
Abstract
Background
Low hand grip strength (HGS) is associated with the risk of cardiovascular diseases, but the association between HGS and myocardial infarction/angina pectoris (MIAP) is unclear. Furthermore, there have been no studies examining the associations of MIAP with anthropometric indices, absolute HGS indices, and relative HGS indices calculated by dividing absolute HGS values by body mass index (BMI), waist circumference (WC), waist-to-height ratio (WHtR), or weight values. Therefore, the objective of this study was to examine the associations of MIAP with absolute and relative HGS combined with several anthropometric indices.
Methods
In this large-scale cross-sectional study, a total of 12,963 subjects from the National Health and Nutrition Examination Survey were included. Odds ratios and 95% confidence intervals for the associations of MIAP with anthropometric indices, absolute HGS indices, and relative HGS indices were computed from binary logistic regression models. We built 3 models: a crude model, a model that was adjusted for age (Model 1), and a model that was adjusted for other relevant covariates (Model 2).
Results
For men, the average age was 61.55 ± 0.16 years in the MIAP group and 66.49 ± 0.61 years in the non-MIAP group. For women, the average age was 61.99 ± 0.14 years in the MIAP group and 70.48 ± 0.61 years in the non-MIAP group. For both sexes, the MIAP group had lower diastolic blood pressure, shorter stature, greater WC, and a greater WHtR than did the non-MIAP group, and women tended to have greater systolic blood pressure, weight, and BMI than in men. HGS was strongly associated with the risk of MIAP in the Korean population. In men, relative HGS indices combined with WC and the WHtR had greater associations with MIAP than did the anthropometric indices and absolute HGS indices. However, in women, anthropometric indices, including weight, BMI, WC, and WHtR, were more strongly associated with MIAP than were absolute and relative HGS indices, unlike in men. When comparing absolute and relative HGS indices in women, relative HGS indices combined with BMI and weight was more strongly related to MIAP than was absolute HGS indices.
Conclusions
MIAP might be better identified by relative HGS than absolute HGS in both sexes. The overall magnitudes of the associations of MIAP with absolute and relative HGS are greater in men than in women.
Similar content being viewed by others
Introduction
Myocardial infarction (MI) is an important cause of mortality and disability worldwide [1,2,3]. MI is defined as myocardial cell necrosis, vascular occlusion, or thrombosis according to the status of long-term ischemia and the complexities of the cellular functions of inflammation and scar formation [1,2,3]. MI is the first manifestation of coronary artery disease (CAD) and is one of several critical manifestations (angina pectoris, heart failure, and unexpected death) of coronary heart disease [2, 3]. Customarily, the concept of acute coronary syndrome (ACS) includes patients with unstable angina pectoris, ST-segment elevation MI, or non-ST-elevation MI according to clinical criteria [2, 3].
Recently, low hand grip strength (HGS) was strongly associated with the risk of several diseases, such as MI/angina pectoris (MIAP) [4,5,6,7,8,9,10,11,12,13,14,15], stroke [5,6,7, 9], heart disease [12], nonalcoholic fatty liver disease [16], myocardial ischemia [17], diabetes [13, 18, 19], metabolic syndrome [20], depression [21, 22] and pulmonary dysfunction [23], cardiovascular mortality and noncardiovascular mortality [4,5,6,7, 9, 10], cardiovascular health biomarkers [14, 15], and quality of life [24]. However, the associations between HGS and MIAP or cardiovascular risks are unclear. Many studies have reported that low absolute HGS is a strong predictor of MIAP in many countries [4,5,6,7,8,9,10,11,12], whereas some studies have argued that HGS is not associated with cardiovascular risk factors or cardiovascular mortality [25,26,27]. On the other hand, more recently, several studies examined the association between relative HGS (HGS divided by weight, height, or body fat mass) and several diseases, such as cancer [28], type 2 diabetes [13], cardiometabolic disease [14, 15], and metabolic syndrome [20]. Although many studies have examined the association between the absolute HGS index and MIAP, to our knowledge, there have been no studies examining the association between MIAP and both absolute and relative HGS indices. Therefore, the objectives of this study were to examine the associations of MIAP with anthropometric indices, absolute HGS indices, and relative HGS indices combined with several anthropometric indices and to identify the indices most strongly associated with this disease.
The originality and significance of this study are that it is the first to compare the association between MIAP and absolute and relative HGS combined with various anthropometric indices and to demonstrate that relative HGS is more strongly associated with MIAP than is absolute HGS in both men and women in a large-scale Korean population.
Methods
Study design and population
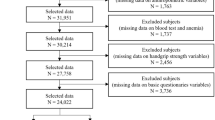
In this large-scale cross-sectional study, we utilized the Korea National Health and Nutrition Examination Survey (KNHANES) dataset provided by the Korea Disease Control and Prevention Agency (KDCA). The KNHANES is a nationwide health and nutrition survey conducted annually to produce statistics with national representativeness and reliability on the health status, health behavior, and food and nutritional intake of the population. The survey collects data through health interview surveys, health examination surveys, and nutrition surveys [29,30,31]. In this study, we used recent HGS and MIAP data from 2014 to 2019. The data from 2020 were not included in this study, as the measurement of HGS was suspended due to the spread of COVID-19. From 2014 to 2019, a total of 47,309 participants (men = 21,566, women = 25,743) participated in the health interview survey and examination conducted by mobile examination vehicles. The target participants of this study were adults aged 50 years or older in South Korea. Initially, participants were selected based on age, and participants with missing data on anthropometric variables, basic questionnaire variables, and HGS variables were excluded. Further details regarding the participant selection process are visually presented in Fig. 1. Ultimately, a total of 12,963 participants who were not missing data for the study variables were included.

Sample selection procedure used in this study
Ethics approval
The KNHANES was approved by the Research Ethics Committee of the KDCA (IRB: 2013-07CON-03–4 C, 2013-12EXP-03–5 C, 2018-01-03-P-A, 2018-01-03-C-A). This study, which was based on the KNHANES dataset, was also ethically approved by the Institutional Review Board of the Korea Institute of Oriental Medicine (IRB No. I-2209/009 − 001). This study was conducted in accordance with the Helsinki Declaration, and all methods followed relevant guidelines and regulations [29,30,31].
Definitions of MIAP
The primary outcome of this study was MIAP. We defined MIAP patients as a single MIAP group according to previous methods in various cross-sectional and follow-up studies [32,33,34,35,36]. The presence of MIAP was determined by two questions included in the health interview survey: “Have you been diagnosed with MI by a doctor?” and “Have you been diagnosed with angina by a doctor?“. Participants who answered “yes” to either question were included in the MIAP group, and those who answered “no” to both questions were included in the non-MIAP group. To overcome respondent recall bias in the diagnosis of MIAP, the health interview survey was carried out through a face-to-face interview with experts and well-trained staff according to the established guidelines [29,30,31]. The status of other diseases, such as hypertension, diabetes, hypercholesterolemia, and hypertriglyceridemia, was determined using blood tests and health interview survey data according to the KDCA guidelines [31]. Hypertension was defined as a systolic blood pressure (SBP) of 140 mmHg or higher, a diastolic blood pressure (DBP) of 90 mmHg or higher, or the current use of antihypertensive medication [37, 38]. Diabetes status was defined as a fasting plasma glucose level of 126 mg/dl or higher, a glycated hemoglobin level of 6.5% or higher, the current use of antidiabetic medication, the use of insulin injection therapy, or a diagnosis of diabetes by a doctor [38, 39]. Hypercholesterolemia was defined as a fasting total cholesterol level of 240 mg/dl or higher or the current use of cholesterol-lowering medication [40, 41]. Hypertriglyceridemia was defined as a fasting triglyceride level of 200 mg/dl or higher [41, 42].
Covariates
We included demographic and health behavior-related variables such as residential area, education level, occupation type, household income, stress, alcohol consumption, smoking status, family history of ischemic heart disease (IHD), resistance exercise, and walking exercise as covariates. The demographic data were collected through an interview method, while the health behavior-related data were collected through a self-administered questionnaire. Residential areas were classified into two categories based on the subjects’ current residential location: urban and rural. Education level was categorized into four categories, ranging from an elementary school or lower, middle school, high school, and university or higher. Occupation type was divided into seven categories, ranging from unemployed to white-collar workers, office workers, service workers, farmers or fishers, blue-collar workers, elementary occupations, and unemployed. Household income was divided into four levels as equivalent income quartiles based on average monthly income, and stress was classified into four groups (extremely, very, slightly, and rarely) according to the degree of perceived stress. Alcohol consumption was categorized into seven levels (never drinker, former drinker 1 year prior, < 1 drink per month, 1 drink per month, 2∼4 drinks per month, 2∼3 drinks per week, and > = 4 drinks per week) based on the frequency of alcohol consumption in the past year, and smoking status was classified into three groups (current smoker, former smoker, and never smoker) according to current and past smoking status [29,30,31]. Information on family history of IHD was obtained through the question “Have your father, mother, or siblings ever been diagnosed with ischemic heart disease by a doctor?” Resistance exercise was classified into four categories (never, 1∼2 days per week, 3∼4 days per week, and > = 5 days per week) based on the question “How many days did you perform strength training, such as push-ups, sit-ups, dumbbell training, kettlebell training, or barbell training, in the past week?“, and walking exercise was expressed in minutes per week.
Measurement
In this study, we analyzed the associations between MIAP and variables related to HGS and anthropometric indices. HGS and anthropometric data were collected by trained examiners who received specific education and training in strict standardization and quality control measures. HGS was measured after excluding subjects who had a history of hand/wrist surgery or who had experienced functional limitations or discomfort in the last three months, which could make it difficult to measure HGS. A digital HGS dynamometer (T.K. K 5401, Japan) was used to measure HGS; the subjects stood upright, their feet were shoulder-width apart, and they faced forward, with their shoulders naturally lowered so that their elbows and wrists did not touch their torso or bend. The measurement began with the dominant hand, taking a 1-minute break between hands and repeating the measurement three times per hand. Absolute HGS was measured as the maximum HGS of the dominant hand (MaxGS-DH), the maximum HGS of the nondominant hand (MaxGS-nonDH), the maximum HGS of both hands (MaxGS-BHs) and the average HGS of both hands (meanGS-BHs). Relative HGS was calculated by dividing the absolute HGS values by body mass index (BMI), waist circumference (WC), waist-to-height ratio (WHtR), and weight values [43, 44]. For the anthropometric variables, height and weight were measured using an automatic measuring device (JENIX DS-102, Dong Sahn Jenix Co., Seoul, Korea) in units of 0.1 cm and 0.1 kg, respectively. BMI was computed by dividing weight (kg) by height squared (m2). WC was measured using a tape measure (Seca 200, Hamburg, Germany) in units of 0.1 cm, and the WHtR was obtained by dividing WC by height. SBP and DBP were measured thrice using a standard mercury sphygmomanometer (Baumanometer Wall Unit 33(0850)/USA) and then averaged using the second and third measurements.
Statistical analysis
To obtain a representative sample of the entire South Korean population, the KNHANES utilized data from the Population and Housing Census and Joint Housing Price Disclosure as the basis for sample extraction. By applying a two-stage stratified cluster sampling method with survey districts and households as the first and second-stage sampling units, respectively, a representative sample was selected for the KNHANES. Additionally, through household verification surveys, the status of all residences and households in the selected areas was assessed, and households were chosen to participate in health surveys, examinations, and nutritional assessments. In the KNHANES, weights are calculated and provided using information collected from household verification surveys. The basic weights consist of health survey and examination weights, as well as nutritional survey weights. Within the basic weights, separate weights are provided based on the age of the target survey participants, differences in the survey participants, and differences in the survey period. Moreover, considering the simultaneous analysis of multiple variables, the KNHANES also provides association analysis weights that encompass various survey sections, domains, and items. Detailed explanations related to the weights can be found in [31]. In this study, we followed the KDCA guidelines [29,30,31] and applied health survey and examination weights to conduct complex sample analyses.
All analyses were performed using IBM SPSS Statistics 21 and considering a statistical significance level of 0.05. The characteristics of the subjects were described by dividing men and women into groups with and without MIAP. Categorical variables are expressed as percentages and standard errors, while continuous variables are expressed as the means and standard errors. Sex differences in the analyzed variables were examined using t tests based on general linear models for continuous variables and Rao–Scott chi-square tests for categorical variables.
Results
Participant demographic characteristics
The characteristics of the study participants are shown in Table 1. The associations of MIAP with anthropometric indices, absolute HGS indices, and relative HGS indices were analyzed by calculating odds ratios (ORs) and 95% confidence intervals (CIs) through a binary logistic regression model after data standardization. The final sample consisted of 12,963 South Korean adults older than 50 years, including 5,584 (43.08%) men and 7,379 (56.92%) women. The prevalence of MIAP among South Korean adults over 50 years of age was 4.23%, with a higher incidence in men (6.14%) than in women (2.78%). All variables used in the analysis, except for IHD family history, SBP, and BMI, exhibited statistically significant differences between men and women. For the demographic variables, including age, residential area, marital status, education level, occupation type, and household income, significant differences were observed between the non-MIAP group and the MIAP group in all variables, except for residential area and marital status in men and residential area in women. The MIAP group tended to be older, have a lower education level, have a higher unemployment rate, and have a lower household income than the non-MIAP group for both sexes. Among the variables related to health behaviors, resistance exercise significantly differed between the MIAP and non-MIAP groups for men (p = 0.004) but not for women (p = 0.582). The MIAP group tended to perform less resistance exercise than the non-MIAP group. There were significant differences in stress (p = 0.044) and alcohol consumption (p = 0.001) between the two groups for women but not for men. The MIAP group tended to experience more stress (i.e., “very” and “rarely”) and have lower alcohol consumption than did the non-MIAP group. For both men and women, there were significant differences between the MIAP and non-MIAP groups in terms of disease-related variables such as IHD family history, hypertension, diabetes, and hypercholesterolemia, but not hypertriglyceridemia. A greater proportion of the MIAP group had an IHD family history and hypertension, diabetes, or hypercholesterolemia than did the non-MIAP group.
For anthropometric indices and blood pressure, significant differences in DBP (p < 0.001), height (p = 0.012), WC (p = 0.001), and the WHtR (p < 0.001) were found between the MIAP and non-MIAP groups for men, and all variables showed statistically significant between-group differences in women. Overall, the MIAP group had a lower DBP, shorter stature, greater WC, and greater WHtR than did the non-MIAP group for both men and women, and women tended to have higher SBP, weight, and BMI. Regarding HGS-related variables, significant differences were observed between the two groups in all HGS-related variables, excluding the dominant hand variable, for both men and women. The HGS of the MIAP group tended to be lower than that of the non-MIAP group, with greater differences observed in men than in women.
Associations of MIAP with anthropometric indices and HGS
We created three models based on adjusted variables: the crude model was not adjusted; Model 1 was adjusted for age; and Model 2 was adjusted for age, residential area, education level, occupation type, household income, stress, alcohol consumption, smoking status, family history of IHD, resistance exercise, and walking exercise. Tables 2 and 3 show the associations of MIAP with anthropometric indices, absolute HGS indices, and relative HGS indices. In men, although most absolute and relative HGS indices were strongly associated with MAIP, relative HGS indices combined with WC and the WHtR had a greater association with MIAP than did anthropometric indices and absolute HGS indices in all crude analyses and in adjusted Models 1 and 2. MIAP showed a stronger negative association with MaxGS-nonDH/WC (adjusted odds ratio (adj. OR) = 0.68 [0.58–0.80], p = < 0.001), MaxGS-BHs/WC (adj. OR = 0.69 [0.58–0.81], p = < 0.001), MaxGS-nonDH/WHtR (adj. OR = 0.69 [0.58–0.82], p = < 0.001), and MaxGS-BHs/WHtR (adj. OR = 0.69 [0.58–0.83], p = < 0.001) compared to the other variables in Model 2. However, in women, anthropometric indices were more strongly associated with MIAP than were absolute and relative HGS indices. MIAP was more positively associated with weight (adj. OR = 1.41 [1.24–1.60], p = < 0.001), BMI (adj. OR = 1.44 [1.26–1.64], p = < 0.001), WC (adj. OR = 1.42 [1.23–1.63], p = < 0.001), and the WHtR (adj. OR = 1.42 [1.22–1.65], p = < 0.001) in adjusted Model 2. According to the comparisons between absolute and relative HGS indices, all absolute HGS indices and other relative HGS indices were strongly associated with MIAP, but all associations disappeared in adjusted models 1 and 2, except for 4 relative HGS combined with weight and BMI indices. Specifically, MIAP showed a negative association with MaxGS-DH/BMI (adj. OR = 0.82 [0.67-1.00], p = 0.047), MaxGS-DH/Weight (adj. OR = 0.81 [0.68–0.96], p = 0.017), MaxGS-BHs/Weight (adj. OR = 0.82 [0.69–0.97], p = 0.021), and MeanGS-BHs/Weight (adj. OR = 0.84 [0.71-1.00], p = 0.048) in adjusted Model 2. In both men and women, relative HGS was more strongly and more significantly associated with MIAP than was absolute HGS, even though anthropometric indices were more strongly associated with MIAP than were HGS indices in women.
Discussion
In this large-scale cross-sectional study, we examined the associations of MIAP with anthropometric indices, absolute HGS indices, and relative HGS indices. We found that HGS was strongly associated with the risk of MIAP in the Korean population. MIAP might be better identified by relative HGS than absolute HGS in both sexes, but anthropometric indices were more strongly associated with MIAP than HGS indices in women. The overall magnitudes of the associations of MIAP with absolute and relative HGS are greater in men than in women.
Generally, the risk factors for MIAP include increasing age [45]; sex and ethnicity [46]; a history of cardiovascular diseases (CVDs) [45,46,47]; hypertension [9, 45,46,47]; diabetes [9, 45,46,47]; dyslipidemia [46]; abnormal serum lipid levels such as proinsulin, C-reactive protein (CRP), uric acid, high-density lipoprotein cholesterol (HDL) cholesterol, and non-HDL cholesterol levels [9, 32, 47,48,49,50]; genetics [46]; smoking [9, 46,47,48, 51]; obesity [9, 46, 47, 51]; alcohol consumption [9, 47, 51, 52]; high DBP [48]; low physical activity or heavy exercise [9, 46, 47]; oxidative stress [51]; low education level [9]; psychosocial factors [47]; and low HGS [4,5,6,7, 9, 10]. However, these risk factors may differ according to sex, ethnic group or country. For example, low alcohol consumption is related to a low or moderate reduction in MI risk, but the protective effect of low alcohol consumption is greater in women than in men [52]. Additionally, a protective effect has been observed in many countries but not in South Asian countries such as India, Pakistan, Nepal, or Bangladesh [52]. Furthermore, the mean age of onset of MI was approximately 9 years later in men than in women in many ethnic groups and countries [47].
To date, an association between HGS and MIAP has been reported in various ethnic groups and countries. Leong et al. [4] examined the association of HGS with MI risk, stroke risk, and cardiovascular mortality risk in 139,691 subjects across 17 high-income and low-income countries. They reported that HGS was inversely associated with MI and stroke risk after adjustment for various potential confounders and argued that HGS was a predictor of death in patients with cardiovascular or noncardiovascular disease. Chainani et al. [6] assessed the association of cardiovascular mortality with HGS and gait speed via a systematic review and argued that low HGS and gait speed were linked to a high risk of cardiovascular mortality across diverse populations. Additionally, Lopez-Jaramillo et al. [7] investigated the relationship between HGS and CVDs such as MI, stroke, or death in patients with prediabetes and diabetes and documented that higher HGS was related to a lower incidence of death and cardiovascular events in both men and women, irrespective of adiposity and whether they resided in a high- or low-income country. Park et al. [8] examined the causal effect of HGS and walking pace on MI and CVD risk based on observational investigations and genetic instruments and reported that observational and genetically predicted low HGS and slow walking pace predicted the risk of MI or cardiovascular mortality. Yusuf et al. [9] tested the association of HGS with MI, stroke, and CVD risk based on data from the Prospective Urban Rural Epidemiology (PURE) study and reported that low HGS was a risk factor for MI, CVD, and stroke. Xu and Hao examined the causal effect of HGS on MI and CAD risk using single nucleotide polymorphisms (rs3121278 and rs752045) as genetic instruments for HGS in a Mendelian randomization study [10]. They argued that an increase of 1 kg in genetically determined HGS decreased the odds of MI by 7%. In the Korean population, several studies have examined the association of CVDs with absolute and relative HGS [11, 12]. Jang et al. [12] evaluated the association of heart disease (MIAP and congestive heart failure) with absolute and relative HGS through a longitudinal study. After adjustment for various confounders, they argued that relative HGS (HGS/BMI) was more strongly associated with heart disease than were absolute and dominant HGS in both men and women. Kim et al. [11] examined the association between relative HGS and cardiometabolic risk factors such as MIAP, hypertension, type 2 diabetes, osteoporosis, and obesity. They documented that MIAP was associated with relative HGS in a crude analysis but not in an adjusted analysis. These studies only used HGS/BMI as a relative HGS index [11, 12]; therefore, the results of these studies were limited by comparing only absolute HGS and one relative HGS index (HGS/BMI). A comparison of our findings with the results of previous studies showed that our findings were consistent with the results of previous studies [4, 6, 7, 9, 11, 12], indicating that low HGS was significantly related to the risk of MIAP or CVDs. Additionally, we agreed that relative HGS was superior to absolute or dominant HGS, as shown in the results of a previous study [12]. However, our findings differed from the results of other previous studies [11]. The results of our study showed that relative HGS indices combined with BMI and weight were significantly associated with MIAP in both men and women according to both the crude and adjusted models. We assume that the reasons for this discrepancy are the differences in the use of relative HGS indices, target diseases, or adjustment for covariates.
More recently, several studies have emphasized the usefulness of relative HGS indices combined with BMI, WC, weight, height, and fat mass in the identification of several diseases [13,14,15, 20]. Kis et al. [13] evaluated the predictive power of relative HGS indices for identifying older patients with type 2 diabetes and reported that the HGS/WC index was the best predictor of type 2 diabetes in older patients. Lee et al. [14] examined the association of cardiometabolic risk factors with relative HGS in Taiwanese men and women and argued that the HGS/BMI was a better indicator of cardiometabolic health than was absolute HGS. Similarly, Lawman et al. [15] tested the association between HGS and cardiovascular health biomarkers in U.S. adults and documented that the HGS/BMI was more strongly associated with cardiovascular biomarkers than was absolute HGS. Byeon et al. [20] examined the relationship of metabolic syndrome with absolute HGS and relative HGS in Korean adults and demonstrated that the HGS/weight index was more strongly associated with the incidence of metabolic syndrome than was absolute HGS. Although several studies have reported an association between the relative HGS index and the risk of several diseases, no studies have reported an association between relative HGS and MIAP.
The pathological mechanism by which low HGS is associated with an increased risk of MIAP, CVD, and mortality is unclear [4, 12], even though HGS is useful as a simple and inexpensive indicator of many diseases. However, possible explanations or mechanisms for the association can be suggested. First, our results revealed sex-specific differences in that the association between MIAP and HGS persisted in all the adjusted models for men, but for women, the association disappeared in the age-adjusted model. There are sex-specific differences in HGS according to age, hormonal changes, blood profile, and disease, such as arthritis and stroke [11, 44, 53]. A reduction in HGS was associated with aging and hormonal imbalances in women [44, 53]. Additionally, the sex-specific factors associated with HGS were diabetes, stroke, or osteoporosis in men and osteoarthritis in women [54]. HGS was associated with triglyceride and high-density lipoprotein levels in men and fasting plasma glucose levels in women [55]. In Korea, the prevalence of arthritis was much greater in women than in men [44]. In contrast, MIAP was more prevalent in men than in women [11]. Additionally, muscle strength and hormonal changes during aging differ according to sex [11]. The frequency of muscular and resistance exercise was much greater in men than in women in this study. We assumed that these conditions may induce sex differences in the association between HGS and MIAP. However, the cause of these sex differences is still unclear, and further studies are needed. Second, relative HGS was negatively associated with insulin resistance in both sexes [11]. Insulin resistance was linked to independent cardiovascular risk factors, including MIAP, due to its association with inflammation, such as glycometabolic abnormalities, high-sensitivity C-reactive protein (hs-CRP) levels, and fibrinogen levels [50, 56, 57]. For example, Hs-CRP, an inflammatory index, has a negative effect on relative HGS [11]. The biological mechanism underlying the relationship between chronic inflammation and low physical function was explained by the fact that inflammatory markers such as high CRP and interleukin-6 levels are inversely and independently related to poor physical performance and HGS [57]. Inflammation is the body’s defense response against disorders of homeostasis due to a local release of cytokines [57]. Cytokines are related to physiological functions such as muscle tissue turnover and immunoregulation, and their circulating levels are associated with CVD [57, 58]. Additionally, obesity and visceral adiposity are causally associated with insulin resistance [11, 59] and were suggested to be risk factors for MIAP in previous studies [9, 46, 47, 51]. Like these studies, the present study demonstrated that obesity indices such as weight, BMI, WC, and the WHtR were strongly associated with MIAP in both men and women according to the adjusted models. Sarcopenia and sarcopenic obesity are associated with a high risk of cardiometabolic and musculoskeletal diseases and reduced muscle mass and strength [11, 60, 61]. Furthermore, HGS is closely related to DBP, total cholesterol, LDL-cholesterol, and triglyceride levels [11, 61], and these markers are known to be risk factors for MIAP [9, 32, 45,46,47,48,49,50].
Our study has several limitations. We cannot establish a cause‒effect relationship due to the cross-sectional design. Additionally, data on the diagnosis of MIAP were obtained via questionnaires. Therefore, to overcome respondent recall bias in the diagnosis of MIAP, a health interview survey was performed through a face-to-face interview with experts and well-trained staff according to specific guidelines [29,30,31]. Despite these limitations, the statistical results of this study are strong and powerful because the very large KNHANES dataset includes a nationally representative sample of the Korean population. To our knowledge, this is the first study to compare anthropometric indices, absolute HGS indices, and relative HGS indices and their associations with MIAP risk in a large population-based investigation.
In conclusion, we examined the associations of MIAP with anthropometric indices, absolute HGS indices, and relative HGS indices. In men, the relative HGS indices combined with WC and the WHtR had greater associations with MIAP than did the anthropometric and absolute HGS indices. However, anthropometric indices were more strongly associated with MIAP than were absolute and relative HGS indices in women. When comparing absolute and relative HGS indices in women, except for anthropometric indices, relative HGS indices combined with BMI and body weight were more strongly related to MIAP than were absolute HGS indices.
Data availability
Data used in this study are available from the Korea National Health and Nutrition Examination Survey (KNHANES) performed by the Korea Centers for Disease Control and Prevention (KCDC). Anyone can freely access the data (https://knhanes.kdca.go.kr/knhanes/sub03/sub03_02_05.do).
Abbreviations
- HGS:
-
hand grip strength
- MaxGS-DH:
-
maximum grip strength of the dominant hand
- MaxGS-nonDH:
-
maximum grip strength of the nondominant hand
- MaxGS-BHs:
-
maximum grip strength of both hands
- MeanGS-BHs:
-
mean grip strength of both hands
- BMI:
-
body mass index
- WC:
-
waist circumference
- WHtR:
-
waist-to-height ratio
- MIAP:
-
myocardial infarction/angina pectoris
- MI:
-
myocardial infarction
- IHD:
-
ischemic heart disease
- SBP:
-
systolic blood pressure
- DBP:
-
diastolic blood pressure
- ACS:
-
acute coronary syndrome
References
Yap J, Irei J, Lozano-Gerona J, Vanapruks S, Bishop T, Boisvert WA. Macrophages in cardiac remodelling after myocardial infarction. Nat Rev Cardiol. 2023;20:373–85.
Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138:e618–51.
Mendis S, Thygesen K, Kuulasmaa K, Giampaoli S, Mähönen M, Blackett KN, et al. World health organization definition of myocardial infarction: 2008-09 revision. Int J Epidemiol. 2011;40:139–46.
Leong DP, Teo KK, Rangarajan S, Lopez-Jaramillo P, Avezum A Jr, Orlandini A, et al. Prognostic value of grip strength: findings from the prospective urban rural epidemiology (PURE) study. Lancet. 2015;386:266–73.
Taylor J. Hand grip strength predicts myocardial infarction and stroke. Eur Heart J. 2015;36:1845.
Chainani V, Shaharyar S, Dave K, Choksi V, Ravindranathan S, Hanno R, et al. Objective measures of the frailty syndrome (hand grip strength and gait speed) and cardiovascular mortality: a systematic review. Int J Cardiol. 2016;215:487–93.
Lopez-Jaramillo P, Cohen DD, Gómez-Arbeláez D, Bosch J, Dyal L, Yusuf S, et al. Association of handgrip strength to cardiovascular mortality in pre-diabetic and diabetic patients: a subanalysis of the ORIGIN trial. Int J Cardiol. 2014;174:458–61.
Park S, Lee S, Kim Y, Lee Y, Kang MW, Kim K, et al. Relation of poor handgrip strength or slow walking pace to risk of myocardial infarction and fatality. Am J Cardiol. 2022;162:58–65.
Yusuf S, Joseph P, Rangarajan S, Islam S, Mente A, Hystad P, et al. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): a prospective cohort study. Lancet. 2020;395:795–808.
Xu L, Hao YT. Effect of handgrip on coronary artery disease and myocardial infarction: a mendelian randomization study. Sci Rep. 2017;7:954.
Kim YM, Kim S, Bae J, Kim SH, Won YJ. Association between relative hand-grip strength and chronic cardiometabolic and musculoskeletal diseases in koreans: a cross-sectional study. Arch Gerontol Geriatr. 2021;92:104181.
Jang SK, Kim JH, Lee Y. Effect of relative handgrip strength on cardiovascular disease among Korean adults aged 45 years and older: results from the Korean longitudinal study of aging (2006–2016). Arch Gerontol Geriatr. 2020;86:103937.
Kis OS, Buch A, Eldor R, Moran DS. Hand grip strength relative to waist circumference as a means to identify men and women possessing intact mobility in a cohort of older adults with type 2 diabetes. Biomedicines. 2023;11:352.
Lee WJ, Peng LN, Chiou ST, Chen LK. Relative handgrip strength is a simple indicator of cardiometabolic risk among middle-aged and older people: a nationwide population-based study in Taiwan. PLoS ONE. 2016;11:e0160876.
Lawman HG, Troiano RP, Perna FM, Wang CY, Fryar CD, Ogden CL. Associations of relative handgrip strength and cardiovascular disease biomarkers in U.S. adults, 2011–2012. Am J Prev Med. 2016;50:677–83.
Lee I, Cho J, Park J, Kang H. Association of hand-grip strength and non-alcoholic fatty liver disease index in older adults. J Exerc Nutr Biochem. 2018;22:62–8.
Aono J, Higashi H, Higaki J, Ikeda S. The usefulness of the hand grip-exercise test in the diagnosis of myocardial ischaemia in patients with coronary-subclavian artery steal syndrome. Eur Heart J. 2017;38:1691.
Lee MJ, Khang AR, Yi D, Kang YH. Low relative hand grip strength is associated with a higher risk for diabetes and impaired fasting glucose among the Korean population. PLoS ONE. 2022;17:e0275746.
Hamasaki H. What can hand grip strength tell us about type 2 diabetes? Mortality, morbidities and risk of diabetes. Expert Rev Endocrinol Metab. 2021;16:237–50.
Byeon JY, Lee MK, Yu MS, Kang MJ, Lee DH, Kim KC, et al. Lower relative handgrip strength is significantly associated with a higher prevalence of the metabolic syndrome in adults. Metab Syndr Relat Disord. 2019;17:280–8.
Marques A, Matos MG, Henriques-Neto D, Peralta M, Gouveia ÉR, Tesler R, et al. Grip strength and depression symptoms among middle-age and older adults. Mayo Clin Proc. 2020;95:2134–43.
Smith L, White S, Stubbs B, Hu L, Veronese N, Vancampfort D, et al. Depressive symptoms, handgrip strength, and weight status in US older adults. J Affect Disord. 2018;238:305–10.
Cho J, Johnson BD, Watt KD, Kim CH. Greater muscular strength is associated with a lower risk of pulmonary dysfunction in individuals with non-alcoholic fatty liver disease. J Clin Med. 2022;11:4151.
Hong YS, Kim H. Hand grip strength and health-related quality of life in postmenopausal women: a national population-based study. Menopause. 2021;28:1330–9.
Gubelmann C, Vollenweider P, Marques-Vidal P. Association of grip strength with cardiovascular risk markers. Eur J Prev Cardiol. 2017;24:514–21.
Chen PJ, Lin MH, Peng LN, Liu CL, Chang CW, Lin YT, et al. Predicting cause-specific mortality of older men living in the Veterans home by handgrip strength and walking speed: a 3-year, prospective cohort study in Taiwan. J Am Med Dir Assoc. 2012;13:517–21.
Takata Y, Ansai T, Akifusa S, Soh I, Yoshitake Y, Kimura Y, et al. Physical fitness and 4-year mortality in an 80-year-old population. J Gerontol Biol Sci Med Sci. 2007;62:851–8.
Parra-Soto S, Pell JP, Celis-Morales C, Ho FK. Absolute and relative grip strength as predictors of cancer: prospective cohort study of 445 552 participants in UK Biobank. J Cachexia Sarcopenia Muscle. 2022;13:325–32.
Korea Disease Control and Prevention Agency: The Sixth Korea National Health and Nutrition Examination Survey (KNHANES VI-2,3). Korea: Korea Disease Control and Prevention Agency. 2015. https://knhanes.kdca.go.kr/knhanes/sub03/sub03_02_05.do. Accessed 4 May 2023.
Korea Disease Control and Prevention Agency: The Seventh Korea National Health and Nutrition Examination Survey (KNHANES VII-1,2,3). Korea: Korea Disease Control and Prevention Agency. 2018. Available from: https://knhanes.kdca.go.kr/knhanes/sub03/sub03_02_05.do. Accessed 4 May 2023.
Korea Disease Control and Prevention Agency: The Eighth Korea National Health and Nutrition Examination Survey (KNHANES VIII-1). Korea: Korea Disease Control and Prevention Agency. 2019. https://knhanes.kdca.go.kr/knhanes/sub03/sub03_02_05.do. Accessed 4 May 2023.
Rossi E, Biasucci LM, Citterio F, Pelliccioni S, Monaco C, Ginnetti F, et al. Risk of myocardial infarction and angina in patients with severe peripheral vascular disease: predictive role of C-reactive protein. Circulation. 2002;105:800–3.
Jespersen CM, Als-Nielsen B, Damgaard M, Hansen JF, Hansen S, Helø OH, et al. Randomised placebo controlled multicentre trial to assess short term clarithromycin for patients with stable coronary heart disease: CLARICOR trial. BMJ. 2006;332:22–7.
Manzi S, Meilahn EN, Rairie JE, Conte CG, Medsger TA Jr, Jansen-McWilliams L, et al. Age-specific incidence rates of myocardial infarction and angina in women with systemic lupus erythematosus: comparison with the Framingham Study. Am J Epidemiol. 1997;145:408–15.
Chi JH, Lee BJ. Association of myocardial infarction and angina pectoris with obesity and biochemical indices in the South Korean population. Sci Rep. 2022;12:13769.
Perez GH, Nicolau JC, Romano BW, Laranjeira R. Smoking-associated factors in myocardial infarction and unstable angina: do gender differences exist? Addict Behav. 2007;32:1295–301.
Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D, et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension. 2020;75(6):1334–57.
Chi JH, Lee BJ. Risk factors for hypertension and diabetes comorbidity in a Korean population: a cross-sectional study. PLoS ONE. 2022;17(1):e0262757.
World Health Organization, Screening for Type 2 Diabetes. Report of a World Health Organization and International Diabetes Federation meeting, Geneva, 2003.
Laufs U, Dent R, Kostenuik PJ, Toth PP, Catapano AL, Chapman MJ. Why is hypercholesterolaemia so prevalent? A view from evolutionary medicine. Eur Heart J. 2019;40(33):2825–30.
Cohen JD, Cziraky MJ, Cai Q, Wallace A, Wasser T, Crouse JR, et al. 30-year trends in serum lipids among United States adults: results from the National Health and Nutrition examination surveys II, III, and 1999–2006. Am J Cardiol. 2010;106(7):969–75.
Lee BJ, Kim JY. Indicators of hypertriglyceridemia from anthropometric measures based on data mining. Comput Biol Med. 2015;57:201–11.
Lee BJ, Chi JH. Association between anemia and grip strength indices combined with anthropometry in the Korean population. Sci Rep. 2023;13(1):18517.
Chi JH, Lee BJ. Association between arthritis and hand grip strength indices combined with anthropometry in an older Korean population. PLoS ONE. 2023;18(8):e0291046.
Valensi P, Lorgis L, Cottin Y. Prevalence, incidence, predictive factors and prognosis of silent myocardial infarction: a review of the literature. Arch Cardiovasc Dis. 2011;104:178–88.
Galih A, Tjahjono CT, Widito S, Ruspiono E. Acute myocardial infarction in a 25-years-old male: understanding the risk and comprehensive management. Heart Sci J. 2023;4:44–50.
Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364:937–52.
Dunder K, Lind L, Lagerqvist B, Zethelius B, Vessby B, Lithell H. Cardiovascular risk factors for stable angina pectoris versus unheralded myocardial infarction. Am Heart J. 2004;147:502–8.
Sathvik M, Kalva ECSS, Suma G. A study on acute myocardial infarction and its prognostic predictors. Cureus. 2023;15:e34775.
Caccamo G, Bonura F, Bonura F, Vitale G, Novo G, Evola S, et al. Insulin resistance and acute coronary syndrome. Atherosclerosis. 2010;211:672–5.
Rasool R, Unar A, Jafar TH, Chanihoon GQ, Mubeen B. A role of thyroid hormones in acute myocardial infarction: an update. Curr Cardiol Rev. 2023;19:e280422204209.
Leong DP, Smyth A, Teo KK, McKee M, Rangarajan S, Pais P, et al. Patterns of alcohol consumption and myocardial infarction risk: observations from 52 countries in the INTERHEART case-control study. Circulation. 2014;130:390–8.
Sobue Y, Suzuki M, Ohashi Y, Koshima H, Okui N, Funahashi K, et al. Validation of grip strength as a measure of frailty in rheumatoid arthritis. Sci Rep. 2022;12:21090.
Kwak Y, Kim Y, Chung H. Sex-Associated differences in the Handgrip Strength of Elderly individuals. West J Nurs Res. 2020;42(4):262–8.
Raed A, Bilz J, Cortez-Cooper M, Young L, Chen L, Cromer P, et al. Handgrip and sex-specific cardiometabolic risk factors in Hispanic/Latino migrant farmworkers. Sci Rep. 2021;11(1):10272.
Choi KM, Lee KW, Kim SG, Kim NH, Park CG, Seo HS, et al. Inflammation, insulin resistance, and glucose intolerance in acute myocardial infarction patients without a previous diagnosis of diabetes mellitus. J Clin Endocrinol Metab. 2005;90:175–80.
Cesari M, Penninx BWJH, Pahor M, Lauretani F, Corsi AM, Williams GR, et al. Inflammatory markers and physical performance in older persons: the InCHIANTI study. J Gerontol Biol Sci Med Sci. 2004;59:242–8.
Skoog T, Dichtl W, Boquist S, Skoglund-Andersson C, Karpe F, Tang R, et al. Plasma tumour necrosis factor-alpha and early carotid atherosclerosis in healthy middle-aged men. Eur Heart J. 2002;23:376–83.
Lebovitz HE, Banerji MA. Point: visceral adiposity is causally related to insulin resistance. Diabetes Care. 2005;28:2322–5.
Cleasby ME, Jamieson PM, Atherton PJ. Insulin resistance and sarcopenia: mechanistic links between common co-morbidities. J Endocrinol. 2016;229:R67–81.
Sayer AA, Syddall HE, Dennison EM, Martin HJ, Phillips DIW, Cooper C, et al. Grip strength and the metabolic syndrome: findings from the hertfordshire cohort study. QJM. 2007;100:707–13.
Funding
This study was supported by the Korea Institute of Oriental Medicine (KIOM; Grant nos. KSN1823130 and KSN1922110), funded by the Korean government.
Author information
Authors and Affiliations
Contributions
Chi JH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Writing– original draft, and Writing– review & editing. Lee BJ: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Writing– original draft, and Writing– review & editing. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
The National Health and Nutrition Examination Survey (KNHANES) was approved by the Research Ethics Committee of the Korea Disease Control and Prevention Agency (IRB: 2013-07CON-03–4 C, 2013-12EXP-03–5 C, 2018-01-03-P-A, 2018-01-03-C-A). This study, which was based on the KNHANES dataset, was also ethically approved by the Institutional Review Board of the Korea Institute of Oriental Medicine (IRB No. I-2209/009 − 001). This study was conducted in accordance with the Helsinki Declaration, and all methods followed relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors have no conflicts of interest to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chi, J.H., Lee, B.J. Association of relative hand grip strength with myocardial infarction and angina pectoris in the Korean population: a large-scale cross-sectional study. BMC Public Health 24, 941 (2024). https://doi.org/10.1186/s12889-024-18409-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-18409-w