
Abstract
Background
Dependency on screen viewing (SV) has reached unprecedented levels, and mental health issues are becoming a major public health concern. However, the associations between SV, including variations in purposes, devices, and timing, and mental health remain unclear. This study aims to provide insights into these associations among university students.
Methods
This analysis used baseline data from a longitudinal cohort study among first-year university students matriculating in the 2021–2022 academic year. Self-reported data on sociodemographics, health behaviors and mental health outcomes alongside anthropometric measurements were collected. Unadjusted and adjusted logistic regression analyses were conducted.
Results
The average age of the 997 valid students was 20.2 years, with 59.6% being female and 41.4% male. Students spent 14.3 h daily on SV, with females reporting higher SV than males. Daily SV was predominant for study purposes (7.6 h/day). Computer usage was the highest (7.0 h/day), while TV usage was the lowest (1.7 h/day). Poor mental wellbeing was reported by 33.6% of students, while 13.9% experienced psychological distress. Compared to students with low total SV, those with high levels were more likely to have poor mental wellbeing [OR (95% CI): 1.40 (0.99, 1.98)] and psychological distress [1.56 (1.00, 2.44)]. High levels of recreational and study related SV were significantly associated with poor mental wellbeing [1.81 (1.27, 2.56)] and psychological distress [1.75 (1.11, 2.83)], respectively. Those with high levels of computer time were more likely to have poor mental wellbeing [1.44 (1.01, 2.06)], and high weekend day SV was associated with greater odds of psychological distress [2.16 (1.17, 4.06)].
Conclusions
SV among university students was high, as was the high prevalence of poor mental wellbeing and psychological distress. Greater SV was associated with poor mental wellbeing and psychological distress. Differences according to purpose of SV were noted. Although recreational SV was associated with poor mental wellbeing, study related SV was associated with psychological distress. Variations across different devices and timing were also noted. This highlights the need for further longitudinal research to understand the impact of SV on mental health and to guide interventions for promoting mental health of university students globally.
Similar content being viewed by others


Background
Screen viewing (SV) is typically defined as time spent in front of any digital/electronic device, such as television (TV), mobile phones, tablets, or computers [1, 2]. The dependency on screens for communication, information consumption, and entertainment has reached record levels among young adults, particularly university students [3]. Multiple countries including Canada, France, the United States, China, and South Africa have reported that the average SV for college students might vary from 5.5 to 11.5 h per day [4,5,6,7,8,9,10,11], with some studies considering only mobile phone use [4,5,6,7,8]. It has been established that young individuals from households with higher educational and financial statuses engage in more SV. Furthermore, East Asian countries tend to utilize smartphones more frequently than other regions [12]. This observation aligns with the wide variety of smartphone choices available in these countries and their rapid rate of technological adoption [12, 13]. However, the literature on the purpose behind screen use and type of screen device is much more limited, especially within the Asian context. Therefore, a detailed examination of SV behavior among Singaporean university students is crucial for understanding trends within both Asia and developed countries. Singapore is distinguished by having the highest per capita income in Asia and is also a global frontrunner in terms of the proportion of its population holding university degrees [14]. Additionally, the transition to college life, coupled with academic pressures, social changes, and lifestyle behavior changes, may have a profound impact on the mental wellbeing of university students in Singapore [15]. Poor mental wellbeing and psychological distress are increasingly recognized as major public health concerns among young adults, with higher incidence rates reported in this age group than in others [16, 17]. A global meta-analysis revealed that the pooled prevalence of depression and suicide-related outcomes was 14% and 25%, respectively, among university students [18]. Several cohort studies have shown that levels of psychological distress and anxiety increased after entering college and that distress levels did not return to pre-enrolment levels [16, 19].
Previous studies have examined the impact of SV on mental health in young generations, primarily children and adolescents, and it has been reported that SV might undermine wellbeing and exacerbate distress [20,21,22,23]. The evidence in young adults is less consistent. Some studies have indicated that young adults with high levels of anxiety or depression exhibit higher levels of smartphone SV, while other studies have found no meaningful association between mental health and SV among undergraduate students [6, 24]. Notably, the existing research has mainly focused on total SV, with limited research examining how different devices and the purposes for which they are used might influence this relationship. One study reported that the relationship between SV and mental health is more pronounced for computer and mobile phone use than for television viewing [1]. A possible explanation is that television is passive and mainly viewed for recreational purposes, whereas mobile technologies are interactive or interpersonal and mainly used for various academic activities and social communication [25]. However, none of the previous studies have specifically examined the associations between SV patterns and mental health among university students [24, 26, 27].
Investigating the specific impacts of device type and usage purpose on mental health is crucial, as different patterns of SV behavior may have different impacts on mental health [25, 28,29,30,31]. By distinguishing between beneficial, benign, and harmful screen device usage, we can develop more targeted interventions and strategies to improve the overall wellbeing of university students worldwide. Therefore, the present study aimed to provide a comprehensive understanding of SV patterns and their associations with mental wellbeing and psychological distress. This approach addresses the aforementioned research gap regarding the patterns of SV and their associations with mental health among university students, particularly concerning the types of devices used, the purposes of use, and the timing of use.
Methods
Participants and procedures
The Healthy Campus Initiative (HCI) cohort study is a four-year longitudinal study following first-year students at the National University of Singapore (NUS) through to completion of their undergraduate degree. This article focused on the baseline findings from the cohort study. Student recruitment and baseline data collection were conducted over six months between September 2021 and February 2022. When students participated in mandatory health checks as part of matriculation they were invited to participate in the study. Participation was voluntary and ethics approval was provided by the Departmental Ethics Review Committee (DERC) and the project approval number was SSHSPH137.
The study included participants who were first-year students in four-year degree programs at NUS and who declared that they intended to stay in Singapore for the duration of their studies. Participants who did not provide informed consent for participation and those who did not complete the survey were excluded from the study. The participant recruitment process is shown in Fig. 1. Project briefings were held one-to-one in person for approximately 15% (1084 students) of the total approached students. Written informed consent was obtained from each participant. The present analysis was based on 997 students who provided consent and valid baseline surveys.

Flow diagram for study participants
Assessment of screen viewing (SV) behavior
The questions were based on a screen time questionnaire and modeled on the domain-specific Adult Sedentary Behavior Questionnaire (ASBQ) [32]. Ten items assess the duration students spend on different devices, including TV, handheld or mobile devices (e.g. smartphones or tablets), and computers, on weekdays and weekend days. The purpose of screen viewing was determined as recreational or for study/work, respectively. All TV viewing time was categorized as recreational. For mobile phone and computer screen viewing, additional questions were asked to determine the amount of time spent on study and work. Ten screen viewing variables were derived and organized into four groups. The first group contained total screen viewing which was the average screen usage time per day. The second included two variables: study related screen viewing and recreational screen viewing per day. The third group included weekday screen viewing and weekend day screen viewing, and this referred to the average amount of SV per weekday or weekend day. The fourth was classified according to the device, including TV screen viewing, handheld or mobile device screen viewing, and computer screen viewing, and the average device usage time per day across different devices was derived. All SV variables were additionally categorized into low, medium, and high tertiles.
Assessment of mental wellbeing
The five-item World Health Organization Wellbeing Index (WHO-5) is a concise self-reported measure designed to evaluate current mental well-being. Comprising five items rated on a 6-point Likert scale, individuals were asked to reflect on their feelings over the past two weeks. The questions inquired about cheerfulness, calmness, activity levels, quality of sleep, and the presence of daily interests. Responses were scored from 0 to 5, and to obtain a percentage score ranging from 0 to 100, the raw score was multiplied by 4. Higher scores represented better mental wellbeing. WHO-5 scores > 50 were categorized as good mental wellbeing and those ≤ 50 were considered as poor mental wellbeing [33].
Assessment of psychological distress
The Kessler Psychological Distress Scale (K6) is a brief 6-item self-report inventory designed to assess psychological distress based on depressive and anxiety-related symptoms experienced over the past four weeks. The items included inquiries about the frequency of feeling nervous, hopeless, restless or fidgety, so depressed that nothing could cheer you up, that everything was an effort, and worthless. Participants rated their responses on a scale ranging from 0 (none of the time) to 4 (all the time). The total score ranged from 6 to 30, with higher scores representing greater psychological distress. K6 scores ≤ 13 were categorized as no psychological distress, and those > 13 were considered as psychological distress [34,35,36].
Covariates
Age, sex, citizenship, ethnicity, and faculty were collected using standard questionnaires. Citizenship was divided into Singaporean /Permanent Residents (PRs) and international expatriates. Ethnicity included Chinese and others. Faculty included four categories: 1) humanities and business, 2) science and engineering, 3) health sciences, and 4) others including interdisciplinary fields and faculties formed through collaborations between NUS and other universities. Monthly household income was categorized into groups: less than 3999 SGD, 4000 to 9999 SGD, more than 1,0000 SGD, and does not know/refuse to answer. Whether students worked part-time was also recorded. The height and weight of the participants were measured by a trained researcher using Smitech model DS-103 M stadiometer. Body mass index (BMI) was calculated by dividing weight in kilograms by the square of their height in meters. BMI categories were defined as underweight (< 18.5 kg/m2), normal (18.5–25.0 kg/m2), and overweight (≥ 25.0 kg/m2), providing insights into participants’ weight status [37]. Information on alcohol consumption and smoking status was categorized into “never” and “drinker”, and “never” and “smoker”, respectively.
The Singapore Prospective Study Physical Activity Questionnaire (SP2PAQ) was used to assess the frequency, duration, and intensity of domain-specific PA, including transportation, occupational, leisure, and household activity [38]. This information was used to calculate total time spent performing moderate-to-vigorous intensity physical activities (MVPA) per week. According to the World Health Organization (WHO), students who engaged in at least 150 min of MVPA per week were considered as having sufficient physical activity, and others were regarded as having insufficient physical activity [39]. One of the Pittsburgh Sleep Quality Index (PSQI) [40] was used to determine sleep duration. The question was, “During the past month, how many hours of actual sleep did you get at night? (This may be different than the number of hours you spent in bed.)”. A sleep duration less than 7 h was considered insufficient, and a sleep duration greater than or equal to 7 h was considered sufficient [41].
Statistical analysis
Frequencies and percentages were calculated for categorical variables, while means and standard deviations were determined for continuous variables. Screen viewing (the exposure variables) was analyzed both as categorical and continuous variables, while mental wellbeing and psychological distress (the outcome variables) were binary variables. According to previous literature, factors such as age and sex were identified as potential confounders [3, 20, 24, 26, 42, 43]. Age was treated as a continuous variable, while the remaining confounders were classified as categorical variables. 4% of participants with missing BMI data were imputed with the median. We utilized Student’s t-tests for continuous variables and chi-square tests for categorical variables to assess participants’ characteristics of outcome variables. Student’s t-tests were also conducted to examine sex differences in SV patterns. All sociodemographics, as well as variables significantly associated with outcome variables, were included in subsequent adjusted logistic regression analyses. Unadjusted and adjusted logistic regression models were developed to evaluate the relationships between SV and mental wellbeing or psychological distress. In the unadjusted analysis (Model 1), every single SV variable was included, followed by the inclusion of potential confounders in Model 2. Within distinct SV groups with varying purposes, devices, and timings, SV variables were mutually adjusted in Model 3. R version 4.2.2 was used to perform statistical analysis. Two-sided tests at the 5% level of significance were conducted, and effect sizes and 95% confidence intervals were reported for the respective outcomes.
Results
Sample characteristics
The average age of the 997 valid students was 20.2 years, with 59.6% being female and 41.4% male. Chinese represented 86.3% of the participants, and Singaporean/ Permanent Residents (PRs) accounted for 87.3%. A large percentage of students (48.0%) majored in science and engineering, followed by humanities and business (37.1%), health sciences (9.4%), and others (5.4%). Of the students surveyed, 20.0% had a monthly household income of less than SGD 4000, and 26.6% of students reported having a part-time job. Among the students, 15.1% were classified as underweight, while 11.3% were overweight. Alcohol consumption was reported by 40.2% of the students, and 3.0% reported smoking cigarettes. Additionally, 35.0% of the students engaged in insufficient physical activity, and 39.6% did not achieve adequate sleep. Regarding mental wellbeing, 33.6% of all students experienced poor wellbeing, and approximately 13.9% were identified as suffering from psychological distress (Table 1).
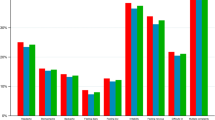
Average total SV of students was 14.3 h per day, and similar durations were reported for both weekdays and weekends (Table 2). On average, students engaged in 7.6 h of daily SV for study and 6 h for recreation. Among the different devices, computers were used the most for an average of 7.0 h per day and TV the least for an average of 1.7 h per day. Females consistently recorded higher SV than males (Fig. 2).

Forest plot of sex-specific screen viewing patterns among university students. *, p-value < 0.05; SD, standard deviation; CI, confidence interval. Error bars represented the 95% confidence interval, indicating the expected range of true differences. The blue reference line indicated a lack of statistical significance if the error bar crosses it
Associations of screen viewing with mental wellbeing
According to the fully adjusted models (Table 3), total SV was associated with mental wellbeing (Global p-value = 0.036). Compared to students with a low level of total SV, those with higher levels of total SV were more likely to have poor wellbeing [OR (95%CI): Medium: 1.54 (1.09, 2.18); High: 1.40 (0.99, 1.98)]. Models differentiated by the purposes of SV revealed a significant association between SV for recreation and wellbeing (Global p-value = 0.001), but not between study related SV. Compared to students with a low level of recreational SV, those with medium and high levels of recreational SV were more likely to have poor wellbeing [Medium: 1.71 (1.21, 2.42); High: 1.81 (1.27, 2.56)]. Device-specific analyses revealed that computer use was associated with mental wellbeing (Global p-value = 0.012), whereas such an association was not observed for TV and handheld device use. Compared to students with a low level of computer SV, those with medium and high levels of computer time were more likely to have poor wellbeing [Medium: 1.64 (1.17, 2.30); High: 1.44 (1.01, 2.06)]. Weekday and weekend day SV were not significantly associated with mental wellbeing.
Associations of screen viewing with psychological distress
In the fully adjusted models (Table 4), daily total SV was associated with psychological distress (Global p-value = 0.010). Compared to students with a lower level of total SV, those with a higher level of total SV were more likely to have psychological distress [Medium: 0.79 (0.48, 1.30); High: 1.56 (1.00, 2.44)]. Furthermore, weekend SV was significantly associated with psychological distress (Global p-value = 0.040), whereas weekday SV showed no such association. Compared to students with a lower level of weekend SV, those with higher levels of weekend SV were more likely to have psychological distress [Medium: 1.24 (0.73, 2.10); High: 2.16 (1.17, 4.06)]. Models differentiated by the purposes of SV revealed a significant association between SV for study and psychological distress (Global p-value = 0.050), whereas no such association was found for recreational SV. Compared to students with a lower level of study related SV, those with higher levels of study related SV were more likely to have psychological distress [Medium: 1.26 (0.77, 2.07); High: 1.75 (1.11, 2.83)]. There was no significant association between the device-specific SV and psychological distress.
Discussion
This study is a comprehensive investigation of university students’ SV patterns across purposes, devices, and timing, and is the first to investigate the relationships between SV patterns and mental wellbeing and psychological distress in university students. Our study showed that university students exhibited very high levels of SV, with females reporting higher SV than males. While most of the SV was spent studying and using computers, students also engaged in a considerable amount of recreational SV and on mobile devices. Previous studies among university students, predominantly from Western countries reported lower SV levels, varying between 5.5 and 11.5 h per day [4,5,6,7,8,9,10,11], whereas students in the present study reported an average of more than 14 h per day. This notable difference could be attributable to the study being conducted during the post-COVID-19 era when online learning was a norm among university students; also, Singapore’s ambition to be a Smart Nation ensured widespread internet access and fostered electronic device use [14, 44]. Additionally, unlike earlier research focusing on specific device types, our study considered SV across multiple device types, reflecting the modern reality of college students’ electronic device use for communication and socialization, information retrieval, and other purposes [45]. Furthermore, studies have indicated that males tend to use screens more frequently than females across all age groups [46, 47], while female university students demonstrate a greater dependency on smartphones than males [24]. Our observations of higher SV in females may stem from differences in leisure preferences, social media usage habits, or study behaviors between different sexes [24]. Moreover, societal norms and expectations regarding technology use, as well as alternative behaviors, such as sports and exercise, could impact SV habits differently for males and females [47]. Further investigation into these factors is essential for a comprehensive understanding of sex differences in SV.
Another important finding of our study is that approximately one in three university students exhibited poor mental wellbeing, and approximately one in seven reported experiencing psychological distress. The mental health of college students is a significant public health concern. According to the World Health Organization’s (WHO) World Mental Health (WMH) Survey, three-quarters of mental illnesses appear before the age of 24, with one-fifth of college students testing positive for mental disorders in a 12-month evaluation [48]. A national mental health survey in Singapore showed that the median age of onset for mental disorders is 22 years, with the highest incidence occurring between the ages of 18 and 24 years [49], and the proportion of young adults with poor mental wellbeing and psychological distress has been gradually increasing in recent years [50]. Previous reviews have examined mental health issues among college students, with most studies being conducted in high-income Western countries [51, 52]. The methodology, assessment instruments, and cultural adaptation of measuring tools differ greatly between studies, which might influence comparability [53]. Furthermore, the prevalence of poor mental wellbeing in Singaporean adults before and during the COVID-19 pandemic was 8.4% and 8.7%, respectively, which is lower than what was reported in our study [54, 55]. It is important to note that our study collected data during the early post-COVID-19 period, and existing literature indicates that the COVID-19 pandemic has had a negative impact on student mental health, particularly in terms of distress [56, 57]. This may explain why poor mental wellbeing was reported to be higher in our study than in Singapore before the pandemic [56, 57].
Total SV in the present study was consistently associated with mental wellbeing and psychological distress, even after adjusting for potential confounders including physical activity and sleep duration. Previous research on the relationship between SV and mental health has yielded inconsistent findings [20, 23, 52]. While some studies have suggested that greater SV is more likely to be associated with higher odds of poor mental wellbeing or psychological distress [46, 58,59,60], others have found no association or even a potential benefit [20, 61, 62]. Notably, most of these studies focused on adolescents rather than university students and often defined high SV as four or five hours without investigating the role of average daily SV beyond 10 h. Therefore, the discrepant findings might be attributable to differences in the study population but also the greater amount of SV observed in our study population. Furthermore, previous studies did not adequately consider the influence of other health behaviors, such as physical activity and sleep, on this relationship. The associations between SV and mental health among university students are not as simple as commonly assumed [63]. Several studies suggest that high SV may displace health-enhancing activities, but individuals with exceptionally high SV might also adopt compensatory mechanisms, such as incorporating positive lifestyle factors like regular physical activity or sufficient sleep, which could mitigate the negative effects on their wellbeing [30, 62]. Our study addresses this complexity by examining the relationship between SV patterns and mental health among Asian university students, considering variables such as physical activity and sleep duration as potential confounders.
Our findings suggest that the relationship between SV and mental health in university students may be linked to the purpose of SV rather than just the duration of exposure [20, 62]. High recreational SV was related to poor mental wellbeing. Research among teenagers corroborates our findings reporting that nearly one-fifth of teenagers with greater recreational SV reported signs of depression [64]. The association between recreational SV and mental wellbeing is intertwined with other factors. For instance, the constant availability of smartphones may instill a perceived obligation to remain accessible at all times and increase social comparison, fostering feelings of stress, depression and loneliness [65, 66]. Additionally, intensive screen engagement may disrupt other fundamental behaviors such as eating, exercising, and sleeping, thereby affecting mental wellbeing [67]. High study related SV on the other hand was associated with increased psychological distress. Few previous studies on the associations between study related SV and mental health issues exist and their findings are inconclusive [62, 68]. The observed association could be explained, however, by the increased pressure and demands of university-level studies. The transition from high school to university introduces new challenges and stressors, such as adapting to a more rigorous academic environment, managing greater workloads, and facing heightened expectations for academic performance [16]. As a result, students may resort to prolonged screen use as a means of studying, completing assignments, or seeking information, inadvertently exacerbating psychological distress. Therefore, our findings shed light on the intricate relationship between SV patterns driven by academic obligations and their impact on mental health outcomes among university students during this pivotal transitional phase.
Furthermore, our study indicated that excessive SV on weekends increased the risk of psychological distress, while weekday SV showed no such association. This finding is relatively novel [69] and suggests the importance of comprehensively examining both weekday and weekend SV patterns. It could be hypothesized that individuals who engage in prolonged SV on weekends may have limited participation in interactive activities, such as face-to-face social interactions, outdoor exercises, and group gatherings, which could lead to a lack of social engagement and fewer opportunities to build social connections [19]. Additionally, excessive SV on weekends may lead to increased exposure to potentially distressing or anxiety-inducing content, such as negative news stories or social media posts. Constant exposure to such content can contribute to heightened feelings of stress, anxiety, and overall psychological distress [70]. These conclusions underscore the importance of investigating the effects of the purposes and timing of SV on mental health outcomes, providing strong evidence for further research.
With regard to the type of device, significant differences were observed, with most time spent on computers and smartphones, while TV usage was considerably lower. The associations between SV and mental health varied across these devices. Television SV showed no association with mental wellbeing or psychological distress. Past studies on television SV have produced inconsistent findings [20, 22, 58]. In our study, the limited television viewing among college students may have contributed to the lack of a statistically significant association with mental health. Conversely, high computer SV was found to be more strongly associated with poor mental wellbeing. While utilizing information and communication technology for appropriate reasons may have potential benefits, excessive internet use is more likely to induce stress and negatively impact mental health among young individuals [71]. Contemporary university students are increasingly inclined toward digital learning, with most of their studies being conducted through computers. This mode of learning may enrich the availability of learning resources and could be more convenient. However, it also brings about greater workloads and competition, potentially leading to poorer mental wellbeing [72]. Additionally, it has been reported that using computers might increase exposure to harmful messages and cyberbullying, while excessive social media scrolling has been linked to increased feelings of loneliness and depression, potentially explaining the impact of computer SV on mental health in our study [31]. However, our research revealed no association between mobile phone SV and mental health, nor did it identify any sex differences in the relationship between SV and mental health (results not shown). Previous studies have reported correlations between mobile device SV and mental health symptoms, particularly among girls, often attributed to social media usage [20, 62, 73]. However, it is important to note that individual variance exists, with youth experiencing different levels of loneliness based on their face-to-face social interaction levels when using social media [58]. Thus, our study’s finding of no association between handheld device SV and mental health may be attributed to students using their mobile phones for multiple purposes, such as social networking, gaming, news, and productivity [74]. This underscores the importance of future research to delve deeper into the content of media usage and explore potential indirect associations through mediation analysis.
This study comprehensively examines SV patterns among university students, marking the first investigation into their association with mental wellbeing and psychological distress across purposes, timings, and devices. However, several limitations should be noted. First, the data relied on self-reporting, which may have been influenced by social desirability or information bias. Second, we summarized SV across different devices, including TVs, handheld devices, and computers. This may lead to an overestimation of the total SV, as multiscreen use is possible. Third, despite the large sample size and collection of variables related to socioeconomic status, there was notable heterogeneity among participants across faculties, with health sciences students representing a significantly smaller proportion compared to other faculties. Fourth, as a cross-sectional study, causal relationships between SV and mental health could not be established. However, it is important to mention that this study is part of a four-year longitudinal study, and while only baseline data was utilized in this analysis, future results from this longitudinal study may further strengthen the evidence.
Conclusions
Our study represents a novel exploration to investigate the screen viewing patterns of university students and their associations with mental wellbeing and psychological distress within the less studied Asian population. Overall, SV among university students was quite high, as was the high prevalence of poor mental wellbeing and psychological distress. Our findings suggest that students who engaged in greater SV were more likely to have poor mental wellbeing and increased psychological distress, even after accounting for other key lifestyle behaviors. While greater recreational SV was associated with poorer wellbeing, greater study related SV was associated with psychological distress. Variations across different devices and timing were also noted. Our results thereby underscore the complexity of these relationships, considering the diverse purposes and content of SV. Future analyses of this longitudinal study and other similar investigations will help to further our understanding of the impact of screen viewing on mental health among university students. These findings can also have implications for public health practitioners, policymakers, and educators, guiding the development of interventions promoting healthy screen use and mental health for university students.
Data availability
All the data generated or analyzed during this study are included in this published article.
Abbreviations
- ASBQ:
-
Adult Sedentary Behavior Questionnaire
- CI:
-
Confidence Interval
- h/d:
-
Hours Per Day
- HCI:
-
Healthy Campus Initiative
- K6:
-
Kessler Psychological Distress Scale
- kg/m2 :
-
Kilogram Per Square Meter
- NUS:
-
National University of Singapore
- OR:
-
Odds Ratio
- PR:
-
Permanent Residents
- PSQI:
-
Pittsburgh Sleep Quality Index
- SD:
-
Standard Deviation
- SGD:
-
Singapore Dollar
- SP2PAQ:
-
Singapore Prospective Study Physical Activity Questionnaire
- SV:
-
Screen Viewing
- TV:
-
Television
- WHO:
-
World Health Organization
- WHO-5:
-
Five-item World Health Organization Wellbeing Index
- WMH:
-
World Mental Health
References
Kaye L, Orben A, Ellis D, Hunter S, Houghton S. The conceptual and methodological mayhem of screen time. Int J Environ Res Public Health. 2020;17(10):3661.
Jain S, Shrivastava S, Mathur A, Pathak D, Pathak A. Prevalence and determinants of excessive screen viewing time in children aged 3–15 years and its effects on Physical Activity, Sleep, Eye symptoms and headache. Int J Environ Res Public Health. 2023;20(4):3449.
Nakshine VS, Thute P, Khatib MN, Sarkar B. Increased screen time as a cause of declining Physical, Psychological Health, and sleep patterns: a Literary Review. Cureus 14(10):e30051.
Tang L, Rifas-Shiman SL, Field AE, Austin SB, Haines J. Self-reported total screen time and viewing modes are Associated with Body Dissatisfaction, Disordered Eating, and Cosmetic surgery intentions among young adults. Nutrients. 2022;14(10):2027.
Qin F, Song Y, Nassis GP, Zhao L, Dong Y, Zhao C, et al. Physical activity, screen time, and Emotional Well-Being during the 2019 Novel Coronavirus Outbreak in China. Int J Environ Res Public Health. 2020;17(14):5170.
Hodes LN, Thomas KGF. Smartphone screen time: inaccuracy of self-reports and influence of psychological and contextual factors. Comput Hum Behav. 2021;115:106616.
Bradley AHM, Howard AL. Stress and Mood associations with Smartphone Use in University students: a 12-Week longitudinal study. Clin Psychol Sci. 2023;11(5):921–41.
Bigot R, Crouette P, Daudey E. Condition de vie et aspirations des Français. In: CREDOC. 2013. https://www.credoc.fr/download/pdf/Rapp/R297.pdf. Accessed 23 Apr 2024.
Hodges N, Zhou E, Trevorrow T, Dietch J. 0023 screen time and insomnia symptoms in University students. Sleep. 2022;45(Suppl 1):A9–11.
Tan ST, Tan SS, Tan CX. Screen time-based sedentary behaviour, eating regulation and weight status of university students during the COVID-19 lockdown. Nutr Food Sci. 2021;52(2):281–91.
Pans M, González LM, Úbeda-Colomer J, Devís-Devís J. Screen time among Spanish university students with disabilities: a self-organizing maps analysis. BMC Public Health. 2019;19(1):995.
United Nations Conference on Trade and Development (UNCTAD). Digital Economy Report 2019: Value Creation and Capture: Implications for Developing Countries. 2019. https://unctad.org/en/PublicationsLibrary/der2019_en.pdf. Accessed 24 Apr 2024.
De-Sola Gutiérrez J, Rodríguez de Fonseca F, Rubio G. Cell-phone addiction: a review. Front Psychiatry. 2016;7:175.
Hossain I, Lim ZZ, Ng JJL, Koh WJ, Wong PS. Public attitudes towards mobile health in Singapore: a cross-sectional study. Mhealth. 2018;4:41.
Hernández-Torrano D, Ibrayeva L, Sparks J, Lim N, Clementi A, Almukhambetova A, et al. Mental Health and Well-Being of University students: a bibliometric mapping of the literature. Front Psychol. 2020;11:1226.
Worsley JD, Pennington A, Corcoran R. Supporting mental health and wellbeing of university and college students: a systematic review of review-level evidence of interventions. PLoS ONE. 2022;17(7):e0266725.
American College Health Association. American College Health Association-National College Health Assessment II: Reference Group Executive Summary Spring. 2019. Silver Spring, MD: American College Health Association; 2019. https://www.acha.org/documents/ncha/NCHA-II_SPRING_2019_US_REFERENCE_GROUP_EXECUTIVE_SUMMARY.pdf. Accessed 24 Apr 2024.
Sheldon E, Simmonds-Buckley M, Bone C, Mascarenhas T, Chan N, Wincott M, et al. Prevalence and risk factors for mental health problems in university undergraduate students: a systematic review with meta-analysis. J Affect Disord. 2021;287:282–92.
Bewick B, Koutsopoulou G, Miles J, Slaa E, Barkham M. Changes in undergraduate students’ psychological well-being as they progress through university. Stud High Educ. 2010;35(6):633–45.
Tang S, Werner-Seidler A, Torok M, Mackinnon AJ, Christensen H. The relationship between screen time and mental health in young people: a systematic review of longitudinal studies. Clin Psychol Rev. 2021;86:102021.
Stiglic N, Viner RM. Effects of screentime on the health and well-being of children and adolescents: a systematic review of reviews. BMJ Open. 2019;9(1):e023191.
Wang X, Li Y, Fan H. The associations between screen time-based sedentary behavior and depression: a systematic review and meta-analysis. BMC Public Health. 2019;19(1):1524.
Deyo A, Wallace J, Kidwell KM. Screen time and mental health in college students: time in nature as a protective factor. J Am Coll Health. 2023;0(0):1–8.
Alavi SS, Ghanizadeh M, Farahani M, Jannatifard F, Esmaili Alamuti S, Mohammadi MR. Addictive use of smartphones and Mental disorders in University students. Iran J Psychiatry. 2020;15(2):96–104.
Sweetser P, Johnson D, Ozdowska A, Wyeth P. Active versus Passive screen time for Young Children. AJEC. 2012;37(4):94–8.
Rosenthal SR, Zhou J, Booth ST. Association between mobile phone screen time and depressive symptoms among college students: a threshold effect. Hum Behav Emerg Tech. 2021;3(3):432–40.
Wu X, Tao S, Zhang Y, Zhang S, Tao F. Low physical activity and high screen time can increase the risks of Mental Health problems and poor Sleep Quality among Chinese College Students. PLoS ONE. 2015;10(3):e0119607.
Bernard JY, Padmapriya N, Chen B, Cai S, Tan KH, Yap F, et al. Predictors of screen viewing time in young Singaporean children: the GUSTO cohort. Int J Behav Nutr Phys Act. 2017;14(1):1–10.
Kamaleddine AN, Antar HA, Ali BTA, Hammoudi SF, Lee J, Lee T, et al. Effect of screen time on physical and Mental Health and Eating habits during COVID-19 Lockdown in Lebanon. Psychiatry Investig. 2022;19(3):220–8.
Biddle SJH, García Bengoechea E, Pedisic Z, Bennie J, Vergeer I, Wiesner G. Screen time, other sedentary behaviours, and obesity risk in adults: a review of reviews. Curr Obes Rep. 2017;6(2):134–47.
Khan A, Lee EY, Janssen I, Tremblay MS. Associations of Passive and active screen Time with Psychosomatic complaints of adolescents. Am J Prev Med. 2022;63(1):24–32.
Chu AHY, Ng SHX, Koh D, Müller-Riemenschneider F. Domain-specific adult sedentary Behaviour Questionnaire (ASBQ) and the GPAQ single-item question: a reliability and validity study in an Asian Population. Int J Environ Res Public Health. 2018;15(4):739.
Topp CW, Østergaard SD, Søndergaard S, Bech P. The WHO-5 well-being index: a systematic review of the literature. Psychother Psychosom. 2015;84(3):167–76.
Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey replication (NCS-R). JAMA. 2003;289(23):3095–105.
Kessler RC, Andrews G, Colpe LJ, Hiripi E, Mroczek DK, Normand SLT, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32(6):959–76.
Kessler RC, Green JG, Gruber MJ, Sampson NA, Bromet E, Cuitan M, et al. Screening for serious mental illness in the general population with the K6 screening scale: results from the WHO World Mental Health (WMH) survey initiative. Int J Methods Psychiatr Res. 2010;19(S1):4–22.
Centers for Disease Control and Prevention. All About Adult BMI. https://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html (2022). Accessed 16 Mar 2024.
Nang EEK, Gitau Ngunjiri SA, Wu Y, Salim A, Tai ES, Lee J, et al. Validity of the international physical activity questionnaire and the Singapore prospective study program physical activity questionnaire in a multiethnic urban Asian population. BMC Med Res Methodolregi. 2011;11(1):141.
World Health Organization - Regional Office for the Eastern Mediterranean. Promoting physical activity. http://www.emro.who.int/health-education/physical-activitiy/promoting-physical-activity/What-is-the-recommended-amount-of-exercise.html (2024). Accessed 23 Apr 2024.
Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213.
Hirshkowitz M, Whiton K, Albert SM, Alessi C, Bruni O, DonCarlos L, et al. National Sleep Foundation’s updated sleep duration recommendations: final report. Sleep Health. 2015;1(4):233–43.
Twenge JM, Farley E. Not all screen time is created equal: associations with mental health vary by activity and gender. Soc Psychiatry Psychiatr Epidemiol. 2021;56(2):207–17.
Gao X, Zhang J, Yang Y, Cao Z. Sedentary behavior, screen time and mental health of college students: a Meta-analysis. Zhonghua Liu Xing Bing Xue Za Zhi. 2023;44(3):477–85.
Sipahi E, Saayi Z. The world’s first Smart Nation vision: the case of Singapore. SCRD. 2024;8:41–58.
Mavaddat N, Sadler E, Lim L, Williams K, Warburton E, Kinmonth AL, et al. Perceptions of self-rated health among stroke survivors: a qualitative study in the United Kingdom. BMC Geriatr. 2018;18(1):81.
Kjellenberg K, Ekblom O, Ahlen J, Helgadóttir B, Nyberg G. Cross-sectional associations between physical activity pattern, sports participation, screen time and mental health in Swedish adolescents. BMJ Open. 2022;12(8):e061929.
Su W, Han X, Jin C, Yan Y, Potenza MN. Are males more likely to be addicted to the internet than females? A meta-analysis involving 34 global jurisdictions. Comput Hum Behav. 2019;99:86–100.
Auerbach RP, Alonso J, Axinn WG, Cuijpers P, Ebert DD, Green JG, et al. Mental disorders among college students in the WHO World Mental Health Surveys. Psychol Med. 2016;46(14):2955–70.
Vaingankar JA, Rekhi G, Subramaniam M, Abdin E, Chong SA. Age of onset of life-time mental disorders and treatment contact. Soc Psychiatry Psychiatr Epidemiol. 2013;48(5):835–43.
Spinazze PA, Kasteleyn MJ, Aardoom JJ, Car J, Chavannes NH. Cross-sectional Analysis of University Students’ Health using a Digitised Health Survey. Int J Environ Res Public Health. 2020;17(9):3009.
Pedrelli P, Nyer M, Yeung A, Zulauf C, Wilens T. College students: Mental Health problems and treatment considerations. Acad Psychiatry. 2015;39(5):503–11.
Campbell F, Blank L, Cantrell A, Baxter S, Blackmore C, Dixon J, et al. Factors that influence mental health of university and college students in the UK: a systematic review. BMC Public Health. 2022;22(1):1778.
Dessauvagie AS, Dang HM, Nguyen TAT, Groen G. Mental Health of University Students in Southeastern Asia: a systematic review. Asia Pac J Public Health. 2022;34(2–3):172–81.
Tian-Ci Quek T, Wai-San Tam W, Tran X, Zhang B, Zhang M, Su-Hui Ho Z. The global prevalence of anxiety among medical students: a Meta-analysis. Int J Environ Res Public Health. 2019;16(15):2735.
Ministry of Health. Singapore, Institute of Mental Health, Singapore. Covid-19 mental wellness taskforce report. https://www.moh.gov.sg/docs/librariesprovider5/covid-19-report/comwt-report.pdf (2020). Accessed 23 Apr 2024.
Cao W, Fang Z, Hou G, Han M, Xu X, Dong J, et al. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020;287:112934.
Sundarasen S, Chinna K, Kamaludin K, Nurunnabi M, Baloch GM, Khoshaim HB, et al. Psychological impact of COVID-19 and Lockdown among University students in Malaysia: implications and policy recommendations. Int J Environ Res Public Health. 2020;17(17):6206.
Twenge JM, Campbell WK. Associations between screen time and lower psychological well-being among children and adolescents: evidence from a population-based study. Prev Med Rep. 2018;12:271–83.
Babic MJ, Smith JJ, Morgan PJ, Eather N, Plotnikoff RC, Lubans DR. Longitudinal associations between changes in screen-time and mental health outcomes in adolescents. Ment Health Phys Act. 2017;12:124–31.
Orben A, Przybylski AK. The association between adolescent well-being and digital technology use. Nat Hum Behav. 2019;3(2):173–82.
Odgers C. Smartphones are bad for some teens, not all. Nature. 2018;554(7693):432–4.
Santos RMS, Mendes CG, Sen Bressani GY, de Alcantara Ventura S, de Almeida Nogueira YJ, de Miranda DM, et al. The associations between screen time and mental health in adolescents: a systematic review. BMC Psychol. 2023;11(1):127.
Parkes A, Sweeting H, Wight D, Henderson M. Do television and electronic games predict children’s psychosocial adjustment? Longitudinal research using the UK Millennium Cohort Study. Arch Dis Child. 2013;98(5):341–8.
Khan A, Burton NW. Is physical inactivity associated with depressive symptoms among adolescents with high screen time? Evidence from a developing country. Ment Health Phys Act. 2017;12:94–9.
Pedersen J, Rasmussen MGB, Sørensen SO, Mortensen SR, Olesen LG, Brage S, et al. Effects of limiting digital screen use on well-being, mood, and biomarkers of stress in adults. Npj Mental Health Res. 2022;1(1):1–10.
Thomée S, Dellve L, Härenstam A, Hagberg M. Perceived connections between information and communication technology use and mental symptoms among young adults - a qualitative study. BMC Public Health. 2010;10(1):66.
Afifi TD, Zamanzadeh N, Harrison K, Acevedo Callejas M, WIRED. The impact of media and technology use on stress (cortisol) and inflammation (interleukin IL-6) in fast paced families. Comput Hum Behav. 2018;81:265–73.
Yan H, Zhang R, Oniffrey TM, Chen G, Wang Y, Wu Y, et al. Associations among screen time and unhealthy behaviors, academic performance, and well-being in Chinese adolescents. Int J Environ Res Public Health. 2017;14(6):596.
Przybylski AK, Weinstein N. A large-scale test of the Goldilocks hypothesis: quantifying the relations between digital-screen use and the mental well-being of adolescents. Psychol Sci. 2017;28(2):204–15.
Tang CSkum, Koh YYW. Online social networking addiction among college students in Singapore: Comorbidity with behavioral addiction and affective disorder. Asian J Psychiatr. 2017;25:175–8.
Yu CC, Tou NX, Low JA. Internet Use and effects on Mental Well-being during the Lockdown phase of the COVID-19 pandemic in younger Versus older adults: observational cross-sectional study. JMIR Form Res. 2024;8:e46824.
Zink J, Belcher BR, Imm K, Leventhal AM. The relationship between screen-based sedentary behaviors and symptoms of depression and anxiety in youth: a systematic review of moderating variables. BMC Public Health. 2020;20(1):472.
Keles B, McCrae N, Grealish A. A systematic review: the influence of social media on depression, anxiety and psychological distress in adolescents. Int J Adolesc Youth. 2020;25(1):79–93.
Iyengar K, Mabrouk A, Jain VK, Venkatesan A, Vaishya R. Learning opportunities from COVID-19 and future effects on health care system. Diabetes Metab Syndr. 2020;14(5):943–6.
Acknowledgements
The authors thank the participants of the Healthy Campus Initiative study, staff involved in the data collection and management, and the Healthy Campus Initiative study group.
Funding
This study was supported by funding from the Singapore Ministry of Health Office of Healthcare Transformation and the National University of Singapore.
Author information
Authors and Affiliations
Contributions
LLTE, XHC, AET, Nicholas P, and FMR designed and led the Healthy Campus Initiative study; LLTE and NP collected the baseline data; CMY performed the statistical analysis with guidance from Natarajan P, BCT, and FMR; CMY drafted the manuscript; Natarajan P, BCT and FMR critically reviewed the manuscript; all authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Participation in this study was voluntary, and informed consent was obtained. Ethics approval was provided by the Departmental Ethics Review Committee (DERC), with the project approval number SSHSPH137.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, M., Padmapriya, N., Chua, X.H. et al. Screen viewing patterns and their association with mental wellbeing and psychological distress: a cross-sectional study amongst university students. BMC Public Health 24, 2097 (2024). https://doi.org/10.1186/s12889-024-19608-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19608-1