQA, MNU), manuscript review (RTA, BLE, PCL, EMC), manuscript approval (RTA, EMC).
Corresponding author
Ethics declarations
Ethics approval and consent to participate
In compliance with institutional guidelines for research involving human subjects, the St. Frances Cabrini Medical Center-Asian Eye Institute (SCMC-AEI) Ethics Review Committee has officially approved the study protocol and waived the need to obtain participants’ informed consent. The decision was made on the basis of the study’s retrospective design, low participant risk, and use of anonymized data. The decision was made after a careful evaluation of the research protocol and ethical issues, with a strong emphasis on protecting participant rights and welfare. All procedures were carried out in complete conformity to ethical norms and guidelines.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ang, R.E.T., Estolano, B.L., Luz, P.H.C. et al. Comparison of measurements and calculated lens power using three biometers: a Scheimpflug tomographer with partial coherence interferometry and two swept source optical coherence tomographers. BMC Ophthalmol 24, 410 (2024). https://doi.org/10.1186/s12886-024-03658-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-024-03658-5