
Abstract
Background
Tenofovir disoproxil fumarate (TDF) is effectively used as the first-line antiviral for chronic hepatitis B virus (HBV) infection in adults and children older than 12 years. To date, no confirmed case of virologic breakthrough (VBT) in a pediatric case has been reported.
Case presentation
Here we describe a case of a 5-year old, asymptomatically infected with HBV infection two months after chemotherapy for precursor B acute lymphoblastic leukemia (ALL). Although the 5-year old male is South African, his family originated from Guinea. At the end of the one-year follow-up, the infection progressed to chronic HBV infection, with a high viral load. At 36 weeks (8 months) post-treatment with lamivudine (LAM), there was a partial virologic response (PVR) and after 61 weeks (14 months), he was switched to TDF rescue monotherapy. Even with TDF treatment, he still experienced VBT and subsequent PVR. The full-length genome of HBV isolated 78 weeks after the switch to rescue TDF monotherapy was sequenced and belonged to genotype E. In addition to the LAM mutations (rtS256G and rtM267L), missense mutations in B-cell, T-cell, HLA class I and II-restricted epitopes emerged, which were to evade and escape host surveillance, leading to delayed viral clearance, persistence and disease progression. Two further events of VBT occurred between weeks 113 and 141 of TDF rescue-therapy. Viral loads and liver enzymes are normalizing progressively with long-term therapy.
Conclusion
Although the host immune reconstitution may be delayed, prolonged TDF treatment was effective in treating this pediatric case of HBV infection with VBT and PVR.
Similar content being viewed by others


Background
HBV infection is an ongoing global health problem. According to the World Health Organization (WHO) global coverage rate of three doses of the hepatitis B virus (HBV) vaccine is estimated to be 84%. This vaccination coverage has resulted in a decrease in the incidence of HBV infection. Nevertheless, HBV infection persists in highly endemic regions, including Africa and South East Asia.
Early childhood HBV infection leads to a much higher rate of persistent infection and long-term complications such as liver cirrhosis and hepatocellular carcinoma (HCC) [1, 2]. In endemic countries, HBV infection occurs mainly during infancy and early childhood. The risk of developing chronic infection is higher in newborns (90%) than in infants/young children (< 5 years old) (25–30%) and immunocompetent older children and adults (< 5%) [3]. Therefore, childhood HBV infection presents medical and public health challenges. In regions with a high prevalence, HBV infection is mostly transmitted either from mother to child at birth (perinatally) as seen in Asia or through exposure to infected blood or body fluid (horizontally) early in life mainly from HBsAg-positive family members/household contacts, playmates or by unsafe medical interventions as seen in Africa [4]. Perinatal or childhood infection is distinct from infection in adulthood [5]. It is characterized by a long-lasting immune-tolerant phase, with no or few symptoms with mild and stable liver disease, persistently high HBV viral load (>107copies/mL), minimal or no inflammation in the liver [6].
Acute lymphoblastic leukemia (ALL) is the most common childhood malignancy, accounting for approximately 25% of all childhood cancers and about 75% of pediatric acute leukemias [7]. A majority of ALL cases develop in children and teenagers (under 15 years of age), mainly in males, with peak incidence in the 2- to 5-year age group. ALL is identified morphologically by more than 25% of leukemic bone marrow blasts [8]. ALL is further subtyped into either B or T cell lineage ALL (WHO classification), being predominately B-cell lineage (85%) [9]. Fortunately, with the improvement in chemotherapy technologies and conservative treatment, the 10-year survival rate for pediatric ALL is 91% [10]. However, infectious complications remain major causes of morbidity and mortality in ALL patients.
Patients with acute leukemia (including ALL) are immunocompromised, characterized by impaired leukocyte proliferation and aberrant maturation, resulting in compromised granulocyte function [11, 12]. In addition, a weaker immune defence system renders pediatric patients more susceptible to bacterial, fungal, and viral infections [11]. Furthermore, medications used in standard chemotherapy regimens are known to be immune-suppressive by affecting leukocyte function, resulting in prolonged neutropenia [12]. Prolonged neutropenia is a risk factor for infections in ALL [13, 14]. Infectious complications are the leading cause of treatment-related morbidity and mortality in pediatric ALL [15] and are highest during the induction and consolidation phases [16, 17].
HBV infection is frequent in patients with acute leukemia [18, 19], and children with this haematological dyscrasia have a higher risk of chronic HBV infection [20], especially for those living in highly endemic countries [21]. For patients with hematological malignancies, new viral infections after the onset of ALL and reactivation of latent infection are the common manifestations of infection during the period of weaker immunity [16, 22]. The general guideline consensus is to routinely screen high-risk patients, especially individuals born in intermediate or high HBV prevalence countries, for HBsAg, anti-HBc, and anti-HBs, prior to immunosuppressive therapy [23].
Here, we report a young male in ALL remission with chronic HBV, genotype E infection. He was treated with lamivudine (LAM), followed by tenofovir (TDF) as rescue monotherapy. Multiple events of virologic breakthrough (VBT) and partial virologic response (PVR) were observed during antiviral treatment, with HBV developing LAM resistance but not TDF resistance mutations. Immune escape mutations in immune epitopes were also detected. These mutations could have induced ineffective HBV-specific immune responses, favoring HBV persistence, leading to VBT and PVR.
Case presentation
In October 2010, while visiting Angola, the one year old South African-born male, whose parents originated in Guinea, first became ill and was admitted to the hospital and received two blood transfusions. The child arrived in Johannesburg acutely ill. He was profoundly anemic with bruises, in respiratory distress, and congestive cardiac failure. Before admission, the patient was transfused with packed cells, received alkalinizing fluid, and two full days of Amoxicillin and Clavulanate prescribed by his pediatrician in Johannesburg. He was referred and admitted to the Pediatric Haematology and Oncology Unit, Charlotte Maxeke Johannesburg Academic Hospital (CMJAH), Johannesburg, South Africa. Initial assessment showed the patient had the signs and symptoms of significant lymphadenopathy, anemia, thrombocytopenia, and neutropenia.
A bone marrow aspiration analysis showed 97% blasts, which were small to intermediate in size of high nuclear-to-cytoplasm (NC) ratio, basophilic cytoplasm with occasional folded nuclei and vacuolated cytoplasm. Immunophenotype analysis of bone marrow sample showed 85% CD19/CD10 co-expressing cells, small to intermediate-sized cells expressing the following antigens: CD45+, CD10++, CD19++, CD22+/++, HLA-DR++ and CD38+++, one half of these cells express CD13+ and one third expressed CD15 dim. Cytogenetic analysis revealed diploid karyotype with a chromosomal t(1;19) translocation. Available data characterized this case as precursor B acute lymphoblastic leukemia (ALL), with aberrant myeloid marker expression. At the time of diagnosis, the patient was one year and 11 months old. Although hepatitis B status is routinely assessed prior to commencement of chemotherapy, there was no available hepatitis B serology result on this patient. In November 2010, he was started on a Modified Berlin-Frankfurt-Munster (BFM)-95 protocol (high risk) and treatment was completed in November 2013.
In January 2014, at the age of 5 years, while on a follow up visit for his ALL to the Pediatric Hematology and Oncology Unit, CMJAH, the child was first detected to have asymptomatic HBV infection, without clinical signs of acute hepatitis. Even though the boy had received the complete HBV vaccination schedule at 7, 11 and 24 weeks after birth, he tested positive for HBsAg. The laboratory panel showed normal alkaline phosphatase, normal total bilirubin and conjugated bilirubin, normal aspartate aminotransferase (AST), mildly elevated, alanine aminotransferase (ALT), negative for anti-HBs and anti-HBc, positive for HBeAg and HBeAb. The decision was to monitor the patient, with regular assessment.
In late 2013, the mother of the child had been diagnosed with acute HBV infection and resolved the infection without treatment. Immediately after the mother’s diagnosis, the other family members were screened for HBV infection. The father tested negative for HBsAg and anti-HBs but was positive for anti-HBc. The younger female sibling of the boy tested negative for HBV infection.
In February 2015, during a follow-up, a high HBV viral load (1.7 × 108 IU/mL) was detected. Further laboratory tests revealed elevated AST: 44 IU/L and ALT: 61 IU/L, with positivity for HBsAg and HBeAg, and undetectable anti-HBs. The patient was referred to the Pediatric Hepatology Unit at CMJAH and diagnosed as chronic hepatitis B (CHB) infection in the immune-tolerant phase transitioning into HBeAg-positive immune-active phase and started on oral LAM (100 mg, daily).
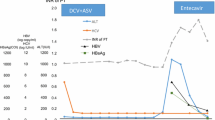
Upon monitoring, the first partial viral response (PVR) was detected at 36 weeks of LAM therapy (Fig. 1). PVR is defined as more than 1 log10 IU/mL decrease in HBV DNA but still detectable by real-time PCR, after at least 24 weeks of therapy of low genetic barrier (48 weeks for high genetic barrier) to resistance nucleot(s)ides analogue (NA) treatment [24, 25]. Thus, tenofovir (TDF)-based rescue monotherapy was introduced after 61 weeks of LAM therapy. The TDF dosage assessed by age and body weight was 225 mg once a day. After switching to TDF, the HBV DNA viral load continued to decline for 18 weeks (Fig. 1). Thereafter, the patient experienced viral breakthrough (VBT), at 46 weeks after the initiation of TDF. VBT is defined as ≥1 log10 IU/ml increase in serum HBV DNA level from nadir in two consecutive samples, 1 month apart, in patients who have responded and have been compliant with antiviral medication [26]. The level of ALT increased further to 146 IU/L, at the VBT event (Fig. 1).

Time course of antiviral treatment and HBV viral load/ALT monitored from 2015 to 2019. The child was 23 months old when lamivudine treatment was initiated. Time points for HBeAg, HBsAg and HBsAb serology tests are shown with green stars. [Abbreviations ALT: amino alanine transferase, LAM: lamivudine, PVR: partial virologic response, TDF: tenofovir, VBT: viral breakthrough]
Hepatitis D virus (HDV) is known to affect HBV viral load. To preclude the possibility of HDV/HBV co-infection or superinfection, the HDV RNA PCR test was ordered after 78 weeks of TDF treatment (National Health Laboratory Services, South Africa). The patient was HDV-negative.
Concurrently, HBV DNA was extracted from serum, using the QIA Amp DNA mini kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. The complete full-length HBV genome was amplified using the methods described previously, with the Platinum™ SuperFi™ PCR master mix (Invitrogen, Carlsbad, CA, USA) after 78 weeks of TDF treatment [27]. PCR products were directly sequenced using the Sanger protocol (Inqaba Biotech, Pretoria, South Africa). Assembly of the sequenced fragments was performed using an in-house developed bioinformatic tool [28] and the generated full length consensus sequence blasted on the NCBI database (https://www.ncbi.nlm.nih.gov/). The complete nucleotide sequence of HBV isolate has been deposited in GenBank under the accession number OM256457. The alignment of the sequenced full-length HBV to representative full-length genotype A to E sequences available in the public repository was performed by MUSCLE v3.8 algorithm (Edgar Robert C). Phylogenetic analysis with bootstrap evaluation was performed using the maximum likelihood method with the Gamma Generalized Time Reversible (GRT + G) model of nucleotide substitution as implemented in the RAxML version 8.0.20 [29]. The resulting phylogenetic tree was converted to midpoint rooted, annotated and visualized using the Interactive Tree of Life version 5.7 [30].
Phylogenetic analysis of full-length HBV genome revealed the patient was infected with genotype E, clustering with reference sequences from Angola (Fig. 2). When compared to the consensus genotype E sequence, LAM but no TDF resistance mutations were detected. Analysis from deduced amino acid sequences showed the presence of specific substitutions. Most of the mutations were localized to HLA class I- and II-restricted epitopes, CD4+ T-, CD8+ T-, and B-cells immune epitopes (Table 1). With the absence of TDF mutation, the decision was to continue with TDF-treatment. TDF dosage was further adjusted to 300 mg after 141 weeks of TDF rescue-therapy when body weight was above 35 kg. Between 113 to 141 weeks of TDF rescue-therapy, another two events of VBT were observed, with the overall trend of decreasing serum HBV DNA, and progressively declining serum AST and ALT activities. However, the patient remained HBeAg-positive, HBsAg-positive and HBsAb-negative throughout his drug therapy (Fig. 1).

Phylogenetic analysis of HBV full-length sequence isolated from paediatric patient. A midpoint rooted phylogenetic tree constructed by maximum likelihood using RaxML is supported by bootstrap values performed at 1000 replicates with a cut off value of 80%. The reference strains from GenBank are designated by their accession number and the country of origin/isolation. The tree is rooted to an outlier sequence of genotype B from Vietnam. The sequenced isolate OM256457 is shown in red with a grey background
The HDV RNA PCR test was repeated when the low viral load persisted after 141 weeks of TDF treatment. The second HDV PCR test was also negative. In view of the recognised TDF associated nephrotoxicity, renal function was regularly monitored by use of urinalysis, serum urea & electrolytes, serum phosphorus, magnesium, calcium, creatinine and calculation of estimated glomerular filtration rate (eGFR) [31]. Values of all these parameters were normal throughout the patient’s follow-up and will continue to be monitored while the patient remains on TDF. Since prolonged low HBV viremia is associated with a higher risk of HCC, the patient will be continuously monitored until the treatment target is reached.
Discussion and conclusion
The infection of the child, even though he had been vaccinated against HBV, was possible, especially considering his mother was HBV-positive, the child was diagnosed with ALL, had received a blood transfusion and was treated with the Berlin-Frankfurt-Munich (BFM)-95 regimen. Furthermore, mutations in the HBV isolated may be responsible for persistence of the virus and immune escape despite treatment with LAM and TDF.
Phylogenetic analysis revealed the child was infected with genotype E HBV, which is prevalent in West and Central Africa [32]. All genotype E strains have the same characteristics: an in-frame deletion of three nucleotides (one amino acid) in the 5′-pre-S1, a signature pattern of amino acids in the pre-S1 region and the serological subtype ayw4. Another unique attribute of genotype E strains is the introduction of another start codon Met83 in the pre-S1 region that may result in the translation of an elongated middle hepatitis B surface protein [33]. Moreover, the HBV sequence clustered with sequences of the southwest African origin (Angola, Namibia, and DRC), which have unique mutations of T57I in the s gene and V30L in the x gene [29, 34].
From the child’s history, two routes of transmission can be implicated: either mother-to-child transmission, considering the mother was diagnosed with CHB or transmitted by the blood transfusion received in Angola, before the diagnosis of ALL. There is a possibility that the child infected the mother. As the mother had spontaneously resolved the infection, we were unable to isolate and sequence HBV from her blood, to determine the infecting genotype. HBV seroprevalence among blood donors in Angola has been reported to be relatively high at 6.74% [35] and thus the blood transfusion may be a possible source of the infection. In most sub-Saharan African countries, including Angola, quality assurance of screening transfusion transmissible infections remains a key challenge to ensure blood safety. In countries with resource limitations, rapid diagnostic tests with lower sensitivity and specificity are extensively used, including hepatitis B core antibody testing (anti-HBc) at the exclusion of more sensitive HBV nucleic acid testing [36]. Furthermore, the strain of HBV isolated from the child was found to co-cluster with HBV isolated previously from Angola and to share signature amino acids of that clade (Fig. 2) [29, 30].
Treatment for ALL ended in November 2013 and HBV infection and its clinical manifestations, including ALT elevations (Fig. 1), were evident 16 months later, when the immune reconstitution would have commenced. ALL is known to be immunosuppressive and 52% of pediatric hematologic malignancy patients lose immunity against HBV [37]. Moreover, anti-neoplastic treatments suppress cellular and humoral immunity in children with ALL during chemotherapy and long term remission [38,39,40]. The majority of Korean pediatric ALL patients (78%) lost anti-HBs after chemotherapy [41]. The BFM-95 protocol administered is immunosuppressive, with methotrexate suppressing the B-cell compartment [42], and cyclophosphamide and cytarabine depleting early linkage T-cells, and affecting T-cell proliferation [43]. From this case it is evident that even though the child had been vaccinated, it is important for practicing oncologists in HBV endemic areas to actively screen pre-chemotherapy patients for HBV, administer antiviral prophylaxis to reduce the incidence of reactivation or infection [44]. Reactivation of HBV infection is a well-described complication associated with hematologic disorder patients undergoing chemotherapy treatment. Viral reactivation can arise in post-initiation, between the treatment cycle and post-therapy [45]. Even during the immune reconstitution period, ALL children in remission have defective humoral and cellular immunity and are more predisposed to acquire severe infection [46,47,48]. Younger children experience a longer period of immune suppression and prominent delayed B-cell recovery [49,50,51]. This leads to vaccine-acquired immunological memory loss, diminished immunoglobulin titers to a level below protection and restricted immune functions [52].
To achieve persistent infection, HBV exploits different strategies to evade the host’s adaptive immunity by targeting the CD4+ T-, CD8+ T-, regulatory T-, and B-cells [53]. A weaker CD4+ T-cell response will promote the accumulation of a mutant strain, immune escape, and prolong persistence. Amino acid substitutions, which are significantly associated with liver disease progression from the inactive carrier through CHB to cirrhosis and/or HCC [54], were identified in the B-cell, T-cell, HLA class I, and II-restricted epitopes of HBV (Table 1). These substitutions can affect the binding affinity and interaction of antigenic peptides to both the presenting HLA epitopes and T-cell receptors, altering immune recognition, and affecting priming, activation, and proliferation of HBV specific CD4+ T-cells [55] and CD+ 8 T-cells [56]. This will affect B-cell activation, clonal expansion, and differentiation, decreasing neutralizing immunoglobulin production and delaying viral clearance.
preS1N97K is located within the overlapping B-cell /T-cell epitope region [57, 58], which is frequently mutated in HBV from CHB patients [54]. Similar to preS1, the preS2 also encompasses immune-dominant B- and T-cell epitopes [59, 60]. In particular, preS2 residues 6–8 (STT) are essential to maintain stable antigenic structure in this region [61]. Thus, the preS2T7I can affect the hydrophilicity and reduce antigenicity. sP52L is inside the HLA class I-restricted epitope of the HBsAg [62]. It was previously found in HBV isolated from immunosuppressed post-liver transplant patients with subsequent recurrence of HBV infection, following anti-HBs immunoglobulin treatment [63], from a HBsAg-positive HCC patient [64] and from vaccinated children in Taiwan [65]. Three mutations, namely xV30L, xD36G, and xA47T mapped to the B-cell epitope of HBx protein (residue 29–48) [66]. These mutations are frequently found in HBV isolated from HCC patients [54]. Residue 64 in the core gene maps to a well-characterized main immune dominant CD4 + T-cell epitope [67]. cE64D was previously reported to reduce T-cell proliferation in vitro [55] and correlated to HBV-associated liver disease progression [68]. The cL100I mutation is found within the overlapping CD4+ T- and CD8+ T-cell epitope of core gene. This mutation is believed to develop under selection pressure from the T-cells to escape the immune clearance [69].
The residual viremia observed at 36 weeks (~ 8 months) after initiation of LAM, was indicative of PVR (Fig. 1). This inadequate response, a good predictor for VBT [70], is a result of the development of resistance mutations in response to selective pressure [71]. In fact, in addition to the immune escape mutations, two lesser-known LAM resistance mutations (rtS256G and rtM267L) developed (Table 1), which were previously identified in LAM-failed CHB patients [72]. Their spatial proximity close to the active site of reverse transcriptase (RT) domain may be responsible for the development of LAM resistance [72]. Within one year of LAM treatment, 34 to 65% of children treated with LAM can develop LAM resistance mutations [73, 74] and 25.9% VBT [75]. However, because of its low cost, safety and ease of oral administration compared to interferon-α therapy, LAM may be the only choice for first-line hepatitis B therapy for children younger than 12 years in developing countries [76]. In this case, close monitoring is advised.
TDF has the highest antiviral activity and resistance barrier of all available NA treatments for HBV [77]. It is safe, effective and well-tolerated long-term. Although no renal dysfunction was documented in our patient, TDF has a low but significant risk of kidney injury. Nephrotoxicity is characterised by a proximal renal tubular dysfunction resembling Fanconi syndrome with hypophosphatemia, hypouricemia, aminoaciduria and glycosuria. TDF nephrotoxicity can manifest as a decrease in GFR and may be associated with acute kidney injury or chronic kidney injury. Regular monitoring of proximal tubular function and serum creatinine clearance is required to minimize the risk [31]. TDF is used as monotherapy [78] both in adults and children, with 100% viral clearance at 96 weeks (22 months) treatment [79, 80]. However, in the present case a reasonable response occurred only after two VBT events at 113 weeks (26 months) and 141 weeks (32 months) of TDF treatment, respectively (Fig. 1). This response is longer than that observed in genotype E HBeAg-positive infected individuals, who achieved undetectable viral load in 52 weeks (12 months), 100% response rate in 15–18 months therapy, 85.7% ALT normalized in 12 months and 100% ALT normalized in 18 months [81]. However, PVR has been documented previously, where 18% HBeAg-positive patients showed PVR after 48 weeks (11 months) TDF treatment [82]. There are a number of reasons that can account for PVR and VBT to TDF. One controversial study reported VBT associated with TDF resistance mutations [83]. However, this was not the case in the present study because no TDF mutations were detected (Table 1). It is possible that the high viral loads before initiation and at 12 weeks (3 months) of treatment may be responsible. Pre-treatment HBeAg positivity, high baseline HBV DNA (viral load ≥6.34 log 10 IU/mL), and 3rd month (viral load ≥1.91 log 10 IU/mL) are recognized as predictive factors for non-response during TDF therapy [82]. The observed multiple incidences of VBT and PVR in this pediatric patient can be attributed to the underlying delay/partial immune reconstitution from chemotherapy for ALL and the presence of immune escape mutations described above. However, the most common TDF VBT is related to non-compliance [78]. Unfortunately, the test for compliance is not available in South Africa to preclude this. As a precautionary measure, parents of the patient were educated on the importance of therapy compliance.
This case report describes an ALL paediatric patient, who developed genotype E CHB and when treated with LAM followed by TDF, showed PVR and VBT. Although TDF is an effective rescue therapy for patients who do not respond to LAM, it is important that the treatment is prolonged, especially in immunocompromised cases, in order to achieve the desired response of viral clearance. Moreover, it is important that children initiating chemotherapy for ALL are screened for immunization against HBV, even if they had previously been vaccinated for HBV infection, especially in endemic areas.
Availability of data and materials
All the information supporting our conclusions and relevant references are included in the manuscript. The dataset generated and/or analysed during the current study is available in the GenBank repository https://www.ncbi.nlm.nih.gov/genbank/ [Accesssion number: OM256457].
Abbreviations
- ALT:
-
Alanine aminotransferase
- ALL:
-
Acute lymphoblastic leukemia
- AST:
-
Serum aspartate aminotransferase
- BFM:
-
Berlin-Frankfurt-Munich
- CHB:
-
Chronic Hepatitis B
- HBV:
-
Hepatitis B virus
- HDV:
-
Hepatitis D virus
- HCC:
-
Hepatocellular carcinoma
- LAM:
-
Lamivudine
- NA:
-
Nucleot(s)ides analogue (NA)
- PVR:
-
Partial virologic response
- TDF:
-
Tenofovir disoproxil fumarate
- VBT:
-
Virologic breakthrough
References
Shah U, Kelly D, Chang M-H, Fujisawa T, Heller S, González-Peralta RP, et al. Management of Chronic Hepatitis B in children. J Pediatr Gastroenterol Nutr. 2009;48(4):399–404.
Hong M, Bertoletti A. Tolerance and immunity to pathogens in early life: insights from HBV infection. Semin Immunopathol. 2017;39(6):643–52.
MacLachlan JH, Cowie BC. Hepatitis B virus epidemiology. Cold Spring Harb Perspect Med. 2015;5(5):a021410.
Kramvis A. The clinical implications of hepatitis B virus genotypes and HBeAg in pediatrics. Rev Med Virol. 2016;26(4):285–303.
Fattovich G, Bortolotti F, Donato F. Natural history of chronic hepatitis B: special emphasis on disease progression and prognostic factors. J Hepatol. 2008;48(2):335–52.
Lok ASF, Lai C-L. A longitudinal follow-up of asymptomatic hepatitis B surface antigen-positive chinese children. Hepatology. 1988;8(5):1130–3.
Esparza SD, Sakamoto KM. Topics in pediatric leukemia--acute lymphoblastic leukemia. MedGenMed. 2005;7(1):23.
Kato M, Manabe A. Treatment and biology of pediatric acute lymphoblastic leukemia. Pediatr Int. 2018;60(1):4–12.
Chiaretti S, Zini G, Bassan R. Diagnosis and subclassification of acute lymphoblastic leukemia. Mediterr J Hematol Infect Dis. 2014;6(1):e2014073.
Pui C-H, Evans WE. A 50-year journey to cure childhood acute lymphoblastic leukemia. Semin Hematol. 2013;50(3):185–96.
Young LS. Management of Infections in Leukemia and Lymphoma. In: Rubin RH, Young LS, Van Furth R, editors. Clinical Approach to Infection in the Compromised Host. Boston, MA: Springer US; 2002. p. 497–526.
Chandran, R. , Hakki, M. , Spurgeon, S. . Infections in Leukemia. In: Azevedo, L. , editor. Sepsis - An Ongoing and Significant Challenge [Internet]. London: IntechOpen; 2012 [cited 2022 Mar 15]. Available from: https://www.intechopen.com/chapters/39664. https://doi.org/10.5772/50193.
Inaba H, Pei D, Wolf J, Howard SC, Hayden RT, Go M, et al. Infection-related complications during treatment for childhood acute lymphoblastic leukemia. Ann Oncol. 2017;28(2):386–92.
Afzal S, Ethier MC, Dupuis LL, Tang L, Punnett AS, Richardson SE, Allen U, Abla O, Sung L. Risk factors for infection-related outcomes during induction therapy for childhood acute lymphoblastic leukemia. Pediatr Infect Dis J. 2009;28(12):1064-8.
Katsimpardi K, Papadakis V, Pangalis A, Parcharidou A, Panagiotou JP, Soutis M, et al. Infections in a pediatric patient cohort with acute lymphoblastic leukemia during the entire course of treatment. Support Care Cancer. 2006;14(3):277–84.
Busca A. Viral infections in patients with hematological malignancies. Leuk Suppl. 2012;1(Suppl 2):S24–5.
O’Connor D, Bate J, Wade R, Clack R, Dhir S, Hough R, et al. Infection-related mortality in children with acute lymphoblastic leukemia: an analysis of infectious deaths on UKALL2003. Blood. 2014;124(7):1056–61.
Cowan DH, Kouroupis GM, Leers WD. Occurrence of hepatitis and hepatitis B surface antigen in adult patients with acute leukemia. Can Med Assoc J. 1975;112(6):693–7.
Mansouri N, Movafagh A, Sayad A, Ghafouri-Fard S, Darvish H, Zare-Abdollahi D, et al. Hepatitis B virus infection in patients with blood disorders: a concise review in pediatric study. Iran J Pediatric Hematol Oncol. 2014;4(4):178–87.
Locasciulli A, Santamaria M, Masera G, Schiavon E, Alberti A, Realdi G. Hepatitis B virus markers in children with acute leukemia: the effect of chemotherapy. J Med Virol. 1985;15(1):29–33.
Guruprasad B, Kavitha S, Aruna Kumari BS, Vijaykumar BR, Sumati BG, Mahua S, et al. Risk of hepatitis B infection in pediatric acute lymphoblastic leukemia in a tertiary care center from South India. Pediatr Blood Cancer. 2014;61(9):1616–9.
Moschovi M, Adamaki M, Vlahopoulos SA. Progress in treatment of viral infections in children with acute lymphoblastic leukemia. Oncol Rev. 2016;10(1):300.
Bozza C, Cinausero M, Iacono D, Puglisi F. Hepatitis B and cancer: a practical guide for the oncologist. Crit Rev Oncol Hematol. 2016;98:137–46.
Lampertico P, Agarwal K, Berg T, Buti M, Janssen HLA, Papatheodoridis G, et al. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67(2):370–98.
European Association for the Study of the L. EASL clinical practice guidelines: management of chronic hepatitis B virus infection. J Hepatol. 2012;57(1):167–85.
Lok AS, Zoulim F, Locarnini S, Bartholomeusz A, Ghany MG, Pawlotsky J-M, et al. Antiviral drug-resistant HBV: standardization of nomenclature and assays and recommendations for management. Hepatology. 2007;46(1):254–65.
Günther S, Li BC, Miska S, Krüger DH, Meisel H, Will H. A novel method for efficient amplification of whole hepatitis B virus genomes permits rapid functional analysis and reveals deletion mutants in immunosuppressed patients. J Virol. 1995;69(9):5437–44.
Bell TG, Kramvis A. Fragment merger: an online tool to merge overlapping long sequence fragments. Viruses. 2013;5(3):824–33.
Stamatakis A. RAxML version 8: a tool for phylogenetic analysis and post-analysis of large phylogenies. Bioinformatics. 2014;30(9):1312–3.
Letunic I, Bork P. Interactive tree of life (iTOL) v4: recent updates and new developments. Nucleic Acids Res. 2019;47(W1):W256–9.
Deray G, Buti M, Gane E, Jia J-D, Chan HLY, Craxi A, et al. Hepatitis B virus infection and the kidney: renal abnormalities in HBV patients, antiviral drugs handling, and specific follow-up. Adv Hepatol. 2015;2015:596829.
Kramvis A, Kew MC. Epidemiology of hepatitis B virus in Africa, its genotypes and clinical associations of genotypes. Hepatol Res. 2007;37(s1):S9–S19.
Kramvis A, Restorp K, Norder H, Botha JF, Magnius LO, Kew MC. Full genome analysis of hepatitis B virus genotype E strains from South-Western Africa and Madagascar reveals low genetic variability. J Med Virol. 2005;77(1):47–52.
Lago BV, Mello FC, Ribas FS, Valente F, Soares CC, Niel C, et al. Analysis of complete nucleotide sequences of Angolan hepatitis B virus isolates reveals the existence of a separate lineage within genotype E. PLoS One. 2014;9(3):e92223.
Apata IW, Averhoff F, Pitman J, Bjork A, Yu J, Amin NA, et al. Centers for disease C et al: Progress toward prevention of transfusion-transmitted hepatitis B and hepatitis C infection--sub-Saharan Africa, 2000-2011. MMWR Morb Mortal Wkly Rep. 2014;63(29):613–9.
Weimer A, Tagny CT, Tapko JB, Gouws C, Tobian AAR, Ness PM, et al. Blood transfusion safety in sub-Saharan Africa: a literature review of changes and challenges in the 21st century. Transfusion. 2019;59(1):412–27.
Zignol M, Peracchi M, Tridello G, Pillon M, Fregonese F, D'Elia R, et al. Assessment of humoral immunity to poliomyelitis, tetanus, hepatitis B, measles, rubella, and mumps in children after chemotherapy. Cancer. 2004;101(3):635–41.
Katz J, Walter BN, Bennetts GA, Cairo MS. Abnormal cellular and humoral immunity in childhood acute lymphoblastic leukemia in long-term remission. West J Med. 1987;146(2):179–87.
Perkins JL, Harris A, Pozos TC. Immune dysfunction after completion of childhood leukemia therapy. J Pediatr Hematol Oncol. 2017;39(1):1–5.
Smith S, Schiffman G, Karayalcin G, Bonagura V. Immunodeficiency in long-term survivors of acute lymphoblastic leukemia treated with Berlin-Frankfurt-Münster therapy. J Pediatr. 1995;127(1):68–75.
Choi YB, Lee NH, Yi ES, Kim Y-J, Koo HH. Changes in hepatitis B antibody status after chemotherapy in children with acute lymphoblastic leukemia. Pediatr Blood Cancer. 2019;66(12):e27904.
Bertino JR. Karnofsky memorial lecture. Ode to methotrexate. J Clin Oncol. 1993;11(1):5–14.
Singh N, Perazzelli J, Grupp SA, Barrett DM. Early memory phenotypes drive T cell proliferation in patients with pediatric malignancies. Sci Transl Med. 2016;8(320):320ra323.
Hoofnagle JH. Reactivation of hepatitis B. Hepatology. 2009;49(S5):S156–65.
Wang B, Mufti G, Agarwal K. Reactivation of hepatitis B virus infection in patients with hematologic disorders. Haematologica. 2019;104(3):435–43.
Brodtman DH, Rosenthal DW, Redner A, Lanzkowsky P, Bonagura VR. Immunodeficiency in children with acute lymphoblastic leukemia after completion of modern aggressive chemotherapeutic regimens. J Pediatr. 2005;146(5):654–61.
Geerlinks AV, Issekutz T, Wahlstrom JT, Sullivan KE, Cowan MJ, Dvorak CC, et al. Severe, persistent, and fatal T-cell immunodeficiency following therapy for infantile leukemia. Pediatr Blood Cancer. 2016;63(11):2046–9.
Kosmidis S, Baka M, Bouhoutsou D, Doganis D, Kallergi C, Douladiris N, et al. Longitudinal assessment of immunological status and rate of immune recovery following treatment in children with ALL. Pediatr Blood Cancer. 2008;50(3):528–32.
Caver TE, Slobod KS, Flynn PM, Behm FG, Hudson MM, Turner EV, et al. Profound abnormality of the B/T lymphocyte ratio during chemotherapy for pediatric acute lymphoblastic leukemia. Leukemia. 1998;12(4):619–22.
van Tilburg CM, van der Velden VHJ, Sanders EAM, Wolfs TFW, Gaiser JF, de Haas V, et al. Reduced versus intensive chemotherapy for childhood acute lymphoblastic leukemia: impact on lymphocyte compartment composition. Leuk Res. 2011;35(4):484–91.
Layward L, Levinsky RJ, Butler M. Long-term abnormalities in T and B lymphocyte function in children following treatment for acute lymphoblastic Leukaemia. Br J Haematol. 1981;49(2):251–8.
van Tilburg CM, Sanders EAM, Rovers MM, Wolfs TFW, Bierings MB. Loss of antibodies and response to (re-)vaccination in children after treatment for acute lymphocytic leukemia: a systematic review. Leukemia. 2006;20(10):1717–22.
Ortega-Prieto AM, Dorner M. Immune evasion strategies during chronic hepatitis B and C virus infection. Vaccines (Basel). 2017;5(3):24.
Ghosh S, Mondal RK, Banerjee P, Nandi M, Sarkar S, Das K, et al. Tracking the naturally occurring mutations across the full-length genome of hepatitis B virus of genotype D in different phases of chronic e-antigen-negative infection. Clin Microbiol Infect. 2012;18(10):E412–8.
Torre F, Cramp M, Owsianka A, Dornan E, Marsden H, Carman W, et al. Direct evidence that naturally occurring mutations within hepatitis B core epitope alter CD4+ T-cell reactivity. J Med Virol. 2004;72(3):370–6.
Timm J, Walker CM. Mutational escape of CD8+ T cell epitopes: implications for prevention and therapy of persistent hepatitis virus infections. Med Microbiol Immunol. 2015;204(1):29–38.
Ferrari C, Cavalli A, Penna A, Valli A, Bertoletti A, Pedretti G, et al. Fine specificity of the human T-cell response to the hepatitis B virus preS1 antigen. Gastroenterology. 1992;103(1):255–63.
Zhang A-Y, Lai C-L, Huang F-Y, Seto W-K, Fung J. Wong DK-H, Yuen M-F: evolutionary changes of hepatitis B virus pre-S mutations prior to development of hepatocellular carcinoma. PLoS One. 2015;10(9):e0139478.
Milich DR, McLachlan A, Thornton GB, Hughes JL. Antibody production to the nucleocapsid and envelope of the hepatitis B virus primed by a single synthetic T cell site. Nature. 1987;329(6139):547–9.
Milich DR, McLachlan A, Chisari FV, Kent SB, Thorton GB. Immune response to the pre-S(1) region of the hepatitis B surface antigen (HBsAg): a pre-S(1)-specific T cell response can bypass nonresponsiveness to the pre-S(2) and S regions of HBsAg. J Immunol. 1986;137(1):315.
Myung Kyu L, Kil Lyong K, Kyung-Soo H. Evaluation of N-terminal role in peptide antigenicity of the PreS2 region of the hepatitis B virus surface antigen. Mol Cells. 1997;7(3):340–6.
Chisari FV, Ferrari C. Hepatitis B virus Immunopathogenesis. Annu Rev Immunol. 1995;13(1):29–60.
Grottola A, Buttafoco P, Del Buono MG, Cremonini C, Colantoni A, Gelmini R, et al. Pretransplantation pre-S2 and S protein heterogeneity predisposes to hepatitis B virus recurrence after liver transplantation. Liver Transpl. 2002;8(5):443–8.
Pollicino T, Raffa G, Costantino L, Lisa A, Campello C, Squadrito G, et al. Molecular and functional analysis of occult hepatitis B virus isolates from patients with hepatocellular carcinoma. Hepatology. 2007;45(2):277–85.
Lin Y-M, Jow G-M, Mu S-C, Chen B-F. Naturally occurring hepatitis B virus B-cell and T-cell epitope mutants in hepatitis B vaccinated children. ScientificWorldJournal. 2013;2013:571875.
Park OY, Jin YH, Lee M, Shin H-J, Kim H-I, Cho H, et al. Characterization and gene cloning of monoclonal antibody specific for the hepatitis B virus X protein. Hybridoma. 2000;19(1):73–80.
Ferrari C, Bertoletti A, Penna A, Cavalli A, Valli A, Missale G, et al. Identification of immunodominant T cell epitopes of the hepatitis B virus nucleocapsid antigen. J Clin Invest. 1991;88(1):214–22.
Al-Qahtani AA, Al-Anazi MR, Nazir N, Abdo AA, Sanai FM, Al-Hamoudi WK, et al. The correlation between hepatitis B virus Precore/Core mutations and the progression of severe liver disease. Front Cell Infect Microbiol. 2018;8:355.
Ehata T, Omata M, Yokosuka O, Hosoda K, Ohto M. Variations in codons 84-101 in the core nucleotide sequence correlate with hepatocellular injury in chronic hepatitis B virus infection. J Clin Invest. 1992;89(1):332–8.
Alam S, Azam G, Mustafa G, Ahmad N, Islam B, Podder PK, et al. Pretreatment and on-treatment predictors of viral breakthrough in lamivudine therapy for chronic hepatitis B. Hepatol Int. 2008;2(4):494–7.
Kasırga E. Lamivudine resistance in children with chronic hepatitis B. World J Hepatol. 2015;7(6):896–902.
Banerjee P, Chakraborty A, Mondal RK, Khatun M, Datta S, Das K, et al. HBV quasispecies composition in lamivudine-failed chronic hepatitis B patients and its influence on virological response to Tenofovir-based rescue therapy. Sci Rep. 2017;7:44742.
Ni Y-H, Huang F-C, Wu T-C, Kong M-S, Jeng Y-M, Chen P-J, et al. Lamivudine treatment in maternally transmitted chronic hepatitis B virus infection patients. Pediatr Int. 2005;47(4):372–7.
Hartman C, Berkowitz D, Eshach-Adiv O, Hino B, Rimon N, Satinger I, et al. Long-term lamivudine therapy for chronic hepatitis B infection in children unresponsive to interferon. J Pediatr Gastroenterol Nutr. 2006;43(4):494–8.
Hong SJ, Kim YH, Choe B-H, Park HJ, Tak W-Y, Kweon Y-O. Current role of lamivudine regarding therapeutic response and resistance in children with chronic hepatitis B. Pediatr Gastroenterol Hepatol Nutr. 2013;16(2):80–8.
Sokal EM, Paganelli M, Wirth S, Socha P, Vajro P, Lacaille F, et al. Management of chronic hepatitis B in childhood: ESPGHAN clinical practice guidelines consensus of an expert panel on behalf of the European Society of Pediatric Gastroenterology, Hepatology and nutrition. J Hepatol. 2013;59(4):814–29.
Paganelli M, Stephenne X, Sokal EM. Chronic hepatitis B in children and adolescents. J Hepatol. 2012;57(4):885–96.
Jeon H-J, Jung SW, Park NH, Yang Y, Noh J-H, Ahn J-S, et al. Efficacy of tenofovir-based rescue therapy for chronic hepatitis B patients with resistance to lamivudine and entecavir. Clin Mol Hepatol. 2017;23(3):230–8.
Marcellin P, Zoulim F, Hézode C, Causse X, Roche B, Truchi R, et al. Effectiveness and safety of Tenofovir Disoproxil Fumarate in chronic hepatitis B: a 3-year, prospective, real-world study in France. Dig Dis Sci. 2016;61(10):3072–83.
Choe JY, Ko JS, Choe B-H, Kim JE, Kang B, Lee KJ, et al. Antiviral efficacy of Tenofovir Monotherapy in children with Nucleos(t)ide-naive chronic hepatitis B. J Korean Med Sci. 2018;33(2): e11
Cuenca-Gómez JÁ, Lozano-Serrano AB, Cabezas-Fernández MT, Soriano-Pérez MJ, Vázquez-Villegas J, Estévez-Escobar M, et al. Chronic hepatitis B genotype E in African migrants: response to nucleos(t)ide treatment in real clinical practice. BMC Infect Dis. 2018;18(1):568.
Song JE, Lee CH, Kim BS. Efficacy of long-term tenofovir disoproxil fumarate therapy in chronic hepatitis B patients with partial virologic response in real practice. Korean J Intern Med. 2019;34(4):802–10.
Cho WH, Lee HJ, Bang KB, Kim SB, Song IH. Development of tenofovir disoproxil fumarate resistance after complete viral suppression in a patient with treatment-naïve chronic hepatitis B: a case report and review of the literature. World J Gastroenterol. 2018;24(17):1919–24.
Acknowledgements
The authors thank Dr. Bernard Goodwin, Consultant, Paediatric Haematology and Oncology, Charlotte Maxeke Johannesburg Academic Hospital, for assistance with retrieval of records on diagnosis and treatment of acute lymphoid leukemia of the case.
Funding
National Research Foundation of South Africa (UGN #65530 and UGN #93516), University of the Witwatersrand. Cancer Association of South Africa (CANSA). The funders had no involvement in conduct of the research and/or preparation of the article.
Author information
Authors and Affiliations
Contributions
CYC carried out all experimental work and wrote the first draft of the manuscript; CH treated the patient, analyzed and interpreted the patient data regarding the chronic hepatitis B and recognized the uniqueness of the case; PW treated the patient, analyzed and interpreted the patient data regarding the chronic hepatitis B; LAIO carried out the phylogenetic analyses; ES was the consulting hepatologist who treated the mother and he provided insight on interpretation of patient data; AK was involved in study supervision, conceptualization of the laboratory work, providing resources and funding, critical review and revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent to participate in this study was obtained from the mother of the patient. The study was approved by the Human Research Ethics Committee (Medical), University of the Witwatersrand, South Africa. The protocol number is M18110.8.
Consent for publication
Informed written consent was obtained from the patient’s mother for the publication of this study.
Competing interests
The authors declare they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, CY., Hajinicolaou, C., Walabh, P. et al. Molecular characterization of hepatitis B virus (HBV) isolated from a pediatric case of acute lymphoid leukemia, with a delayed response to antiviral treatment: a case report. BMC Pediatr 22, 168 (2022). https://doi.org/10.1186/s12887-022-03204-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-022-03204-6