
Abstract
Background
Although several school-based cognitive behavioural intervention programmes have been developed in Japan to prevent and improve children’s anxiety disorders, the substantial time required for their completion remains a problem.
Methods
A brief version of the cognitive behavioural programme called ‘Journey of the Brave’, developed for Japanese children was conducted among 90 children aged 10‒11 years using 20-min short classroom activities, and its effectiveness was examined. The children were divided into two groups: the intervention (n = 31) and control groups (n = 59). The control group did not attend any programme sessions and followed regular school curriculum. We conducted 14 weekly programme sessions and assessed children at pre-intervention, post-intervention, and 2-month follow-up (6 months after the beginning). The primary and secondary outcome measures were the Spence Children’s Anxiety Scale (SCAS) to assess children’s anxiety symptoms and the Strengths and Difficulties Questionnaire (SDQ) to measure behaviour problems, respectively.
Results
A statistically significant reduction in the SCAS score in the intervention group was found at 2-month follow-up compared with the control group. A significant reduction was also observed in the SDQ score.
Conclusions
Our findings suggested that the ‘Journey of the Brave’ programme, which requires only 5 h of short classroom activities, demonstrates promising results compared with previous programmes. A larger randomised control trial would be desirable.
Trial registration
UMIN, UMIN000009021, Registered 10 March 2012.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Anxiety disorder is one of the most prevalent psychological disorders experienced in childhood and adolescence [1,2,3]. Some studies have demonstrated that the 6 to 12-month prevalence of anxiety disorders among children and adolescents is approximately 10% [4,5,6]. Children with anxiety are prone to maladaptation at school. For example, they experience panic attacks, fatigue, or sleep disturbance from anxiety, which may lead to underachievement [7]. Additionally, those with low self-esteem may avoid social relations and have negative peer interactions [8], resulting in school absenteeism [9].
Although the current record of school absenteeism in Japan, by all available measures, has not reduced over time, in 2014, Japan’s Ministry of Education [10] reported that the primary reason for absenteeism in elementary schools was ‘emotional confusion (e.g. anxiety)’. Additionally, Ishikawa et al. [11] associated school absenteeism with anxiety and depression. Children with developmental problems including attention deficit hyperactivity disorder and Autism Spectrum Disorder often express symptoms of anxiety [12]. If left untreated, anxiety in childhood can lead to an increased risk of other psychological disorders, the impairment of development, and disturbances in career domains [13,14,15]. Therefore, prevention and early intervention is important to prevent problems in adulthood [16,17,18].
Schools offer an optimal setting for interventions to prevent and reduce anxiety among children [19,20,21]. Primary interventions can be defined as either universal, selected, or indicated [22]. The school setting is an ideal environment for universal intervention targeting the entire student population [23, 24]. Schools have several advantages, such as enabling easier access to programme sessions, reducing stigmatisation, and enhancing peer support [25,26,27].
Cognitive behavioural therapy (CBT) is a recommended treatment choice for anxiety disorders among children [28,29,30]. CBT-based anxiety prevention programmes have been developed in other countries, and their effects have been demonstrated in meta-analysis studies in universal interventions at schools [31, 32]. Among them, one of the most widely recognised school-based CBT programmes is the ‘FRIENDS’ programme which aims to decrease anxiety and to promote resilience of children [33]. FRIENDS has gained recognition as an effective programme for the reduction and prevention of anxiety and depressive symptoms by the World Health Organisation [34] with several significant anxiety reduction results. For example, Neil and Christensen [35] reported that the effect size of the FRIENDS programme targeting anxiety at follow-up was 0.33–0.41 and 0.62 in both Barrett and Turner’s [36] and Lowry-Webster et al.’s [37] studies.
Although FRIENDS was developed in Australia and its implementations and effectiveness verification studies have been conducted worldwide, predominantly in Western countries [36,37,38,39], it is rarely tried in Japan. It is difficult to directly import programmes developed in Western countries to Japanese schools owing to socio-cultural differences [40]. Therefore, a Japan-original CBT-based programme ‘Journey of the Brave’ for Japanese children was independently developed, and an initiative to examine the effects [40] began in 2014. The initial trial was conducted outside the school setting as a preliminary study, and the results demonstrated that the programme was effective based on parents’ evaluations. Thereafter, intervention studies in elementary schools have been conducted showing significant programme effectiveness [41].
Current study
Despite the availability of an effective CBT-based intervention for childhood anxiety that is applicable to the school setting, there are several issues to its implementation in schools in Japan.
The first issue is the session length of the programme [42, 43]. Studies report that students’ attention declines in the first 10‒15 min of a lecture [44]. The session length must be short enough to maintain children’s concentration. Each session of the universal approach programme usually lasts from 60–90 min in other countries [35], and it is estimated that the total time required to complete the programme is 10–15 h. The initial trial of the ‘Journey of the Brave’ programme [40] comprised ten 45-min sessions, taking 7.5 h to complete. As schools have other academic requirements and school events, pragmatic challenges such as space and time availability in schools must be addressed when providing mental health programmes [42, 45]. Using the time frame of short classroom activities in implementing the ‘Journey of the Brave’ programme is advisable to address the issue of programme length.
The second issue concerns the time of the day when the program is implemented. A study evaluated the effects of the after-school CBT programme on the anxiety of children with high anxiety symptoms [46]. According to a child self-report, the study results indicated no significant effects on symptoms of anxiety among children who received the CBT programme. The result of their study was partially explained by high absenteeism owing to delivering the programme after school. A report on adult stress has indicated that the mind does not experience equal levels of stress and conflict in the morning and the evening [47, 48]. Thus, it is beneficial to implement the programme as part of short class activities in the morning in a school schedule.
The third issue is regarding the age at which the program is implemented. Most elementary schools in Japan have class shuffles when children are promoted from the 4th (9–10 years old) to the 5th (10–11 years old) grade. This environmental change poses a negative mental health effect on children, causing increased anxiety [49, 50]. Thus, it is necessary to build new friendships, and most children might be anxious during this period. Additionally, Grade 5 (10- to 11-year-olds) children have a new responsibility as school leaders and meet increased opportunities for social communication, forcing them to face higher pressure and anxiety after the class re-shuffle. Thus, the programme to manage anxiety, which comprises the necessary contents for 10- to 11-year-old children, may match their will to learn and deepen their understanding of contents.
Considering the aforementioned aspects, this study aimed to implement and examine the effectiveness of the CBT-based programme intervention ‘Journey of the Brave’ using short classroom activities among 10- to 11-year-old children.
Method
Procedure
Participants and informed consent
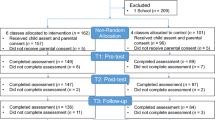
Our team member, who was working in a school in the vicinity of Tokyo as the nurse teacher, explained the study protocol and the schoolmaster granted permission for data collection. As it was compulsory for children to receive class sessions in each class, it was impossible to randomly assign the intervention and control groups. Thus, the approval of the schoolmaster was received with the condition that non-randomised design was applied assigning one of three 5th grade classes as the intervention while the remaining two as the control group. The cross-over design was applied whereas the control group also took programme sessions later. Programme explanations with consent forms were delivered through the children to their parents, who provided consent on behalf of their children. The completed consent forms were returned to the school. A total of 93 consent forms were distributed and 92 returned (57 male participants and 35 female participants) with parent’s consent. One child did not respond because of a psychological block about coming to school (Fig. 1).

Flow-chart shows the number of children recruited, dropout in the evaluation at each point, and sample count of MMRM. Abbreviations: MMRM, mixed-effect model for repeated measures
Intervention group
A class consisting of 31 (19 boys, 12 girls) children, with an average age of 10.0 (SD = 0) received 14 weekly sessions of ‘Journey of the Brave’ once a week. Each child was provided a workbook that they used throughout the programme.
Control group
Prior to programme commencement for the intervention group, the parents of children from the control group in two classes consisting of 61 children (36 boys, 23 girls) with the average age of 10.1 (SD = 0.3) were explained that the control group will attend the sessions later. Two children were unable to obtain signed consent forms from their parents. During the programme, children in the control group received the regular school curriculum (e.g. reading, calculation exercises) facilitated by the classroom teacher.
Programme facilitators and training
The ‘Journey of the Brave’ programme was led by two facilitators. The main programme facilitator was the nurse teacher of the school and was majoring in Cognitive Behaviour Physiology as a graduate student at the time of the study. We designated the teacher in charge of this class as the sub-facilitator of the programme. Prior to conducting the programme, the facilitators were provided t hours’ training once every 2 weeks for 3 months by the first author who developed the original programme. During the implementation phase, the facilitators contacted the first author once a week to discuss problems and/or questions that arose during the intervention sessions, and received supervision and support.
Description of journey of the brave programme
The ‘Journey of the Brave’ programme was developed for 9- to 12-year-old children, focussing on feelings of anxiety and the key behaviour changes to manage these feelings [40]. It comprises multiple 10 45-min-long sessions. The programme contents are based on the protocol of CBT for anxiety treatment. It includes contents such as psychological education, relaxation, case formulation of anxiety, exposure, cognitive restructuring, and assertiveness skills when faced with social anxiety. The largest difference between this programme and existing CBT-based ones is that the content was developed based on the socio-cultural background of Japan. For example, while many of the FRIENDS contents include group activities, the ‘Journey of the Brave’ programme is constructed with an individual study format because several children in Japanese schools experience social anxiety, and group activities increase their anxiety. Additionally, the illustrations and characters in the programme workbook are familiar to Japanese children. Moreover, each session is designed to take less than 45 min and a teacher-friendly manual is prepared.
Programme implementation using short classroom activities time
In Japan, there are short classroom activities in the morning as part of regular curriculum in most elementary schools. However, the way this time is used differs in every school, and in many cases, the time allocated for this is 20 min (8:20–8:40 for example). The activities include both active physical movement and passive learning such as reading and calculation. Individual content is decided by each school as long as it fits the purpose of children’s overall health promotion. Therefore, mental health programmes such as the one introduced here is quite appropriate.
Therefore, to implement the ‘Journey of the Brave’ in the 20-min class morning activities time slot in school in Japan, we divided each session into two. Additionally, we decided to not include the session on assertiveness skills, because the same theme had already been handled in the existing school curriculum. The cognitive restructuring session was allotted the entire 45 min to ensure children’s comprehension. Thus, the number of sessions of this programme increased to 14; however, the total implementation time decreased to approximately 5 h (Table 1).
Measurements
The participating children completed a set of sequential questionnaires during the session at three different time points: pre-intervention, post-intervention, and 2-month follow-up. Except for the evaluation form, they completed the self-report measures during their regular class time. The parents of the intervention group children received the evaluation form at home through their children, and they returned the forms to the school after completion.
Quantitative data to verify effectiveness
Spence children’s anxiety scale (SCAS)
The primary outcome measure was the anxiety symptoms reported by children, measured using the Spence Children’s Anxiety Scale [51], one of the most valid measurements for assessing child anxiety meeting the diagnostic standard. The questions are applicable to 8- to 15-year-old children, and good reliability and validity coefficients of the SCAS Japanese version have been reported [52]. The SCAS includes 38 items regarding children’s anxiety symptoms divided into six subcategories: separation anxiety, social phobia, panic disorder/agoraphobia, generalised anxiety disorder, physical injury fears, and obsessive–compulsive disorder. SCAS scores range between 0 (never) and 3 (always), and the maximum possible score is 114.
Strengths and difficulties questionnaire (SDQ)
The secondary outcome measure was behaviour problems, measured using the self-report version of the Goodman SDQ [53]. The questions were applicable to 4- to 16-year-old children. Reliability and validity coefficients of the Japanese versions of the SDQ have been reported [54]. The SDQ includes 25 items, with each item scored 0 (not true), 1 (somewhat true), or 2 (certainly true), according to the perceived severity of the symptom. The items are divided into five subcategories: emotional symptoms, behaviour problems, hyperactivity/inattention, peer relationship problems, and pro-social behaviour. A total difficulties score (TDS) is computed by summing the scores of the first four subcategories, and the maximum possible score is 40.
Qualitative data to assess acceptability and feasibility
Programme evaluation form for children
This form was used to measure children’s acceptance and satisfaction with the programme. Participants were asked to rate the extent to which they could understand the components of this programme and how helpful the skills they learned were in their daily life. This form utilised a four-point Likert-scale, and the respondents were asked to rate each item according to their own experience; the response options were ‘yes’, ‘a little’, ‘not really’, and ‘no.’ A numerical equivalent was assigned to each answer, and percentages were analysed. Additionally, children were asked to write free comments about the programme. Furthermore, the programme sub-facilitator asked the children to provide free comments on the quality and feasibility of the programme after the intervention.
Programme evaluation form for parents
This form was used to assess the parents’ evaluation of the programme and its perceived effects on their children. Parents were asked how helpful they thought the programme was for their children and how this program met their expectations. This form used a four-point Likert-scale, with the response options and analysis methods being the same as that in the evaluation form for children. Free comments were also obtained about the programme.
Statistical analysis
For the baseline variables, summary statistics were constructed using frequencies and proportions for categorical data, and means and standard deviations (SDs) for continuous variables. The participant characteristics were compared using a chi-square test for categorical outcomes and a t-test or the Wilcoxon rank sum test for continuous variables, as appropriate. Additionally, t-tests were conducted on both SCAS and SDQ at baseline to confirm the difference between groups.
To confirm the SCAS and the SDQ score changes at 2-month follow-up from baseline, primary analysis was performed using the mixed-effects model for repeated measures (MMRM) with intervention group, time (week), and interactions between treatment group and time (week) as fixed effects; an unstructured covariate was used to model the covariance of within-subject variability. MMRM analysis used all the available data and assumed that any missing observations were missing at random. Under the ignorable missing data framework, MMRM analysis is a robust approach for estimating the true treatment difference and controlling Type I error rates [55, 56]. However, when data are not missing at random, these inferential techniques that are valid for missing-at-random data are typically invalid [57, 58].
To compare the efficacy and effectiveness of the intervention programme, SCAS and SDQ effect size (ES) estimates were calculated using Cohen’s d [59]. Cohen’s d values were calculated as the difference between the intervention and the control groups’ means divided by the pooled standard deviation. According to Cohen [59], an effect size of 0.2 is considered small, 0.5 is considered medium, and 0.8 is considered large.
All statistical tests were two-tailed, and a p-value of 0.05 was employed. Other statistical analyses were performed with IBM SPSS Statistics for Windows, Version 17.0 (IBM, Armonk, New York, USA), and SAS software version 9.4 (SAS Institute, Cary, NC, USA).
Results
A total of 90 children (31 and 59 in the intervention and control groups, respectively) completed the questionnaire, and their data were used for analyses (Fig. 1). The differences in gender and age were analysed between the intervention and control group children at pre-test. There were no significant differences (Table 2). Next, to compare the differences in baseline SCAS scores at pre-test between the intervention and control groups, t-tests were conducted. There were no significant differences in SCAS scores (Table 2). T-tests were also conducted to compare the differences in baseline SDQ scores at pre-test between the intervention and control groups. Although there was no significant difference in the SCAS score, significant differences in the SDQ scores were observed (Table 2).
The SCAS score changes are indicated in Fig. 2 and Table 3. At 2-month follow-up, the estimated mean reductions in SCAS from baseline by MMRM were -7.17 in the intervention group (95% CI = -10.64 – -3.70) and -1.40 in the control group (95% CI = -3.91 – 1.11), and the between group difference was -5.77 (95% CI = -10.07 – -1.47, p = 0.009; Table 4). The effect size (Cohen’s d) estimate at 2-month follow-up was 0.46 between the intervention and control groups.

Mean total SCAS score change of each group during the study. shows the SCAS score of the intervention group and the control group for each time period. Abbreviations: SCAS, Spence Children’s Anxiety Scale
The SDQ score changes are indicated in Fig. 3 and Table 3. At 2-month follow-up, the mean reductions in the change of SDQ scores from baseline were -1.81 in the intervention group (95% CI = -2.93 – -0.70) and -0.22 in the control group (95% CI = -1.02 – 0.59), and the between- group difference was -1.60 (95% CI = -2.98 – -0.21, p = 0.024; Table 4). The effect size (Cohen’s d) estimate at 2-month follow-up was 0.15 between the intervention and control groups.

Mean total SDQ scores in each group during the study. shows the SDQ score of the intervention and control groups for each time period. Abbreviations: SDQ, Strengths and Difficulties Questionnaire
Evaluation form to assess acceptability and feasibility
Evaluation forms for children were returned by all the children (n = 31) in the intervention group. In total, 81% of children responded that they were able to cope with anxiety by themselves, and 84% responded that the skills they learned during the programme will be helpful in daily life. Additionally, 94% of the children were satisfied with learning the programme in the school setting.
Evaluation forms for parents were returned by 29 parents in the intervention group. In total, 86% of them responded that the skills that their children learned during the programme would be helpful in their daily life, and 97% felt that the programme should be implemented in school settings. Excerpts of free comments about the programme in the intervention group are provided in Figs. 4 and 5.

Excerpts from free comments on the ‘Journey of the Brave’ programme (intervention group children). presents some of the free comments from the intervention group children about the programme after the intervention

Excerpts from free comments on the ‘Journey of the Brave’ programme (intervention group parents). presents some of the free comments from the intervention group parents about the programme after the intervention
Furthermore, the sub-facilitator evaluated the programme as follows:
-
The timing was good because it was after the class shuffle.
-
Conducting the exposure task progressively, was especially adequate for children.
-
The session pertaining to maladaptive cognition was helpful in classifying the cognitive style of the children.
-
I would like to receive feedback and enhance the skills learned during the programme to apply them to school life.
Discussion
The results of our study showed a statistically significant reduction in the intervention group at 2-month follow-up in anxiety symptoms and behaviour problems compared with the usual care control group despite the programme being delivered in a short and divided time format. This result confirms the positive effect shown in the previous pilot study [40] as well as the following effectiveness verification studies [41, 60].
The original ‘Journey of the Brave’ programme took 10 weekly sessions, with each session lasting 60 min compared with that of our study with a duration of only five hours. Additionally, the qualitative data received in the evaluation form were mostly positive, and we judged that there was no problem in the acceptability and feasibility of the programme, indicating its efficiency. The result, if verified under more robust research design, may help overcome some barriers to implementing this in Japan because it can be smoothly incorporated into the school timetable and saves manpower.
However, the numerous limitations of this study should be noted. First, there was the issue of recruitment bias. As it was difficult to identify the participating school, the school where one of our research team members was working as the nursing teacher was designated as the study field; moreover, she served as the facilitator of the programme. The possibility of daily relationships between the teacher and the children may have impacted our results. Additionally, we employed a nonrandomised control design. It was impossible to evade the contamination risk between the intervention and control groups as children from the same grade year and school were selected as the control group. Conducting a study with a randomised control design is recommended to establish evidence of CBT practices. Therefore, it is necessary to conduct a study with a randomised block control design by removing moderators and mediators of anxiety in the future (e.g., characteristics of class and school events).
Second, important factors such as reliability of the facilitator and programme fidelity are not explored. The facilitator of this study had acquired the ‘Journey of the Brave’ facilitator qualification, had completed the training course of Improving Access to Psychological Therapies, and was studying CBT. She was familiar with the programme as she was one of the members of the research team receiving advice and supervision from the programme author once a week. However, we were unable to quantitively evaluate reliability and programme fidelity because objective measures were not used. In the future, using a device to monitor the facilitator who is implementing the programme is necessary.
Finally, this study does not report beyond the 2-month follow-up time point. Further research is needed to investigate longer follow-up durations (e.g. 1-year, 2-years) to determine the impact of the programme over time. It has been indicated that children are at risk for emotional and behavioural problems during the transition time when they advance from elementary school to junior high school [61]. Therefore, evaluation during this period is important to determine the long-term effects of this intervention.
As stated above, rigorousness of this study is missing on multiple grounds. Hereafter, we wish to secure greater visibility and credibility with a more robust study design to disseminate findings of superior quality.
Conclusions
This study demonstrated that the delivery of the ‘Journey of the Brave’ programme in the form of brief classroom activities results in a significant reduction in anxiety symptoms and behavioural problems. Our findings suggest that the programme, which is completed in only 5 h, is as effective as programmes that have taken over 10 h to complete in previous studies. The significant room for improvement in the current study warrants future research with improved designs.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CBT:
-
Cognitive Behavioural Therapy
- ADHD:
-
Attention Deficit Hyperactivity Disorder
- SCAS:
-
Spence Children’s Anxiety Scale
- SDQ:
-
Strengths and Difficulties Questionnaire
- MMRM:
-
Mixed-effect model for repeated measures
References
Cartwright-Hatton S. Anxiety of childhood and adolescence: challenges and opportunities. Clin Psychol Rev. 2006;26:813–6.
Essau CA, Conradt J, Petermann F. Frequency, comorbidity, and psychosocial impairment of anxiety disorders in German adolescents. J Anxiety Disord. 2000;14:263–79.
Rapee RM, Schniering CA, Hudson JL. Anxiety disorders during childhood and adolescence: origins and treatment. Annu Rev Clin Psychol. 2009;5:311–41.
Breton JJ, Bergeron L, Valla JP, Berthiaume C, Gaudet N, Lambert J, et al. Quebec child mental health survey: prevalence of DSM III-R mental health disorders. J Child Psychol Psychiatry. 1999;40:375–84.
Shaffer D, Fisher P, Dulcan MK, Davies M, Piacentini J, Schwab-Stone ME, et al. The NIMH Diagnostic Interview Schedule for Children Version 2.3 (DISC-2.3): description, acceptability, prevalence rates, and performance in the MECA Study. Methods for the Epidemiology of Child and Adolescent Mental Disorders Study. J Am Acad Child Adolesc Psychiatry version. 1996;23(35):865–77.
Wittchen HU, Nelson CB, Lachner G. Prevalence of mental disorders and psychosocial impairments in adolescents and young adults. Psychol Med. 1998;28:109–26.
Briesch AM, Hagermoser Sanetti LM, Briesch JM. Reducing the prevalence of anxiety in children and adolescents: an evaluation of the evidence base for the FRIENDS for life program. Sch Ment Health. 2010;2:155–65.
Ginsburg GS, La Greca AM, Silverman WK. Social anxiety in children with anxiety disorders: relation with social and emotional functioning. J Abnorm Child Psychol. 1998;26:175–85.
Egger HL, Costello EJ, Angold A. School refusal and psychiatric disorders: a community study. J Am Acad Child Adolesc Psychiatry. 2003;42:797–807.
Ministry of Education. Research on issues over teacher guidance toward student's misbehavior (in Japanese). http://www.mext.go.jp/b_menu/houdou/26/10/__icsFiles/afieldfile/2014/10/16/1351936_01_1.pdf. Accessed 9 Dec 2017, 2014; 2014.
Ishikawa S, Sato H, Nomura H, Kiyamura M, Kawano J, Inoue K, et al. An investigation on mechanism of maintaining school non-attendant behaviors: application of school refusal assessment scale. Jpn J Cogn Ther. 2012;5:83–93.
Gordon-Lipkin E, Marvin AR, Law JK, et al. Anxiety and mood disorder in children with autism spectrum disorder and ADHD. Pediatrics. 2018;141(4):e20171377.
Bittner A, Egger HL, Erkanli A, Jane Costello EJ, Foley DL, Angold A. What do childhood anxiety disorders predict? J Child Psychol Psychiatry. 2007;48:1174–83.
Norton GR, McLeod L, Guertin J, Hewitt PL, Walker JR, Stein MB. Panic disorder or social phobia: which is worse? Behav Res Ther. 1996;34:273–6.
Rubin KH, Root AK, Parents BJ. peers, and social withdrawal in childhood: a relationship perspective. New Dir Child Adolesc Dev. 2010;127:79–94.
Donovan CL, Spence SH. Prevention of childhood anxiety disorders. Clin Psychol Rev. 2000;20:509–31.
Liddle I, Macmillan S. Evaluating the friends programme in a Scottish setting. Educ Psychol Pract. 2010;26:53–67.
Rapee RM, Kennedy S, Ingram M, Edwards S, Sweeney L. Prevention and early intervention of anxiety disorders in inhibited preschool children. J Consult Clin Psychol. 2005;73:488–97.
Stallard P, Taylor G, Anderson R, Daniels H, Simpson N, Phillips R, et al. School-based intervention to reduce anxiety in children: study protocol for a randomized controlled trial (PACES). Trials. 2012;13:227. https://doi.org/10.1186/1745-6215-13-227.
Tashman NA, Weist MD, Acosta O, Bickham NL, Grady M, Nabors L, et al. Toward the integration of prevention mental health programs. Child Serv Soc Pol Res Pract. 2000;3:97–115.
Tomb M, Hunter L. Prevention of anxiety in children and adolescents in a school setting: the role of school-based practitioners. Child Sch. 2004;26:87–101.
Mrazek PJ, Haggerty RJ. Reducing Risks for Mental Disorders: Frontiers for Preventive Intervention Research. Washington, DC: National Academies Press; 1994.
Ginsburg GS, Becker KD, Kingery JN, Nichols T. Transporting CBT for childhood anxiety disorders into inner-city school-based mental health clinics. Cogn Behav Pract. 2008;15:148–58.
Masia-Warner C, Nangle DW, Hansen DJ. Bringing evidence-based child mental health services to the schools: general issues and specific populations. Educ Treat Child. 2006;29:165–72.
Barrett PM, Farrell LJ, Ollendick TH, Dadds M. Long-term outcomes of an Australian universal prevention trial of anxiety and depression symptoms in children and youth: an evaluation of the FRIENDS program. J Clin Child Adolesc Psychol. 2006;35:403–11.
Miller LD, Laye-Gindhu A, Liu Y, March JS, Thordarson DS, Garland EJ. Evaluation of a preventive intervention for child anxiety in two randomized attention-control school trials. Behav Res Ther. 2011;49:315–23.
Storch EA, Crisp HL. Taking it to the schools–transporting empirically supported treatments for childhood psychopathology to the school setting. Clin Child Fam Psychol Rev. 2004;7:191–3.
Ishikawa SI, Okajima I, Matsuoka H, Sakano Y. Cognitive behavioural therapy for anxiety disorders in children and adolescents: a meta-analysis. Child Adolesc Ment Health. 2007;12:164–72.
Silverman WK, Pina AA, Viswesvaran C. Evidence-based psychosocial treatments for phobic and anxiety disorders in children and adolescents. J Clin Child Adolesc Psychol. 2008;37:105–30.
Wergeland GJH, Fjermestad KW, Marin CE, Haugland BSM, Bjaastad JF, Oeding K, et al. An effectiveness study of individual vs. group cognitive behavioral therapy for anxiety disorders in youth. Behav Res Ther. 2014;57:1–12.
Sanchez AL, Cornacchio D, Poznanski B, Golik AM, Chou T, Comer JS. The effectiveness of school-based mental health services for elementary-aged children: a meta-analysis. J Am Acad Child Adolesc Psychiatry. 2018;57:153–65.
Werner Seilder A, Perry Y, Calear AL, Newby JM, Christensen H. School-based depression and anxiety prevention programs for young people: A systematic review and meta-analysis. Clin Psychol Rev. 2017;51:30–47.
R Ruttledge E Devitt G Greene M Mullany E Charles J Frehill M Moriarty 2016 A randomised controlled trial of the FRIENDS for Life emotional resilience programme delivered by teachers in Irish primary schools Child Psychology 33 69 89
Walkup JT, Albano AM, Piacentini J, Birmaher B, Compton SN, Sherrill JT, et al. Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. N Engl J Med. 2008;359:2753–66.
Neil AL, Christensen H. Efficacy and effectiveness of school-based prevention and early intervention programs for anxiety. Clin Psychol Rev. 2009;29:208–15.
Barrett PM, Turner C. Prevention of anxiety symptoms in primary school children: preliminary results from a universal trial. Br J Clin Psychol. 2001;40:399–410.
Lowry-Webster HM, Barrett PM, Dadds MR. A universal prevention trial of anxiety and depressive symptomatology in childhood: preliminary data from an Australian study. Behav Change. 2001;18:36–50.
Barrett PM, Lock S, Farrell LJ. Developmental differences in universal preventive intervention for child anxiety. Clin Child Psychol Psychiatry. 2005;10:539–55.
Essau CA, Conradt J, Sasagawa S, Ollendick TH. Prevention of anxiety symptoms in children: results from a universal school-based trial. Behav Ther. 2012;43:450–64.
Urao Y, Yoshinaga N, Asano K, Ishikawa R, Tano A, Sato Y, et al. Effectiveness of a cognitive behavioural therapy-based anxiety prevention programme for children: a preliminary quasi-experimental study in Japan. Child Adolesc Psychiatry Ment Health. 2016;10:4. https://doi.org/10.1186/s13034-016-0091-x.
Urao Y, Yoshida M, Koshiba T, Sato Y, Ishikawa S, Shimizu E. Effectiveness of a cognitive behavioural therapy-based anxiety prevention programme at an elementary school in Japan: a quasi-experimental study. Child Adolesc Psychiatry Ment Health. 2018;12:33.
Masia-Warner C, Klein RG, Dent HC, Fisher PH, Alvir J, Albano AM, et al. School-based intervention for adolescents with social anxiety disorder: results of a controlled study. J Abnorm Child Psychol. 2005;33:707–22.
Mychailyszyn MP, Beidas RS, Benjamin CL, Edmunds JM, Podell JL, Cohen JS, et al. Assessing and treating child anxiety in schools. Psychol Sch. 2011;48:223–32.
Özabacı N. Cognitive behavioural therapy for violent behaviour in children and adolescents: a meta-analysis. Child Youth Serv Rev. 2011;33:1989–93.
Mcloone J, Hudson JL, Rapee RM. Treating anxiety disorders in a school setting. Educ Treat Child. 2006;29:219–42.
August GJ, Lee SS, Bloomquist ML, Realmuto GM, Hektner JM. Maintenance effects of an evidence-based prevention innovation for aggressive children living in culturally diverse urban neighborhoods: the Early Risers effectiveness study. J Emot Behav Disord. 2004;12:194–205.
Challen AR, Machin SJ, Gillham JE. The UK resilience programme: a school-based universal nonrandomized pragmatic controlled trial. J Consult Clin Psychol. 2014;82:75–89.
August GJ, Lee SS, Bloomquist ML, Realmuto GM, Hektner JM. Dissemination of an evidence-based prevention innovation for aggressive children living in culturally diverse, urban neighbor hoods: the Early Risers effectiveness study. Prev Sci. 2003;4:271–86.
Costello EJ, Mustillo S, Erkanli A, Keeler G, Angold A. Prevalence and development of psychiatric disorders in childhood and adolescence. Arch Gen Psychiatry. 2003;60:837–44.
Stallard P, Simpson N, Anderson S, Carter T, Osborn C, Bush S. An evaluation of the friends programme: a cognitive behaviour therapy intervention to promote emotional resilience. Arch Dis Child. 2005;90:1016–9.
Spence SH. A measure of anxiety symptoms among children. Behav Res Ther. 1998;36:545–66.
Ishikawa S, Sato H, Sasagawa S. Anxiety disorder symptoms in Japanese children and adolescents. J Anxiety Disord. 2009;23:104–11.
Goodman R, Meltzer H, Bailey V. The strengths and difficulties questionnaire: a pilot study on the validity of the self-report version. Eur Child Adolesc Psychiatry. 1998;7:125–30.
Harada S, Ito D, Mochizuki N, Tanaka Y, Daigoku S, Takayanagi S, et al. Examining the construct validity of the Japanese version of the Strengths and Difficulties Questionnaire-self rating Form: correlations with depression, aggression, and the SDQ-Parent Rating Form. Psychiatr Neurol Paediatr Jpn. 2014;53:343–51.
Mallinckrodt CH, Clark WS, David SR. Accounting for dropout bias using mixed-effects models. J Biopharm Stat. 2001;11:9–21.
Siddiqui O, Hung HM, O’Neill R. MMRM vs. LOCF: a comprehensive comparison based on simulation study and 25 NDA datasets. J Biopharm Stat. 2009;19:227–46.
Little RJ, D’Agostino R, Cohen ML, Dickersin K, Emerson SS, Farrar JT, et al. The N Engl J Med. 2012;367:1355–60.
National Research Council. The prevention and treatment of missing data in clinical trials. Washington, DC: National Academies Press; 2010. http://www.nap.edu/catalog.php?record_id-12955. Accessed 9 December 2017.
Cohen J. Statistical Power Analysis in the Behavioral Sciences. 2nd ed. Hillsdale: Erlbaum; 1988.
Urao Y, Ohira I, Koshiba T, Ishikawa S, Sato Y, Shimizu E. Classroom-based cognitive behavioural therapy: a large-scale non-randomised controlled trial of the ‘Journey of the Brave.’ Child Adolesc Psychiatry Ment Health. 2021;15:21.
Greene RW, Ollendick TH. Evaluation of a multidimensional program for sixth-graders in transition from elementary to middle school. J Community Psychol. 1993;21:162–76.
Acknowledgements
We would like to thank the school, children, and parents who participated in the study.
Funding
This work was supported by JSPS KAKENHI Grant Number 15K21267.
Author information
Authors and Affiliations
Contributions
YU, MY, and ES designed the study. ES managed and supervised the study. MY conducted this programme and collected the data. YU and MY managed the database and YS analysed the data. YU and MY drafted the report. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol was approved by the ethics committee of Chiba University in accordance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects as well as the Declaration of Helsinki. All methods were carried out in accordance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects. Signed parental consent for the participation of children was obtained following the informed consent procedure. Our study was performed in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Urao, Y., Yoshida, M., Sato, Y. et al. School-based cognitive behavioural intervention programme for addressing anxiety in 10- to 11-year-olds using short classroom activities in Japan: a quasi-experimental study. BMC Psychiatry 22, 658 (2022). https://doi.org/10.1186/s12888-022-04326-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-022-04326-y