
Abstract
Background
Exposure to air pollution is an important risk factor for intracerebral hemorrhage (ICH), which is a major cause of death worldwide. However, the relationship between ICH mortality and air quality improvement has been poorly studied. This study aims to evaluate the impact of the air pollution control policies in the Beijing-Tianjin-Hebei region on ICH mortality among Tianjin residents.
Methods
This study used an interrupted time series analysis. We fitted autoregressive integrated moving average (ARIMA) models to assess the changes in ICH deaths before and after the interventions of air pollution control policies based on the data of ICH deaths in Tianjin collected by the Tianjin Center for Disease Control and Prevention.
Results
Between 2009 and 2020, there were 63,944 ICH deaths in Tianjin, and there was an overall decreasing trend in ICH mortality. The intervention conducted in June 2014 resulted in a statistically significant (p = 0.03) long-term trend change, reducing the number of deaths from ICH by 0.69 (95% confidence interval [CI]: -1.30 to -0.07) per month. The intervention in October 2017 resulted in a statistically significant (p = 0.04) immediate decrease of 25.74 (95% CI: -50.62 to -0.85) deaths from ICH in that month. The intervention in December 2017 caused a statistically significant (p = 0.04) immediate reduction of 26.58 (95% CI: -52.02 to -1.14) deaths from ICH in that month. The intervention in March 2018 resulted in a statistically significant (p = 0.02) immediate decrease of 30.40 (95% CI: -56.41 to -4.40) deaths from ICH in that month. No significant differences were observed in the changes of male ICH mortality after any of the four interventions. However, female ICH deaths showed statistically significant long-term trend change after the intervention in June 2014 and immediate changes after the interventions in December 2017 and March 2018. Overall, the interventions prevented an estimated 5984.76 deaths due to ICH.
Conclusion
During the study period, some interventions of air pollution control policies were significantly associated with the reductions in the number of deaths from ICH among residents in Tianjin. ICH survivors and females were more sensitive to the protective effects of the interventions. Interventions for air pollution control can achieve public health gains in cities with high levels of air pollution.
Similar content being viewed by others

Background
Stroke is the second leading cause of death globally, resulting in over 6 million deaths annually, including 2 million in China [1]. Intracerebral hemorrhage (ICH) is the second most common subtype of stroke, characterized by high morbidity, disability, and mortality. It causes a severe burden on patients and society in China and worldwide [2, 3].
In China, hemorrhagic stroke comprises a greater proportion of all stroke cases compared to in western countries [1]. In 2016, the incidence of ischemic stroke in China was approximately twice that of hemorrhagic stroke, but hemorrhagic stroke had a higher mortality rate than ischemic stroke [4]. Moreover, hemorrhagic stroke contributed more to years of life lost (YLL) and disability adjusted life years (DALYs) than ischemic stroke, indicating that hemorrhagic stroke poses a greater risk of premature death for the Chinese population [5].
The 2015 Global Burden of Disease Study analyzed the 25 years of data and found that air pollution significantly affects DALYs and mortality caused by ischemic heart disease, cerebrovascular disease, and chronic obstructive pulmonary disease [6]. In fact, growing evidence suggests that short-term exposure to air pollution increases the incidence and mortality of ICH [7,8,9,10,11].
Tianjin, located in the Beijing-Tianjin-Hebei region, with a total resident population of 15.6 million, is the largest open coastal city in northern China [12]. In 2015, the mortality rate of ICH in Tianjin was 51.46/100,000, while the standardized mortality rate was 29.00/100,000 [13]. The mortality rate of ICH in Tianjin was decreasing in the population aged ≥ 45 years, but the mortality rate in those aged < 35 years, especially in men, was increasing [13].
The Beijing-Tianjin-Hebei region suffered the heaviest air pollution in China due to multiple factors, including the concentrations of heavy industries, geographical location, and meteorological conditions that are not conducive to the diffusion of pollutants. The annual average concentrations of major pollutants such as Fine particulate matter (PM2.5), Coarse particulate matter (PM10), Sulphur dioxide (SO2), and Nitrogen dioxide (NO2) in the Beijing-Tianjin-Hebei region are higher than the national average, and the air pollution is particularly severe after entering the heating period in winter [14]. In 2014, 1,710 severe pollution events occurred in 70 cities at or above the prefecture level in Beijing-Tianjin-Hebei and surrounding areas, accounting for 41% of the national total [15].
In order to control air pollution and protect people's health and economic development, the Chinese government implemented a series of intervention policies. In June 2014, the "Key Work of Joint Prevention and Control for Air Pollution in Beijing-Tianjin-Hebei and Surrounding Areas in 2014" was officially published. The policy required the Beijing-Tianjin-Hebei region and the surrounding areas to take unified actions to manage industrial emissions and traffic pollution jointly in the region [16]. Additionally, in response to the aggravation of air pollution in autumn and winter, the Ministry of Environmental Protection issued "The Action Plan for Air Pollution Comprehensive Control in Beijing-Tianjin-Hebei and Its Surrounding Areas in Autumn and Winter 2017–2018" in 2017 [16].
Several studies have found that comprehensive air pollution prevention measures have led to sustained improvements in air quality in the Beijing-Tianjin-Hebei region and surrounding areas [17,18,19]. The annual average concentrations of air pollutants (PM2.5, PM10, SO2, NO2, and CO) have decreased. Additionally, the days of heavy and serious air pollution each year have significantly decreased, while the number of days with good and excellent air quality has increased yearly.
Since the implementation of the air pollution control policy in 2014, the ICH mortality in Tianjin has decreased year by year. The reduction in air pollution exposure is expected to impact ICH deaths, but the specific impact of these policies on public health is not yet clear.
To the best of our knowledge, no previous research has yet evaluated the impact of air pollution intervention policies on cerebral hemorrhage deaths in China. As the implementation of the policies provided rare natural experiments, this study used an interrupted time series analysis to quantitatively assess the effects of the policies on the number of ICH deaths by comparing the changes in the number of ICH deaths in Tianjin before and after the implementation of the policies.
Materials and methods
Data
The death data of ICH from January 1, 2009, to December 31, 2020, were obtained from the All Cause of Death Registration System (CDRs) of Tianjin Center for Disease Control and Prevention, which covers the whole population of Tianjin. All deaths caused by ICH were identified using death certificates with death codes I61.x and I69.1 according to the International Classification of Disease, 10th Revision (ICD-10). In order to ensure the reliability of death data, the overall quality control of death certificates is carried out through a step-by-step quality audit, sampling review, and regular underreporting investigations.
The number of registered population in Tianjin comes from the Population Management Office of Tianjin Public Security Bureau. The sixth National Population Census data was provided by The National Statistics Bureau of China [20].
Design
This study used interrupted time series (ITS) analysis, which is a quasi-experimental design. It is widely used to examine the effects of public health interventions because it is well suited for evaluating health-related outcomes over a defined period at the population level [21, 22]. During the study period, different cities in China had different air pollution control policies, making it difficult to find comparable parallel control groups [17]. Therefore, ITS analysis is appropriate for this study. ITS analysis differs from other intervention study designs in that it involves a before-after comparison within a single population rather than a comparison with a control group [23].
The pre-post design compares the results of indicators before and after the intervention, which may be confounded by biases such as secular trend, cyclical or seasonal effects, random fluctuations, and autocorrelation, making it difficult to draw reliable conclusions [24, 25]. While the interrupted time series design controls for pre- and post-intervention trends by constructing the time series with multiple measurements of the variables before and after the intervention and then using an appropriate model such as a regression model or an autoregressive integrated moving average (ARIMA) model [25].
Modeling using linear regression, logistic regression, or Poisson regression models is a common approach for ITS. Regression models require that the trend conforms to a linear hypothesis. If the regression model is incorrectly used without satisfying the linearity hypothesis, the estimate of policy impact will be biased [26]. When the time series has seasonality or autocorrelation or does not satisfy the linear hypothesis, the ARIMA model can solve these problems [27].
The pre-intervention trend is interrupted at the time of the intervention, and the predicted value that assumes no intervention and the trend continues is called counterfactual. ITS analysis evaluates the effects of interventions by comparing the difference between counterfactual and actual observations [22, 25].
The interventions evaluated were the beginning and end of two air pollution control policies. At the beginning of this study, we consulted official websites of the Chinese and local governments. During the study period, no other air pollution control policies were implemented in the Beijing, Tianjin, and Hebei regions. According to the reports on these websites [16, 28], we compiled the time and content of the four interventions studied in Table 1.
Statistical analysis
The crude mortality rates for ICH and acute ICH were calculated by dividing the annual number of deaths by the population of Tianjin for the corresponding year. The age-sex standardized mortality rate was calculated using the sixth National Population Census data in 2010 as the standard population number.
In order to evaluate the impact of air pollution prevention measures on ICH and acute ICH deaths, this study based on the guidelines [27], using seasonal ARIMA models to fit the time series of the number of all ICH (ICD-10 codes I61.x and I69.1) deaths and the number of acute ICH deaths excluding sequelae of cerebral hemorrhage (ICD-10 code I69.1) in Tianjin. The models identified potential secular trends in mortality for different ICH classifications and predicted scenarios in which no interventions occurred and the trend would continue unchanged.
The seasonal ARIMA model is an analytical tool for modeling data with seasonal fluctuations in the time series. It consists of a combination of two simple models, ARIMA (p, d, q) for the non-seasonal component and ARIMA (P, D, Q) for the seasonal component. The general form of the model is ARIMA (p,d,q) × (P,D,Q)S (p is the autoregressive order, q is the moving average order,and d is differencing order; P is the seasonal autoregressive order, Q is the moving average order, D is the seasonal differencing order, and S is the seasonal period) [29].
In this study, the auto.arima()in the forecast package for R is used to identify model parameters and obtain several alternative models automatically [30]. Then, the optimal model is determined based on the residual test results and the Akaike information criterion (AIC) and Bayesian information criterion (BIC).
In order to test the validity of the model, in addition to the test of autocorrelation and normal distribution of the residuals, the Ljung-Box test is also required. When the p-value is > 0.01, it indicates that the residual series is a white noise series, and the fitted model is able to extract almost all of the sample-related information from the series of observations, making the model significantly valid. When the p-value is < 0.01, the original data will be transformed to conform to normality using the Box-Cox transformation and re-fit the model.
The variables that explain the intervention in the model include the immediate change variable and the long-term trend change variable. The immediate change variable takes the value of 0 before the start of the intervention and 1 after that, while the long-term trend change variable takes the values of 0 to n, with 0 representing no intervention and 1 to n indicating the months after the intervention.
In this study, the counterfactual predicted ICH deaths were compared with the observed deaths using the beginning and end of the two air pollution control policies as the intervention time points. The effects of the air pollution control policies on ICH deaths was evaluated by calculating the immediate changes and long-term trend changes induced by the interventions.
All analyses in this study were performed in R (v.4.2.0).
Results
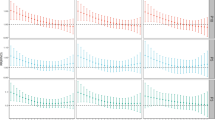
There were 63,784 deaths due to ICH (the ICD-10 codes are I61.x and I69.1) in Tianjin from January 1, 2009, to December 31, 2020, and there were 53,788 acute ICH deaths after excluding the sequelae of cerebral hemorrhage (the ICD-10 code is I69.1). Both the crude mortality rate and age-sex standardized mortality rate of ICH showed a general downward trend. The number of deaths exhibited an annual periodicity and a seasonal trend, with peaks in winter and troughs in summer. The number of deaths, crude mortality rate, and age-sex standardized mortality rate of ICH and acute ICH are reported in Table 2. Figure 1 shows the time series of deaths from ICH and acute ICH.

Time series of deaths from ICH and acute ICH in Tianjin from 2009 to 2020
Select model
The parameters of traditional ARIMA models are determined from autocorrelation and partial autocorrelation plots, which are to some extent subjective. Therefore we identified the ARIMA model terms by using auto.arima() in the forecast package for R. The automatic algorithm was used to find the optimal model with the lowest AIC or BIC. The impact of the air pollution prevention and control policies on ICH mortality was quantitatively evaluated using the optimal ARIMA model.
The tests results indicate that the residuals are normally distributed and not significantly autocorrelated. Meanwhile, the models were subjected to the Ljung-Box test, and the residual series are white noise sequences. Our fitted models can extract almost all the sample-related information from the observation series. Therefore, the models are all significantly effective. The goodness-of-fit of models was assessed using the mean absolute percentage error (MAPE). The results are presented in Table 3.
Model prediction
Interrupted time series analysis revealed a statistically significant change in long-term trend of ICH deaths in Tianjin following the intervention in June 2014. Additionally, statistically significant immediate changes were observed following the interventions in October 2017, December 2017, and March 2018.
The number of deaths due to ICH in Tianjin decreased by 0.69 (95% CI: -1.30 to -0.07) per month under a sustained long-term trend after the intervention in June 2014. The model predicts that 54.51 (95% CI: -102.70 to -5.53) fewer ICH deaths could have been achieved with the impact of that trend during the study period. There were immediate changes that the ICH deaths in Tianjin decreased by 25.74 (95% CI: -50.62 to -0.85), 26.58 (95% CI: -52.02 to -1.14), and 30.40 (95% CI: -56.41 to -4.40) after the interventions in October 2017, December 2017, and March 2018 respectively.
There were no statistically significant differences in the immediate or long-term changes of male ICH deaths in Tianjin after the four interventions. In comparison, female ICH deaths had statistically significant long-term trend changes after the intervention in June 2014 and immediate changes after the interventions in December 2017 and March 2018.
The female ICH deaths in Tianjin decreased by 0.37 (95% CI: -0.61 to -0.13) per month under a sustained long-term trend after the intervention in June 2014. It predicts that 29.23 (95% CI: -48.19 to -10.27) fewer ICH deaths could have been achieved with the impact of that trend during the study period. There were immediate changes that the female ICH deaths in Tianjin decreased by 12.87 (95% CI: -23.7 to -1.98) and 13.08 (95% CI: -24.40 to -1.75) after the interventions in December 2017 and March 2018, respectively.
As is shown in Table 4, there was only a statistically significant immediate change in male acute ICH deaths after the intervention in October 2017, with an immediate reduction in deaths of 22.46 (95% CI: -42.76 to -2.15) in that month. While other changes in acute ICH deaths were not statistically significant according to the interrupted time series analyses.
Without these air pollution control interventions, the number of ICH deaths between June 2014 and December 2020 is estimated to be 37,758.76. It is predicted that 5984.76 ICH deaths will be averted after the implementation of the intervention, reducing expected deaths by 15.85%. The results are presented in Fig. 2.

Comparison of observed and predicted ICH deaths
Discussion
Due to the implementation of the comprehensive air pollution control policies, emissions of air pollutants in the Beijing-Tianjin-Hebei region decreased significantly [17, 31]. Several studies have shown that significant improvements in air quality have correspondingly improved human health in the study area [19, 32]. During 2009 to 2010 and 2012 to 2013, the mortality of ICH in Tianjin exhibited an upward trend. However, the mortality of ICH in Tianjin declined immediately and significantly and has continued to decline since the implementation of air pollution control policies in 2014.
The results indicated that the policy interventions had different effects on ICH mortality, possibly due to the varying goals and contents of the interventions at each stage. The long-term trend change caused by the intervention of the air pollution control policy on ICH deaths in June 2014 was statistically significant. At that time, the " Key Work of Joint Prevention and Control for Air Pollution in Beijing-Tianjin-Hebei and Surrounding Areas in 2014 " was officially published, and unified actions were carried out in Beijing-Tianjin-Hebei and surrounding regions to prevent and control air pollution [16]. Immediate changes in ICH deaths in October 2017, December 2017, and March 2018 were statistically significant. It may be associated with the government's intensified inspections and interventions to achieve air quality-related targets at the beginning and end of the policy's implementation. Therefore, the air quality in Tianjin improved at those time points, leading to significant decreases in ICH deaths.
Gender differences were observed in the effects of the interventions on ICH deaths, as shown in the stratified analysis: There was a statistically significant long-term trend change in ICH deaths for females in June 2014 and statistically significant immediate changes for females in December 2017 and March 2018. In contrast, there were no statistically significant long-term trend or immediate changes in ICH deaths for males. In addition, the results showed that none of those interventions had statistically significant effects on immediate or long-term trend changes in acute ICH mortality among all residents or female residents in Tianjin. These findings suggest that surviving ICH patients and females may be more sensitive to the protective effects of air pollution control policies.
A cohort study conducted in the UK, which accounted for a wide range of potential confounders, demonstrated that the survival rates of stroke patients would decline if they lived in areas with higher levels of air pollution [33]. Another large population-based cohort study showed that patients with hemorrhagic stroke were at a high risk for secondary cardiovascular disease. Compared with ischemic stroke patients, the cardiovascular and all-cause mortality risk in patients with hemorrhagic stroke increased significantly during follow-up [34]. Another analysis of four population-based studies concluded that ICH was associated with an approximately twofold increased risk of arterial ischemic events, ischemic stroke, and myocardial infarction [35].
Numerous studies have consistently demonstrated that women have a worse prognosis after stroke than men [36,37,38]. Despite higher stroke morbidity and mortality rates among men at specific ages, a greater number of women are affected by stroke due to their longer lifespan and the significantly higher incidence of stroke in the oldest age group [39, 40]. In addition, stroke-related outcomes such as disability and quality of life (QOL) are consistently worse among women than men [40].
Several related studies have shown results consistent with our study, indicating that air pollution is associated with an increased risk of ICH mortality. It was found that short-term exposure to NO2 was associated with increased hospital admissions for ICH in a study involving 14 major cities in China [7].There was a positive association between short-term exposure to PM2.5 and mortality of hemorrhagic stroke, with each 10 μg/m3 increase in PM2.5 associated with a 0.37% (95%CI: 0.07% to 0.67%) increase in mortality of hemorrhagic stroke according to a study in Beijing, China [41]. Moreover, a study in Shanghai, China, concluded similarly that the incidence of fatal ICH was associated with PM2.5 exposure [10]. In addition, short-term exposure to ambient SO2 was found to increase the risk of hospitalization for hemorrhagic stroke in a study in Guangzhou, China. The effect that SO2 had on the risk of hemorrhagic stroke reached the maximum value on lag 1 day, with a percentage change of 1.55% (95%CI: 0.02% to 3.11%) per 10 μg/m3 [42]. In the Greater Boston area of the United States, a study suggested that the risk of ICH increased after short-term exposure to ozone [43]. A study conducted in Korea found that a correlation between ozone exposure and subarachnoid hemorrhage as well as a positive association between PM10 and the incidence of ICH [44]. However, certain studies conducted in developed Western countries found that no significant association between air pollution and ICH deaths [45, 46]. This discrepancy may be attributed to differences in composition of air pollutants, pollution levels, meteorological factors, population susceptibility, and other factors between developed and developing countries [47].
Exposure to air pollution is an important risk factor for cardiovascular disease and leads to an increased risk of hemorrhagic stroke by biologically plausible mechanisms. Some pathophysiological alterations caused by air pollution may be related to ICH, such as arterial vasoconstriction, increased blood pressure, and increased vulnerability of brain vessel rupture due to endothelial dysfunction [48]. However, further research is required.
As shown in Fig. 1, the difference between the number of ICH and acute ICH deaths in Tianjin from 2009 to 2020 exhibited an increasing trend, indicating a decrease in acute deaths among all ICH deaths. It was probably due to residents receiving more timely treatment after the onset of ICH, which is associated with the improvement of economic development, the increase in medical resources, the promotion and education of prevention, and the adjustment of health insurance policies [49]. In recent years, Tianjin has established a number of stroke centers, which have played an essential role in the early diagnosis of stroke, reducing time to treatment and decreasing stroke mortality.
In addition to air pollution control policy, other interventions may have contributed to the reduction in ICH deaths, such as healthy lifestyle education, community health management of patients with hypertension since 2008, and the enactment of the Tianjin Act of Tobacco Control in 2012 [12, 50]. However, the implementation periods of these interventions are not consistent with the time points studied, suggesting that the reductions in ICH mortality are more likely to be related to the air pollution control policies.
In response to the outbreak of coronavirus disease 2019 (COVID-19), the Chinese government rapidly implemented a series of prevention and control measures [51]. During the epidemic, measures such as business shutdowns and vehicle restrictions reduced air pollution from industrial production and vehicle emissions [52], potentially affecting the reduction in ICH mortality. Future studies may specifically investigate the effects of COVID-19 prevention and control measures on ICH mortality in Tianjin residents.
Extensive literature has reported the association between air pollutants and stroke. However, few studies have investigated the effects of air pollution control policies on stroke and considered the types of stroke. The interventions of the Chinese government to reduce air pollution provided rare opportunities for quasi-experimental studies. The interrupted time series design is a widely used approach for evaluating policies. This design is based on observing a relatively stable population over time, which reduces the impact of inter-group differences, such as selection bias or unmeasured confounders [23]. In addition, ARIMA models account for within-group characteristics that slowly change long-term over time by modeling potential trends, such as rising economic levels and aging [23]. Another strength of this study is the use of data from The Tianjin All Causes of Death Surveillance System. The data involve a relatively fixed population and covers a long period (144 months in total). This population-based dataset provides greater statistical power to detect long-term trends and assess the health impact.
There are also some potential limitations in this study. Firstly, as an ecological study, it does not reflect the actual individual exposure levels. Therefore, individual-level confounding factors such as smoking, diet, physical activity and others cannot be entirely excluded. Secondly, there is a lack of comparison with other cities during the same period. Since corresponding air pollution control policies were implemented throughout China during the study period, it is difficult to find a comparable control group. Lastly, despite adjusting for underlying time trends, some other population-level variables not controlled for, such as obesity prevalence, prevalence of smoking, secondhand smoke exposure and influenza outbreaks, may have influenced the results, so a clear causal relationship between the reduction in ICH deaths and air pollution control measures cannot be established [23].
Conclusions
The results demonstrated that the interventions of air pollution control policy during the study were significantly associated with reductions in ICH deaths, with greater impacts observed among females and surviving ICH patients. These findings suggest that improving air quality can reduce deaths caused by ICH. This study highlights the importance of controlling air pollution as a preventive measure for ICH mortality. Other regions with high levels of air pollution urgently need to implement similar policies for air pollution control to obtain public health benefits.
Availability of data and materials
The data is from the All-Cause of Death Registration System of Tianjin Center for Disease Control and Prevention. It is not publicly available but is available from the corresponding author on reasonable request.
Abbreviations
- AIC:
-
Akaike Information Criterion
- ARIMA model:
-
Autoregressive Integrated Moving Average model
- BIC:
-
Bayesian Information Criterion
- CDRs:
-
All Cause of Death Registration System
- CI:
-
Confidence interval
- DALYs:
-
Disability adjusted life years
- ICH:
-
Intracerebral hemorrhage
- ITS:
-
Interrupted Time Series
- MAPE:
-
Mean Absolute Percentage Error
- NO2 :
-
Nitrogen dioxide
- PM2.5 :
-
Particulate matter with aerodynamic diameters of < 2.5 μm
- PM10 :
-
Particulate matter with aerodynamic diameters of < 10 μm
- QOL:
-
Quality of life
- SO2 :
-
Sulphur dioxide
- YLL:
-
Years of life lost
References
Sun L, Clarke R, Bennett D, Guo Y, Walters RG, Hill M, Parish S, Millwood IY, Bian Z, Chen Y, et al. Causal associations of blood lipids with risk of ischemic stroke and intracerebral hemorrhage in Chinese adults. Nat Med. 2019;25(4):569–74.
Tsai CF, Thomas B, Sudlow CL. Epidemiology of stroke and its subtypes in Chinese vs white populations: a systematic review. Neurology. 2013;81(3):264–72.
An SJ, Kim TJ, Yoon BW. Epidemiology, Risk Factors, and Clinical Features of Intracerebral Hemorrhage: An Update. J Stroke. 2017;19(1):3–10.
Wang Y, Zhou L, Guo J, Wang Y, Yang Y, Peng Q, Gao Y, Lu W. Secular trends of stroke incidence and mortality in China, 1990 to 2016: The Global Burden of Disease Study 2016. J Stroke Cerebrovasc Dis. 2020;29(8):104959.
Peng Q, Li HL, Wang Y, Lu WL. Changing trend regarding the burden on cerebrovascular diseases between 1990 and 2016 in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2019;40(4):400–5.
Ho A, Lim M, Zheng H, Leow AS, Tan BY, Pek PP, Raju Y, Seow WJ, Yeo TT, Sharma VK, et al. Association of ambient air pollution with risk of hemorrhagic stroke: A time-stratified case crossover analysis of the Singapore stroke registry. Int J Hyg Environ Health. 2022;240:113908.
Liu H, Tian Y, Xu Y, Huang Z, Huang C, Hu Y, Zhang J. Association between ambient air pollution and hospitalization for ischemic and hemorrhagic stroke in China: A multicity case-crossover study. Environ Pollut. 2017;230:234–41.
Dong G, Qian ZM, Wang J, Chen W, Ma W, Trevathan E, Xaverius PK, DeClue R, Wiese A, Langston M, et al. Associations between ambient air pollution and prevalence of stroke and cardiovascular diseases in 33 Chinese communities. Atmos Environ. 2013;77:968–73.
Niu Z, Liu F, Yu H, Wu S, Xiang H. Association between exposure to ambient air pollution and hospital admission, incidence, and mortality of stroke: an updated systematic review and meta-analysis of more than 23 million participants. Environ Health Prev Med. 2021;26(1):15.
Qian Y, Yu H, Cai B, Fang B, Wang C. Association between incidence of fatal intracerebral hemorrhagic stroke and fine particulate air pollution. Environ Health Prev Med. 2019;24(1):38.
Shah AS, Lee KK, McAllister DA, Hunter A, Nair H, Whiteley W, Langrish JP, Newby DE, Mills NL. Short term exposure to air pollution and stroke: systematic review and meta-analysis. BMJ. 2015;350:h1295.
Xiao H, Zhang H, Wang D, Shen C, Xu Z, Zhang Y, Jiang G, Yang G, Wan X, Naghavi M. Impact of smoke-free legislation on acute myocardial infarction and stroke mortality: Tianjin, China, 2007–2015. Tob Control. 2020;29(1):61–7.
Wang DZ, Xue XD, Zhang H, Xu ZL, Zhang Y, Song GD, Wang C, Jiang GH. The trend of intracerebral hemorrhage mortality of the residents with different characteristics in Tianjin, China, 1999–2015. Zhonghua Yu Fang Yi Xue Za Zhi. 2018;52(4):389–95.
Ren L, Yang W, Bai Z. Characteristics of Major Air Pollutants in China. Adv Exp Med Biol. 2017;1017:7–26.
Huang T, Yu Y, Wei Y, Wang H, Huang W, Chen X. Spatial-seasonal characteristics and critical impact factors of PM2.5 concentration in the Beijing-Tianjin-Hebei urban agglomeration. PLoS ONE. 2018;13(9):e201364.
Beijing Municipal Ecology and Environment Bureau. http://sthjj.beijing.gov.cn/bjhrb/index/xxgk69/sthjlyzwg/wrygl/601701/index.html. Accessed 20 Aug 2022.
Wang L, Zhang F, Pilot E, Yu J, Nie C, Holdaway J, Yang L, Li Y, Wang W, Vardoulakis S, et al. Taking Action on Air Pollution Control in the Beijing-Tianjin-Hebei (BTH) Region: Progress, Challenges and Opportunities. Int J Environ Res Public Health. 2018;15(2):306.
Liu S, Chu Y, Hu J. Clean Air Actions and Air Quality Improvements - Beijing-Tianjin-Hebei and Surrounding Areas, China, 2013–2019. China CDC Wkly. 2020;2(23):418–21.
Cao J, Qiu X, Peng L, Gao J, Wang F, Yan X. Impacts of the differences in PM(25) air quality improvement on regional transport and health risk in Beijing-Tianjin-Hebei region during 2013–2017. Chemosphere. 2022;297:134179.
National Statistics Bureau. http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm. Accessed 2 Feb 2023.
Zheng Y, Wu Y, Wang M, Wang Z, Wang S, Wang J, Wu J, Wu T, Chang C, Hu Y. Impact of a comprehensive tobacco control policy package on acute myocardial infarction and stroke hospital admissions in Beijing, China: interrupted time series study. Tob Control. 2020;30(4):434–42.
Bernal JL, Cummins S, Gasparrini A. Interrupted time series regression for the evaluation of public health interventions: a tutorial. Int J Epidemiol. 2017;46(1):348–55.
Lopez BJ, Cummins S, Gasparrini A. The use of controls in interrupted time series studies of public health interventions. Int J Epidemiol. 2018;47(6):2082–93.
Fretheim A, Zhang F, Ross-Degnan D, Oxman AD, Cheyne H, Foy R, Goodacre S, Herrin J, Kerse N, McKinlay RJ, et al. A reanalysis of cluster randomized trials showed interrupted time-series studies were valuable in health system evaluation. J Clin Epidemiol. 2015;68(3):324–33.
Ramsay CR, Matowe L, Grilli R, Grimshaw JM, Thomas RE. Interrupted time series designs in health technology assessment: lessons from two systematic reviews of behavior change strategies. Int J Technol Assess Health Care. 2003;19(4):613–23.
Kontopantelis E, Doran T, Springate DA, Buchan I, Reeves D. Regression based quasi-experimental approach when randomisation is not an option: interrupted time series analysis. BMJ. 2015;350:h2750.
Schaffer AL, Dobbins TA, Pearson SA. Interrupted time series analysis using autoregressive integrated moving average (ARIMA) models: a guide for evaluating large-scale health interventions. Bmc Med Res Methodol. 2021;21(1):58.
Central People's Government of the People's Republic of China. http://www.gov.cn/xinwen/2017-08/25/content_5220248.htm. Accessed 20 Aug 2022.
Hyndman RJ, Athanasopoulos G: Forecasting: principles and practice: OTexts; 2018.
Hyndman RJ, Khandakar Y. Automatic Time Series Forecasting: The forecast Package for R. J Stat Softw. 2008;27:1–22.
Dong Z, Wang S, Xing J, Chang X, Ding D, Zheng H. Regional transport in Beijing-Tianjin-Hebei region and its changes during 2014–2017: The impacts of meteorology and emission reduction. Sci Total Environ. 2020;737:139792.
Wang F, Qiu X, Cao J, Peng L, Zhang N, Yan Y, Li R. Policy-driven changes in the health risk of PM(2.5) and O(3) exposure in China during 2013–2018. Sci Total Environ. 2021;757:143775.
Maheswaran R, Pearson T, Smeeton NC, Beevers SD, Campbell MJ, Wolfe CD. Impact of outdoor air pollution on survival after stroke: population-based cohort study. Stroke. 2010;41(5):869–77.
Akyea RK, Georgiopoulos G, Iyen B, Kai J, Qureshi N, Ntaios G. Comparison of Risk of Serious Cardiovascular Events after Hemorrhagic versus Ischemic Stroke: A Population-Based Study. Thromb Haemost. 2022;122(11):1921–31.
Murthy SB, Zhang C, Diaz I, Levitan EB, Koton S, Bartz TM, DeRosa JT, Strobino K, Colantonio LD, Iadecola C, et al. Association Between Intracerebral Hemorrhage and Subsequent Arterial Ischemic Events in Participants From 4 Population-Based Cohort Studies. Jama Neurol. 2021;78(7):809–16.
Haast RA, Gustafson DR, Kiliaan AJ. Sex differences in stroke. J Cereb Blood Flow Metab. 2012;32(12):2100–7.
Branyan TE, Sohrabji F. Sex differences in stroke co-morbidities. Exp Neurol. 2020;332:113384.
Girijala RL, Sohrabji F, Bush RL. Sex differences in stroke: Review of current knowledge and evidence. Vasc Med. 2017;22(2):135–45.
Cfdc CDC. Prevalence of stroke–United States, 2005. MMWR Morb Mortal Wkly Rep. 2007;56(19):469–74.
Reeves MJ, Bushnell CD, Howard G, Gargano JW, Duncan PW, Lynch G, Khatiwoda A, Lisabeth L. Sex differences in stroke: epidemiology, clinical presentation, medical care, and outcomes. Lancet Neurol. 2008;7(10):915–26.
Zhang R, Liu G, Jiang Y, Li G, Pan Y, Wang Y, Wei Z, Wang J, Wang Y. Acute Effects of Particulate Air Pollution on Ischemic Stroke and Hemorrhagic Stroke Mortality. Front Neurol. 2018;9:827.
Shen S, Li X, Yuan C, Huang Q, Liu D, Ma S, Hui J, Liu R, Wu T, Chen Q. Association of short-term exposure to sulfur dioxide and hospitalization for ischemic and hemorrhagic stroke in Guangzhou, China. BMC Public Health. 2020;20(1):263.
Wilker EH, Mostofsky E, Fossa A, Koutrakis P, Warren A, Charidimou A, Mittleman MA, Viswanathan A: Ambient Pollutants and Spontaneous Intracerebral Hemorrhage in Greater Boston. Stroke 2018:2764–2766.
Han MH, Yi HJ, Ko Y, Kim YS, Lee YJ. Association between hemorrhagic stroke occurrence and meteorological factors and pollutants. BMC Neurol. 2016;16:59.
Maheswaran R, Pearson T, Smeeton NC, Beevers SD, Campbell MJ, Wolfe CD. Outdoor air pollution and incidence of ischemic and hemorrhagic stroke: a small-area level ecological study. Stroke. 2012;43(1):22–7.
Puett RC, Hart JE, Suh H, Mittleman M, Laden F. Particulate matter exposures, mortality, and cardiovascular disease in the health professionals follow-up study. Environ Health Perspect. 2011;119(8):1130–5.
Verhoeven JI, Allach Y, Vaartjes I, Klijn C, de Leeuw FE. Ambient air pollution and the risk of ischaemic and haemorrhagic stroke. Lancet Planet Health. 2021;5(8):e542–52.
Huang K, Liang F, Yang X, Liu F, Li J, Xiao Q, Chen J, Liu X, Cao J, Shen C, et al. Long term exposure to ambient fine particulate matter and incidence of stroke: prospective cohort study from the China-PAR project. BMJ. 2019;367: l6720.
Mendis S. Prevention and care of stroke in low- and middle-income countries; the need for a public health perspective. Int J Stroke. 2010;5(2):86–91.
Xue XD, Jiang GH, Li W, Zhang Y, Li DD, Xie MQ, Wang DZ. Epidemiological characteristics of hemorrhagic stroke among residents in Tianjin from 1999 to 2018. Zhonghua Liu Xing Bing Xue Za Zhi. 2021;42(8):1460–5.
Gao C, Li S, Liu M, Zhang F, Achal V, Tu Y, Zhang S, Cai C. Impact of the COVID-19 pandemic on air pollution in Chinese megacities from the perspective of traffic volume and meteorological factors. Sci Total Environ. 2021;773:145545.
Gao C, Zhang F, Fang D, Wang Q, Liu M. Spatial characteristics of change trends of air pollutants in Chinese urban areas during 2016–2020: The impact of air pollution controls and the COVID-19 pandemic. Atmos Res. 2023;283:106539.
Acknowledgements
Thanks to my mentor, Mr. Wang Dezheng, for the advice and assistance during his busy schedule. Thanks to Dr. Andrea Schaffer for the technical support. Thanks to the colleagues from the Institute for the Prevention and Control of Non-communicable Diseases of the Tianjin CDC and all the staff engaged in death surveillance for their contributions to data collection and quality control.
Funding
This study was funded by National Natural Science Foundation of China (81872590), Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-051A) and Project for Selection of Senior Health Talents in Tianjin (2018).
Author information
Authors and Affiliations
Contributions
Jiahui Xu Formal analysis, Writing – original draft, Methodology; Xiaolin Yin Reviewed the papers, Revised the manuscript; Tingting Jiang Reviewed the papers, Revised the manuscript; Shiyu Wang Reviewed the papers, Revised the manuscript; Dezheng Wang Writing – review & editing, Resources, Funding acquisition, Supervision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable. This study is a secondary data analysis, and no humans were involved.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xu, J., Yin, X., Jiang, T. et al. Effects of air pollution control policies on intracerebral hemorrhage mortality among residents in Tianjin, China. BMC Public Health 23, 858 (2023). https://doi.org/10.1186/s12889-023-15735-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15735-3