
Abstract
Objective
To explore the association between cardiovascular health (CVH) measured by Life’s Essential 8 (LE8) and the prevalence of urinary incontinence (UI).
Method
A cross-section study was conducted using data from the National Health and Nutrition Examination Survey 2007–2012. 22,609 people aged ≥ 20 years with complete information on LE8 metrics and UI questionnaires were enrolled. Participants were divided into three groups (low: < 50, moderate: ≥ 50 and < 80, high: ≥ 80) based on the cut-off of LE8. Weighted proportions, multivariable logistic regression analysis and stratified logistic regression were performed to examine the association between LE8 and the prevalence of three types of UI separately (stress UI (SUI), urge UI (UUI), mixed UI (MUI)) by confounding factors adjusted. Spline smooth was conducted to find whether a linear relationship existed. In addition, sensitive analyses were also conducted to observe the stability.
Result
A total of 22,609 adults were involved in the study, and participants were divided into three groups (low 42.2 ± 6.3, moderate 66.1 ± 8.1, high 86.8 ± 5.1) according to the cut-off points of LE8. The multivariable logistic regression suggested that LE8 is inversely associated with the prevalence of SUI (OR = 0.98, 95%CI 0.98 to 0.99), UUI (OR = 0.98, 95%CI 0.98 to 0.99), and MUI (OR = 0.98, 95%CI 0.97 to 0.98) in the fully-adjusted model. Compared with the low group, people with high scores of LE8 had a lower prevalence of SUI (OR = 0.45, 95%CI 0.37 to 0.55), UUI (OR = 0.49, 95%CI 0.40 to 0.60), and MUI (OR = 0.41, 95%CI 0.30 to 0.55). The result of the sensitive analysis showed the robustness of the main analysis.
Conclusion
The prevalence of UI (SUI, UUI, or MUI) is inversely associated with the LE8 score, which suggests that maintaining a good CVH with a higher LE8 score is accompanied by lower prevalence rates of UUI, SUI, and MUI.
Similar content being viewed by others

Introduction
Urinary incontinence (UI) stands as one of the most prevalent afflictions within the realm of urological disorders, and confounds a substantial number of individuals through its manifestation in lower urinary tract symptoms (LUTS). The three common types of UI are urge UI (UUI), stress UI (SUI), and mixed UI (MUI) which is a combination of the former two types. A large-scale cross-sectional investigation in the USA proves the prevalence of UI is 49.6% in females. Among them, the preeminent type is SUI, constituting about 50%, followed by MUI (34.3%) and UUI (15.9%) [1]. In addition, UI impacts the quality of life and is considered an increasing psychophysiological burden on people and an economic burden on society [2]. UI is influenced by various factors, and the prevalence rates of the subtypes also differ depending on different factors. Although the mechanism of UI is complicated, it is well-known that lifestyle habits (smoking, physical activity, fluid intake) and chronic diseases (cardiovascular disease CVD, obesity, diabetes, hypertension) promote UI development [3,4,5]. Thus, it is indispensable to identify the risk factors and make timely interventions, which will benefit bladder functionality amelioration and UI prevention.
Recent research highlights the significant societal and economic impact of cardiovascular health and urinary incontinence (UI). Evidence suggests a bidirectional relationship between these conditions, with studies showing that poor cardiovascular health increases the risk of developing UI, likely due to shared risk factors like aging, obesity, and diabetes [6]. Conversely, UI has been associated with a higher risk of developing cardiovascular disease, potentially through mechanisms involving chronic inflammation, autonomic dysfunction, and endothelial dysfunction. Both cardiovascular health and UI share common risk factors and pathophysiological mechanisms, such as vascular endothelial dysfunction, autonomic nervous system dysregulation, and chronic inflammation [7,8,9]. These shared pathways indicate potential common underlying causes and imply that interventions targeting cardiovascular risk factors could also impact UI prevalence and severity. Therefore, understanding the connection between UI and cardiovascular health is crucial.
In 2010, the American Heart Association (AHA) set ideal goals for cardiovascular health (CVH), which is defined by Life’s Simple 7 (LS7). Research proves a close correlation between CVH, as quantified by LS7, and the prevalence as well as all-cause mortality of CVD [10]. Some studies also substantiate that the seven goals are related to lower risks of diabetes, cancer, and depression, all of which are the risk factors of CVD [11,12,13]. However, certain inherent limitations have constrained the capacity of LS7 for a comprehensive and systematic assessment of CVH. Therefore, Life's Essential 8 (LE8) was introduced in 2022 to update and enhance the AHA's construct of CVH in rectifying these limitations. Primarily, sleep health was incorporated into the scoring system for the first time. Additionally, the classification of the smoking status now encompasses the use of inhaled nicotine-delivery systems and exposure to secondhand smoke, broadening the scope beyond merely combustible tobacco usage. In addition, the definitions of other factors of LS7 were enriched and corrected, such as plasma glucose and blood lipids [14]. The LE8 scoring framework is more sensitive to individual differences and highlights the influence of societal factors on physical and mental health. It is also more comprehensive and dependable in evaluating cardiovascular health compared to LS7. A recent study found that approximately 19 million adults (47.3%) who were initially classified as having ideal Cardiovascular Health (CVH) based on the LS7 criteria were subsequently reclassified as having middle or low CVH according to LE8 [15].
To the best of our knowledge, there is no research focusing on the association between CVH accessed by the new LE8 metrics and the prevalence of UI. Therefore, our study aimed to explore whether a significant association existed between LE8 and UI using a nationally representative and ethnically diverse populace of adults in the US.
Method
Study population and design
The entirety of the dataset employed for this study was drawn from NHANES 2007–2018 (six cycles: 2007–2008, 2009–2010, 2011–2012, 2013–2014, 2015–2016, 2017–2018). NHANES is a national, representative, and cross-sectional survey that has been updated every two years since 1999. The data in NHANES are based on examinations, questionnaires, and laboratories. The objective of the NHANES is to measure the health and nutrition status of individuals in the United States. Furthermore, the database is accessible to researchers for free. There were 59,842 people involved initially. First, pregnant women (n = 372) and participants aged less than 20 years old (n = 25,072) were removed. Then, people with missing data about LE-8 (n = 10,782) or urinary incontinence (n = 1,007) were eliminated from the study. Finally, a total of 22,609 participants were enrolled (details in Fig. 1).

Flow diagram of obtaining the final inclusion in the population
All NHANES study protocols were approved by the Ethics Review Committee of the National Center for Health Statistics (NCHS), and consent was obtained from all participants.
Life’s essential 8 score
LE8 consists of 8 components, including 4 health behaviors and 4 health factors. The former involves physical activity, diet, nicotine exposure, and sleep. The latter includes blood pressure, non-high-density cholesterol lipoprotein (non-HDL), blood glucose, and body mass index (BMI). Information on physical activity (mins/week), nicotine exposure (combustible tobacco use and secondhand smoke exposure), and sleep (hours/night) was deprived directly from questionnaires. Healthy Eating Index-2015 (HEI-2015) was utilized to assess the quality of diet with 24-h dietary recall [16]. All of the blood samples were obtained with at least 8 h of fasting to assess plasma glucose, blood lipids, and hemoglobin Alc levels. Non-HDL was calculated as total cholesterol—HDL. Systolic and diastolic blood pressures were determined by averaging the first three blood pressure measurements. BMI was calculated as weight(kg)/height(m)2. All of the above operations were performed by well-trained staff using standardized methods. Each scale of the 8 metrics ranged from 0 to 100, and the overall LE8 score was equal to the average of the 8 metrics. The overall score was defined as a category variable (low: < 50, moderate: ≥ 50 and < 80, high: ≥ 80).
Urinary incontinence
People aged over 20 years old were required to answer the question about UI asked by well-trained interviewers. A positive answer to the question “During the past 12 months, have you leaked or lost control of even a small amount of urine with an activity like coughing, lifting, or exercise?” was grouped as SUI. Those who answered “yes” to the question “During the past 12 months, have you leaked or lost control of even a small amount of urine with an urge or pressure to urinate and you couldn't get to the toilet fast enough?” were considered as UUI. Moreover, people who had positive answers to both questions were considered to suffer from MUI. UI was defined when people had any one of the above conditions.
Covariates
The information about covariates was collected through questionnaires, examinations, and laboratories. Continuous variables included age, and poverty income (PIR). Categorical variables included gender, race, marital status, education, alcohol, CVD, stroke, and cancer. Age was classified into 20–34, 35–49, 50–64, and over 65 years old. Marital status was stratified into married/living with a partner, divorced/separated/widowed, and never married. Races were grouped as Mexican Americans, other Hispanics, non-Hispanic black, non-Hispanic white, and other races. The condition of education was grouped as less than 9th grade, 9th to 11th grade, high school graduate, some college, and college graduate or above. Alcohol was defined as never (< 12 drinks in a lifetime), former (≥ 12 drinks in 1 year and not drinking in last year, or not drinking in last year but drinking ≥ 12 drinks in a lifetime), and now. The other covariates (CVD, stroke, and cancer) were categorized as all no/yes.
Statistical analysis
Continuous variables are expressed as mean ± standard errors (SEs), and categorical variables are expressed as percentages. The participants were divided into three groups (low, moderate, and high) based on LE8. Linear regression was used to analyze the relationship between continuous variables, and Chi-square analysis was used to test the correlation between categorical variables.
Three multivariable logistic regression models were conducted to explore the association between LE8 and the three types of UI separately. Stratified analysis and tests for trends were applied for further exploration. The non-adjusted model was out of any variable adjusted. The minimally-adjusted model was adjusted for age, gender, and race. In the fully-adjusted model, the other covariates were adjusted, including marital status, education, PIR, CVD, alcohol, cancer, and stroke. Additionally, a generalized additive model which was utilized in spline smoothing and the likelihood ratio test aimed to demonstrate the linear or non-linear association between LE8 and the prevalence of UUI, SUI, or MUI. Both interactive and subgroup analyses were performed to explore the potential modifiers of the relationship between LE8 and the prevalence of UI. To verify the stability, sensitivity analyses were performed. 1. To ensure the analysis stability and eliminate the impact of extreme values, we conducted a sensitivity analysis where extreme values (LE8 scores > 99% and < 1%) were excluded from the dataset. 2. To verify the linear relationship between LE8 and the prevalence of UI, multivariable logistic regression and spline smoothing were performed.
All analyses in this study were conducted using sample weights recommended by the Centers for Disease Control and Prevention (CDC) from the National Health and Nutrition Examination Survey (NHANES) (Supplementary Material 1). These weights were essential for ensuring the sample's representativeness of the US civilian population and for producing unbiased national estimates. All the above statistical analyses were completed on R 3.6.3 (http://www.R-project.org, the R Foundation) and EmpowerStats (http://www.empowerstats.com, X&Y Solutions, Inc.). P less than 0.05 was considered statistically significant.
Results
Baseline characteristics
This study involved 22,609 adults. The participants were divided into three groups based on the two cut-off points of LE8: low LE8 (n = 2,994), moderate LE8 (n = 15,124), and high LE8 (n = 4,491). There were significant differences in all of the baseline characteristics among the three groups (Table 1). Compared to the other two groups, the high LE8 group involved more females. In addition, the high LE8 group had the youngest subjects (42.0 ± 16.0), the highest PIR (3.5 ± 1.6), and the highest proportions of higher-level education (college or above, 80.3%) and alcohol drinking (81.3%). In contrast, the high LE8 group accounted for the lowest in SUI, UUI, MUI, cancer, stroke, CVD, and single (divorced/separate/widowed and never married) than the other two groups. People with UI (SUI, UUI, MUI) were more likely to have lower overall LE8 scores (64.0 ± 14.9, 64.0 ± 14.9, 62.5 ± 14.9, respectively) (Table S1). The LE8 metrics were almost significantly lower in people with UI, except for the diet score (higher score of HEI-2015 in people with UUI, 41.3 ± 31.3).
Multivariable logistic analysis
Three multivariable logistic regression models were used and showed a negative association between LE8 and the prevalence of SUI, UUI, and MUI (Table 2). In the fully-adjusted model, people with lower LE8 scores had a higher prevalence of SUI (OR = 0.98, 95%CI 0.98 to 0.99), UUI (OR = 0.98, 95%CI 0.98 to 0.99) and MUI (OR = 0.98, 95%CI 0.97 to 0.98) (all P < 0.001). Compared with the low score group, the odds ratios for people with moderate and high LE8 scores to suffer from SUI were 0.66 (95%CI 0.57 to 0.76), 0.45 (0.37 to 0.55), to develop UUI was 0.64 (0.56 to 0.74), 0.49 (0.40 to 0.60), and to gain MUI were 0.67 (0.56 to 0.80), 0.41 (0.30 to 0.55) in the fully-adjusted model. With a 10-point increase in the score, the risk of SUI decreased to 0.84 (95% CI 0.81 to 0.87). The same trend was observed in the people with UUI (OR = 0.84, 95%CI 0.81 to 0.88) or MUI (OR = 0.80, 95%CI 0.76 to 0.85).
Spline smoothing and piecewise regression
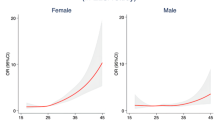
The spline smoothing demonstrated that the LE8 score was negatively and linearly associated with the prevalence of SUI and UUI (Fig. 2). Namely, the dose–response relationship meant that a higher LE8 score was significantly associated with lower prevalence of SUI and UUI.

A spline smoothing demonstrated the association between LE8 and the prevalence of SUI (A), UUI (B), and MUI (C)
The association between the LE8 score and the prevalence of MUI was investigated using smooth curve fitting and piecewise linear regression. Outliers were excluded according to the Chanwennt criterion. The plot revealed a curve association. With a two-segment linear regression model, we calculated an inflection point of 52.5 (Table 3). When the LE8 score was more than 52.5, the risk of developing MUI decreased by 2.2% with the increase of one LE8 point (OR = 0.98, 95%CI 0.97 to 0.98). When the LE8 score was less than 52.5, each unit increase in LE8 tended to increase the 4‰ risk of MUI, though not significantly (OR = 1.00, 95%CI 0.99 to 1.02). P for the likelihood-ratio test was less than 0.001, indicating the association between LE8 and MUI was non-linear.
Analyses of interactions and subgroups
Interaction and subgroup analyses were conducted to find whether some factors modified the association between LE8 and the prevalence of the three types of UI in the fully adjusted model (Table 4). We found the interaction is statistically significant of age and gender on the association between LE8 and the prevalence of SUI or MUI. The association between LE8 and the prevalence of SUI was modified by race and cancer. In addition, the association between LE8 and the prevalence of UUI was affected by PIR and education. However, apart from education, the odds ratio of the stratified analyses with the variables above was less than 1, so the direction was consistent. Therefore, the interactions were deemed spurious and not meaningful. As for the effect on the association between LE8 and the prevalence of UUI made by education, the odds ratios of less than 9th grade, 9-11th grade, high school graduates, some college, and college graduates or above were 1.003, 0.983, 0.983, 0.983, 0.980, respectively, with p of 0.014 for interaction.
Sensitivity analysis
Some sensitivity analyses were conducted to verify the stability of the results. (1) In the fully-adjusted model, the multivariable logistic regression with extreme values of LE8 excluded showed that the negative association between LE8 and SUI, UUI, or MUI was still present (Table S2). (2) There was a significantly negative association between LE8 and the prevalence of UI (OR = 0.982, 95%CI 0.978 to 0.986). The same negative relationship between the two was also observed in the subgroup analysis of LE8 and the test for trend (Table S3). In addition, the spline smoothing proved a negative and linear association between LE8 and the prevalence of UI (Fig. S1).
Discussion
This cross-sectional study demonstrates an inverse association between LE8 and the prevalence of SUI, UUI, or MUI. The dose–response relationship means that a higher LE8 score is significantly associated with a lower prevalence of SUI and UUI. In addition, this study also reveals a curve-decreasing relationship between LE8 and MUI. In other words, with the decrease in LE8 score, the prevalence of MUI gradually increases and eventually stabilizes. Moreover, education significantly affects the association between LE8 and the prevalence of UUI. Sensitivity analysis shows the same inverse trend between LE8 and the three types of UI. Thus, we believe the findings are robust.
As the definition of CVH was updated and called LE8 by AHA, growing evidence proves that the composite LE8 score does a good job of evaluating CVH and predicting inactive cardiovascular outcomes (CVD, stroke, atherosclerotic cardiovascular diseases, and cardiovascular mortality) [17,18,19,20]. Some studies show that people with heart failure are more likely to develop UI and the frequency of UI is high [21, 22]. Another prospective study involving 100 participants presents the same trend and shows that patients with the impact of two diseases combined have a worse quality of life [23]. A meta-analysis with 14 high-quality studies shows that men with moderate to severe LUTS, including UI, have a 68% increased likelihood of experiencing significant adverse cardiac events [24]. These studies demonstrate that CVH is related to LUTS, including voiding and storage symptoms, and strongly support our findings that CVH measured by LE8 is inversely associated with the prevalence of UI. Thus, it is critical that the awareness of monitoring CVH and screening adverse cardiac events shall be raised, which is essential for UI prevention and management. Although the underlying mechanism is complex and yet unclear, the use and dosages of furosemide and beta-blockers may play a modest role [25]. Furthermore, changes in autonomic neuromodulation, inflammatory response, and blood supply by CVH may also significantly affect UI development [3, 26, 27].
The new and updated metrics of LE8 are not only closely related to CVH but also act as protective or detrimental factors for UI. The AHA added sleep health to the initial seven factors (LS7) for CVH assessment in 2022. A prospective study reveals that maintaining healthy sleep patterns (based on sleep duration, chronotype, snoring, insomnia, and daytime dozing) can reduce the risk of CVD associated with a poor lifestyle [28]. Additionally, cardiovascular baroreflex circuits are also indispensable to sleep–wake brain-state regulation, and an interaction may be present [29]. Recently, Chen et al. confirmed a U-shaped association between sleep duration and the prevalence of UI. Normal sleep duration (7 to 9 h) is reversely associated with UI, and people with insufficient or excessive sleep are more likely to develop UI [30]. Moreover, Jooyeon et al. revealed that urinary symptoms were improved significantly with great sleep efficiency via a biofeedback-based sleep improvement program [31]. Therefore, sleep may also mediate the association between CVH and UI, but more research is needed to explore the underlying mechanism.
In addition, the other seven metrics of LE8 are also closely related to UI, and the effect on UI shall not be concealed. Studies show that not only the occurrence but also the components of metabolic syndrome (abdominal obesity, hypertension, diabetes, hyperlipidemia) increase the risk of UI [32, 33]. Other studies prove that a higher intake of certain diet components increases the risk of UI, such as protein, fat, and micronutrients (zinc and vitamin B12) [34, 35]. These diet components will affect the circulating sex hormone, urine secretion, and systemic inflammatory markers, which raise the risk of UI. However, a ketogenic diet can also significantly improve UI [36]. Therefore, a healthy diet may become an effective preventive and interventive strategy. A large cross-sectional study (EPINCONT) for adult women demonstrates that former and current smokers are more likely to develop UI, especially severe UI. Notably, the risk of UI among smoking quitters is still higher than among non-smokers, so a remaining effect may be present [37]. The increased risk of UI in smokers may be attributed to more intense and frequent coughs, the anti-estrogenic effect, and the disruption of collagen synthesis caused by smoking [5, 38, 39]. Moreover, sedentary behavior and less physical activity are recognized as risk factors for UI. A prospective cohort study uncovers an inverse dose–response relationship between active physical activity and the prevalence of UI, which may be achieved in part through weight loss [4]. However, a case–control study demonstrates that greater strenuous activity in the young is positively associated with a higher prevalence of UI in later life [40]. Exercise intensity and exercise volume measure different titles. High-volume physical activity tends to decrease, and high-intensity physical activity tends to raise the risk of UI. In our study, physical activity was systematically quantified through exercise metabolic equivalent to avoiding the bias caused by a single evaluation. Moreover, most studies support this inverse association between physical activity and UI [41, 42]. Thus, the occurrence of UI is considered a possible consequence of a low LE8 score and poor CVH, and maintaining a healthy lifestyle and factors for CVH are critical in preventing UI. Nevertheless, the common pathophysiologic pathways may exist and merit further investigation.
The present study shows that education modifies the association between LE8 and the prevalence of UUI. Namely, the negative relationship is more obvious among people with low education levels (less than 9th grade). Reportedly, less-educated individuals have more potential risk factors (bad lifestyle and poor healthcare) and higher occurrence of CVD [43]. A nationwide study during the COVID-19 pandemic demonstrates that low-educated residents (no more than lower secondary education) are featured by poor clinical awareness and action for major cardiovascular events, which will increase the risk of cardiovascular morbidity and mortality [44]. In addition to the increased UUI risk factors, low-educated individuals are reluctant to talk about UI, and this symptom is less likely to be recognized as a disease, which makes the disease an overlooked and poorly managed condition due to poorer knowledge [45, 46].
The strengths and shortcomings of this study shall also be mentioned. The first and major strength is that it is the first work to explore the association between the prevalence of UI and CVH which is measured by the new LE8 score system, and it makes significant clinical and public health effects because of the UI epidemic. Second, the large sample size of the muti-ethnic and community-based population makes the results more reliable and generalizable. However, the shortcomings shall also be considered. First, the cross-sectional design limits the assessment of the causality between CVH and the prevalence of UI. Second, the information on UI was collected by trained interviewers via unified questionnaires, but a recall basis was inevitable. Third, although adjustments were made for many potential confounding factors, unknown confounding effects due to unmeasured variables cannot be fully ruled out.
Conclusions
The prevalence of UI is inversely associated with the LE8 score. This inverse linear dose–response relationship indicates that excellent CVH with a higher LE8 score is accompanied by lower prevalence rates of UUI, SUI, and MUI. Early therapeutic approaches for UI prevention and intervention may be found via health behaviors and factor regulation for CVH. Nevertheless, further in-depth and high-quality prospective studies are needed to elaborate on the underlying mechanism between CVH and the prevalence of UI.
Availability of data and materials
Data available in a publicly accessible repository that does not issue DOIs. Publicly available datasets were analyzed in this study. These data can be found here: https://www.cdc.gov/nchs/nhanes/index.htm.
References
Dooley Y, Kenton K, Cao G, Luke A, Durazo-Arvizu R, Kramer H, Brubaker L. Urinary incontinence prevalence: results from the National Health and Nutrition Examination Survey. J Urol. 2008;179(2):656–61.
Haylen BT, de Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, Monga A, Petri E, Rizk DE, Sand PK, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 2010;29(1):4–20.
Hotaling JM, Sarma AV, Patel DP, Braffett BH, Cleary PA, Feldman E, Herman WH, Martin CL, Jacobson AM, Wessells H, et al. Cardiovascular Autonomic Neuropathy, Sexual Dysfunction, and Urinary Incontinence in Women With Type 1 Diabetes. Diabetes Care. 2016;39(9):1587–93.
Lamerton TJ, Mielke GI, Brown WJ. Urinary incontinence, body mass index, and physical activity in young women. Am J Obstet Gynecol. 2021;225(2):164.e161-164.e113.
Bump RC, McClish DK. Cigarette smoking and urinary incontinence in women. Am J Obstet Gynecol. 1992;167(5):1213–8.
Markland AD, Vaughan CP, Okosun IS, Goode PS, Burgio KL, Johnson TM 2nd. Cluster analysis of multiple chronic conditions associated with urinary incontinence among women in the USA. BJU Int. 2018;122(6):1041–8.
Dai J, Miller AH, Bremner JD, Goldberg J, Jones L, Shallenberger L, Buckham R, Murrah NV, Veledar E, Wilson PW, et al. Adherence to the mediterranean diet is inversely associated with circulating interleukin-6 among middle-aged men: a twin study. Circulation. 2008;117(2):169–75.
Cartwright R, Afshan I, Derpapas A, Vijaya G, Khullar V. Novel biomarkers for overactive bladder. Nat Rev Urol. 2011;8(3):139–45.
Liu G, Wang X, Sun X, Deng C, Atala A, Zhang Y. The effect of urine-derived stem cells expressing VEGF loaded in collagen hydrogels on myogenesis and innervation following after subcutaneous implantation in nude mice. Biomaterials. 2013;34(34):8617–29.
Peng Y, Wang Z, Dong B, Cao S, Hu J, Adegbija O. Life’s Simple 7 and ischemic heart disease in the general Australian population. PLoS ONE. 2017;12(10): e0187020.
Fretts AM, Howard BV, McKnight B, Duncan GE, Beresford SA, Mete M, Zhang Y, Siscovick DS. Life’s Simple 7 and incidence of diabetes among American Indians: the Strong Heart Family Study. Diabetes Care. 2014;37(8):2240–5.
Han L, You D, Ma W, Astell-Burt T, Feng X, Duan S, Qi L. National Trends in American Heart Association Revised Life’s Simple 7 Metrics Associated With Risk of Mortality Among US Adults. JAMA Netw Open. 2019;2(10): e1913131.
Beydoun MA, Georgescu MF, Hossain S, Beydoun HA, Fanelli-Kuczmarski MT, Evans MK, Zonderman AB. Life’s simple 7 and its association with trajectories in depressive symptoms among urban middle-aged adults. J Affect Disord. 2023;333:447–58.
Lloyd-Jones DM, Allen NB, Anderson CAM, Black T, Brewer LC, Foraker RE, Grandner MA, Lavretsky H, Perak AM, Sharma G, et al. Life’s Essential 8: Updating and Enhancing the American Heart Association’s Construct of Cardiovascular Health: A Presidential Advisory From the American Heart Association. Circulation. 2022;146(5):e18–43.
Shetty NS, Parcha V, Patel N, Yadav I, Basetty C, Li C, Pandey A, Kalra R, Li P, Arora G, et al. AHA Life’s essential 8 and ideal cardiovascular health among young adults. Am J Prev Cardiol. 2023;13: 100452.
Yin S, Wang J, Bai Y, Yang Z, Cui J, Xiao Y, Wang J. Association Between Healthy Eating Index-2015 and Kidney Stones in American Adults: A Cross-Sectional Analysis of NHANES 2007–2018. Front Nutr. 2022;9: 820190.
Li C, Li Y, Zhao M, Zhang C, Bovet P, Xi B. Using the New “Life’s Essential 8” Metrics to Evaluate Trends in Cardiovascular Health Among US Adults From 2005 to 2018: Analysis of Serial Cross-sectional Studies. JMIR Public Health Surveill. 2023;9: e45521.
Perng W, Aris IM, Slopen N, Younoszai N, Swanson V, Mueller NT, Sauder KA, Dabelea D. Application of Life’s Essential 8 to assess cardiovascular health during early childhood. Ann Epidemiol. 2023;80:16–24.
Radovanovic M, Jankovic J, Mandic-Rajcevic S, Dumic I, Hanna RD, Nordstrom CW. Ideal Cardiovascular Health and Risk of Cardiovascular Events or Mortality: A Systematic Review and Meta-Analysis of Prospective Studies. J Clin Med. 2023;12(13):4417.
Li X, Ma H, Wang X, Feng H, Qi L. Life’s Essential 8, Genetic Susceptibility, and Incident Cardiovascular Disease: A Prospective Study. Arterioscler Thromb Vasc Biol. 2023;43(7):1324–33.
Hwang R, Chuan F, Peters R, Kuys S. Frequency of urinary incontinence in people with chronic heart failure. Heart Lung. 2013;42(1):26–31.
Palmer MH, Hardin SR, Behrend C, Collins SK, Madigan CK, Carlson JR. Urinary incontinence and overactive bladder in patients with heart failure. J Urol. 2009;182(1):196–202.
Poole K, Kerlin M, Wynne R. Prevalence and characteristics of urinary incontinence in a cohort of patients with chronic heart failure. Heart Lung. 2017;46(2):67–73.
Gacci M, Corona G, Sebastianelli A, Serni S, De Nunzio C, Maggi M, Vignozzi L, Novara G, McVary KT, Kaplan SA, et al. Male Lower Urinary Tract Symptoms and Cardiovascular Events: A Systematic Review and Meta-analysis. Eur Urol. 2016;70(5):788–96.
Finkelstein MM. Medical conditions, medications, and urinary incontinence. Analysis of a population-based survey. Can Fam Physician. 2002;48:96–101.
Goldberger JJ, Arora R, Buckley U, Shivkumar K. Autonomic Nervous System Dysfunction: JACC Focus Seminar. J Am Coll Cardiol. 2019;73(10):1189–206.
Yu HY, Shin JH, Yun H, Ryu CM, Lee S, Heo J, Lim J, Park J, Hong KS, Chung HM, et al. A Preclinical Study of Human Embryonic Stem Cell-Derived Mesenchymal Stem Cells for Treating Detrusor Underactivity by Chronic Bladder Ischemia. Stem Cell Rev Rep. 2021;17(6):2139–52.
Song Q, Wang M, Zhou T, Sun D, Ma H, Li X, Heianza Y, Qi L. The Lifestyle-Related Cardiovascular Risk Is Modified by Sleep Patterns. Mayo Clin Proc. 2022;97(3):519–30.
Yao Y, Barger Z, Saffari Doost M, Tso CF, Darmohray D, Silverman D, Liu D, Ma C, Cetin A, Yao S, et al. Cardiovascular baroreflex circuit moonlights in sleep control. Neuron. 2022;110(23):3986-3999.e3986.
Chen T, Zhan X, Xiao S, Fu B. U-shaped association between sleep duration and urgency urinary incontinence in women: a cross-sectional study. World J Urol. 2023;41(9):2429–35.
Park J, Park CH, Jun SE, Lee EJ, Kang SW, Kim N. Effects of biofeedback-based sleep improvement program on urinary symptoms and sleep patterns of elderly Korean women with overactive bladder syndrome. BMC Urol. 2019;19(1):109.
Gleicher S, Byler T, Ginzburg N. Association Between Stress Urinary Incontinence and the Components of Metabolic Syndrome Among Females 20–59 Years. Urology. 2020;145:100–5.
Ströher RLM, Sartori MGF, Takano CC, de Araújo MP, Girão M. Metabolic syndrome in women with and without stress urinary incontinence. Int Urogynecol J. 2020;31(1):173–9.
Dallosso H, Matthews R, McGrother C, Donaldson M. Diet as a risk factor for the development of stress urinary incontinence: a longitudinal study in women. Eur J Clin Nutr. 2004;58(6):920–6.
Bauer SR, Kenfield SA, Sorensen M, Subak LL, Phelan S, Gupta LR, Chen B, Suskind AM, Park AJ, Iglesia C, et al. Physical Activity, Diet, and Incident Urinary Incontinence in Postmenopausal Women: Women’s Health Initiative Observational Study. J Gerontol A Biol Sci Med Sci. 2021;76(9):1600–7.
Sun Y, Chen H, Bai Y, Zhang T, Bai W, Jiang B. Ketogenic diet may be a new approach to treatment stress urinary incontinence in obese elderly women: report of five cases. BMC Womens Health. 2022;22(1):402.
Hannestad YS, Rortveit G, Daltveit AK, Hunskaar S. Are smoking and other lifestyle factors associated with female urinary incontinence? The Norwegian EPINCONT Study Bjog. 2003;110(3):247–54.
Bohlin KS, Ankardal M, Pedroletti C, Lindkvist H, Milsom I. The influence of the modifiable life-style factors body mass index and smoking on the outcome of mid-urethral sling procedures for female urinary incontinence. Int Urogynecol J. 2015;26(3):343–51.
Fuganti PE, Gowdy JM, Santiago NC. Obesity and smoking: are they modulators of cough intravesical peak pressure in stress urinary incontinence? Int Braz J Urol. 2011;37(4):528–33.
Nygaard IE, Shaw JM, Bardsley T, Egger MJ. Lifetime physical activity and female stress urinary incontinence. Am J Obstet Gynecol. 2015;213(1):40.e41-40.e10.
Morrisroe SN, Rodriguez LV, Wang PC, Smith AL, Trejo L, Sarkisian CA. Correlates of 1-year incidence of urinary incontinence in older Latino adults enrolled in a community-based physical activity trial. J Am Geriatr Soc. 2014;62(4):740–6.
Maeda N, Urabe Y, Suzuki Y, Hirado D, Morikawa M, Komiya M, Mizuta R, Naito K, Shirakawa T. Cross-Sectional Study of the Prevalence and Symptoms of Urinary Incontinence among Japanese Older Adults: Associations with Physical Activity, Health-Related Quality of Life, and Well-Being. Int J Environ Res Public Health. 2021;18(2):360.
Hoeymans N, Smit HA, Verkleij H, Kromhout D. Cardiovascular risk factors in relation to educational level in 36 000 men and women in The Netherlands. Eur Heart J. 1996;17(4):518–25.
Andersen J, Strandberg-Larsen K, Gerds T, Gislason G, Torp-Pedersen C, Blanche P, Andersson C, Køber L, Fosbøl E, Phelps M, et al. Risk of major cardiovascular events according to educational level before and after the initial COVID-19 public lockdown: a nationwide study. J Epidemiol Community Health. 2021;75(9):829–35.
Xu D, Huang L, Gao J, Li J, Wang X, Wang K. Effects of an education program on toileting behaviors and bladder symptoms in overactive bladder patients with type 2 diabetes: A randomized clinical trial. Int J Nurs Stud. 2018;87:131–9.
Koffi AJD, Doumbia M, Fokou G, Keita M, Koné B, Abé NN. Community knowledge, attitudes and practices related to schistosomiasis and associated healthcare-seeking behaviours in northern Côte d’Ivoire and southern Mauritania. Infect Dis Poverty. 2018;7(1):70.
Acknowledgements
Not applicable.
Funding
This work was supported by the Key Research and Development Projects of Sichuan Science and Technology Department (grant numbers: 2022YFS0306).
Author information
Authors and Affiliations
Contributions
(I) Conception and design: J Wang, YF Xiao, (II) Administrative support and supervision: J Wang, (III) Collection and assembly of data: YF Xiao, YX Tang, JH Wang, S Yin, JW Cui, YQ Yang, K Huang, (IV) Data analysis and interpretation: YF Xiao, YX Tang, YJ Bai, (V) Manuscript writing: YF Xiao, (VI): Final approval of manuscript: all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was performed using public data from the National Center for Health Statistics (NCHS) program and the National Health and Nutrition Examination Survey (NHANES). The data have been de-identified and not merged or augmented in a way that has compromised the privacy of the participants. Therefore, the study requires no further approval and follows ethical guidelines. In addition, participant data were obtained from the publicly available NHANES, so no additional consent was obtained.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xiao, Y., Tang, Y., Wang, J. et al. Cardiovascular health assessed by the new life’s essential 8 and the prevalence of urinary incontinence in adults. BMC Public Health 24, 2136 (2024). https://doi.org/10.1186/s12889-024-19604-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19604-5