
Abstract
Background
Despite the harmful effects of smoking, there have been few studies to pinpoint the factors of this habit, and little is known about it in the East African region. For this reason, this study sought to determine the frequency and factors of cigarette smoking among men in the region.
Methods
Data from recent demographic and health surveys carried out in ten East African countries between 2015 and 2022 were analyzed in this study. Data from 87,022 men was collected. The key factors affecting the smoking rates in the area were investigated using binary and multiple multinomial logistic regression. To ascertain if variables were statistically significant in the final model for binary regression and multiple regression, P values of ≤ 0.2 and < 0.05 were used respectively.
Results
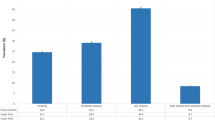
Overall, about 14.69% of people currently smoke cigarettes. Of this about 11.03 (95% CI = 10.82, 11.24) was for daily active tobacco use. As compared to < 26-year-old men, men with an age range of 26–35 years (RRR = 2.17, 95% CI: 2.01,2.34), 36–45 years (RRR = 2.82, 95% CI: 2.60, 3.07), and > 45 years old (RRR = 3.68, 95% CI: 3.38, 4.02), were using cigarettes daily rather than no-smoking cigarettes. Men who had begun their first sexual intercourse at the age of 7–19 years (RRR = 6.27,95% CI, 5.35,7.35), 20–25 years (RRR = 4.01, 95% CI, 3.40,4.72), and greater than 25 years old (RRR = 3.08, 95% CI, 2.55,3.71) have shown a higher relative risk ratio to smoke cigarette daily rather than using not smoke cigarette respectively, married (RRR = 0.86, 95% CI, 0.79,0.93), divorced or widowed (RRR = 2.51, 95% CI, 2.27,2.77), middle wealth index (RRR = 2.11, 95% CI 1.98,2.24), and rich (RRR = 1.44, 95% CI, 1.34,1.54), secondary/higher education (RRR = 0.72, 05% CI, 0.66,0.77), rural men (RRR = 0.69, 95% CI, 0.65,0.73), employed men (RRR = 1.26,95% CI, 1.17,1.36), mass media exposure (RRR = 0.76, 95% CI, 0.73,0.81), men who have one sex partner (RRR = 1.23,95% CI,1.13,1.35), and more than one sex partner (RRR = 1.63, 95% CI, 1.47,1.79) more times as compared to those participants who had no sex partner respectively.
Conclusions
Men in East African nations were substantially more likely to smoke cigarettes if they were older, had less education, had a higher wealth index, were divorced or widowed, had many sexual relationships, had early sexual activity, resided in an urban area, were employed, or had no media exposure. The identified factors should be considered by policymakers and public health professionals to lower smoking initiation and increase smoking cessation among men.
Similar content being viewed by others
Introduction
The use of tobacco is one of the major preventable causes of death worldwide, contributing to an epidemic of Non-Communicable Diseases (NCDs) such as cancer, heart disease, stroke, chronic lung disease, and others [1]. Additionally, it is a significant global preventable cause of early death and disease [1, 2]. Around 1.4 billion adults worldwide, comprising 1.07 billion smokers and 367 million smokeless tobacco users, used tobacco in 2017; the age-standardized global average prevalence of smoking is 19.2% [3]. It led to almost 8 million deaths annually, with those over 45 experiencing a markedly higher mortality risk [3, 4].
According to studies conducted in wealthy nations, the rate of cigarette smoking has sharply declined recently [5]. However, it is frighteningly rising in low-income nations [6, 7]. According to the WHO estimate for 2023, 80% of the 1.3 billion tobacco smokers worldwide reside in low- and middle-income nations [1]. About 36.7% of males and 7.8% of women worldwide used cigarettes in 2020, totaling 22.3% of the population [1]. According to data from the Global Tobacco Surveillance, men in sub-Saharan Africa smoke cigarettes at rates that range from 20 to 60% nationally, and both men and women are using tobacco more often each year [8]. Men and women smoke at rates of 4% and less than 1%, respectively, per the 2016 Ethiopian Demographic and Health Survey (EDHS) report [9].
Numerous studies on the effects of smoking cigarettes have been done. Cigarette smoking among men is attributed to a number of factors, including exposure to smokers (friends, parents, and teachers), the availability of tobacco, low socioeconomic status, subpar academic performance, low self-esteem, a lack of perceived risk of use, and a lack of ability to fend off influences to use tobacco [10,11,12]. Additionally, marital status, wealth, occupation, education, engaging in physical altercations, abusing alcohol, using marijuana, and engaging in sexual activity are all linked to smoking cigarettes [13,14,15].
The WHO set a goal to reduce mortality from chronic respiratory illnesses, cancer, diabetes, and cardiovascular diseases by 25% among people aged 30 to 70 between 2010 and 2025 [16]. The most efficient and cost-effective way to prevent non-communicable diseases in East African nations is to reduce cigarette consumption. Assessing the prevalence and related characteristics in East African nations is crucial because men smoke more cigarettes than smokeless tobacco. Several African nations have ratified the WHO Framework Convention on Tobacco Control, which forbids the use of cigarettes and any other tobacco products in any indoor or outdoor space that may influence child tobacco use [17, 18]. However, there is a lack of information on smoking in East Africa. Furthermore, gender disparity (males smoke more frequently than females), recent empirical knowledge, and current evidence gaps using the recent national health survey data were among the top research gaps that have been addressed in this study. Therefore, the purpose of this study was to utilize multinomial logistic regression to determine the prevalence, frequency, and associated characteristics of cigarette smoking among men in East Africa.
Methods
Study setting and period
With the most recent Demographic and Health Survey (DHS) data, we conducted secondary data analysis in the following East African nations from 2011 to 2022: Burundi, Ethiopia, Kenya, Madagascar, Malawi, Rwanda, Tanzania, Uganda, Zambia, and Zimbabwe. Sample size, and study periods are described below (Table 1).
With a significant emphasis on indicators of fertility, reproductive health, mother and child health, mortality, nutrition, and self-reported health behaviors among adults, the DHS gathers a wide range of objective and self-reported data. Epidemiological research that monitors prevalence, trends, and inequities is made easier by data from the DHS. For the population of the nation, it drew samples that were nationally representative. The nature of the datasets from demographic and health surveys has been described in full elsewhere [19].
Data source
The demography and health survey (DHS) program’s official database, www.measuredhs.com, was used to obtain the data. Population, health, and nutrition monitoring and impact evaluation indicators can be used using data from demographic and health surveys, which are nationally representative household surveys. The DHS employs a stratified two-stage cluster design, with enumeration areas (EA) being the first stage and a sample of homes being picked from each EA in the second. Comprehensive survey methodology [19].
Sample size determination and sampling method
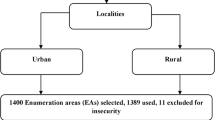
For around 10 of the 13 countries in East Africa, there were recent Demographic and Health Survey (DHS) reports available. The most current conventional census frame was used for each survey taken in the nations mentioned below. The DHS samples frequently divide each administrative geographic region into urban and rural areas. During the first round of sampling, enumeration areas (EAs) were chosen with a probability proportional to their size within each stratum. The systematic sampling strategy chooses a specified number of homes in the chosen EAs in the second stage. After listing the households, a certain number of households from the designated cluster are chosen using equal probability systematic sampling [19].
Data management and statistical analysis
The data set was collected from the website https://dhsprogram.com after receiving a letter from the DHS approving its utilization. Data extraction, recoding, and analysis are performed using Stata version 17. The study included weighting to ensure representativeness, reduce the non-response rate, and produce an accurate statistical estimate (robust standard error) [20]. In binary regression, those variables whose values were less than or equal to 0.20 were selected as candidate variables for the multiple multinomial logistic regression model to estimate factors associated with smoking at a 95% confidence interval (Table 2). In the binary regression, each independent variable was regressed independently to assess whether it fits the minimum p-value of less than or equal to be selected as a candidate variable for the final model. To identify the contributing factors to the prevalence of cigarette smoking among men, a multiple multinomial logistic model was used. The model’s best fit Adjusted Odds Ratio (AOR) with 95% CI was supplied. The descriptive data were compiled using descriptive research, such as frequency count and proportion for categorical data. Bivariable logistic regression was used to choose potential variables for multiple multinomial logistic regression. A logistic model was fitted to test for multicollinearity among the independent variables using the variance inflation factor. The overall fitness of the final regression model was further assessed using the Hosmer and Lemeshow test. The statistical significance level for the final model was set at < 0.05.
Model goodness fits and comparison
As candidate models, three models binary logistic, ordinal, and multinomial logistic regressions were chosen. Given that smoking rates were listed as (no smoking, every day, and occasionally), an approach that was widely utilized was the ordinal logistic regression mode. However, after we tested the proportional odds model (POM) for model Stata command or Brant test, the assumption of the POM was not met, therefore we used a multinomial logistic regression model instead. Actually, there were modest differences between the three models and important parameters. To choose the best ordinal model for the data, use the POM assumptions, which state that all independent factors’ effects are constant across all categories of the outcome variable. The Brant test (p = 0.0001) and the omodel Stata tool were used to confirm the POM assumption’s validity. Comparing ordinal logistic regression models to multinomial models, the AIC, BIC, and LLR were similarly slightly bigger in the ordinal models. As a result, we did not use the POM to examine the relationships between the independent variables and the three categories of cigarette smoking frequencies among men. Therefore, compared to binary and ordinal logistic regressions, the multinomial logistic model was determined to be the best fitting model.
Variance inflation factor (VIF) analysis
Prior to moving on to the analysis phase, each dependent variable’s variance inflation factors and tolerances were evaluated (the specifics are covered in the methodology section). This study’s overall mean VIF was 1.09.
Variables of the study
Dependent variable: the outcome variable of this study was Frequency currently smokes tobacco among men the frequency of currently smoking was given as no smokes (recoded as “0”, every day (recode as “1”), and some days (recoded as “2”). Outcome ascertainments, and data management was done according to the Guide to DHS statistics [19]. After reviewer previous literatures on independent variables regarding smoking the following independent variables included age, age at first sex, number of sex partners, marital status, education, place of residence, wealth index, mass media exposure, currently working status, internet utilization, and sex of the household head were considered [11, 12, 14, 21, 22]. Based on the guide to DHS statistics missing data on whether each type of tobacco was smoked is assumed to indicate non-use of that specific type of tobacco. These missing data are excluded from the numerator but included in the denominator [19].
Results
Sociodemographic characteristics of the study participants
This survey comprised weighted samples from 87,022 men in 10 East African countries. In terms of age, approximately 36,841 (42.34%) of the study participants were just below 26 years old. Regarding place of residence and marital status, 62,462 (71.78%) and 35,615 (40.93%) lived in rural areas and were married, respectively. In terms of educational level, 38,679 (44.45%) of the participants had completed primary school. Media exposure (at least one media exposure among watching television, listening to radio, or reading newspapers or books) was reported by 55,517 (63.80%) of the survey participants. The majority of 73,960 (84.99%) households are headed by men. More than half (62,611) (71.95%) of them did not use the internet in the past 12 months. Slightly more than half (49,578; 56.97%) of the study participants have only one sex partner. About 45,115 (51.84%) of them had started their first sex exposure during their teenage years. Finally, about 39,945 (45.90%) of men came from rich households (Table 3).
Factors associated with smoking among East African men
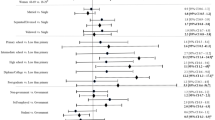
When all other variables were held constant, the variables age (26–35, 36–45, and > 45 years old) were associated with a 2.17, 2.82, and 3.68 times increase in the relative risk ratio (RRR = 2.17, 95% CI, 2.01,2.34), (RRR = 2.82, 95% CI, 2.60, 3.07), and (RRR = 3.68, 95% CI, 3.38, 4.02), respectively, of using a cigarette daily rather than no cigarette when compared to less than 26-year-old men, respectively. Similarly, as compared to men who had no sextual intercourse, those men who had begun their first sexual intercourse at the age of 7–19 years, 20–25 years, and greater than 25 years old have shown a higher relative risk ratio of (RRR = 6.27, 95% CI, 5.35–7.35), (RRR = 4.01, 95% CI, 3.40–4.72), and (RRR = 3.08, 95% CI, 2.55–3.71) more times to smoke cigarettes daily than those who did not smoke cigarettes, respectively. Furthermore, when all other variables were held constant, comparing with single men, those men who had married (RR = 0.86, 95% CI, 0.79, 0.93), and who had divorced or widowed (RR = 2.51, 95% CI, 2.27, 2.77), were times lower to smoke cigarettes daily than to not smoke cigarettes at all, respectively. Regarding wealth index, men with middle and rich households have shown a higher (RRR = 2.11, 95% CI: 1.98–2.24) and (RRR = 1.44, 95% CI: 1.34–1.54) relative risk ratio to smoke daily rather than not smoking cigarettes at all, respectively. However, men who had completed secondary or high education levels had shown a lower relative risk (RR = 0.72, 05% CI, 0.66–0.77) of smoking daily than uneducated men. Similarly, rural men revealed a lower risk ratio of being daily smokers as compared to urban men (RR = 0.69, 95% CI, 0.65–0.73). Conversely, when all other variables were held constant, employed men had shown a higher risk ratio (RR = 1.26, 95% CI, 1.17, 1.36) to utilize cigarettes daily rather than not smoking them at all. Likely, men who had mass media exposure about cigarette smoking had shown a lower relative risk ratio of being a daily smoker (RR = 0.76, 95% CI, 0.73–0.81) as compared to unexposed individuals. Men who have one and more than one sex partner had a higher tendency to smoke cigarettes daily rather than not be smokers at all, with a relative risk ratio of (RRR = 1.23, 95% CI: 1.13–1.5) and (RRR = 1.63, 95% CI: 1.47–1.79) more times as compared to those participants who had no sex partner, respectively (Table 4).
Discussion
Our results show that among the study’s male participants, the frequency of current daily tobacco use was 11.03 (95% CI = 10.82, 11.24) and the frequency of some days usage was 3.66 (95% CI = 3.54, 3.79). Overall, about 14.69% of people currently smoke cigarettes. Our analysis revealed that significant risk factors for cigarette smoking among men in East African countries included higher age, lower education, wealth index, marital status, early sexual activity, multiple sexual partners, media exposure, living in a rural area, and employment status.
When all other factors were held constant, the age ranges of 26 to 35, 36 to 45, and > 45 years old had strong statistical associations with the likelihood of smoking cigarettes daily as opposed to abstaining from smoking (RRR = 2.17, 95% CI, 2.01,2.34), 2.82 to 3.07, and 3.68 to 4.02 as compared to men under the age of 26. This result was consistent with several research conducted in various fields, as older men were found to smoke more frequently than younger males in Ghana [23], Ethiopia [15], five South Asian nations [24], and India [25]. This may have more to do with delaying the start of tobacco use than it does with preventing people from starting to smoke [26]. Why older men smoke more than younger men may also be influenced by social and demographic factors, as well as nicotine dependence. Another study discovered that men who fall into lower socioeconomic and demographic groups (older, uneducated, and poor) are more likely to smoke. Younger males (15–29 years old and 30–44 years old) are discovered to have a decreased risk of smoking compared to older men (45–59 years old). Furthermore, it has been noted that males in higher wealth groups are less likely to smoke than their counterparts in lower wealth categories [15, 23]. However, in terms of smoking patterns, the American Lung Association reports that among men aged 26 or older, heavy smoking rates (more than 24 cigarettes per day) declined by 20% from 1974 to 2018. This shows that the number of elderly men who smoke has been declining over time [27]. Therefore, more research is required to uncover the true causes of age-related triggers in men.
This study discovered that, when all other variables were held constant, comparing with single men, those men who had married (RRR = 0.86, 95% CI, 0.79,0.93), and who had divorced or widowed (RRR = 2.51, 95% CI, 2.27,2.77), times lower to smoke cigarette daily rather than not smoking cigarette at all respectively. Significant psychological suffering can ensue from a widowed, divorce or marital separation, which frequently leads to smoking as a coping mechanism [28, 29]. According to the centers for disease control and prevention (CDC), current cigarette smoking was highest among Americans who were divorced, separated from their partners, or widowed and lowest among those who were married or cohabitating [30].
Men who have one, and more than one sex partners had a higher tendency of smoking cigarette daily rather than to be not a smoker at all with a relative risk ratio of (RRR = 1.23,95% CI,1.13,1.35), and (RRR = 1.63, 95% CI, 1.47,1.79) more times as compared to those participants who had no sex any partner respectively. Men who had their first sextual encounters between the ages of 7 and 19 years, 20 and 25 years, and older than 25 years showed a higher relative risk ratio of (RRR = 6.27, 95% CI, 5.35,7.35), (RRR = 4.01, 95% CI, 3.40,4.72), and (RRR = 3.08, 95% CI, 2.55,3.71), respectively, for daily cigarette smoking rather than not smoking cigarettes as compared who had not sexual intercourse. There is not much data on the precise effect of having several sex partners on male cigarette smoking. However, some research has linked cigarette smoking to a variety of sexual behaviors. For instance, one study indicated that smoking was linked to more sexual partners among men [31]. In a different study, it was discovered that young males who smoke cigarettes and have sex with men report having more casual and transactional partners than non-smokers [32]. According to a third study, having female partners is one of the risk variables for current frequent smoking among Chinese males who engage in male sex [33].
Men in the highest wealth index group were more likely to smoke than men in the lowest wealth index category. This result contrasts with research conducted in Ethiopia [15], five South Asian nations [24], Hungary [34], Ghana [23]. In general, those from lower socioeconomic class have less educational degrees and are more likely to be dependent on alcohol and tobacco. They are also less knowledgeable about the risks associated with smoking [35]. Wealth does not always result in a decrease in cigarette use [36]. Regarding other non-communicable diseases risk variables, investigations conducted in Egypt have revealed a pattern that is similar. In two of these studies, it was found that education protected against obesity and diabetes whereas wealth was found to increase obesity due to higher consumption of high-energy foods [35,36,37,38]. As we’ve already mentioned, our research revealed that males with greater money are more likely to smoke cigarettes. The study’s foundation is multinomial regression, which was used to base it on the frequency of cigarette smoking. Because of this, even while poor men may have a higher likelihood of smoking, they often lack the funds to do so. Other research examined participants’ smoking status or history, which may have contributed to the conclusion that poor men are more likely to smoke than their counterparts. Further research should concentrate on the wealth index to obtain a comprehensive explanation of the link between cigarette smoking and India’s high wealth index.
Similar to earlier research [24, 39, 40], we discovered that males who were employed smoked more cigarettes than men who were not employed. Working people, especially men, may encounter work stress, which may in turn have a favorable effect on smoking. Similarly, individuals can easily become smokers if they had unhealthy interactions with their coworkers or had come across smokers. It is commonly known that men’s smoking intensity and job stress are correlated [15, 41].
In the pooled analysis, we discovered that education significantly influenced cigarette smoking in east Africa while controlling for other characteristics. When compared to males who are typically uneducated, our final model’s results showed that men with a secondary or higher degree of education were less likely to smoke cigarettes. For instance, better education served as a barrier to smoking in a study carried out in five South Asian nations [24], including Malaysia [22], Sri Lanka [39], and Ethiopia [15]. This can be explained by the fact that education helps people become more aware of the negative effects of smoking on their health. More educated persons might use the national stop line and other support programs for quitting smoking. Higher educated individuals in India attempted to quit smoking more than less educated individuals [42].
It was discovered that rural residence has a negative statistically significant impact on smoking. Compared to men from urban origins, men from rural areas were less likely to consume cigarettes every day. Urban residents may be exposed to smoking environments more frequently, which alters people’s smoking habits under these circumstances. The tobacco business may easily target urban residents since marketing is more readily available in metropolitan areas. Urban residents are more prone to smoke cigarettes, according to a European study [24, 43].
Likely, men who had mass media exposure about cigarette smoking had shown a lower relative risk ratio of to be daily smoker by (RRR = 0.76, 95% CI, 0.73,0.81) as compared to unexposed individuals. Men’s cigarette smoking can be significantly impacted by exposure to the media. Adult smoking behavior can be altered by mass media campaigns, according to studies [44, 45]. Strong anti-tobacco mass media efforts and visual health warnings can deter youngsters and other vulnerable populations from starting to smoke, as well as boost the number of current smokers who give up [46]. When campaigns are a component of broader tobacco control initiatives, their effects on smoking cessation are more significant [45]. Reach, intensity, duration, and message type are all factors that influence the outcome of mass media campaigns [45]. A body of research supporting the notion that entertainment media can affect young people’s smoking habit has been conducted to examine the relationship between smoking in entertainment media and youth smoking [47].
Strength and limitations of the study
The primary study strength is that it used a sizable sample size from nationally representative surveys with high response rates, excellent interviewer training, standardized data collection methods across countries, and consistent content across time which produced enough power to analyze the relationship between socio-demographic characteristics and cigarette smoking. The comparison of results across countries was made more powerful statistically by combining databases from ten different countries using pooled analysis. Furthermore, the accuracy and generalizability of the study are improved because the data were adequately sampled across the nation, with a high response rate. In addition, the study used a best fitted multinomial modeling technique to determine the frequencies of cigarette smoking. As a result, the current findings could be extrapolated to healthcare settings and socio-demographic features that are similar. However, this study’s disadvantage is that because the data were obtained from secondary sources and the surveys were cross-sectional, no conclusions about causality could be formed. Another cultural and perception-related variable across countries was not included in the study. Additionally, the self-reporting data was based on actual events, which could lead to recall bias. As a result of societal shame and people’s tendency to be conservative, the prevalence of cigarette smoking may be underreported.
Conclusions
According to our data, men in East African countries were much more likely to smoke cigarettes if they were older, had less education, had a higher wealth index, were divorced/widowed, engaged in many sexual relationships, had early sexual activity, lived in urban region, were employed, or had no media exposures. To decrease smoking initiation and increase smoking cessation among men, policymakers and public health practitioners should consider the factors identified. An improvement in smoking cessation support services can also be an effective intervention.
Targeted education and awareness campaigns, smoke-free policies in urban areas, workplace smoking cessation programs, media-based anti-smoking campaigns, and longitudinal monitoring and surveillance are among the top policy implications of this study. However, it is important to consider the cultural and socio-economic context of East African countries while implementing these policy implications. Tailoring interventions to specific populations and addressing social determinants influencing smoking behavior will increase the likelihood of success in reducing smoking rates among men in East Africa.
Data availability
All data concerning this study are accommodated and presented in this document. The detailed data set can be freely accessible from the www.dhsprogram.com website.
References
Organization WH, Tobacco. Key facts; https://www.who.int/news-room/fact-sheets/detail/tobacco. 2023.
Organization WH. WHO report on the global tobacco epidemic, 2017: monitoring tobacco use and prevention policies. World Health Organization; 2017.
Organization WH. World Health Organization (WHO) report on the global tobacco epidemic 2017-country profile Portugal. Volume 10. Geneva: World Health Organization; 2017. p. 9781410610348.
Zheng W, McLerran DF, Rolland BA, Fu Z, Boffetta P, He J, et al. Burden of total and cause-specific mortality related to tobacco smoking among adults aged ≥ 45 years in Asia: a pooled analysis of 21 cohorts. PLoS Med. 2014;11(4):e1001631.
Tyas SL, Pederson LL. Psychosocial factors related to adolescent smoking: a critical review of the literature. Tob Control. 1998;7(4):409–20.
Rudatsikira E, Muula AS, Siziya S. Prevalence, correlates of and perceptions toward cigarette smoking among adolescents in South Korea. Indian J Pediatr. 2009;76:505–10.
Organization WH. WHO report on the global tobacco epidemic 2015: raising taxes on tobacco. World Health Organization; 2015.
Rachiotis G, Barbouni A, Basagiannis A, Katsioulis A, Kostikas K, Mouchtouri V, et al. Prevalence and determinants of current cigarette smoking and secondhand smoking among Greek adolescents: the global youth tobacco survey (GYTS) 2013 study. BMJ open. 2020;10(2):e034760.
Csa I. Central statistical agency (CSA)[Ethiopia] and ICF. Ethiopia demographic and health survey, Addis Ababa, Ethiopia and Calverton, Maryland, USA. 2016;1.
Escario JJ, Wilkinson AV. Visibility of smoking among schoolteachers in Spain and associations with student smoking: a cross-sectional study. BMJ open. 2018;8(1):e018736.
Ibraimi Z, Shabani D, Murtezani A, Tahirbegolli B, Berisha-Muharremi V. Sociodemographic factors affecting tobacco, alcohol, and cannabis consumption among Kosovar University students. J Child Sci. 2023;13(01):e65–e74.
Bandason T, Rusakaniko S. Prevalence and associated factors of smoking among secondary school students in Harare Zimbabwe. Tob Induc Dis. 2010;8:1–9.
Ary DV, Biglan A. Longitudinal changes in adolescent cigarette smoking behavior: onset and cessation. J Behav Med. 1988;11(4):361–82.
Islam MS, Saif-Ur-Rahman K, Bulbul MMI, Singh D. Prevalence and factors associated with tobacco use among men in India: findings from a nationally representative data. Environ Health Prev Med. 2020;25:1–14.
Gutema BT, Chuka A, Ayele G, Estifaons W, Melketsedik ZA, Tariku EZ, et al. Tobacco use and associated factors among adults reside in Arba Minch health and demographic surveillance site, southern Ethiopia: a cross-sectional study. BMC Public Health. 2021;21(1):1–10.
Organization WH. NCD global monitoring framework. Geneva: World Health Organization; 2011. 2017.
FDRoEMo H. HSTP Health Sector Transformation Plan 2015/16–2019/20 (2008-2012 EFY). 2015.
Organization WH. WHO report on the global tobacco epidemic, 2008: the MPOWER package. World Health Organization; 2008.
Croft TN, Marshall AM, Allen CK, Arnold F, Assaf S, Balian S. Guide to DHS statistics. Rockville: ICF. 2018;645.
Elkasabi M. Sampling and Weighting with DHS Data: https://blog.dhsprogram.com/sampling-weighting-at-dhs/. 2015.
Rachiotis G, Barbouni A, Basagiannis A, Katsioulis A, Kostikas K, Mouchtouri V et al. Prevalence and determinants of current cigarette smoking and secondhand smoking among Greek adolescents: the global youth tobacco survey (GYTS) 2013 study. BMJ open. 2020;10(2).
Lim HK, Ghazali SM, Kee CC, Lim KK, Chan YY, Teh HC, et al. Epidemiology of smoking among Malaysian adult males: prevalence and associated factors. BMC Public Health. 2013;13:1–10.
Nketiah-Amponsah E, Afful-Mensah G, Ampaw S. Determinants of cigarette smoking and smoking intensity among adult males in Ghana. BMC Public Health. 2018;18(1):1–10.
Shariful Islam M, Rashid M, Sizear MI, Hassan R, Rahman M, Parvez SM, et al. Cigarette smoking and associated factors among men in five south Asian countries: a pooled analysis of nationally representative surveys. PLoS ONE. 2022;17(11):e0277758.
Manimunda SP, Benegal V, Sugunan AP, Jeemon P, Balakrishna N, Thennarusu K, et al. Tobacco use and nicotine dependency in a cross-sectional representative sample of 18,018 individuals in Andaman and Nicobar Islands, India. BMC Public Health. 2012;12:1–11.
Barrington-Trimis JL, Braymiller JL, Unger JB, McConnell R, Stokes A, Leventhal AM, et al. Trends in the age of cigarette smoking initiation among young adults in the US from 2002 to 2018. JAMA Netw open. 2020;3(10):e2019022–e.
Fiore MC, Novotny TE, Pierce JP, Hatziandreu EJ, Patel KM, Davis RM. Trends in cigarette smoking in the United States: the changing influence of gender and race. JAMA. 1989;261(1):49–55.
Heuveline P, Timberlake JM. The role of cohabitation in family formation: the United States in comparative perspective. J Marriage Family. 2004;66(5):1214–30.
Clancy N, Zwar N, Richmond R. Depression, smoking and smoking cessation: a qualitative study. Fam Pract. 2013;30(5):587–92.
CDC. Current cigarette smoking among adults in the United States. Centers for Disease Control and Prevention; 2020.
Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, Schootman M, Cottler LB, Bierut LJ. Number of sexual partners and associations with initiation and intensity of substance use. AIDS Behav. 2011;15:869–74.
Storholm ED, Halkitis PN, Siconolfi DE, Moeller RW. Cigarette smoking as part of a syndemic among young men who have sex with men ages 13–29 in New York City. J Urb Health. 2011;88:663–76.
Xu W, Tang W, Zhang J, Shi X, Zheng Y, Kaufman MR. Cigarette smoking and its associations with substance use and HIV-related sexual risks among Chinese men who have sex with men. Int J Environ Res Public Health. 2020;17(5):1653.
Pénzes M, Czeglédi E, Balázs P, Foley KL. Factors associated with tobacco smoking and the belief about weight control effect of smoking among Hungarian adolescents. Cent Eur J Public Health. 2012;20(1):11.
Sreeramareddy CT, Pradhan PMS, Mir IA, Sin S. Smoking and smokeless tobacco use in nine South and Southeast Asian countries: prevalence estimates and social determinants from demographic and health surveys. Popul Health Metrics. 2014;12:1–16.
Abdulrahim S, Jawad M. Socioeconomic differences in smoking in Jordan, Lebanon, Syria, and Palestine: a cross-sectional analysis of national surveys. PLoS ONE. 2018;13(1):e0189829.
Aitsi-Selmi A, Chandola T, Friel S, Nouraei R, Shipley MJ, Marmot MG. Interaction between education and household wealth on the risk of obesity in women in Egypt. PLoS ONE. 2012;7(6):e39507.
Mowafi M, Khadr Z, Subramanian S, Bennett G, Hill A, Kawachi I. Are neighborhood education levels associated with BMI among adults in Cairo. Egypt? Social Sci Med. 2011;72(8):1274–83.
Fernando HN, Wimaladasa ITP, Sathkoralage AN, Ariyadasa AN, Udeni C, Galgamuwa LS, et al. Socioeconomic factors associated with tobacco smoking among adult males in Sri Lanka. BMC Public Health. 2019;19(1):1–8.
Viana TBP, Camargo CLd, Gomes NP, Felzemburgh RDM, Mota RS, Lima CCOJ. Factors associated with cigarette smoking among public school adolescents. Volume 52. Revista da Escola de Enfermagem da USP; 2018.
Green KL, Johnson JV. The effects of psychosocial work organization on patterns of cigarette smoking among male chemical plant employees. Am J Public Health. 1990;80(11):1368–71.
Sheet IF, Davanagere K. National family health survey (NFHS)-4. Ministry of Health and Family Welfare Government of India[Online]. 2015;2016.
Idris BI, Giskes K, Borrell C, Benach J, Costa G, Federico B, et al. Higher smoking prevalence in urban compared to non-urban areas: time trends in six European countries. Health Place. 2007;13(3):702–12.
Bala MM, Strzeszynski L, Topor-Madry R. Mass media interventions for smoking cessation in adults. Cochrane Database Syst Reviews. 2017;(11).
Durkin S, Brennan E, Wakefield M. Mass media campaigns to promote smoking cessation among adults: an integrative review. Tob Control. 2012;21(2):127–38.
Friend K, Levy DT. Reductions in smoking prevalence and cigarette consumption associated with mass-media campaigns. Health Educ Res. 2002;17(1):85–98.
Sargent JD, Gibson J, Heatherton TF. Comparing the effects of entertainment media and tobacco marketing on youth smoking. Tob Control. 2009;18(1):47–53.
Acknowledgements
We would like to acknowledge the DHS program for providing permission for this study following research ethics.
Funding
This study was not supported financially by anyone.
Author information
Authors and Affiliations
Contributions
BT was involved in conceptualization, design, data extraction, statistical analysis, language editing, data interpretation, data curation, article review, validation, and original manuscript writing. MMJ, and NTA reviewed the study’s design and the draft manuscript, checked the analysis, and made a significant contribution. BC, and DAG critical revision for intellectual substance, and article review. The authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethical considerations and data set access
The study was conducted after obtaining a permission letter from www.dhsprogram.com on an online request to access east African DHS data after reviewing the submitted brief descriptions of the survey to the DHS program, and no need of ethical letter approval. The datasets were treated with the utmost confidence. This study was done based on secondary data from east Africa DHS. Issues related to informed consent, confidentiality, anonymity, and privacy of the study participants are already done ethically by the DHS office. We did not manipulate and apply the microdata other than in this study. There was no patient or public involvement in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Terefe, B., Jembere, M.M., Chekole, B. et al. Frequency of cigarette smoking and its associated factors among men in East Africa: a pooled prevalence analysis of national survey using multinomial regression. BMC Public Health 24, 668 (2024). https://doi.org/10.1186/s12889-024-18188-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-18188-4