
Abstract
Background
Zhiguo ethnic groups, commonly known as “the directly-entering-socialism ethnic groups”, represent Chinese ethnic minorities who have undergone a unique social development trajectory by transforming directly from primitive societies to the socialist stage. In recent decades, significant lifestyle transformations have occurred among Zhiguo ethnic groups. Understanding their health lifestyles can play a strategic role in China’s pursuit of universal health coverage. This study aims to examine patterns of health-related lifestyle among Zhiguo ethnic groups and explore whether sociodemographic features and specific indicators related to health status are associated with particular classes.
Methods
A cross-sectional study was conducted in Yunnan Province, China, from July to December 2022. Stratified random sampling method was employed to recruit residents belonging to six Zhiguo ethnic groups aged between 15 and 64. Latent class analysis was performed to identify clusters of health-related behaviors within each ethnic group. Logistic regression was utilized to determine the predictors of health lifestyles.
Results
A total of 1,588 individuals from the Zhiguo ethnic groups participated in this study. Three latent classes representing prevalent health lifestyles among the Zhiguo ethnic groups were identified: “unhealthy lifestyle” (31.80%), “mixed lifestyle” (57.37%), and “healthy lifestyle” (10.83%). In the overall population, individuals belonging to the “healthy lifestyle” group exhibited a higher likelihood of being non-farmers (OR: 2.300, 95% CI: 1.347–3.927), women (OR: 21.459, 95% CI: 13.678–33.667), married individuals (OR: 1.897, 95% CI: 1.146–3.138), and those residing within a walking distance of less than 15 min from the nearest health facility (OR: 2.133, 95% CI: 1.415–3.215). Conversely, individuals in the age cohorts of 30–39 years (OR: 0.277, 95% CI: 0.137–0.558) and 40–49 years (OR: 0.471, 95% CI: 0.232–0.958) showed a decreased likelihood of adopting a healthy lifestyle.
Conclusions
A considerable proportion of the Zhiguo ethnic groups have not adopted healthy lifestyles. Targeted interventions aimed at improving health outcomes within these communities should prioritize addressing the clustering of unfavorable health behaviors, with particular emphasis on single male farmers aged 30–49, and expanding healthcare coverage for individuals residing more than 15 min away from accessible facilities.
Similar content being viewed by others

Background
Health lifestyle theory posits that health lifestyles emerge as patterns of health-related behaviors shaped by the choices individuals make within the context of their available life chances [1]. A healthy lifestyle encapsulates a comprehensive integration of behaviors, norms, identities, and discourse [2]. It includes, but is not limited to, proper dietary choices, abstaining from smoking, moderate alcohol consumption, and regular exercise. These health-related behaviors have been found to be significantly associated with morbidity and life expectancy [3,4,5,6]. In the context of China, certain health risk behaviors such as smoking, physical inactivity, and excessive alcohol consumption, have emerged as prominent contributors to the prevalence of multiple chronic conditions and premature mortality [7]. The high prevalence of these modifiable behaviors imposes a substantial burden on healthcare [8, 9]. Moreover, early exposure to an unhealthy lifestyle can have enduring effects throughout an individual’s lifespan, leading to adverse health outcomes later in life [10]. Therefore, it is crucial to identify and address modifiable unhealthy lifestyles with the aim of preventing the onset and slowing down the progression of chronic diseases. This objective remains pivotal within the field of public health.
Previous studies have indicated that health-related behaviors are influenced by a variety of factors, including individual risk factors and social determinants. Individual risk factors encompass a complex array of demographic, cultural, and economic elements, such as age [11, 12], ethnicity [11], marital status [13], and sex [12, 14]. Social determinants of health, such as domestic context [15], working conditions [16], place of residence [17], education [18], income [19], and health promotion policies [20], play a crucial role in shaping health and quality-of-life outcomes both within and beyond the household [21]. Governments worldwide have implemented measures targeting these social determinants of health to mitigate the severity and distribution of health disparities while enhancing healthcare delivery. While prevailing research has primarily focused on adolescents, older adults, and individuals with chronic ailments, there is a noticeable dearth of studies examining ethnic minority populations. A study conducted in US colleges found that minority people are more likely to engage in high-risk drinking behaviors due to ethnicity-related stress [22]. Correspondingly, another investigation in the UK revealed that lower levels of fruit and vegetable intake appeared among ethnic groups when compared to the White British population [23]. Additionally, findings from a survey carried out in China demonstrated that ethnic minority populations (e.g., Bai, Naxi, and Yi ethnicity), exhibit a higher prevalence of smoking compared to the Han ethnic majority [24].
The concept of the “Zhiguo Ethnic Groups,” also known as the “directly-entering-socialism ethnic groups,” emerged during the 1950s as a designation by the Chinese Government for a subset of ethnic minorities that have undergone a distinct trajectory of social development. During the establishment of the People’s Republic of China, these specific ethnic groups were still in an early stage of societal development. The Communist Party of China implemented specialized policies to facilitate their direct transition from primitive societies to socialism. As a result, eleven ethnic groups were officially recognized under this category: Wa, Pumi, Achang, Lisu, Lahu, Bulang, Jingpo, Nu, Jino, De’ang, and Drung people. These eleven ethnic minorities primarily inhabit remote areas within Yunnan Province in China where they have encountered significant poverty and resource shortages due to their geographical isolation and historical constraints [25,26,27].
In recent decades, significant lifestyle transformations have occurred among the Zhiguo ethnic groups due to poverty alleviation efforts implemented by the Chinese government [27]. However, despite their minority status and distinctive characteristics, there is a scarcity of comprehensive scientific investigations into their health lifestyles. Therefore, comprehending their health lifestyles and exploring approaches for promoting health can play a strategic role in China’s pursuit of universal health coverage and inclusivity within the Healthy China Initiative.
To maximize health benefits, engaging in multiple health behaviors is essential, as the effects of individual behaviors alone may be insufficient for exerting synergistic effects [28]. In recent years, researchers have shifted focus to the combining effects of multiple health-related behaviors, rather than single ones. Studies conducted in the United States [18, 29], Mauritius [30], and Australia [31, 32] have discovered unique patterns of health lifestyles among different populations, such as the “Problems of Violence” pattern, the “Problems of Violence, Alcohol, Tobacco, and Psychological Distress” pattern, and the Mixed Healthy/Unhealthy pattern. These distinct patterns are likely associated with specific health outcomes and may affect the effectiveness of various health promotion programs.
The present study aims to contribute to the growing body of literature by examining patterns of health lifestyles in Zhiguo ethnic groups. To achieve this, we employed Latent Class Analysis (LCA) to identify distinct classes of individuals exhibiting different patterns of engagement in six core health-related behaviors. Furthermore, we aim to explore whether sociodemographic features and specific indicators related to health status are associated with particular classes.
Methods
Sample size calculations
The sample size calculation was derived from the health-related behavior indicators reported in the 2018 National Report of Health Services Survey in China. These indicators include a smoking prevalence of 24.7%, alcohol consumption prevalence of 27.6%, physical activity rate of 49.9%, and health examination participation rate of 47.2%. Specifically, the smoking rate, which is the lowest among these behaviors, served as the basis for estimation, incorporating the following parameters: P = 0.247, δ = 0.0247, deff = 1, \({{\mu }_{\alpha }}\)=1.96. Using the formula: \(N = \frac{{\mu _\alpha ^2 \times P(1 - P)}}{{{\delta ^2}}} \times deff\), the minimum required number of residents was calculated to be at least 1171. Taking into account a dropout rate of 15%, the sample size was determined as 1,347.
Sample selection and data collection
A cross-sectional study was conducted in Yunnan Province, China, from July to December 2022. The population of Yunnan Province, as reported in the seventh national census, was 47,209,277 in 2020, with 15,636,032 individuals (33.12%) belonging to ethnic minorities [33]. In this province, there are 26 indigenous ethnic groups, of which 11 have been officially recognized as Zhiguo ethnic groups.
A stratified random sampling method was adopted to select participants from six villages in Yunnan. Firstly, 16 prefectures in Yunnan were stratified into three clusters based on their geographic location, per capita GDP, and minority population. Three prefectures were then randomly selected from each cluster. Subsequently, one county was chosen from each prefecture and two villages were further chosen from each county using random digits. Finally, with the collaboration of community health workers, participants who belonged to Zhiguo ethnic groups and were aged between 15 and 64 were randomly enrolled in the study. Well-trained interviewers conducted face-to-face interviews using a structured questionnaire. Participants who had resided locally for less than three months, those who had impaired communication abilities, and those who were reluctant to collaborate with the interviewers were excluded from the study. In total, 1,588 respondents were included in the final analysis after excluding 33 individuals for missing data in the health lifestyle survey.
Variables
Socioeconomic status
Socioeconomic status was assessed as an independent variable in this study using a three-factor approach, encompassing educational attainment, monthly household income, and occupation. Educational attainment was evaluated on a two-point ordinal scale, including categories of junior high school or below and senior high school or above. Monthly household income was rated on a three-point scale: 1 denoting under 3,000 RMB, 2 representing 3,000–6,999 RMB, and 3 indicating 7,000 RMB and above. Occupations were categorized into two distinct groups: farmers and non-farmers.
Demographic characteristics
The demographic characteristics examined in this study included ethnicity, sex, marital status, and age. Ethnicity was determined based on self-identified ethnic classification. This study specifically focused on the Zhiguo ethnic groups residing in Yunnan Province. Within this context, we specifically investigated six major groups from the 11 Zhiguo ethnic minorities: Wa, Lisu, Nu, Jino, Lahu, and Bulang individuals. Sex was assessed as a binary variable while age was categorized into ordinal groups: 15–29 years, 30–39 years, 40–49 years, 50–59 years, and 60 years and older. Marital status was classified into two categories: married and unmarried (i.e., widowed, never married, and divorced).
Indicators related to health status
The study measured several health-related indicators to compare the defined clusters of health lifestyles among Zhiguo ethnic groups. These variables included self-reported chronic disease, health literacy, and travel time on foot to the nearest health facility. Health literacy was evaluated using the Brief Health Literacy Screen (BHLS), a verbally administered survey consisting of three questions [34]. The BHLS scale ranged from 3 to 15, with higher scores indicating greater levels of health literacy. A score ≦ 9 indicated low health literacy, while a score > 9 indicated adequate health literacy [35]. In this study, chronic diseases refer to noncommunicable diseases primarily encompassing cardiovascular diseases, cancers, chronic respiratory diseases, metabolic disorders, and similar conditions. The self-reported history of chronic disease diagnosed by a medical professional was categorized as either present or absent. Travel time on foot to the nearest health facility was reported in two categories: ≦15 min and > 15 min.
Health-related behaviors
The present study employed a cluster analysis approach to identify and classify five health-related behaviors, namely smoking status, physical activity, sleep duration, alcohol consumption, health examination participation, and BMI categories. These behaviors were derived from a comprehensive review of prior research and evidence-based practices [29, 36]. To better characterize the typological attributes of healthy or unhealthy behaviors predominant within the Zhiguo ethnic group, health-related behavior variables were dichotomized as follows: “0” indicated less healthy behaviors, and “1” represented more positive behaviors.
-
(i) Smoking status
Participants were inquired regarding their tobacco use within the past 30 days. Subsequently, responses were categorized into two distinct groups: current smokers, defined as individuals who consumed tobacco products either on a daily basis or less frequently, and non-smokers, encompassing those who did not report current use of any tobacco products, including both never-smokers and former smokers [37].
-
(ii) Physical activity
Physical activity is quantified by examining both the frequency and duration of exercise undertaken by individuals within a specific time frame. In this study, physical activity was operationalized as engaging in physical exercise exceeding three times per week, with each session lasting a minimum of thirty minutes [38, 39]. Based on this operational definition, participants were classified into two groups for the physical activity analysis: physically active (engaging in regular physical activity) and physically inactive (not participating in physical activity on a weekly basis).
-
(iii) Sleep duration
The sleep duration was determined by assessing the habitual nightly sleep hours reported by the respondents. This metric is widely recognized for its simplicity in comprehending, recalling, and recording sleep quality, rendering it well-suited for investigating the sleep patterns of diverse demographic groups [36, 40]. In this study, sleep duration was dichotomized into moderate sleep duration, defined as seven to nine hours per night, and non-optimal sleep duration, characterized by less than seven hours or more than nine hours per night [41].
-
(iv) Alcohol consumption
Based on the national guideline of Residents Nutrition and Health Monitoring survey in China [42], alcohol consumption was assessed by dividing respondents into “drinkers” (who reported any alcohol use in the past year) and “non-drinkers” (who did not).
-
(v) Health examination participation
Health examination participation was evaluated by categorizing respondents into two groups: those who had undergone health screenings in the past 12 months and those who had not .
-
(vi) BMI categories
BMI categories were determined based on participants’ self-reported measurements of height and weight. According to the WHO classification for the Asian population, BMI was stratified as follows: underweight (< 18.5 kg/m2), normal weight (18.5–22.9 kg/m2), and overweight or obesity (> 23 kg/m2).
The appendix presents the initial inquiries along with their respective frequencies for the six health lifestyle variables.
Statistical strategy
We utilized Mplus8.0, a statistical modeling software designed to facilitate the sequential execution of multiple models, to perform LCA for probabilistic classification of individuals into distinct and mutually exclusive latent subgroups based on six health-related behavior variables. The primary objective of this analysis was to maximize the similarity of health-related behavior combinations within each class. Additionally, each case was assigned a probability of belonging to a specific class.
Initially, we employed a parsimonious class model and iteratively refined it by fitting additional models with increasing numbers of classes. Ultimately, the number of classes was determined using commonly employed fit indices such as Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), adjusted Bayesian Information Criterion (aBIC), and entropy values. Entropy values, ranging from 0 to 1, indicate the accuracy of categorical classification, with higher values suggesting greater accuracy. An entropy value of ≧ 0.80 suggests 90% accuracy in category classification [43]. Lower AIC, BIC, and aBIC values imply better model fit [44].
Furthermore, the model fit was assessed by comparing the k class model to the k-1 class model using Lo-Mendell Rubin (LMR) and Bootstrap Likelihood Ratio Test (BLRT). A statistically significant p-value in the LMR and BLRT suggests that the k class model has a better fit than the k-1 class model [45].
Our study sought to meticulously delineate the patterns of health behaviors prevalent among individuals belonging to the six Zhiguo ethnic groups. While the precise quantity and configuration of health behavior typologies within this population remain unknown, we strive to strike a balance between the interpretability of findings and avoidance of excessive categorization. Thus, we concurrently considered the pragmatic implications of our findings and objective measures of model fit to determine the optimal delineation of classes. Following the identification of distinct clusters within various minority populations through LCA analysis, we proceeded to employ logistic regression in Stata as a subsequent step to examine the influence of sociodemographic features and specific health-related indicators on health lifestyles across different Zhiguo ethnic groups. We calculated Odd Ratio (OR) and their corresponding 95% Confidence Interval (CI) to evaluate the risk factors associated with specific latent classes of health behavior. Statistical significance was determined at a level of P < 0.05.
Results
Sociodemographic characteristics and health status of participants
Among the 1,588 participants surveyed, a diverse representation of Zhiguo ethnic groups was observed, with an even distribution among Wa (16.12%), Lisu (15.93%), Nu (17.19%), Jino (21.16%), Lahu (15.18%), and Bulang people (14.42%). The sex ratio reflected a slight predominance of women, with a male-to-female ratio of 1:1.05. The participants had an average age 41.75 years (SD = 13.84), and the majority were married (70.15%). In terms of socioeconomic status, a significant portion of the participants had attained junior school education or below (84.89%), identified as farmers (74.56%) and reported a monthly income below 3,000 RMB ($465 USD) (55.10%).
In terms of health-related characteristics, more than half the participants had a low health literacy level (51.89%). A significant proportion could access the nearest health facility within a 15-minute walk (55.29%), and nearly one-third reported the presence chronic disease (30.92%). Further details on sociodemographic and health status-related characteristics of the six ethnic groups were aggregated and presented in Table 1.
Characteristics of health-related behaviors
Based on the survey conducted among respondents from the six Zhiguo ethnic groups, the findings revealed a smoking prevalence of 31.80% in the population. Moreover, the survey revealed an alcohol consumption prevalence of 37.41%, with 65.49% of individuals undergoing regular physical examinations. The proportion of the surveyed population actively engaged in regular physical activity was noted at 25.44%. Additionally, 55.92% reported a moderate sleep duration, while 40.37% had a normal weight.
Table 2 presents the distribution of health-related behaviors among individuals from different Zhiguo ethnic groups. Substantial variations were observed across ethnic groups regarding physical activity, alcohol consumption, BMI categories and physical examination practices. However, no significant difference was found in smoking prevalence and sleep duration across these groups. Compared to participants from Wa, Jino, and Bulang ethnicities, a higher proportion of Lisu and Nu people reported complete abstinence from alcohol consumption. Furthermore, a lower percentage of Bulang participants reported undergoing physical examinations, being underweight or overweight, and engaging in physical activity compared to other ethnic groups.
Classes of clustered health-related behaviors
Using the LCA method, we identified four distinct profiles of health-related behaviors. The identification of these profiles was based on rigorous numerical measures of model fit, as outlined in Table 3. Results from the LMR and BLRT tests suggested that the three-class model provided superior fit to the survey data compared to the two-class model, with an entropy value of 0.873 signifying excellent separation between classes. Although AIC, BIC, and aBIC values were similar for both models, only the three-class model revealed a qualitatively distinct class absent in the two-class model. In light of both statistical fitness and pragmatic considerations, we concluded that the three-class model was parsimonious and substantively robust.
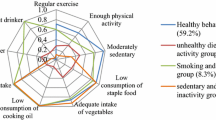
Based on the three-class model, item probabilities for the three identified latent classes were estimated, and their proportions in the sample were depicted in Fig. 1. Class 1, consisting of 10.83% of all respondents, emerged as a “group with healthy lifestyle”. This group exhibited the highest prevalence of physical activity engagement (100%) and adherence to physical examination (87.9%), along with a low probability of smoking (11.4%) and alcohol consumption (15.7%). Class 2, representing the largest cluster with 57.4% of all respondents, was defined as a “group with mixed lifestyle”. Individuals in this cluster predominantly abstained from smoking and alcohol (100.0% and 75.3%, respectively) and displayed relatively high rates of physical examinations participation (64.0%) and physical inactivity (85.4%). Class 3, comprising 31.80% of the total sample, was characterized as a “group with an unhealthy lifestyle”. Participants in this class showed a relatively low likelihood of engaging in physical activity (21.7%), undergoing physical examination (61.0%), and maintaining a moderate sleep duration (55.0%). They exhibited the highest probability of smoking (100%) and alcohol consumption (69.1%).

Item-response probabilities for health lifestyle indicators and participant distribution of the latent class of health lifestyle
Classes of health lifestyle across ethnically diverse population groups
Figure 2 depicts the classes of health lifestyle across the six ethnic populations. A chi-square test revealed significant differences in the distribution of clustered health lifestyle categories (χ2 = 56.226, P < 0.001). For instance, proportion of individuals in the Bulang people who belonged to the “healthy lifestyle” group was only 4.37%, which was significantly lower than the 20.55% observed in the Lisu people. Moreover, the “unhealthy lifestyle” had a higher proportion in the Jino people (35.42%) than in the Lahu people (25.31%).

Classes of health lifestyles across six ethnic groups
Logistic regression of latent class of health lifestyle across six ethnic groups
The results of logistic regression analysis are presented in Table 4, with the “unhealthy lifestyle” group serving as the reference group against which the “healthy lifestyle” group is compared. In the overall population, individuals belonging to the “healthy lifestyle” group exhibited a higher probability of being non-farmers (OR: 2.300, 95% CI: 1.347–3.927), women (OR: 21.459, 95% CI: 13.678–33.667), married (OR: 1.897, 95% CI: 1.146–3.138) and proximity to a health facility within a 15-minute walk (OR: 2.133, 95% CI: 1.415–3.215). Conversely, in comparison with individuals aged 15–29, those aged 30–39 (OR: 0.277, 95% CI: 0.137–0.558) and 40–49 (OR: 0.471, 95% CI: 0.232–0.958) showed a lower odds of adopting a healthy lifestyle.
Among all six Zhiguo ethnic groups, men were more likely to be associated to the “unhealthy lifestyle” group. Except for Jino and Lahu ethnicities, no significant associations were observed between socioeconomic status, health literacy and individuals’ preferences. Ethnic disparities were evident in terms of factors influencing health lifestyles; for instance, among the Nu ethnic group, individuals without chronic diseases exhibited a lower propensity for embracing a healthy lifestyle (OR: 0.308, 95% CI: 0.106–0.895).
Discussion
Describing health-related behaviors as clusters rather than individual practices provides valuable insights into the coexistence of positive and negative health behaviors among individuals, rather than exclusive adoption of one behavior over the other [18]. The presence of both healthy and unhealthy behaviors can be elucidated by Compensatory Health Beliefs (CHBs), which demonstrate that engaging in certain healthy behaviors can counterbalance or “neutralize” the negative impacts of unhealthy behaviors [46, 47].
In our study, we focused on six Zhiguo ethnic groups to identify six health-related behaviors by categorizing the population into three distinct clusters. By incorporating both health-promoting and health-compromising behaviors in our typologies, we could differentiate between individuals actively pursuing good health and those simply avoiding unhealthy behaviors. Furthermore, we explored the associations between these typologies and key demographic characteristics, health status indicators, as well as socioeconomic status, thereby shedding light on the relationship between these factors and distinct patterns of health lifestyles.
The study identified three latent classes denoting prevalent health lifestyles among the Zhiguo ethnic groups: Class 1, characterized by a “healthy lifestyle” (10.83% of the total sample); Class 2, characterized by a “mixed lifestyle” (57.37% of the total sample); and Class 3, characterized by an “unhealthy lifestyle” (31.80% of the total sample). The prevalence distributions across these three latent classes indicated a predominant representation of individuals adhereing to unhealthy or mixed lifestyles (90% of the studied sample), with a small proportion (10%) demonstrating consistently healthy lifestyles. These findings underscore limited health-promoting practices among Zhiguo ethnic groups.
Further analysis was conducted to delve into the factors influencing the health lifestyle of Zhiguo ethnic groups. Logistic regression revealed that sex is a significant factor shaping the health lifestyle choices of all six ethnic groups. Among Zhiguo ethnic groups, women exhibited a heightened propensity, ranging from 13 to 80 times more likely than men, to choose healthy lifestyles. This trend aligns with previous research indicating lower rates of hazardous drinking and tobacco smoking but higher rates of physical inactivity among women [48]. Several potential explanations for this sex disparity have been proposed, including societal norms mandating men to maintain their socialization and masculinity, thereby fostering increased rates of smoking and alcohol consumption [49, 50]. It is evident that future efforts should prioritize tailored interventions targeting men through health education initiatives and advocacy campaigns focused on tobacco control and alcohol restriction.
It is noteworthy that within the Zhiguo ethnic groups, there appears to be a decreased inclination among middle-aged and young adults to engage in health-promoting behaviors. Concurrently with societal progress, there has been a notable shift in the leading causes of mortality among Zhiguo ethnic groups, with chronic non-communicable diseases emerging as the predominant contributors [51]. To advance preventive strategies effectively, it is imperative to prioritize interventions aimed at promoting healthy lifestyle specifically targeting middle-aged adults. This targeted approach plays a crucial role in early mitigating and managing the prevalence and impact of chronic diseases [52].
The logistic regression analysis results suggest that travel time on foot to the nearest health facility may serve as a significant determinant influencing individuals’ health lifestyle choices, as observed across different populations. Individuals residing in remote areas with restricted access to healthcare facilities may be susceptible to a lack of awareness regarding lifestyle modifications and the promotion of healthy behaviors due to the absence of effective nudging mechanisms [53]. To effectively address these challenges, the Healthy China Initiative is committed to enhancing the functionality of primary healthcare service networks and optimizing the allocation of healthcare resources, particularly focusing on western regions and underserved areas. Moving forward, strategies such as improving healthcare accessibility, implementing telemedicine technologies, and establishing community-based health education programs are imperative. These efforts seek to empower individuals residing in remote regions by enabling them to make informed decisions while embracing health-conscious lifestyles.
In contrast to previous studies that have underscored the importance of socioeconomic factors, such as education, income and occupation [54, 55], our study discerns no substantial correlation between these variables and health lifestyle among the majority of Zhiguo ethnic groups. This disparity in findings may be attributed to the relatively equal distribution of socioeconomic status within the surveyed ethnic groups, resulting in limited health disparities within the population. Therefore, our study suggests that in populations with minimal variation in socioeconomic status, the impact of socioeconomic factors on health outcomes may not be as pronounced. Consequently, interventions targeting health-related lifestyle necessitate consideration of alternative contributing factors.
Our analysis highlights the significance of ethnic identity in shaping “behavioral niches“ [29]. The diverse cultures and habits among ethnic groups in our study underscore the pivotal role of ethnic identity as a potent determinant of behavior patterns. Using chi-square tests, we discerned substantial variations in health lifestyle profiles among different ethnic groups. These findings are consistent with previous research, exemplified by a study conducted in Hubei province, China, which reported statistically significant differences in the prevalence of health behaviors between Han Chinese and ethnic minority residents [56]. While no significant differences were found in the conditional probability distributions of smoking and moderate sleep duration among the Zhiguo ethnic group, notable disparities emerged regarding physical activity, alcohol consumption, BMI categories and physical examination domains. These discrepancies indicate that these four behaviors serve as primary determinants of health lifestyle clusters within ethnic minorities. Cultural customs and the environmental factors associated with generations-long residence can be attributed to these differences. For instance, higher rates of alcohol consumption among the Wa, Jino, and Bulang ethnic groups may be imputed to cultural norms that perceive alcohol as a crucial facilitator for social interaction [57, 58]. Conversely, adherence to religious rules among Lisu and Nu inhabitants has led to moderated smoking and drinking behavior, resulting in lower incidences of excessive alcohol intake [59, 60]. Additionally, worth noting is that limited access to medical resources faced by the Bulang ethnic group residing in remote mountainous regions for generations impedes their engagement in health promotion activities like physical examinations [61, 62]. Geographical barriers, coupled with relatively lower income, may further hinder their adoption of preventive behaviors.
As intercultural contact continues to evolve, Zhiguo ethnic groups may face a dual challenge in lifestyles choices as they navigate the balance between preserving traditional cultural customs and engaging in modern social movements. For instance, the health lifestyle preferences of Nu people are influenced by the presence or absence of chronic diseases. Therefore, targeted preventative interventions should be implemented in these ethnic groups, prioritizing initiatives aimed at modifying harmful pre-existing habits (e.g., excessive alcohol consumption and smoking [63, 64]) and mitigating the negative effects of contemporary unhealthy behaviors (e.g., sedentary behavior, late-night activities, and excessive reliance on electronic devices [65, 66]).
This study focuses on investigate the health lifestyles of Zhiguo ethnic groups residing in rural areas of Yunnan Province, China. By offering crucial empirical insights, it contributes to the advancement of health research within these distinct demographic segments. The implications derived from our findings can be extrapolated to similar contexts characterized by a convergence of diverse ethnic minority populations and resource-constrained communities. Several constraints merit acknowledgment in our study. Firstly, we only examined 6 out of the 11 Zhiguo ethnic minority groups. Thus, it is recommended to conduct further investigations on the remaining ethnic groups to mitigate potential selection bias and ensure comprehensive representation. Secondly, our survey was predicated on self-reported data, rendering it susceptible to social desirability bias and recall distortion. Thirdly, the use of LCA requires categorical indicators for class identification. It is noteworthy that dichotomizing health-related behavioral variables might influence the emergence of latent classes. Fourthly, our study did not investigate the specific pathways through which ethnicity exerts influence on health lifestyles. However, our findings contribute significantly to elucidating the manner in which ethnic identity shapes health behaviors, thereby emphasizing the necessity for targeted interventions aimed at addressing health disparities among diverse ethnic groups. Future research can explore how ethnicity influences the clustering of health-related behaviors, thus providing a more nuanced understanding of the specific mechanisms through which ethnicity impacts health lifestyles. Finally, additional variables such as dietary habits can be pertinent to consider, as they constitute integral components of health-related behaviors. Incorporating such variables will facilitate the formulation of more effective interventions to improve the health lifestyles among diverse ethnic groups and reduce health disparities. Such efforts are crucial for achieving optimal health outcomes across diverse demographic strata.
Conclusions
The present study demonstrates distinct clustering patterns of health-related behavior within the Zhiguo ethnic groups, indicating a substantial proportion of this population has not embraced healthy lifestyles. Targeted interventions aimed at improving health outcomes within the Zhiguo ethnic communities should prioritize addressing the clustering phenomenon of unfavorable health behaviors, with particular emphasis on single male farmers aged 30–49, and expanding healthcare coverage for individuals residing more than 15-minute proximity to accessible healthcare facilities.
Data availability
Additional data not included in the manuscript can be obtained upon reasonable request to the corresponding author.
Abbreviations
- LCA:
-
Latent Class Analysis
- GDP:
-
Gross Domestic Product
- AIC:
-
Akaike Information Criterion
- BIC:
-
Bayesian Information Criterion
- aBIC:
-
Adjusted Bayesian information criterion
- LMR:
-
Lo-Mendell Rubin
- BLRT:
-
Bootstrap Likelihood Ratio Test
- OR:
-
Odd Ratio
- CI:
-
Confidence Interval
- SD:
-
Standard Deviation
- BHLS:
-
Brief Health Literacy Screen
- BMI:
-
Body Mass Index
- CHBs:
-
Compensatory Health Beliefs
References
Cockerham W, Rütten A, Abel T. Conceptualizing Contemporary Health lifestyles: moving Beyond Weber. Sociol Q. 1997;38(2):321–42.
Mollborn S, Modile A. Dedicated to being healthy: Young adults’ deployments of health-focused cultural capital. Soc Sci Med. 2022;293(114648). https://doi.org/10.1016/j.socscimed.2021.114648.
Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. JAMA. 2004;291(10):1238–45. https://doi.org/10.1001/jama.291.10.1238.
Johnson NB, Hayes LD, Brown K, Hoo EC, Ethier KA. CDC National Health Report: leading causes of morbidity and mortality and associated behavioral risk and protective factors–United States, 2005–2013. MMWR Supplements. 2014;63(4):3–27.
Reiner M, Niermann C, Jekauc D, Woll A. Long-term health benefits of physical activity–a systematic review of longitudinal studies. BMC Public Health. 2013;13:813. https://doi.org/10.1186/1471-2458-13-813.
Lawrence EM, Mollborn S, Hummer RA. Health lifestyles across the transition to adulthood: Implications for health. Social science & medicine (1982). 2017; 193:23–32. https://doi.org/10.1016/j.socscimed.2017.09.041
Thomas Craig KJ, Morgan LC, Chen CH, Michie S, Fusco N, Snowdon JL, Scheufele E, Gagliardi T, Sill S. Systematic review of context-aware digital behavior change interventions to improve health. Translational Behav Med. 2021;11(5):1037–48. https://doi.org/10.1093/tbm/ibaa099.
Kazibwe J, Tran PB, Annerstedt KS. The household financial burden of non-communicable diseases in low- and middle-income countries: a systematic review. Health Res Policy Syst. 2021;19(1):96. https://doi.org/10.1186/s12961-021-00732-y.
Gheorghe A, Griffiths U, Murphy A, Legido-Quigley H, Lamptey P, Perel P. The economic burden of cardiovascular disease and hypertension in low- and middle-income countries: a systematic review. BMC Public Health. 2018;18(1):975. https://doi.org/10.1186/s12889-018-5806-x.
Seabrook JA, Avison WR. Socioeconomic status and cumulative disadvantage processes across the life course: implications for health outcomes. Can Rev Sociol = Revue canadienne de sociologie. 2012;49(1):50–68. https://doi.org/10.1111/j.1755-618x.2011.01280.x.
Nudelman G, Yakubovich S. Patterns of health lifestyle behaviours: findings from a representative sample of Israel. BMC Public Health. 2022;22(1):2099. https://doi.org/10.1186/s12889-022-14535-5.
Duncan MJ, Oftedal S, Rebar AL, Murawski B, Short CE, Rayward AT, Vandelanotte C. Patterns of physical activity, sitting time, and sleep in Australian adults: a latent class analysis. Sleep Health. 2020;6(6):828–34. https://doi.org/10.1016/j.sleh.2020.04.006.
Wang X, Gao H, Xu H. Cluster analysis of unhealthy lifestyles among Elderly adults with prediabetes: a cross-sectional study in Rural China. Diabetes Therapy: Res Treat Educ Diabetes Relat Disorders. 2019;10(5):1935–48. https://doi.org/10.1007/s13300-019-00676-1.
Chen Y, Wang P, He Y, Jiang F, Liu H, Liu Y, Liu T, Tang YL, Zhu J. Gender differences in the association between lifestyle behaviors and mental health among psychiatrists in China. J Affect Disord. 2022;318:196–203. https://doi.org/10.1016/j.jad.2022.08.089.
Nasreddine L, Hwalla N, Saliba A, Akl C, Naja F. Prevalence and Correlates of Preschool Overweight and Obesity amidst the Nutrition Transition: findings from a National Cross-sectional Study in Lebanon. Nutrients. 2017;9(3). https://doi.org/10.3390/nu9030266.
Sigblad F, Savela M, Okenwa Emegwa L. Managers’ perceptions of factors affecting employees’ uptake of Workplace Health Promotion (WHP) offers. Front Public Health. 2020;8:145. https://doi.org/10.3389/fpubh.2020.00145.
McCormack L, Wey H, Meendering J, Specker B. Differences in physical activity and Diet patterns between non-rural and rural adults. Nutrients. 2018;10(11). https://doi.org/10.3390/nu10111601.
Skalamera J, Hummer RA. Educational attainment and the clustering of health-related behavior among U.S. young adults. Prev Med. 2016;84:83–9. https://doi.org/10.1016/j.ypmed.2015.12.011.
Gor B, Nepal VP, Dongardive R, Dorai VK, Pande M. Is Socioeconomic Advantage Associated with Positive Health Behaviors and Health outcomes among Asian indians? Health Serv Res Managerial Epidemiol. 2019;6(2333392819830371). https://doi.org/10.1177/2333392819830371.
Bae SG, Kim JY, Kim KY, Park SW, Bae J, Lee WK. Changes in dietary behavior among adolescents and their association with government nutrition policies in Korea, 2005–2009. Journal of preventive medicine and public health = Yebang. Uihakhoe Chi. 2012;45(1):47–59. https://doi.org/10.3961/jpmph.2012.45.1.47.
Schuh MR, Bush ML. Evaluating Equity Through the Social Determinants of Hearing Health. Ear and hearing. 2022; 43(Suppl 1):15s-22s. https://doi.org/10.1097/aud.0000000000001188
Pittman DM, Cho Kim S, Hunter CD, Obasi EM. The role of minority stress in second-generation black emerging adult college students’ high-risk drinking behaviors. Cult Divers Ethn Minor Psychol. 2017;23(3):445–55. https://doi.org/10.1037/cdp0000135.
Wang S, Li S. Exploring Generational Differences of British Ethnic Minorities in smoking behavior, frequency of Alcohol Consumption, and Dietary Style. Int J Environ Res Public Health. 2019;16(12). https://doi.org/10.3390/ijerph16122241.
Yang S, Liu S, Wang Y, Wan H, Zhao D, Li Y, Chen SS, Wu Y, Dustin L, Azen S, et al. High blood pressure in Chinese ethnic minorities: report from rural Yunnan Province. Am J Hypertens. 2011;24(11):1209–14. https://doi.org/10.1038/ajh.2011.127.
Cheng X. Social Development and modernization of the ‘Zhi Guo’ ethnic group in Yunnan. Kunming: Yunnan People’s Publishing House; 2002.
Jiang M, Xiong L, Yang M. The Backward and Foreword of the Development Research on Yunnan Border’s Zhiguo Nationality. Bord Econ Cult. 2011(01):171–3.
You W, Zeng Y. On the Development Drive of Minority Nationalities-A Study based on the poverty alleviation practice of directly-entering-socialism ethnic groups in Yunnan. Social Sci Yunnan. 2020(06):117–24.
Spring B, Moller AC, Coons MJ. Multiple health behaviours: overview and implications. Journal of public health (Oxford, England). 2012; 34 Suppl 1(Suppl 1):i3–10. https://doi.org/10.1093/pubmed/fdr111
Saint Onge JM, Krueger PM. Health Lifestyle behaviors among U.S. adults. SSM - Popul Health. 2017;3:89–98. https://doi.org/10.1016/j.ssmph.2016.12.009.
Hoogstoel F, Samadoulougou S, Lorant V, Kirakoya-Samadoulougou F. A latent class analysis of Health lifestyles in relation to suicidality among adolescents in Mauritius. Int J Environ Res Public Health. 2021;18(13). https://doi.org/10.3390/ijerph18136934.
Oftedal S, Vandelanotte C, Duncan MJ. Patterns of Diet, physical activity, sitting and Sleep are Associated with Socio-Demographic, behavioural, and Health-Risk indicators in adults. Int J Environ Res Public Health. 2019;16(13). https://doi.org/10.3390/ijerph16132375.
Rabel M, Laxy M, Thorand B, Peters A, Schwettmann L, Mess F. Clustering of Health-related behavior patterns and demographics. Results from the Population-based KORA S4/F4 cohort study. Front Public Health. 2018;6:387. https://doi.org/10.3389/fpubh.2018.00387.
Statistics YPBo. Yunnan statistical yearbook. In., edn.: China Statistics; 2022. p. 357.
Chew LD, Bradley KA, Boyko EJ. Brief questions to identify patients with inadequate health literacy. Fam Med. 2004;36(8):588–94.
Willens DE, Kripalani S, Schildcrout JS, Cawthon C, Wallston K, Mion LC, Davis C, Danciu I, Rothman RL, Roumie CL. Association of brief health literacy screening and blood pressure in primary care. J Health Communication. 2013;18(1):129–42. https://doi.org/10.1080/10810730.2013.825663.
Zhang L, Bi X, Ding Z. Health lifestyles and Chinese oldest-old’s subjective well-being-evidence from a latent class analysis. BMC Geriatr. 2021;21(1):206. https://doi.org/10.1186/s12877-021-02121-0.
Ghazali SM, Seman Z, Cheong KC, Hock LK, Manickam M, Kuay LK, Yusoff AF, Mustafa FI, Mustafa AN. Sociodemographic factors associated with multiple cardiovascular risk factors among Malaysian adults. BMC Public Health. 2015;15:68. https://doi.org/10.1186/s12889-015-1432-z.
Wang X, Li W, Song F, Wang L, Fu Q, Cao S, Gan Y, Zhang W, Yue W, Yan F, et al. Carotid atherosclerosis detected by Ultrasonography: A National Cross-sectional Study. J Am Heart Association. 2018;7(8). https://doi.org/10.1161/jaha.118.008701.
Wang A, Liu J, Li C, Gao J, Li X, Chen S, Wu S, Ding H, Fan H, Hou S. Cumulative exposure to high-sensitivity C-Reactive protein predicts the risk of Cardiovascular Disease. J Am Heart Association. 2017;6(10). https://doi.org/10.1161/jaha.117.005610.
Ahmad K, Keramat SA, Ormsby GM, Kabir E, Khanam R. Clustering of lifestyle and health behaviours in Australian adolescents and associations with obesity, self-rated health and quality of life. BMC Public Health. 2023;23(1):847. https://doi.org/10.1186/s12889-023-15724-6.
Hruby A, Manson JE, Qi L, Malik VS, Rimm EB, Sun Q, Willett WC, Hu FB. Determinants and consequences of obesity. Am J Public Health. 2016;106(9):1656–62. https://doi.org/10.2105/ajph.2016.303326.
Prevention CCfDCa,Chronic Disease and Nutrition Surveillance in Chinese Adults. (2018)-Workbook, (2020-10-21), [2024-05-26], https://ncncd.chinacdc.cn/jcysj/jcsj/202010/t20201021_222263.htm
Lubke G, Muthén BO. Performance of factor mixture models as a function of model size, Covariate effects, and class-specific parameters. Struct Equation Modeling: Multidisciplinary J. 2007;14(1):26–47. https://doi.org/10.1080/10705510709336735.
Lanza ST, Collins LM, Lemmon DR, Schafer JL. PROC LCA: a SAS Procedure for Latent Class Analysis. Structural equation modeling: a multidisciplinary journal. 2007; 14(4):671–94. https://doi.org/10.1080/10705510701575602
Li G, Liu J, Wen H, Shen Q. Changes in Depression among adolescents: a multiple-Group Latent Profile Transition Analysis. Psychol Res Behav Manage. 2023;16:319–32. https://doi.org/10.2147/prbm.S390116.
Cao XL, Wang SB, Zhong BL, Zhang L, Ungvari GS, Ng CH, Li L, Chiu HF, Lok GK, Lu JP, et al. The prevalence of insomnia in the general population in China: a meta-analysis. PLoS ONE. 2017;12(2):e0170772. https://doi.org/10.1371/journal.pone.0170772.
Rabia M, Knäuper B, Miquelon P. The eternal quest for optimal balance between maximizing pleasure and minimizing harm: the compensatory health beliefs model. Br J Health Psychol. 2006;11(Pt 1):139–53. https://doi.org/10.1348/135910705x52237.
Haug S, Schaub MP, Salis Gross C, John U, Meyer C. Predictors of hazardous drinking, tobacco smoking and physical inactivity in vocational school students. BMC Public Health. 2013;13:475. https://doi.org/10.1186/1471-2458-13-475.
Edwardson CL, Gorely T, Pearson N, Atkin A. Sources of activity-related social support and adolescents’ objectively measured after-school and weekend physical activity: gender and age differences. J Phys Act Health. 2013;10(8):1153–8. https://doi.org/10.1123/jpah.10.8.1153.
Xia L, Jiang F, Rakofsky J, Zhang Y, Zhang K, Liu T, Liu Y, Liu H, Tang YL, Cigarette, Smoking. Health-related behaviors, and Burnout among Mental Health professionals in China: a Nationwide Survey. Front Psychiatry. 2020;11:706. https://doi.org/10.3389/fpsyt.2020.00706.
Wu K, Tang X, Huang Y, Shi Q, Chen Y, Deng R. Analysis on the causes of death among ethnic groups with cross-stage development in Yunnan province,2015–2019. Chin Prev Med. 2021;22(12):920–5. https://doi.org/10.16506/j.1009-6639.2021.12.006.
Li Y, Schoufour J, Wang DD, Dhana K, Pan A, Liu X, Song M, Liu G, Shin HJ, Sun Q, et al. Healthy lifestyle and life expectancy free of cancer, cardiovascular disease, and type 2 diabetes: prospective cohort study. BMJ (Clinical Res ed). 2020;368:l6669. https://doi.org/10.1136/bmj.l6669.
Liu YL, Lu CW, Shi L, Liou YM, Lee LT, Huang KC. Low intensive lifestyle modification in young adults with metabolic syndrome a community-based interventional study in Taiwan. Medicine. 2015;94(22):e916. https://doi.org/10.1097/md.0000000000000916.
Xue Y, Lu J, Zheng X, Zhang J, Lin H, Qin Z, Zhang C. The relationship between socioeconomic status and depression among the older adults: the mediating role of health promoting lifestyle. J Affect Disord. 2021;285:22–8. https://doi.org/10.1016/j.jad.2021.01.085.
Allen L, Williams J, Townsend N, Mikkelsen B, Roberts N, Foster C, Wickramasinghe K. Socioeconomic status and non-communicable disease behavioural risk factors in low-income and lower-middle-income countries: a systematic review. Lancet Global Health. 2017;5(3):e277–89. https://doi.org/10.1016/s2214-109x(17)30058-x.
Huang R. Study on Lmproving Health Literacy of Rural Residents in ethnic areas under the healthy China Strategy——Based on the Survey from Enshi Autonomous Prefecture. J Cent China Normal University(Humanities Social Sciences). 2018;57(04):19–26.
Guo W, Xu X, Zhao X, Zhu K, Zhang Y. Alcoholism: a problem that should not be ignored in cultural change: a survey of alcohol consumption in ethnic minority areas. Ethnic Today. 2003;11:40–3.
H LJ, D ZX ZL, Y LP YZ. A study on Alcohol Consumption and Social Change among ethnic minorities in Yunnan. Shanghai Archives Psychiatry. 2010;22(S1):440–3.
Cui Y, Gao Z. Substitution or sublation:a study on the practice of the sinicization of christianity in the nusu people from the perspective of religious relations. Religious Stud. 2022(01):6–13.
Hei Y, Yang L. Localization and ethnic identity of christian faith in Lisu people. World Religious Cultures. 2016;01:23–7.
Zhang S, Liu J, Lo EC, Chu CH. Dental caries status of Bulang preschool children in Southwest China. BMC Oral Health. 2014;14:16. https://doi.org/10.1186/1472-6831-14-16.
Yap P, Du ZW, Chen R, Zhang LP, Wu FW, Wang J, Wang XZ, Zhou H, Zhou XN, Utzinger J, et al. Soil-transmitted helminth infections and physical fitness in school-aged Bulang children in southwest China: results from a cross-sectional survey. Parasites Vectors. 2012;5:50. https://doi.org/10.1186/1756-3305-5-50.
Luo XF, Duan S, Duan QX, Pu YC, Yang YC, Wong FY, He N. Prevalence and correlates of alcohol use and subsequent sexual activity among adult males in a rural community of ethnic minorities in Yunnan Province, China. Biosci Trends. 2012;6(6):288–95.
Cai L, Wang XM, Fan LM, Cui WL, Golden AR. Socioeconomic disparities in prevalence and behaviors of smoking in rural Southwest China. BMC Public Health. 2019;19(1):1117. https://doi.org/10.1186/s12889-019-7455-0.
Meng SQ, Cheng JL, Li YY, Yang XQ, Zheng JW, Chang XW, Shi Y, Chen Y, Lu L, Sun Y, et al. Global prevalence of digital addiction in general population: a systematic review and meta-analysis. Clin Psychol Rev. 2022;92:102128. https://doi.org/10.1016/j.cpr.2022.102128.
Anderson S, Currie CL, Copeland JL. Sedentary behavior among adults: the role of community belonging. Prev Med Rep. 2016;4:238–41. https://doi.org/10.1016/j.pmedr.2016.06.014.
Acknowledgements
We would like to acknowledge study participants, data collectors and all community workers operating within the designated survey area for their dedicated cooperation.
Funding
The study was funded by the Science and Technology Plan Project of Science and Technology Department of Yunnan Province (NO. 202201AY070001-024); Yunnan High-level Talent Support Plan (YNQR-QNRC-2018-140) and Provincial Talent Program for Young Scholar and Technical Reserve Personnel (202305AC160046).
Author information
Authors and Affiliations
Contributions
KW, JC, RD, and YH conceived the study and designed the protocols. CY, RD and YH supervised the study implementation and advised on the data analysis. JC, KW and XL contributed to the development of the questionnaire, data collection. JC analyzed the data. KW drafted the original manuscript. YX, RD, and YH revised the manuscript. All authors reviewed and approved the final manuscript. RD and YH are the guarantors of this study.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol was reviewed and approved by the Ethics Review Committee of Kunming Medical University (Approval NO. KMMU2021MEC095). Adhering to the ethical principle of voluntary participation, all prospective participants were provided with the autonomy to make an informed decision regarding their willingness to participate in the research. For minors, informed assent was duly obtained from their parents or legal guardians. All study subjects were explicitly informed of their right to withdraw from the study at any point without facing adverse consequences. To ensure transparency, participants received a comprehensive explanation of the study’s objectives and procedures before being requested to provide their informed consent through the signing of a consent form. During the data collection phase, personal identifying information, such as names and phone numbers, was deliberately omitted from the recorded data to ensure anonymity. Instead, numerical codes were assigned to each participant to facilitate data coding and organization securely. The collected information underwent proper coding procedures and remained strictly confidential throughout the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wu, K., Chen, J., Xiao, Y. et al. Health lifestyles of six Zhiguo ethnic groups in China: a latent class analysis. BMC Public Health 24, 2279 (2024). https://doi.org/10.1186/s12889-024-19743-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19743-9