
Abstract
Background
Maternal mortality (MM) remains a real scourge that hits hardest in the poorest regions of the world, particularly those affected by conflict. However, despite this worrying reality, few studies have been conducted about MM ratio in the Democratic Republic of Congo (DRC). The study aimed to describe the trends as well as the epidemiological profile and causes of reported institutional maternal deaths between 2013 and 2022 in Eastern DRC.
Methods
A retrospective descriptive study was conducted between March 2023 and August 2023 in eight Health Zones (HZ), five in South Kivu Province (Mwana, Minova, Miti-Murhesa, Kamituga and Idjwi) and three in North Kivu Province (Kirotshe, Karisimbi and Kayna) in the eastern region of the DRC. Our study covers 242 health facilities: 168 health centers (HC), 16 referral health centers (RHCs),50 referral hospitals (RH) and 8 general referral hospitals (GRHs). Data from registers and medical records of maternal deaths recorded in these zones from 2013–2022 were extracted along with information on the number of deliveries and live births. Sociodemographic, clinical parameters, blood and ultrasound tests and suspected causes of death between provinces were assessed.
Results
In total, we obtained 177 files on deceased women. Of these, 143 (80.8%) were retained for the present study, including 75 in the 3 HZs of North Kivu and 68 in the 5 HZs of South Kivu. From 2013 to 2022, study sites experienced two significant drops in maternal mortality ratio (MMR) (in 2015 and 2018), and a spike in 2016–2017. Nonetheless, the combined MMR (across study sites) started and ended the 10-year study period at approximately the same level (53 and 57 deaths per 100,000 live births in 2013 and 2022 respectively). Overall, 62,6% of the deaths were reported from secondary hospital. Most deaths were of married women in their thirties (93.5%). Almost half (47.8%) had not completed four antenatal consultations. The main direct causes of death were, in decreasing order of frequency: post-partum haemorrhage (55.2%), uterine rupture (14.0), hypertensive disorders (8.4%), abortion (7.7%) puerperal infections (2.8%) and placental abruption (0.7%). When comparing among provinces, reported abortion-related maternal mortality (14.1% vs 0%) was more frequent in North Kivu than in South Kivu.
Conclusion
This study imperatively highlights the need for targeted interventions to reduce maternal mortality. By emphasizing the crucial importance of antenatal consultations, intrapartum/immediate post-partum care and quality of care, significant progress can be made in guaranteeing maternal health and reducing many avoidable deaths.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
The Democratic Republic of Congo (DRC) is among the countries with the highest maternal mortality ratio (MMR) in the world. Over the past two decades, maternal mortality figures have fluctuated considerably. Between 2010 and 2015, the MMR continues to fluctuate without ever falling below the sustainable development targets. The MMR for 2020 was estimated at 547 with an uncertainty interval of 377 to 907, and the estimates for the years 2000, 2005, 2010, and 2015 all fall within this interval. The report indicates that the average annual rate of reduction is only 1.2% between 2000 and 2020 [1, 2].
After almost two decades of civil war, the DRC remains a complex humanitarian emergency, with devastated health infrastructures and a disrupted civil society [3]. The effects of the conflict on women's health and well-being are profound; the DRC is said to be one of the worst conflict zones for women and children in the world [4, 5]. The destruction of health infrastructure during the war has led to insufficient capacity to meet the health needs of the population and has resulted in poor health among refugees and internally displaced persons (IDPs) and avoidable deaths [3]. In addition, the DRC faces the challenge of low public funding for the health sector [6,7,8]. The North and South Kivu provinces in Eastern DRC have been prey to armed conflict for some twenty years. The region has been transformed into a zone of anarchy where civilians are pillaged, raped and killed by identified or informal armed groups. These two provinces are facing clashes between the Congolese army and elements of various armed groups. This has led to displacement of thousands of people and deterioration of the health care system, making it difficult for mothers and children to access health services. Furthermore, in these crisis-affected contexts, a large number of births and maternal death (MD) are not even documented. Overall, North Kivu has experienced a higher intensity of conflict than South Kivu [9,10,11].
In the light of the above, it is necessary to provide robust and reliable results that will inform subsequent efforts and strategies to develop or strengthen the Maternal, Perinatal Death Surveillance and Response (MPDSR) system in a crisis context, and particularly in the eastern region of the DRC affected by armed conflict and massive population displacement. Given persistently high MMR figure, it is imperative to assess its trend over the last decade in this region. However, despite this worrying reality, few studies have been carried out on this subject in the region to assess recent & current MMR and identify the main causes of death [12, 13]. The aim of this work was to describe the epidemiological profile and causes of institutional maternal deaths documented in health system records over the last ten years (2013–2022) in the North and South Kivu provinces in Eastern DRC.
Methods
Location and study design
Our study was carried out in the provinces of North and South Kivu in the east of the DRC. Study locations included all health facilities (general referral hospitals (GRH), referral hospitals (RH) referral health centers (RHC) and Health centers (HC) in three health zones (HZs) in the province of North Kivu (ZS of Kirotshe, Karisimbi and Kayna) and five in the province of South Kivu (Mwana, Minova, Miti-Murhesa, Kamituga and Idjwi). Study sites were chosen because of their geographical accessibility and relative stability compared to other areas heavily affected by armed conflict in the same provinces, as well as the fact that they were the areas where the “Direction du Développement et de la Coopération (DDC)”, the Swiss agency for development and international cooperation, our partner, provided funding for the study. A HZ is an administrative entity that represents the operational unit for planning and implementing health services in the DRC. It operates as a tiered system consisting of a network of health facilities, supervised by the Central Health Zone Office (CHZO), with increasing service capacity along a chain of referral. Health centers (HC) are first-line facilities dedicated to primary health care tasks grouped under the term minimum package of activities (curative, preventive, promotional and support activities) that are delegated to a team of multi-purpose nurses. This includes family planning, antenatal- and postnatal care, obstetric care (for normal deliveries), newborn care, child vaccination, integrated management of childhood illness, and treatment of severe acute malnutrition.In addition to this type of health facility, there are Health Posts and Dispensaries that offer a range of activities more or less similar to those of HC.All these health facilities refer cases that are beyond their means and competencies to a RHC or the RH (Secondary hospitals). These two last types of health facilities offer a larger broad of health activities, grouped under the term Complementary Package of Activities that covers internal medicine, hospitalization, surgical and reference services, in addition to technical support to health centres through integrated supervision.Thus, with regard to maternal and neonatal care, the HC, dispensaries and health posts offer Basic Emergency Obstetric and Newborn Care (BEmONC), while the RHC, RH, and GRH are intended to offer Comprehensive Emergency Obstetric and Newborn Care (CEmONCOur study covers 8 HZ with 242 health facilities: 168 health centres, 50 referral hospitals, 16 RHCs and 8 GRHs.
Type of study and Sampling
This was a retrospective record review of maternal deaths documented in health system records over the last ten years (2013–2022). Patient records and health facility registers were reviewed along with available maternal death audit reports. Data extracted on all reported maternal deaths that occurred from January 1, 2013 to December 31, 2022 were included in the analysis. Maternal deaths audits, available on the day of the survey in the CHZO and health facilities, were carried out to assess the epidemiological profile and causes of MM over the last ten years. Older registers and charts were obtained from central offices and more recent from facilities.
Data collection and outcomes
Data collection took place between March 2023 and August 2023. Four teams of three people carried out the data collection in the selected health zones. Data collection was facilitated using a standardized and piloted data extraction template (Facility Based Maternal Death Review form used in Eastern DRC). All medical records available on the day of the survey in the health facilities (gynaeco-obstetrics department) and in the CHZOs were extracted from registers and available patient files/audits. In each medical record of the deceased subjects, sociodemographic (age, level of education, and marital status) and clinical data (antenatal care (ANC) visits, maternal weight, obstetric history of the mother, reason of delivery admission, length of hospitalization, method of delivery, blood (complete blood count, serological test and blood typing) and ultra sound testing and cause of death were included in the present study. Files that did not contain data on key variables, such as age, prenatal visits, obstetric formula, mode of delivery, and causes of death, were excluded. Maternal deaths were classified into two categories based on the causes reported in the records by a qualified physician who was part of the data collection team: (i) Deaths due to direct causes: these were deaths resulting from obstetric complications (pregnancy, labour and the post-natal period) as well as interventions, omissions, incorrect treatment or a chain of events resulting from one of the above factors and (ii) Deaths due to indirect causes: these were deaths resulting from a pre-existing illness or a condition that appeared during pregnancy but was not due to direct obstetric causes but was aggravated by the physiological effects of pregnancy. The MMR was calculated by dividing recorded maternal deaths by the total recorded live births over the same period in the HZ, then multiplying by 100,000.
Statistics analysis
Data were extracted using Kobotoolbox software and analyzed using Stata 16 software. For each record obtained, a de-identified ID was created in the database so as not to refer to the deceased patient or the health facility that reported the death, in order to respect anonymity. Categorical variables were summarized as count and proportion, and continuous variables as mean with standard deviation or median (min–max), according to the distribution.
Results
In total, we obtained 177 files on deaths of women of reproductive age. Of these, 143 (80.8%) were retained for the present study, including 75 in the 3 HZs of North Kivu and 68 in the 5 HZs of South Kivu. Among the 34 excluded deaths (19.2%), 27 had insufficient information documented at the facilities and 7 were a result of sudden deaths occurred and we were unable to determine the cause of death to assess if it was a maternal death. In terms of live births (LB) from 2013 to 2022, 253,289 LB were registered. Of these, 145,436 were recorded in South Kivu and 107,853 in North Kivu.
Trends in institutional maternal mortality ratio (2013–2022)
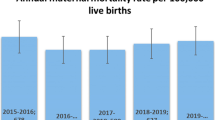
From 2013 to 2022, the study sites experienced two significant drops in MMR (in 2015 and 2018), and a spike in 2016–2017. Nonetheless, the combined MMR (across study sites) started and ended the 10-year study period at approximately the same level (53 and 57 maternal deaths per 100,000 live births in 2013 and 2022, respectively- see Fig. 1). MMR estimates disaggregated by province show similar trends for both North and South Kivu. However, the MMR in North Kivu sites plateaued between 2017 and 2019 at approximately 25 maternal deaths per 100, 000 live births (Fig. 1).

Institutional maternal mortality trends, disaggregated by province (2013- 2022)
Table 1 summarizes the trends in MMR from 2013 to 2022 in the target HZ. These can be grouped into three distinct patterns: (i) Fluctuating Trends: Some HZs, like Mwana and Kamituga, displayed sawtooth patterns, with peaks and troughs over the decade, indicating variable MMR. (ii) Stable to Increasing Trends: Idjwi HZ showed a rising curve that peaked and then steadily declined, whereas Miti-Murhesa and Kirotshe HZs had low or increasing trends respectively (iii) high peaks with subsequent declines: Minova and Karisimbi HZs experienced M-shaped or high peak trends followed by significant reductions. Some health zones have worrying MMRs, notably Kamituga (with 267 per 100.000 LB in 2014 and finishing with 199 per 100.000 live births in 2022), Minova (161 per 100.000 LB in 2021) and Karisimbi (513 per 100.000 LB in 2020, 138 per 100.000 LB in 2021).
Socio-demographic characteristics and obstetric/medical history of deceased patients
Table 2 summarizes the location and socio-demographic characteristics of the identified maternal deaths. More than half of maternal deaths reviewed were reported in secondary hospitals (hospitals and referral health centres). Almost 15% of MD occurred in non-integrated facilities (private hospital). The situation of MD occurring in non-integrated facilities is more marked in South Kivu than in North Kivu.
The average patient age was 30 years at death. Nearly half of patients had no secondary education. Finally, most patients (over 90%) were married, although the proportion of single women tended to be higher in North Kivu than in South Kivu. The average weight was 60 kg. Most of the patients were large multiparous women with a median parity of 5. However, deceased women had a median birth spacing of 24 months. Nearly half (48%) of patients had not undergone 4 ANC. The majority of patients accessed facility care by foot.
Overall, half the patients came directly from home at the time of their admission. However, almost 45% of cases were transferred from nearby health facilities. Finally, of the whole women who died, almost a third had already had at least one abortion in their lives. However, the proportion of abortions in these women's histories was almost twice as high in North Kivu as in South Kivu.
Clinical characteristics
The clinical characteristics of the patients are shown in Table 3. On delivery admission, 55.5%, 38.2% and 17.3% of patients presented with lumbopelvic pain, heavy bleeding (metrorrhagia) and loss of consciousness, respectively. The majority of patients (71.3%) had been in hospital for less than 24 h before succumbing. Fifty-eight percent of deaths reviewed occurred post-partum period, 22.4% in intrapartum period, and 19.6% antepartum. Nearly half of the identified deaths were during or after caesarean sections (C-sections). Finally, 40% of C-section was indicated because of scarring of the uterus.
Blood and ultrasound tests
A small proportion of pregnant women had abdominal ultrasounds (16,5%) and/or blood tests, including haemograms (35,2%) and serological test (HIV, hepatitis B and C) (19,8%). On the other hand, blood typing was carried out in most cases (61.5%). As for comparing between provinces, a large proportion of women in South Kivu had access to serological tests, haemograms and blood typing (Table 3).
Declared causes of death
The causes of death are summarized in Table 4. The main direct causes of death were, in decreasing order of frequency: post-partum haemorrhage (55.2%), uterine rupture (14.0), hypertensive disorders (8.4%), abortions (7.7%) puerperal infections (2.8%) and placental abruption (0.7%). In addition, indirect causes, in particular heart disease and malaria, were responsible of 11.2% of death. Comparison by province shows that abortions resulting in death were more frequent in North Kivu than in South Kivu (Table 4).
Discussion
Our study is the first to assess the evolution of the institutional MMR, the epidemiological profile, and the main causes of maternal deaths reported at facilities in 8 health zones in North and South Kivu.
High level of MMR over the decade despite efforts made to help women
Our results show that between 2013 and 2022, data show certain sites in the DRC two significant decreases and one spike in the MMR, leading to an overall stable MMR over the decade (starting at 53 deaths per 100,000 live births in 2013 and slightly increasing to 57 deaths per 100,000 live births in 2022). This is a major finding of this work. In fact, there was a consistently high level of MMR, despite efforts made to help women. This could be ascribed to several factors that could be analyzed under the “three delays model”.
The first delay is in the decision to consult the services, once danger signs have been noted. With regard to the level of education, our finding that nearly half of the women who died were illiterate is consistent with the data reported by several authors, but also with the general conclusions of the World Health Organization (WHO) indicating that disadvantaged and uneducated women are more vulnerable to morbidity and MD [14,15,16,17]. Indeed, lack of knowledge of warning signals linked to maternal health is a major factor contributing to delays in seeking obstetric care, resulting in high mortality [8, 9, 18]. This convergence of observations reinforces the universal importance of education as a crucial determinant of maternal health. In addition, it is worrying to note that almost half of pregnant women (47.83%) of the present study did not benefit from ≥ 4 ANCs. These findings are in line with similar observations at national, regional and even international level, highlighting a persistent problem in ANC access [19]. Indeed, high rates of non-attendance have been documented in the DRC (80% below 4 ANC) [20]. Cultural perceptions of pregnancy as a natural event lead many women to undervalue medical care during pregnancy, resulting in high maternal and perinatal morbidity and mortality [21,22,23]. Financial constraints and limited access to antenatal care and diagnostic tests, such as ultrasounds, in rural areas further hinder early detection and treatment of maternal and fetal complications. Furthermore, most of the deceased women had walked to the health facility This could be explained, in addition to limited financial resources of households, by the low equipment of health facilities as regards ambulances and emergency services to transport patients (second delay: transport to services). According to the service delivery report published in 2019, only 19% of facilities in the DRC had a vehicle in working order for emergency transport of patients [8]. In addition to lack of transportation means, logistical challenges to access certain health facilities are also common (poor road conditions, insecurity linked to armed groups, and long distances between hospitals and the population), making it impossible to reach the facility in time by motor vehicle.
(iii) Finally, the third delay is in the decision-making process by the health providers regarding the type of care provided to women. In the present study, the predominance of maternal deaths in the first 24 h after delivery (immediate post-partum) is in line with data reported by other authors. This is also well known from a clinical and epidemiological perspective (greatest risk on/around the day of birth) [24, 25]. This delay highlights the initial severity of their condition, an observation that may be explained by various obstacles, such as delay in seeking healthcare, lack of transportation means, late obstetric evacuations, shortage of resuscitation equipment, and sociocultural factors, such as late recourse to maternity hospital after home delivery [26,27,28]. It should be noted that the initial severity of women's condition can also be attributed to a failure in the transfer system. Indeed, 45% of the women who died had been transferred, which suggests that delay in transfer from primary care to referral facilities could be a critical factor leading to delayed care. This may help explain the considerable proportion (19.4%) of maternal deaths reported in Heath center, highlighting the importance of improving the referral system, in particular by providing qualified healthcare professionals to ensure appropriate emergency care for mothers. Furthermore, the main cause of death was post-partum haemorrhage, as per findings of several studies in developing countries and SSA [20, 25, 29,30,31]. The high incidence of MD in sub-Saharan Africa is largely due to lack of resources to ensure quality maternal health care, often linked to unsupervised deliveries and poorly staffed health facilities [29, 32, 33]. In addition, the unavailability of key maternal and child health interventions makes it much more difficult to reduce this heavy burden [3]. Delays in making decisions to seek care, referrals to appropriate levels of care and limited access to health facilities, particularly when delivery occurs at home or in inadequate primary care facilities also contribute to maternal mortality in the region [27, 29]. In brief, although progress was made in reducing MMR globally, MMR remains a major public health issue in our study region, having increased after 2019 to the 2013 level.
As for the parity and gravidity of the deceased, the medians were five and six, respectively. Some authors have reported that the incidence of maternal mortality increases as one moves from low parity to multiparity, and from multiparity to high multiparity [16, 20]. The median birth spacing in our study was 24 months. This short birth spacing may prevent complete replenishment of maternal protein reserves, iron stores and replacement of other micronutrients lost during the previous pregnancy, thus leading to worsening nutritional deficits with an increased risk of maternal death linked to postpartum haemorrhage [34, 35]. This once again emphasize the unmet need of prioritizing access to safe, voluntary family planning as a fundamental right for all women. Furthermore, the promotion of statutory regulations favoring family planning policies that guarantee constant and reliable supply of quality contraceptives would help reduce the burden of maternal mortality.
Fluctuation pattern of reported institutional Maternal Mortality Ratio (iMMR)
The MMR observed in our study remains a heavy burden to combat in relation to the SDGs, which aim to reduce global MMR < 70 maternal deaths per 100,000 live births. On the other hand, this MMR is below the national average reported for 2021 (institutional MMR-DRC: 160 in 2021) [36]. In addition, another study conducted in 2022 in 3 health zones of Maniema province in Eastern DRC, estimated the institutional MMR at 620 maternal deaths per 100,000 live births [20]. Differences between institutional MMR estimates in the national MMR, Maniema and South and North Kivu provinces could be explained by the fact that all HZs included in the present study benefited from steady funding, but also by the fact that MD outside health facilities were not taken into account as well as differences in methodology. Indeed, in most of these HZs, MNH services are fully funded by non-governmental organizations, often waiving user fees, contributing to improvements in both access to health services and retention of health workers through secure payment of wages and other financial incentives [37].
The overall MMR in 2022 in the study areas was 57 deaths per 100,000 live births, with fluctuations from 2013 to 2021 with the lowest reporting of deaths being 20 cases in 2018 and the highest peak being 103 deaths per 100,000 live births in 2016. In addition to the disparities across HZ, there were significant fluctuations within the same HZ from one year to the next.
This fluctuation pattern of reported MMR, with sudden increases in the number of reported cases followed by falls in reporting, sometimes reaching zero (meaning no deaths experienced or none reported), could on the one hand be explained by an improvement in the reporting of deaths, although the latter remains limited to deaths occurring in integrated health facilities, excluding deaths occurring in the community or in facilities not integrated into the health system; on the other hand, it could be explained by the failure of certain facilities in the zone to report deaths, due to disciplinary measures or sanctions when a death occurs in a facility. Indeed, health workers may be tempted to under-report negative outcomes such as deaths for fear of blame or financial penalties (as per performance-based financing system) [3, 37,38,39,40,41].
But beyond all this, there are well-documented challenges of under-reporting deaths in high mortality burden environments [42, 43]. Moreover, these challenges are exacerbated in conflict-affected environments such as the eastern DRC. The first challenge was the lack of documentation and/or inadequate storage of medical records. The second was the challenges related to stigma, such as cultural beliefs about pregnancy and/or its termination. Third, some studies identified issues arising from how the process of death notification/recording was organized [44, 45]. In regions plagued by crises such as the DRC, the establishment and maintenance of robust health surveillance systems are important for addressing maternal mortality effectively [41]. The MPDSR system [46] emerges as an innovative tool aiming at systematically capturing and analyzing data on maternal and child deaths. This surveillance mechanism is essential not only for identifying the immediate causes of such fatalities but also for understanding the underlying factors contributing to these outcomes.
Impact of armed conflict on maternal health in the two provinces
In our study, we found that unlike women who died in South Kivu, those who died in North Kivu had lower parity and gestational age. In addition, they showed a higher proportion of previous abortions than those from South Kivu. This could well be explained by the high frequency of active conflict in the North Kivu ZS, unlike in the South Kivu ZS. In fact, fertility in the context of conflict could decrease due to demographic changes (reduced frequency of marriage and separation from spouse) and biological effects (reduced fertility or increased spontaneous abortion, particularly when famine coexists [5]. In addition, a reduction in access to modern contraceptives and an increase in sexual violence could lead to more abortions in the context of clandestine voluntary termination of pregnancy. This may well be illustrated by certain studies which have shown a reduction in fertility during the active phase of the conflict. For example, in Cambodia, fertility fell by around a third compared with pre-civil war levels between 1975 and 1979 [47]. Similarly, Fertility rates in Angola, Ethiopia, and Eritrea have shown a notable decrease, which can be directly attributed to the conflicts affecting these countries. The societal disruptions and economic hardships brought on by prolonged conflicts have played a significant role in this demographic change [5, 48,49,50]. The common reasons for these reductions in fertility were the separation of spouses, decreased weddings, lower fertility and increased risk of spontaneous abortion, particularly when famine coexists.
Certain methodological limitations should be taken into account when interpreting the present results. Firstly, the selection of HZs was based on the support of specific partners and safety concerns, which could lead to potential biases in the representativeness of the results. Secondly, the exclusion of certain medical records due to gaps in information (19,2%) may constitute a significant limitation if the missing data turned out to be different from those collected. Thirdly, the causes of death were those mentioned by the health facilities in the death registers and in the patients' medical records and not on the basis of the ICD-10/11 classification of causes of death due to the lack of training of healthcare providers in the health facilities of North and South Kivu in the classification of causes of death according to ICD-10/11. Fourthly, over a 10-year period, several healthcare facilities may have started operating long before and then had to close their doors. All this may have influenced our findings in one way or another. Finally, the availability of data, by deficiencies in the registers, on the stage of pregnancy at the time of admission, whether or not the patient was assisted by qualified staff, and on a number of comorbidities would have been crucial to our work and would have given much greater support to our explanations and arguments. It is therefore necessary to capitalize on this for future research in our region.
Conclusion
This study highlights the worrying reality of maternal mortality in South and North Kivu provinces in the DRC and the need for improved documentation and reporting of deaths so that data can be used to improve services/programs. Despite the efforts made, maternal mortality ratio remain high, underlining the need for urgent action to improve access to quality maternal health care. Targeted interventions such as the establishment and maintenance of MPDSR system are needed to reduce maternal mortality. By emphasizing the crucial importance of intrapartum/immediate postpartum and quality of care, significant progress can be made in guaranteeing maternal health and reducing these avoidable deaths.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- ANC:
-
Antenatal Care
- CHWs:
-
Community health workers
- CHZO:
-
Central Health Zones Office
- DDC:
-
Swiss agency for development and international cooperation
- DRC:
-
Democratic Republic of Congo
- GRH:
-
General referral hospitals
- HC:
-
Health centers
- HIV:
-
Human Immunodeficiency Virus
- HZs:
-
Health zones
- LB:
-
Live births
- MD:
-
Maternal Deaths
- MMR:
-
Maternal mortality ratio
- MPDSR:
-
Maternal, Perinatal Death Surveillance and Response
- RH:
-
Referral hospitals
- RHC:
-
Referral health centers
- SSA:
-
Sub-Saharan Africa
References
Trends in maternal mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division. Geneva: World Health Organization; 2023. Licence: CC BY-NC-SA 3.0 IGO . https://iris.who.int/bitstream/handle/10665/366225/9789240068759-eng.pdf?sequence=1
World Health Organization. Maternal mortality. 2019. Available from: https://www.who.int/fr/news-room/factsheets/detail/maternal-mortality.
Malembaka EB, Altare C, Bigirinama RN, Bisimwa G, Banywesize R, Tabbal N, et al. The use of health facility data to assess the effects of armed conflicts on maternal and child health: experience from the Kivu, DR Congo. BMC Health Serv Res. 2021;21(Suppl 1):195.
Wagner Z, Heft-Neal S, Wise PH, Black RE, Burke M, Boerma T, et al. Women and children living in areas of armed conflict in Africa: a geospatial analysis of mortality and orphanhood. Lancet Glob Health déc. 2019;7(12):e1622–31.
Bendavid E, Boerma T, Akseer N, Langer A, Malembaka EB, Okiro EA, et al. The effects of armed conflict on the health of women and children. Lancet Lond Engl. 2021;397(10273):522–32 6 févr.
The World Bank Group : ÉTUDE SUR L’ESPACE BUDGÉTAIRE DU SECTEUR DE LA SANTÉ EN RDC :LA RDC PEUT SI ELLE LE VEUT RÉALISER LA CSU. 2019. https://www.globalfinancingfacility.org/fr/resource/etude-sur-lespacebudgetaire-du-secteur-de-la-sante-en-rdc-la-rdc-peut-si-elle-le-veut.
Montagu D, Sudhinaraset M, Diamond-Smith N, Campbell O, Gabrysch S, Freedman L, et al. Where women go to deliver: understanding the changing landscape of childbirth in Africa and Asia. Health Policy Plan. 2017;32(8):1146–52.
Ecole de Santé Publique de l’Université de Kinshasa (ESPK) et ICF: Évaluation des Prestations des Services de soins de Santé (EPSS RDC) 2017- 2018. Kinshasa, RDC et Rockville, Maryland, USA : ESPK et ICF. 2019
Centers for Disease Control and Prevention (CDC). Elevated mortality associated with armed conflict–Democratic Republic of Congo, 2002. MMWR Morb Mortal Wkly Rep. 2003;52(20):469–71.
Omba Kalonda JC. Socioeconomic impact of armed conflict on the health of women and children in the Democratic Republic of the Congo. Med Trop Rev Corps Sante Colon. 2011;71(2):192–6.
Coghlan B, Brennan RJ, Ngoy P, Dofara D, Otto B, Clements M, et al. Mortality in the Democratic Republic of Congo: a nationwide survey. Lancet Lond Engl. 2006;367(9504):44–51.
Jarrett P, Zadravecz FJ, O’Keefe J, Nshombo M, Karume A, Roberts L. Evaluation of a population mobility, mortality, and birth surveillance system in South Kivu, Democratic Republic of the Congo. Disasters avr. 2020;44(2):390–407.
Masirika BI, Masirika Irenge B, Kajibwami Birindwa E, Obstétrique G, Traitant M. Analyse des facteurs Explicatifs des décès maternels intra hospitaliers dans la zone de Santé Rurale de Miti-Murhesa, RDC . 2021. Cité 21 févr 2024. Disponible sur: https://hal.science/hal-03412153
Stone PK. Biocultural perspectives on maternal mortality and obstetrical death from the past to the present. Am J Phys Anthropol janv. 2016;159(Suppl 61):S150-171.
Borde MT. Geographical and Socioeconomic Inequalities in Maternal Mortality in Ethiopia. Int J Soc Determinants Health Health Serv. 2023;53(3):282–93.
Stefanovic V. Education in developing countries and reducing maternal mortality: a forgotten piece of the puzzle? J Perinat Med. 2021;49(9):1042–7.
Khalili M, Mashrouteh M, Haghdoost A, Torkian S, Chegeni M. Systematic review and meta-analysis of maternal mortality ratio and related factors in the Islamic Republic of Iran. East Mediterr Health J Rev Sante Mediterr Orient Al-Majallah Al-Sihhiyah Li-Sharq Al-Mutawassit. 2023;29(5):380–401.
Onambele L, Ortega-Leon W, Guillen-Aguinaga S, Forjaz MJ, Yoseph A, Guillen-Aguinaga L, et al. Maternal Mortality in Africa: Regional Trends (2000–2017). Int J Environ Res Public Health. 2022;19(20):13146.
Kawungezi PC, AkiiBua D, Aleni C, Chitayi M, Niwaha A, Kazibwe A, et al. Attendance and Utilization of Antenatal Care (ANC) Services: Multi-Center Study in Upcountry Areas of Uganda. Open J Prev Med. 2015;5(3):132–42.
Ramazani IBE, Ntela SDM, Ahouah M, Ishoso DK, Monique RT. Maternal mortality study in the Eastern Democratic Republic of the Congo. BMC Pregnancy Childbirth. 2022;22(1):452.
Chimatiro CS, Hajison P, Chipeta E, Muula AS. Understanding barriers preventing pregnant women from starting antenatal clinic in the first trimester of pregnancy in Ntcheu District-Malawi. Reprod Health. 2018;15(1):158.
Wang H, Frasco E, Takesue R, Tang K. Maternal education level and maternal healthcare utilization in the Democratic Republic of the Congo: an analysis of the multiple indicator cluster survey 2017/18. BMC Health Serv Res. 2021;21(1):850.
Ahmed M, Demissie M, Worku A, Abrha A, Berhane Y. Socio-cultural factors favoring home delivery in Afar pastoral community, northeast Ethiopia: A Qualitative Study. Reprod Health. 2019;16(1):171.
Kea AZ, Lindtjorn B, Gebretsadik A, Hinderaker SG. Variation in maternal mortality in Sidama National Regional State, southern Ethiopia: A population based cross sectional household survey. PLOS ONE. 2023;18(3):e0272110.
Tesfaye G, Loxton D, Chojenta C, Assefa N, Smith R. Magnitude, trends and causes of maternal mortality among reproductive aged women in Kersa health and demographic surveillance system, eastern Ethiopia. BMC Womens Health. 2018;18(1):198.
V F, F R, I L, F O. Identifying barriers from home to the appropriate hospital through near-miss audits in developing countries. Best Pract Res Clin Obstet Gynaecol. juin 2009. Cité 12 janv 2024;23(3). Disponible sur: https://pubmed.ncbi.nlm.nih.gov/19250874/
Fong RM, Kaiser JL, Ngoma T, Vian T, Bwalya M, Sakanga VR, et al. Barriers and facilitators to facility-based delivery in rural Zambia: a qualitative study of women’s perceptions after implementation of an improved maternity waiting homes intervention. BMJ Open. 2022;12(7):e058512.
Shiferaw MA, Bekele D, Surur F, Dereje B, Tolu LB. Maternal Death Review at a Tertiary Hospital in Ethiopia. Ethiop J Health Sci janv. 2021;31(1):35–42.
Musarandega R, Nyakura M, Machekano R, Pattinson R, Munjanja SP. Causes of maternal mortality in Sub-Saharan Africa: A systematic review of studies published from 2015 to 2020. J Glob Health. 2021;11:04048.
Ezegwui H, Onoh R, Ikeako L, Onyebuchi A, Umeora O, Ezeonu P, et al. Investigating Maternal Mortality in a Public Teaching Hospital, Abakaliki, Ebonyi State. Nigeria Ann Med Health Sci Res. 2013;3(1):75–80.
Ronsmans C, Graham WJ. Lancet Maternal Survival Series steering group. Maternal mortality: who, when, where, and why. Lancet Lond Engl. 2006;368(9542):1189–200.
Gross D. Improving child and adolescent health and health care quality: report from the pediatric health and health care quality measures committee of the Institute of Medicine. J Pediatr Health Care Off Publ Natl Assoc Pediatr Nurse Assoc Pract. 2011;25(6):405–8.
Barber SL, Gertler PJ. Empowering women to obtain high quality care: evidence from an evaluation of Mexico’s conditional cash transfer programme. Health Policy Plan janv. 2009;24(1):18–25.
Ujah IaO, Aisien OA, Mutihir JT, Vanderjagt DJ, Glew RH, Uguru VE. Factors contributing to maternal mortality in north-central Nigeria: a seventeen-year review. Afr J Reprod Health. 2005;9(3):27–40.
Thiam M. MORTALITE MATERNELLE AU CENTRE HOSPITALIER REGIONAL DE THIES : ETIOLOGIES ET FACTEURS DETERMINANTS, A PROPOS DE 239 DECES. J SAGO Gynécologie – Obstétrique Santé Reprod. 2017. Cité 21 févr 2024;18(1). Disponible sur: http://www.jsago.org/index.php/jsago/article/view/3
Countdown to 2030 for the health of women, children and adolescents,UNICEF, GFF, World Health Organization, APHRC. Indicateurs de santé reproductive, maternelle, néonatale et infantile. Réunion Annuelle des pays. Geneva: World Health Organization; 2023. https://www.countdown2030.org/wp-content/uploads/2024/02/Rapport-RDC_Final.pdf.
Maini R, Mounier-Jack S, Borghi J. Performance-based financing versus improving salary payments to workers: insights from the Democratic Republic of Congo. BMJ Glob Health. 2018;3(5): e000958.
RDC-PROSANIplus: Renforcement de la communication des données sanitaires et amélioration de leur qualité́ et utilisation grâce à l’intégration des données nationales et celles du projet dans la plateforme DHIS 2: enseignements tirés de la RDC. In. 2018. https://pdf.usaid.gov/pdf_docs/PA00TF1R.pdf.
Mary M, Tappis H, Scudder E, Creanga AA. Complexities of implementing Maternal and Perinatal Death Surveillance and Response in crisis-affected contexts: a comparative case study. Confl Health. 2024;18(1):45.
Kinney MV, Day LT, Palestra F, Biswas A, Jackson D, Roos N, et al. Overcoming blame culture: key strategies to catalyse maternal and perinatal death surveillance and response. BJOG Int J Obstet Gynaecol mai. 2022;129(6):839–44.
Mary M, Tappis H, Scudder E, Creanga AA. Implementation of maternal and perinatal death surveillance and response and related death review interventions in humanitarian settings: A scoping review. J Glob Health. 2024;14:04133.
Gudo ES. Mozambique Sample Vital Statistics System: Filling the Gaps for Mortality Data. Am J Trop Med Hyg. 2023;108(5_Suppl):3–4.
Boerma T. Addressing the Gaps in Mortality Data: A Case for National Mortality Surveillance. Am J Trop Med Hyg. 2023;108(5_Suppl):1–2.
Ahmed SMA, Cresswell JA, Say L. Incompleteness and misclassification of maternal death recording: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2023;23(1):794.
Qin SS, Vinluan J, McCahy P. Analysis of potential clinical management issues in unreported mortality data from an Australian health service. ANZ J Surg mai. 2023;93(5):1181–4.
World Health Organization: Maternal and perinatal death surveillance and response: materials to support implementation. Geneva: World Health Organization; 2022. https://www.who.int/fr/publications/i/item/9789240036666.
de Walque D. The socio-demographic legacy of the Khmer Rouge period in Cambodia. Popul Stud juill. 2006;60(2):223–31.
Agadjanian V, Prata N. War, peace, and fertility in Angola. Demography mai. 2002;39(2):215–31.
Lindstrom DP, Berhanu B. The impact of war, famine, and economic decline on marital fertility in Ethiopia. Demography mai. 1999;36(2):247–61.
Blanc AK. The role of conflict in the rapid fertility decline in Eritrea and prospects for the future. Stud Fam Plann déc. 2004;35(4):236–45.
Acknowledgements
We thank all the participants who took part in this study and made it possible. We also acknowledge the support of the research staff (and data collectors) of the Ecole Regionale de Santé Publique of the Université Catholique de Bukavu, the North and South Kivu Provincial Health Division and the “Direction du Développement et de la Coopération (DDC)” who support-ed our study at different levels.
Funding
This research was funded by the “Direction du Développement et de la Coopération (DDC)”, the swiss agency for development and international cooperation.
Author information
Authors and Affiliations
Contributions
PM, EN and GB conceived and designed the experiments. PM, Jc L and GN did the data collection. MD contributed to specific areas of data analysis and quality control. PM, Jc L and GN analyzed the data. PM wrote the first draft of the manuscript. MPH, MM, HT, CC, ChC,RB, MD and GB contributed to the writing of the manuscript and agree with the manuscript’s results and conclusions. All authors reviewed the submitted manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed consent was obtained from all subjects. Respondents provided signed informed consent for participation to the study, either by written signature or by fingerprints, depending on literacy. All procedures performed in this study were approved by the Institutional Ethics Committee of the Université Catholique de Bukavu under the reference UCB/CIES/NC/021/2022 and were in accordance with the 1964 Helsinki declaration and its later amendments.
Consent for publication
N/A.
Competing of interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mwene-Batu, P., Ndokabilya, E., Lembebu, J.C. et al. Maternal mortality in Eastern Democratic Republic of Congo: a 10-year multi-zonal institutional death review. BMC Public Health 24, 2280 (2024). https://doi.org/10.1186/s12889-024-19804-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19804-z