
Abstract
Introduction
In the United States (US), racial and socioeconomic disparities have been implicated in pediatric intensive care unit (PICU) admissions and outcomes, with higher rates of critical illness in more deprived areas. The degree to which this persists despite insurance coverage is unknown. We investigated whether disparities exist in PICU admission and mortality according to socioeconomic position and race in children receiving Medicaid.
Methods
Using Medicaid data from 2007–2014 from 23 US states, we tested the association between area level deprivation and race on PICU admission (among hospitalized children) and mortality (among PICU admissions). Race was categorized as Black, White, other and missing. Patient-level ZIP Code was used to generate a multicomponent variable describing area-level social vulnerability index (SVI). Race and SVI were simultaneously tested for associations with PICU admission and mortality.
Results
The cohort contained 8,914,347 children (23·0% Black). There was no clear trend in odds of PICU admission by SVI; however, children residing in the most vulnerable quartile had increased PICU mortality (aOR 1·12 (95%CI 1·04–1·20; p = 0·0021). Black children had higher odds of PICU admission (aOR 1·04; 95% CI 1·03–1·05; p < 0·0001) and higher mortality (aOR 1·09; 95% CI 1·02–1·16; p = 0·0109) relative to White children. Substantial state-level variation was apparent, with the odds of mortality in Black children varying from 0·62 to 1·8.
Conclusion
In a Medicaid cohort from 2007–2014, children with greater socioeconomic vulnerability had increased odds of PICU mortality. Black children were at increased risk of PICU admission and mortality, with substantial state-level variation. Our work highlights the persistence of sociodemographic disparities in outcomes even among insured children.
Similar content being viewed by others


Introduction
Background
There is substantial evidence from the United States (US) of disparities in incidence and outcome of childhood critical illness by race, ethnicity and socioeconomic position [1, 2]. Disparities in mortality according to race (as a social construct and a proxy for individual or systemic racism) have been reported in critically ill children with oncologic diagnoses and sepsis [1, 3,4,5]. However, the association of race with mortality has not been consistently reported, and inclusion of severity of illness or related socioeconomic variables, such as insurance status and access to healthcare, can affect the reported relationship [6, 7]. Admission to the pediatric intensive care unit (PICU) is often used either as evidence of illness severity, and occasionally as inclusion criteria for a study. However, this creates a selection bias if PICU admission itself is impacted by race. Evidence regarding disparities in PICU admission according to race and/or ethnicity show mixed results [8,9,10]. Overall, accuracy of recorded of race, ethnicity and socioeconomic position, unintentional selection biases, and inconsistent control for confounders contribute to conflicting results across studies [11, 12].
One important plausible confounder of the association between race and outcomes (PICU admission or mortality) is the social vulnerability of the area where a child resides, which is intrinsically linked to racism and socioeconomics in the US [13]. The most common reasons for PICU admission are respiratory illness [14, 15], congenital illness [14], and injury or poisoning [14, 15]. Prior studies from the US have shown higher rates of PICU admission in children residing in more socioeconomically deprived areas [16,17,18,19], and certain common PICU diagnoses, specifically severe asthma and traumatic injuries, are also associated with socioeconomic deprivation [20, 21].
Prior research has yielded conflicting evidence on the role of neighborhood-level socioeconomic position and race and/or ethnicity on rates of PICU admissions and outcomes, highlighting a significant gap in our understanding of these dynamics [1, 2]. This ambiguity underscores the need for targeted investigation into how specific racial disparities influence these healthcare metrics.
Objectives
We analyzed a multistate Medicaid database, aiming to isolate the effects of social vulnerability and race on PICU admission and mortality. We reasoned that using a Medicaid database would restrict our analysis to children with a baseline level of access to public insurance, thus minimizing access due to insurance as a potential confounder or mediator of any reported associations. Recognizing Medicaid's state-level administration, we also consider the potential for state-specific variations to elucidate the complex interplay between state policy, cultural milieu, sociodemographic factors and outcomes. We acknowledge the significant changes in healthcare access and policy, particularly post-ACA, and the shifting perceptions regarding race as a social construct following recent societal events. Although this study looks at data which is 10 years old, this paper can still provide a useful benchmark for future research using more recent data. We hypothesised that racial disparities exist in PICU admission rates and mortality, influenced by area-level socioeconomic vulnerability.
Methods
Design and setting
This was a population-based, retrospective cohort study, using Medicaid Analytic eXtract (MAX) data maintained by the Centers for Medicare and Medicaid Services from the years 2007 to 2014. MAX includes person-level claims on Medicaid demographics, eligibility, and utilization on individuals with qualifying socioeconomic status. Medicaid, one of the largest healthcare payers in the United States, covers approximately 37% of children. We chose to use MAX rather than more recent (2015 and later) Transformed Medicaid Statistical Information Systems (T-MSISs) because MAX provided extensive quality-control, data validation, and harmonization at the federal level, permitting a cleaner multistate analysis; by comparison, T-MSIS data quality and validation varies by state. We included states based on data availability and quality for the years studied. Quality was assessed by how complete the data were longitudinally over time, and whether managed care claims were available in the dataset, versus just including information on enrolment of children in a managed care plan [22, 23]. Variables were assessed using individual variable quality reports [24].
Data sources
We used Medicaid data from 23 US states (Arizona, Arkansas, Connecticut, Georgia, Hawaii, Indiana, Iowa, Louisiana, Michigan, Minnesota, Mississippi, Missouri, New York, Ohio, Oklahoma, Oregon, South Dakota, Tennessee, Utah, Vermont, Virginia, Washington and Wyoming) from the years 2007 to 2014.
Participants
The study population included patients under 21 years of age (who had not yet reached their 21st birthday) in the MAX database from 2007 to 2014. Neonates managed in the NICU were excluded from the study by excluding patients with the neonatal CPT codes (appendix 1).
PICU population was defined by using CPT codes and revenue codes (appendix 1). Revenue codes have been shown in the adult population to be a sensitive and specific way of identifying an ICU population [25].
Variables
The co-primary independent variables under investigation were area-level social vulnerability index (SVI) and race. We selected SVI because it encompasses a comprehensive set of indicators across multiple domains of socioeconomic status, which allowed us to see what aspects of deprivation are more closely associated with PICU admission and outcome. Socioeconomic position was defined using patient-level ZIP Code to extract socioeconomic variables from the CDC/ATSDR SVI, allowing us to generate a multicomponent variable describing area-level SVI [26]. The SVI uses 16 variables from the US census data to determine the social vulnerability of every census tract. Variables are grouped into the following four themes. 1) socioeconomic (below poverty, unemployed, income, no high school diploma, 2) household composition/disability (aged 65 and over, aged 17 and younger, civilian with a disability, single-parent household), 3) minority status/language (minority, speaks English “Less than Well”), 4) housing type/transportation (multi-unit structures, mobile homes, crowding, no vehicle, group quarters). We report composite SVI as the main area-level socioeconomic exposure, but also separately analyzed each of the four themes above. A higher SVI score indicates higher vulnerability (quartile 1 least vulnerable and quartile 4 most vulnerable).
Race was categorized as Black, White, Other, or Missing. These were examined separately in univariable analyses and then included together in models. Due to substantial state-level inconsistencies regarding the availability and accuracy of ethnicity coding (Hispanic/Latino versus not Hispanic/Latino), we could not reliably capture Hispanic/Latino ethnicity. Hispanic patients are included in the “other” category.
The primary outcome was any PICU admission during the 8 years of the analysis. The secondary outcome was mortality (patient disposition codes 20,40,41 and 42 were flagged as death) in an analysis restricted to PICU patients.
Other included variables based on relevant individual variables (age categories, sex, presence of complex chronic condition (as defined by Feudtner [27]) reason for being on Medicaid (poverty, expansion waver, CASH or other). Federal Information Processing System (FIPS) codes (numbers which uniquely identify counties and county equivalents in the United States average population 100,000) were included as a random effect in the overall and state-specific models.
Sample size
A pragmatic approach was taken, and all eligible records were used. No formal sample size calculation was done.
Statistical methods
Descriptive statistics were used to characterize the cohort. For composite SVI and race, and separately for each of the four component SVI themes, univariate and multivariable logistic regression were used to test for association with PICU admission and PICU mortality. SVI and race were modelled together in the main analyses. FIPS (i.e., local geographic area) was modelled as a random effect. We performed separate regressions for the entire cohort and individually by state to investigate state-level variability. In the analysis by state some models failed to converge with FIPS as a random effect due to small numbers in some local geographic areas; in those states, effect estimates are presented without accounting for FIPS.
A pre-planned interaction tests were done to assess whether there was any evidence of effect modification of race by SVI.
The amount of missing data on race and ethnicity varied substantially by state, with South Dakota and Connecticut recording no missing data on race or ethnicity and Iowa recording 50·5% patients with missing ethnicity. Most states had < 10% missing data (supplemental Table 1 and supplemental Fig. 1)· There was no missing data for patient age and sex, and 1.7% of the cohort were missing data on ZIP Code. The percentage of records missing area level socioeconomic variables was 9·8% which again varied substantially by state (supplemental Table 1). Because of conceptual limitations introduced by imputing missing race or SVI with incomplete information (e.g., without surnames), we restricted our analyses to analyses where race or SVI were not missing. Analyses were done using SAS version 9.4 (2016) and R Core Team (2022).
Ethics approval and consent to participate
The Institutional Review Board of The Children’s Hospital of Philadelphia reviewed this project and declared that it met the criteria for non-human subjects research, compliant with the terms outlined in a data use agreement with the Centers for Medicare and Medicaid Services for use of the data. Because patients were not contacted or identified in the dataset, consent to participate was waived by the Institutional Review Board of The Children’s Hospital of Philadelphia.
Results
Participants
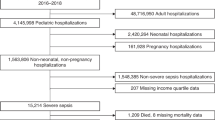
The final cohort included 8,914,347 patients of twenty years of age or less, of whom 425,330 were admitted to PICU between 2007 and 2014 (Table 1). Data from 23 states were included. New York contributed the largest number of patients (n = 1,675,492) and Vermont the least (n = 24,359).
Description of the cohort
Most children in the cohort were less than 1 year of age (57·3% n = 5,106,440), with the median age of the PICU cohort (5 years [IQR 1–15 years]) being older than the non-PICU cohort (median 0 years [IQR 0–13 years]). The prevalence of chronic complex condition was significantly higher in the PICU cohort (69·1%) compared to children not admitted to the PICU (15·9%). Mortality in the PICU cohort was 2·2% compared to 0·1% in the remainder of the cohort (Table 1). In the entire cohort, 23.0% had race recorded as Black and 42·8% as White, 11·9% of the cohort were missing data on race and/or ethnicity, with substantial variation between states (supplemental Fig. 1).
When restricted to PICU admissions, non-survivors were significantly more likely than survivors to be less than 1 year of age (30·5% vs 22·1% respectively) and to have a chronic complex condition (92·4% vs 68·6%) (Table 2). Among PICU survivors, 26·8% were of Black race, while 43·4% were White. Among the children who died, 27·2% were of Black race and 41·8% were White.
There was a clear association between SVI and race: across all states, a higher proportion of Black children resided in the most vulnerable SVI quartile compared to White (Fig. 1).

Proportion of Black and White Children in the Most Deprived Social Vulnerability Quartile by State
Outcomes according to composite SVI
When investigating the association between PICU admission and composite SVI, in univariable analysis there were reduced odds of PICU admission for children living in more deprived quartiles, this was not significant in multivariable analysis (Table 3). Children residing in the most vulnerable quartile had increased PICU mortality (aOR1·12, 95%CI 1·04–1·20; p = 0·002) (Table 4). In the analysis looking at the association of the most vulnerable composite SVI quartile and PICU admission and mortality across states, there was some variability, although not as pronounced as for race (supplemental Fig. 2) for PICU admission.
Outcomes according to individual SVI themes
In the analysis exploring the association between individual SVI themes, PICU admission, and risk of mortality (supplementary Table 2), four key themes were examined: socioeconomic (theme 1), household composition/disability (theme 2), minority status/language (theme 3), and housing type/transportation (theme 4). Divergent results between themes were found for both outcome measures.
For Theme 1 (socioeconomic)multivariable analysis, patients showed increasing odds of PICU admission with higher degrees of vulnerability. When testing the association between social vulnerability and mortality among children admitted to PICU there were non-significant trends towards increased mortality in the more vulnerable quartile compared to the least for socioeconomic vulnerability.
In Theme 2 (household composition/disability), analyses indicated a trend towards lower odds of PICU admission in the more vulnerable quartile. The most vulnerable quartile exhibited a 5% decrease in the odds of admission compared to the least vulnerable quartile (aOR 0·95; 95% confidence interval [CI] 0·94–0·97, p < 0·0001). There was a non-significant trend towards increased mortality in more vulnerable quartiles.
In the analysis for Theme 3 (minority status/language), the most deprived quartile showed a 2% reduction in the odds of PICU admission compared to the least deprived quartile (aOR 0·98; 95% CI 0·96–1·00, p = 0·0179). No significant trend was observed in the analysis for Theme 4 (housing type/transportation). Significantly increased mortality was seen in children residing in the most vulnerable quartile for housing type/transportation compared to the least (aOR 1·09; 95%CI 1·00–1·19 p = 0·0421).
Outcomes according to race
In the fully adjusted multivariable models for all states (with SVI included in the model), Black race was associated with higher odds of PICU admission (aOR 1·04; 95% CI 1·03–1·05; p < 0·0001) (Fig. 2, Table 3). Black race was associated with 1·08 increased odds of mortality once admitted to PICU, compared to White (95% CI 1·01–1·15; p = 0·0176) (Fig. 3, Table 4). When looking at racial disparities in admission and mortality by state, significant variance was seen (Figs. 2 and 3). The state with the highest odds of mortality for Black children, relative to White children, had nearly double the mortality odds (aOR 1·75; 95% CI 1·04–2·97 p = 0·04). There was no evidence of interaction between race and deprivation for the outcome of PICU mortality (p = 0.898). For the outcome of PICU admission the test is significant for the inclusion of an interaction (p < 0.0001. Results are presented stratified in the supplemental material (supplemental Table 3).

Multivariable odds of PICU admission in Black children with White children as reference by state (n = number of hospital admissions for state) (entire cohort n = 9,439,919)

Multivariable odds of PICU mortality in Black children with White children as reference by state (PICU cohort n = 476,886)
Discussion
In our large nationally representative study using data from 2007–2014, we found disparities by race and by SVI for PICU admissions and mortality rates in children covered by Medicaid. Black children had higher odds of both PICU admission and increased risk of mortality once admitted to PICU, even when conditioned on Medicaid and controlling for SVI. Relative odds of PICU admission and mortality in Black children varied according to the state in which they were admitted, with some states showing over 50% increased odds of mortality in Black children. Race was significantly associated with neighborhood SVI, with Black children more likely to reside in more vulnerable ZIP Codes. There was increased mortality observed in PICU in children living in the most vulnerable areas after accounting for race, with higher odds of mortality in children residing in the most vulnerable quartile of housing type/transportation (Theme 4) when analyzing SVI components.
We found limited evidence of an association between PICU admissions and worsening SVI in our multistate analysis, with slightly increased odds of PICU admission in children in the most vulnerable quartile for socioeconomics (Theme 1) and lower odds of PICU admission in the most vulnerable quartile for household composition/disability (Theme 2) and minority status/language (Theme 3). One prior study investigating the area surrounding a single major children’s hospital found that census tracts with the highest rates of childhood poverty had the highest rates of PICU admissions and most PICU bed-day rates [16]. Additionally, worse socioeconomic status has been associated with higher rates of asthma and injury [14, 15], which are two of the most common reasons for admission to the PICU [20, 21]. Deeper analyses into whether specific medical diagnoses or ability to access care despite insurance (e.g., household composition, vehicle ownership) drive associations with PICU admission (either higher or lower odds) are warranted. Specifically, an assessment as to whether household composition/disability and minority status/language represent barriers to recognition of illness severity, and thus lower odds of PICU admission, are indicated.
Our study confirms strong overall and regional trends in racial disparities in outcomes of hospitalized children across the US, with worse outcomes for Black children [3, 4]. The persistence of racial disparities in this cohort, despite restricting to a Medicaid cohort and adjusting for area-level SVI, suggests that racism, either systemic, institutional, or personal, is a strong residual mechanism behind the disparities found. Importantly, the interrelatedness of race, socioeconomic deprivation, healthcare access, and related factors makes it challenging to determine which variables are driving worse outcomes in Black children. The state-level disparities suggest possible effects of state-level variation in Medicaid implementation or in patient case-mix, suggesting that higher PICU admissions and higher mortality for Black children may be modifiable by state-level policies. Our study time-period ends at the time of the 2014 Affordable Care Act (ACA) Medicaid expansion, and future studies assessing longitudinal rates of PICU admission and mortality in Black children in states with and without Medicaid expansion are necessary. Medicaid expansion has been associated with some improved insurance coverage in pediatric oncology in expansion states [28]. Overall, the interaction between states’ economic metrics, racial demographics and Medicaid policy remains understudied in pediatrics.
It is notable that while some signal towards worse outcome is apparent in children from more socially vulnerable areas, this is not particularly pronounced. There are several plausible explanations for this. Patient-level socioeconomic position and community SVI, while correlated, are not precise analogues [29]. Area-level SVI may not be a true marker of individual socioeconomic position, risking ecological bias. This dataset is also conditioned on patients who are on Medicaid and so is selecting a more homogenous group, and residual socioeconomic differences may not be as apparent within this dataset. Many children’s hospitals are located in high poverty areas with high needs [30], and it is possible that this might mitigate some of the pejorative effects of socioeconomic disparities due to improved access to care, thereby explaining the limited evidence for disparities found by area-level SVI. Finally, modelling SVI and race together risks over-adjusting, and thus potentially biasing the causal association between SVI (and race) and outcomes.
Our study had some important limitations. As routine data there may be coding errors and misclassification of race/ethnicity, socioeconomic position or outcome. We identified our pediatric intensive care cohort using CPT billing codes and it is possible that these may not accurately capture the PICU population; however, we can see clear differences in this cohort, such as higher mortality and greater number of complex chronic condition, making it plausible that this cohort reflects a typical PICU cohort. We also were not able to identify patients with multiple readmissions, risking inappropriate precision of our effect estimates. As an administrative dataset, there was a substantial amount of missing data, and inconsistency with coding Hispanic/Latino patients meant we could not reliably capture patients with Hispanic/Latino ethnicity. Not analyzing Hispanic/Latino children separately limits our understanding of the unique healthcare challenges and disparities faced by this demographic group. Hispanic/Latino children represent a significant and growing portion of the pediatric population in the United States, and prior research has shown that they often face unique barriers to healthcare access, such as language barriers, and potential immigration-related fears, which can all contribute to disparities in health outcomes [31]. By grouping Hispanic/Latino children with other races/ethnicities, we may not capture the specific factors influencing their PICU admissions and outcomes, potentially overlooking critical areas for intervention and policy improvement.
Studies have shown that patients who are missing data on race/ethnicity differ systematically from those who do, such as being more likely to be low income [32]. It is unclear what resources are dedicated to collecting and cleaning this data, with some data being gathered by self-report and other data being assigned with varying accuracy [33]. To account for this missing data, we included patients missing data as a category in our analysis and present results for this group. We are also only able to capture PICU mortality, and as such our study potentially underestimates mortality, although is likely a reasonable estimate of hospital mortality. Pre-hospital mechanisms contributing to childhood mortality, such as from accidents or injuries, could not be assessed, including if subjects died in an emergency department and were not hospitalized.
The limitations of our study are partly offset by some important strengths. We use a large dataset including over 4 million patients over 7 years. The dataset allowed us to look at ZIP Code-level socioeconomic indicators using a multi-themed metric. Although this data is 10 years old it is the most complete set of multi-state Medicaid data available, making it potentially more generalizable. This study provides a landscape of the state disparities in PICU prior to expansion of Medicaid, and will provide a baseline for future studies to assess for improvements. Additionally, the dataset includes diagnostic codes allowing us to identify and adjust for children with chronic complex conditions, which is an important confounder. [28] A range of states are represented geographically making our study more representative than many single-center and regional databases. Medicaid covered approximately 26.8% of children in the US in 2008, increasing to 37.7% in 2014, providing robust demographic information on individuals with low socioeconomic status at the national level, allowing us to account for the geographic heterogeneity in the USA with respect to racial disparities and outcome [34].
Conclusion
Children covered by Medicaid of Black race were at increased risk of PICU admission and mortality, with substantial state-level variation, emphasizing geographic variability as a major driver of systemic racism in Pediatrics. Race was associated with neighborhood socioeconomic vulnerability, and children in areas with higher levels of vulnerability had higher mortality. Further work is needed to develop targeted policy and healthcare interventions to reduce racial and socioeconomic disparities. Future research should focus on evaluating the effectiveness of any interventions and exploring strategies to ensure equitable healthcare access. A decade of Medicaid access in some of these states will provide a natural experiment for assessing whether disparities were impacted. Accurate documentation of a child’s race/ethnicity in administrative records is essential to understand if healthcare disparities occur. The Transformed Medicaid Statistical Information System (T-MSIS) the current largest national database of children’s Medicaid race/ethnicity data collection quality is low of for the majority of states. T-MSIS could improve its data collection on racial disparities by standardizing race and ethnicity categories and formatting, and supporting complete and accurate data collection across states to understand the racial disparities experienced by Black children. Our study findings underscore the complex interplay between race, social vulnerability and outcomes, emphasizing the need for comprehensive assessment and tailored interventions to address disparities in PICU utilization and outcomes.
Availability of data and materials
The datasets generated and/or analyzed during the current study are from the Medicaid Analytic eXtract (MAX) repository. These data are publicly accessible but require an application for access through the Research Data Assistance Center (ResDAC). To apply for access or find more information, please visit the ResDAC website at https://resdac.org and navigate to the 'Get Data' section.
Abbreviations
- ATSDR:
-
Agency for Toxic Substances and Disease Registry
- CDC:
-
Centers for Disease Control and Prevention
- CPT:
-
Current Procedural Terminology
- FIPS:
-
Federal Information Processing System
- MAX:
-
Medicaid Analytic eXtract
- PICU:
-
Pediatric intensive care unit
- SVI:
-
Social vulnerability index
- US:
-
United States
References
Mitchell HK, Reddy A, Perry MA, Gathers C-A, Fowler JC, Yehya N. Racial, ethnic, and socioeconomic disparities in paediatric critical care in the USA. Lancet Child Adolesc Health. 2021;5:739–50.
Andrist E, Clarke RG, Phelps KB, et al. Understanding Disparities in the Pediatric ICU: A Scoping Review. Pediatrics. 2024;153(5):e2023063415. https://doi.org/10.1542/PEDS.2023-063415.
Mitchell HK, Reddy A, Montoya-Williams D, Harhay M, Fowler JC, Yehya N. Hospital outcomes for children with severe sepsis in the USA by race or ethnicity and insurance status: a population-based, retrospective cohort study. Lancet Child Adolesc Health 2020; published online Dec. https://doi.org/10.1016/S2352-4642(20)30341-2.
Leimanis Laurens M, Snyder K, Davis AT, Fitzgerald RK, Hackbarth R, Rajasekaran S. Racial/Ethnic Minority Children With Cancer Experience Higher Mortality on Admission to the ICU in the United States. Pediatr Crit Care Med. 2020;21:859–68.
Winestone LE, Getz KD, Miller TP, et al. The role of acuity of illness at presentation in early mortality in black children with acute myeloid leukemia. Am J Hematol. 2017;92:141–8.
Epstein D, Wong CF, Khemani RG, et al. Race/Ethnicity is not associated with mortality in the PICU. Pediatrics. 2011;127(3):e588-97. https://doi.org/10.1542/PEDS.2010-0394.
Lopez AM, Tilford JM, Anand KJS, et al. Variation in pediatric intensive care therapies and outcomes by race, gender, and insurance status. Pediatr Crit Care Med. 2006;7:2–6.
Turner D, Simpson P, Li S-H, Scanlon M, Quasney MW. Racial disparities in pediatric intensive care unit admissions. South Med J. 2011;104:640–6.
Epstein D, Reibel M, Unger JB, et al. The effect of neighborhood and individual characteristics on pediatric critical illness. J Community Health. 2014;39:753–9.
Chamberlain JM, Joseph JG, Patel KM, Pollack MM. Differences in severity-adjusted pediatric hospitalization rates are associated with race/ethnicity. Pediatrics. 2007;119:e1319–24.
Kachmar AG, Connolly CA, Wolf S, Curley MAQ. Socioeconomic Status in Pediatric Health Research: A Scoping Review. J Pediatr. 2019;213:163–70.
Zurca AD, Suttle ML, October TW. An Antiracism Approach to Conducting, Reporting, and Evaluating Pediatric Critical Care Research. Pediatr Crit Care Med. 2022;23:129–32.
Kehm RD, Spector LG, Poynter JN, Vock DM, Altekruse SF, Osypuk TL. Does socioeconomic status account for racial and ethnic disparities in childhood cancer survival? Cancer. 2018;124:4090–7.
Heneghan JA, Rogerson C, Goodman DM, Hall M, Kohne JG, Kane JM. Epidemiology of Pediatric Critical Care Admissions in 43 United States Children’s Hospitals, 2014–2019. Pediatr Crit Care Med. 2022;23:484–92.
Killien EY, Keller MR, Watson RS, Hartman ME, Epidemiology of Intensive Care Admissions for Children in the US From,. to 2019. JAMA Pediatr. 2001;2023:177. https://doi.org/10.1001/JAMAPEDIATRICS.2023.0184.
Andrist E, Riley CL, Brokamp C, et al. Neighborhood poverty and pediatric intensive care use. Pediatrics. 2019;144: e20190748.
Myers CN, Chandran A, Psoter KJ, Bergmann JP, Galiatsatos P. Indicators of Neighborhood-Level Socioeconomic Position and Pediatric Critical Illness. Chest. 2023;164:1434–43.
Naclerio AL, Gardner JW, Pollack MM. Socioeconomic factors and emergency pediatric ICU admissions. Ann N Y Acad Sci. 1999;896:379–82.
McCrory MC, Akande M, Slain KN, et al. Child Opportunity Index and Pediatric Intensive Care Outcomes: A Multicenter Retrospective Study in the United States. Pediatr Crit Care Med. 2024;25:323–34.
Trinidad S, Kotagal M. Socioeconomic Factors and Pediatric Injury. Curr Trauma Rep. 2023;9(2):47–55. https://doi.org/10.1007/S40719-023-00251-X.
Bratton SL, Roberts JS, Watson RS, Cabana MD. Acute severe asthma: Outcome and Medicaid insurance. Pediatr Crit Care Med. 2002;3:234–8.
Byrd VLH, Dodd AH. Assessing the usability of encounter data for enrollees in comprehensive managed care 2010–2011. 2015. Available at: https://www.cms.gov/Research-Statistics-Data-and-Systems/Computer-Data-and-Systems/MedicaidDataSourcesGenInfo/Downloads/MAX_Encounter_Brief_2010_2011.pdf (accessed 19 Aug 2024).
Ruttner L, Borck R, Nysenbaum J, Williams S. Guide to MAX Data. 2015. Available at: https://www.cms.gov/Research-Statistics-Data-and-Systems/Computer-Data-and-Systems/MedicaidDataSourcesGenInfo/Downloads/MAX_IB21_MAX_Data_Guide.pdf (accessed 19 Aug 2024).
https://www.cms.gov/Research-Statistics-Data-and-Systems/Computer-Data-and-Systems/MedicaidDataSourcesGenInfo/MAX-Validation-Reports (Accessed 30 Jan 2023).
Weissman GE, Hubbard RA, Kohn R, et al. Validation of an Administrative Definition of ICU Admission Using Revenue Center Codes. Crit Care Med. 2017;45:e758–62.
Flanagan BE, Gregory EW, Atsdr /, et al. A Social Vulnerability Index for Disaster Management. Article 3 Journal of Homeland Security and Emergency Management 2011; 8. https://doi.org/10.2202/1547-7355.1792.
Feudtner C, Feinstein JA, Zhong W, Hall M, Dai D. Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation. BMC Pediatr. 2014;14:199.
Barnes JM, Barker AR, King AA, Johnson KJ. Association of Medicaid Expansion With Insurance Coverage Among Children With Cancer. JAMA Pediatr. 2020;174:581–91.
Moss JL, Johnson NJ, Yu M, Altekruse SF, Cronin KA. Comparisons of individual- and area-level socioeconomic status as proxies for individual-level measures: evidence from the Mortality Disparities in American Communities study. Popul Health Metr. 2021;19(1):1. https://doi.org/10.1186/S12963-020-00244-X.
Sills MR, Hall M, Colvin JD, et al. Association of Social Determinants With Children’s Hospitals’ Preventable Readmissions Performance. JAMA Pediatr. 2016;170:350–8.
Slopen N, Umaña-Taylor AJ, Shonkoff JP, Carle AC, Hatzenbuehler ML. State-Level Anti-Immigrant Sentiment and Policies and Health Risks in US Latino Children. Pediatrics. 2023;152(3):e2022057581.https://doi.org/10.1542/PEDS.2022-057581.
Sholle ET, Pinheiro LC, Adekkanattu P, et al. Underserved populations with missing race ethnicity data differ significantly from those with structured race/ethnicity documentation. J Am Med Inform Assoc. 2019;26:722–9.
Johnson JA, Moore B, Hwang EK, Hickner A, Yeo H. The accuracy of race & ethnicity data in US based healthcare databases: A systematic review. Am J Surg. 2023. https://doi.org/10.1016/J.AMJSURG.2023.05.011.
Kaiser Family Foundation (KFF). Health Insurance Coverage of Children 0–18. 2022. Available at: https://www.kff.org/other/state-indicator/children-0-18/ (accessed 19 Aug 2024).
Funding
Nadir Yehya is supported by National Institutes of Health (NIH) grant number K23-HL136688.
Hannah Mitchell is supported by a National Institute for Health and Care Research Academic Clinical Fellowship.
Author information
Authors and Affiliations
Contributions
HM and NY conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript. SL helped devise the statistical analysis plan and reviewed and revised the manuscript for important intellectual content. JR and MP coordinated data management and carried out the initial analyses, drafted methods, and critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Institutional Review Board of The Children’s Hospital of Philadelphia reviewed this project and declared that it met the criteria for non-human subjects research, compliant with the terms outlined in a data use agreement with the Centers for Medicare and Medicaid Services for use of the data. Because patients were not contacted or identified in the dataset, consent to participate was waived by the Institutional Review Board of The Children’s Hospital of Philadelphia.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mitchell, H.K., Radack, J., Passarella, M. et al. A multi-state analysis on the effect of deprivation and race on PICU admission and mortality in children receiving Medicaid in United States (2007–2014). BMC Pediatr 24, 565 (2024). https://doi.org/10.1186/s12887-024-05031-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-024-05031-3