
Abstract
Background
The global prevalence of overweight and obesity in children under the age of five has emerged as a significant issue in recent years. Physical activity and fitness among children and adolescents have declined globally in the past few decades. Studies have indicated a link between levels of physical activity and cognitive performance in preschool children.
Methods
This quasi-experimental study investigated the effects of three different types of physical education programmes on the physical fitness and emotional competence of 239 preschoolers(mean age = 5.49 ± 0.60 years, 54.4% boys)in Haikou, China. The preschoolers were grouped based on which programme they were assigned to: the “Hello Sunshine” ball skills programme (HS group), ordinary physical education (OPE group), and free play (FP group). The “Hello Sunshine” ball skills programme used both a structured curriculum design and autonomous activity selection during outdoor time., which were conducive to children’s physical fitness.The National Physical Fitness Measurement Standards Manual and the shortened version of the Social Competence and Behavior Evaluation Scale (SCBE-30) were used to assess physical fitness and emotional competence, respectively. These assessments were conducted both before and after the ten-week intervention period. The analysis utilised a mixed-effects model for physical fitness and a mixed-model ANOVA for the SCBE data.
Results
The HS group and OPE group demonstrated significantly improvement in the standing long jump, 10-m shuttle run and balance beam walking than the FP group; meanwhile, only anxious-withdrawal levels showed a significant grouping effect and group-by-time interaction effect. After the intervention, both the HS group and the FP group showed significantly lower scores for anxiety compared to the OPE group, with no significant difference observed between the HS and FP groups.
Conclusions
The results suggested that structured ball skills programmes may promote physical fitness and reduce anxiety. The integration of effective physical exercise programmes into preschool curricula holds the potential for promoting holistic development.
Similar content being viewed by others
Background
The early childhood stage is crucial for physical, emotional, social, and intellectual development. However, according to authoritative reports, global prevalence of overweight and obesity in children under the age of five has emerged as a significant issue in recent years, with 37 million children under the age of 5 being overweight in 2022 [1, 2]. In children, physical fitness is a significant indicator of healthy growth, development, and overall well-being, encompassing the effective coordination of various body systems to perform daily activities and maintain good health [3]. Physical fitness can be broadly categorized into health-related and performance-related components. Health-related physical fitness includes cardiorespiratory endurance, muscular strength, muscular endurance, flexibility, and body composition. These components are critical for overall health and the prevention of diseases. Performance-related physical fitness, on the other hand, focuses on attributes such as agility, balance, coordination, power, reaction time, and speed, which are crucial for optimal performance in physical activities and sports [4].
Various countries have developed measurement methods to assess physical fitness and implemented continuous tracking to monitor changes in individuals’ fitness levels. Recent data highlights that physical activity (PA) and fitness among children and adolescents have declined globally in the past few decades; in particular, cardiopulmonary endurance has demonstrated a long-term negative trend, with an overall change of about 1.5 standard deviations for both boys and girls [5, 6]. The situation in China is also concerning. Although data indicate that, over the past two decades, the physical growth and nutritional status of Chinese preschool children have notably improved, overweight and obesity are becoming increasingly prominent in this population [7]. In line with this, most preschool children’s physical activities do not meet the recommended standards [8]; indeed, the 2020 Chinese National Fitness Survey revealed a downward trend in certain physical fitness indicators among preschoolers over the past decade. For example, boys showed a 1.3% decrease in jumping with both feet and a 6.6% decrease in broad jump performance, while girls showed decreases of 1.6% and 5.3%, respectively, in the same activities [9].
Studies have indicated a positive link between physical fitness and levels of PA [10] and cognitive performance [11, 12] in preschool children. Furthermore, cognitive, emotional, and social competencies do not exist in isolation but rather coalesce and develop in tandem throughout the lifespan and create strong academic and health outcomes [13]. Emotional competence encompasses the capacity to recognise, comprehend, express, and manage emotions [14]. Research findings have indicated that emotional competence during the preschool years plays a significant role in fostering social competence and carries long-lasting implications [15]. Research has shown that age and gender can significantly impact children’s social competence, behavior problems, and emotional regulation, with preschool boys generally being more aggressive and having poorer social skills compared to girls [16], and social competence improving progressively with age [17]. The early development of social and emotional skills is a crucial factor in predicting academic preparedness and future achievement in education [18, 19]. Moreover, nurturing children’s social and emotional competence not only enhances their cognitive abilities but also fosters positive attitudes towards school and improves student behaviour [20, 21]. In the conceptual model of Health through Sport [22], engagement in sports is positively associated with individual psychological, social, and societal well-being. On the other hand, previous studies have found that physical exercise influences emotional competence through various neurobiological mechanisms, including the release of mood-regulating neurotransmitters and the enhancement of neuroplasticity [23,24,25].Neuroimaging evidence found improved cognitive function [26] and positive social interactions during PA [27], which may further support the development of emotional competence.In contrast, certain evidence suggested that children with limited motor abilities experience social and emotional challenges, such as elevated levels of anxiety and depression, and that these problems appear as early as age four [28, 29].
Kindergarten, recognised as a pivotal environment for promoting PA, offers significant advantages and has the potential to generate numerous public health benefits [30]. Recent research suggests that policies implemented in kindergartens can have an impact on children’s participation in PA, the duration of outdoor activities, and the strategies employed by teachers to encourage PA [30, 31]. In the past, intervention studies have primarily been focused on interventions at kindergartens [32, 33], joint family-kindergarten programmes [34], and multifaceted kindergarten-family-community programmes [35]. These studies have employed specific types of intervention methods, including strength-dominated exercise [36], ball skills [37] and mixed physical exercises [33, 38, 39] to explore the effects of exercise programmes on children’s physical and motor domains. However, two recent systematic reviews have reported that methodologies of existing studies reporting the positive effects of body-oriented interventions on social-emotional competencies, such as empathy and social interaction, were of limited high methodological quality(such as the implementation of blinding) [40, 41].
In China, due to variations in kindergartens’ specific characteristics and requirements for facilities, teachers, and premises, there are three main forms of preschool physical education. These include unique sports-oriented curricula designed by kindergartens themselves (i.e., a kindergarten provides a range of specialised sports and physical education programmes, capitalising on school resources, favourable geography, and teachers’ expertise, e.g. national football characteristic kindergarten), the adoption of general physical education materials (i.e., some ordinary public kindergartens in China adopt the unified physical education textbooks of each province and city), and free play (i.e., PA time is dominated by children’s free play) [42]. During the pandemic, kindergartens adapted their PA programmes to ensure the safety and well-being of children. Activities now focus on individual play and movement, with an emphasis on maintaining social distancing. Notably, outdoor activities that used balls as a medium were a fun way to engage in physical exercise, such as throwing, catching, and kicking exercises. These activities help children enhance their PA participantion, motor skills, and spatial awareness while maintaining a safe distance. Especially noteworthy is that ball skills reflect the ability to control objects and are a part of fundamental movement skills [43]. Evidence suggests that the comprehensive development of fundamental movement skills in childhood, particularly ball skills, is considered crucial for acquiring more intricate movement patterns and increasing the likelihood of successful participation in both team and individual sports [44, 45]. For instance, “SKIP” (Successful Kinesthetic Instruction for Preschoolers) [46] and “CHAMP” (Children’s Health Activity Motor Programme) [37] emphasise the development of ball skills to enhance these capabilities. Given the potential health effects of implementing physical education in kindergartens, this study explored the impact of a ball skill-based programme, “Hello Sunshine”, on physical fitness and emotional competence in preschool children. Specifically, it was hypothesised that three different models of physical education programmes for preschoolers, the “Hello Sunshine” programme, traditional physical education, and free play activities would enhance the children’s physical fitness and emotional competence; however, it was also hypothesised that the “Hello Sunshine” programme would have a more significant impact on enhancing physical fitness and emotional competence in preschool children than traditional physical education and free play activities.
Methods
Study design and population
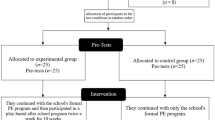
This study was designed as a quasi-experimental trial with a ten-week physical exercise programme intervention, and pre- and post-intervention assessments. The pre-registration research protocol obtained approval from the Ethics Committee for Human Research at Khan Kaen University, demonstrating adherence to the ethical standards outlined in the Declaration of Helsinki (Ethical approval number: HE642100), and was registered with the Chinese Clinical Trial Registry(ChiCTR ChiCTR2000035414)on 8 October 2020.
Preschoolers from grades K2-K3 in three different types of kindergartens (sports-focused, ordinary public, and non-profit private kindergartens) in the centre of Haikou City, China participated in the study. Each kindergarten class was considered an experimental unit, and children were selected from two classes in the K2 and K3 grades. The eligibility criteria for the children were as follows: (1) to be in good health and typically developing, (2) 4–6 years old, (3) no additional sports club training, and (4) primary caregiver provided informed consent. Children with known learning and physical disabilities, motor delays, and medical or psychological diagnoses were excluded.
Participants
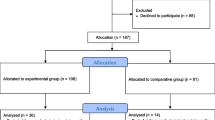
WinPepi software was utilised and referenced Westendorp et al. [47] to calculate the sample size. A significance level of 5%, power of 80%, confidence level of 95%, and dropout rate of 20% were utilized in the study. Initially, 249 preschool children were recruited and divided into three groups of 83 based on their respective kindergarten physical education models. However, ten children were excluded from the analysis due to missing or outlier data for one or more outcome variables. Therefore, data from 239 preschool children (mean age and sex) were included in the statistical analysis. Detailed demographic and anthropometric data were presented in Table 1.
Intervention
All three preschool groups participated in 30-minute physical education classes.The K2 group attended one class per week, while the K3 group attended two classes per week. Additionally, all groups had 30-minute outdoor classes every day, five days a week, throughout the ten-week intervention period. Apart from physical education and outdoor classes, the daily activities of the students in the three groups were similar.
Hello sunshine group (HS group)
“Hello Sunshine” followed a structured, age-based curriculum focused on ball skills. This curriculumis a school-based programme collaboratively developed by physical education experts and experienced PE teachers from the kindergarten. It was created by upgrading and expanding the kindergarten’s existing sports curriculum, which included basketball and football and had been successfully implemented for three years. The upgraded curriculum incorporated additional ball activities, such as badminton, table tennis, and handball. During the 10-week intervention, this enhanced curriculum was used to teach children various ball skills in physical education (PE) classes These sessions included “ball sense,” dribbling, passing, and gameplay. Outdoor classes featured both pre-set ball skills and optional area ball games. Skilled PE teachers guided the children through predetermined game scenarios during PE classes, where they demonstrated and explained basic ball skills and knowledge through games or stories. During the outdoor class time, the children had a high level of autonomy and could explore various ball-game stations independently. Each class was organised with a structure comprising a 5-minute warm-up, a 20–25-minute exercise session, and a 5-minute cool-down activity. Outdoor time allows for a significant level of autonomy. Apart from the optional ball skills activity once a week (K2) or twice a week (K3), participants could choose their exercise area during the remaining outdoor time, including options like the equipment area or bicycle zone. More details on how this programme may be implemented are available elsewhere [48].
Ordinary physical education (OPE group)
In the OPE group, PE classes were taught by a dedicated PE teacher who followed a specific kindergarten textbook.This textbook covered various themes related to health and physical activity, such as fundamental movement skills, and exercises promoting overall physical fitness. The outdoor class time for this group was the same as that of the HS group; however, the children were allowed to engage in free play in different areas.
Free play group (FP group)
In the FP group, preschoolers had the opportunity to freely play using various playground facilities, such as slides and sandboxes, under the supervision of kindergarten teachers who did not have a PE background.
Outcome measures
To assess physical fitness and emotional competence, a preschool physical fitness test battery and a teacher-reported questionnaire on children’s emotional competence were used [49]. All measurements were conducted in the respective kindergartens. A team of trained and experienced researchers followed the standard operating procedures for the tests.
Physical fitness measures
The National Physical Fitness Measurement Standards Manual [50] was used; the physical fitness testing battery included anthropometric data (height, weight), sit and reach test, the standing long jump test, the double-leg timed hop test, the 10-m shuttle run, balance beam walking, and tennis ball throwing. Each participant is tested twice for each item, and the best result is recorded.
(1) Sit and reach test: This test measures the flexibility of the lower back and hamstrings, which is the ability of these muscle groups to stretch and allow a range of motion. Participants sit on the floor with legs extended straight ahead and reach forward as far as possible, keeping the knees straight. The distance reached is recorded.
(2) Standing long jump test: This test assesses explosive leg strength, defined as the ability of the leg muscles to exert maximum force in a short period of time. It is measured by the distance a participant can jump forward from a standing position.
(3) Double-leg timed hop test: This test evaluates lower body strength and power, which involves the ability of the leg muscles to generate force repeatedly over a period of time. Participants perform consecutive hops on both legs over ten soft blocks spaced 0.5 m apart on a flat surface. The total time taken to complete the hops is recorded from the start signal until both feet land past the tenth block.
10-m shuttle run: This test measures agility and speed, defined as the ability to change direction quickly and move rapidly. Participants run back and forth between two lines set 10 m apart as quickly as possible, touch an object with their hand at return line, then turn and sprint back to the starting line.The total time to complete a set number of shuttles is recorded.
Balance beam walking: This test assesses balance and coordination, the abilities to maintain body stability and control movements smoothly. Participants walk across a narrow beam without stepping off, and the time taken to complete the walk is recorded.
Tennis ball throwing test: This test measures upper body coordination and strength, defined as the ability of the upper body muscles to work together to produce a forceful and precise movement. Participants throw a tennis ball as far as possible from a designated point, and the distance the ball is thrown is recorded.
Emotional competence measures
The shortened version of the Social Competence and Behavior Evaluation Scale (SCBE-30) was used to measure the participants’ levels of emotional competency, which developed by LaFreniere and Jean in 1996, the SCBE-30 comprises 30 items, each scored on a 6-point Likert scale, where 1 represents ‘never’ and 6 represents ‘always‘ [51]. The scale includes three subdomains: social competence, anger aggression, and anxiouswithdrawal, and scoring for each subscale was calculated by summing the scores of specific items related to that factor. It has shown strong inter-rater and test-retest reliability, as well as strong internal consistency and temporal stability [51]. In this study, the Chinese version of the SCBE-30 [49] filled out for each child individually by their teacher. The scale exhibited strong internal consistency, with Cronbach’s α values of 0.91 for the social competence dimension, 0.88 for the anger-aggression dimension, 0.91 for anxious withdrawal, and an overall Cronbach’s α value of 0.92.
Procedure
Kindergarten students were recruited at the beginning of the school term in March 2022. The teacher placed an informed consent form in each student’s backpack for parents to review. These forms included detailed information about the study’s purpose, procedures, potential risks and benefits, and the confidentiality of the collected data. Contact information for the researchers was also provided, allowing parents to ask any additional questions. Researchers and teachers then screened the children whose parents returned the signed consent forms.
All measures were conducted within the kindergartens over a span of two weeks. For the physical fitness assessments, children were tested individually by trained researchers in a designated area within the kindergarten to minimize distractions. Prior to the testing, all children participated in approximately 5 min warm-up routine included light aerobic exercises, dynamic stretching. Each test was demonstrated by the researchers before the children performed them to ensure they understood the procedures. Adequate rest was provided between tests to ensure the children’s comfort and optimal performance. For the emotional competence assessment, teachers completed the SCBE-30 questionnaire based on their observations of the children over the previous month. Teachers filled out the questionnaires in a quiet setting, free from interruptions, to ensure they could provide thoughtful and accurate responses. Researchers were available to clarify any questions regarding the questionnaire to ensure consistency in the responses.
Data collection and analysis
Analyses were performed using IBM SPSS (version 25.0; IBM, Armonk, NJ, USA). A normality study was conducted, and further descriptive statistics were obtained. Intragroup comparisons were performed using paired t-tests or Wilcoxon paired-sample tests based on the data distribution or scoring criteria. The raw data of the physical fitness tests were analysed using a longitudinal model, employing a mixed-effects model (with gender, age, height, weight, and baseline data as covariates), and forest plots were created using the R programming language (R4.2.1). Using age and gender as covariates, a 3 (HS, OPE, and FP) × 2 (baseline and after 10 weeks) mixed-model ANOVA comparison was employed for the SCBE data, considering the absence of baseline differences between the groups. The effect size, denoted by Partial η2 (pŋ2), was utilised to quantify the magnitude of the effect, with small (0.01), medium (0.06), and large (0.14) classifications.
Results
Effects of physical education on physical fitness among the three groups
The statistical differences in physical fitness parameters from pre- to the post-test among the children in the three groups were shown in Table 2. Significant improvements in pre-post differences were found for the HS, OPE and FP groups in standing long jump, and 10-m shuttle run. In addition, the HS group showed significant improvements in tennis ball throwing (p < 0.05), while the FP group demonstrated a significant increase in sit-and-reach test. The model showed that the HS group performed better than the FP group (p < 0.05) and had a small-to-medium effect size (0.036–0.121) in all tests except the sit and reach item (F = 1.093, p = 0.337). In addition, the HS group performed better than the FP group in tennis ball throwing (F = 4.52, p = 0.012). Both HS and OPE groups exhibited significantly greater improvements compared to FP group in the standing long jump (F = 16.449, p < 0.001), 10-m shuttle run (F = 15.117, p < 0.001), and balance beam walking (F = 11.378, p < 0.001) (Fig. 1).

Effects of the HS and OPE groups on physical fitness parameters compared to FP group, Sex, age, height, weight, and baseline values were adjusted as covariates.Data were presented as mean between-group differences with 95% confidence intervals (Note Double-leg timed hop, 10-m shuttle run, and Balance beam walking are compared based on timing (s), while Tennis ball throwing is compared based on distance(m). No significant differences were found in the three groups of sit-and-reach tests, so they were not shown in the figure. The wide confidence interval of the standing long jump results also affected the overall image quality and was not displayed)
Effects of physical education on emotional competence among the three groups
The SCBE results demonstrated no significant differences in the mean values of social competence [F(2, 236) = 2.772, p = 0.065], anger aggression [F(2, 236) = 2.717, p = 0.068], and anxious withdrawal [F(2, 236) = 3.037, p = 0.05] among the three groups of children in their baseline level tests. Further analysis of the results showed no significant changes in the main effect of time in the three dimensions before and after the intervention (p > 0.05). The main effect of grouping was found on anger aggression[F(2, 236) = 3.801, p = 0.024, Partial η2 = 0.031] and anxious-withdrawal [F (2, 236) = 4.278, p = 0.015, Partial η2 = 0.035], with significant differences in scores among the three groups after the intervention; however, the corresponding interaction between grouping and time were not significant. Meanwhile, the results of the anxious-withdrawal levels showed an obvious grouping effect [F(2, 236) = 4.278, p = 0.015, Partialη2 = 0.035], with a significant interaction effect observed between the grouping and time [F(2, 236) = 7.802, p = 0.001, Partialη2 = 0.063] (Table 3). Multiple comparisons indicated that there were no significant differences in anxiety scores among the groups before the intervention. However, after the intervention, both the HS group(p = 0.02) and the FP group(p < 0.001) showed significantly lower scores compared to the OPE group, with no significant difference observed between the HS and FP groups (Table 4).
Discussion
The preschool stage is widely recognised as a crucial period for implementing interventions aimed at promoting PA participantion [52], owing to the strong plasticity of young children. It is believed that increasing PA levels during early childhood not only improves children’s health and motor skills but also promotes healthy and active lifestyles in the longer term [53]. The vast majority of children spend approximately eight hours per day in daycare (mainly kindergartens) [54]. As key intervention environments for PA participation, kindergartens have many advantages and can produce a wide range of public health benefits. This quasi-experimental study explored the effects of the HS intervention curriculum on children’s physical fitness and emotional competence and compared them with the effects of the interventions in the OPE and FP groups.
Beneficial effects on physical fitness
The results of the present study showed significant improvements in most of physical fitness measures after ten -weeks physical exercise intervention, with the HS and OPE groups showing better results than FP group in terms of explosive leg powe (standing long jump), agility and speed (10-m shuttle run), and dynamic balance (balance beam walking), and HS group having a longer tennis throwing distance compared to the other groups. This result concurs with previous studies, wherein structured PA course interventions improved physical fitness. In a quasi-experimental study, after a nine-month structured multi-sport programme (60 min of basic/gross and fine motor skills and ball play-based exercises twice a week), children showed sustained improvements in physical fitness, particularly strength, speed, agility, and flexibility [38]. Another study of a 30-minute PA intervention and PA homework for 4-to-5 years old children over one academic year discovered improvements in static balance (single-leg stance), explosive leg strength (standing long jump), jumping coordination, and agility during the follow-up period [55]. Wang et al. [33]compared the effects of a 16-week programme among our physical exercise interventions on physical fitness of children aged 4–5 years and found that the ball games and multiple activity groups had an advantage over the basic movements group and rhythm activities group in terms of improving physical fitness. As suggested by similar studies, diverse PA modules and structured multi-sport programmes have demonstrated notable benefits in enhancing physical fitness in preschoolers when compared to free play or regular PA [38, 56]. This study explored the effect of the “Hello Sunshine” programme, a ball skills-based programme that teaches children a variety of motor skills and encourages them to repeatedly practice them. Abundant research evidence supports a significant positive correlation between fundamental movement skills and cardiovascular health, as well as muscle strength and endurance [57, 58]. Strong evidence indicates a positive association between fundamental movement skills proficiency and PA levels in children and adolescents [59]. Considering the Stodden’s classic conceptual model [60], the development of motor skill competence is regarded as a primary underlying mechanism for promoting engagement in PA and fitness, which partly explains why the HS group improved their performance on most physical tests more than the other groups. However, we also found that the lower back and legs flexibilitydid not change significantly in HS and OPE groups except for the FP group, indicating a need for targeted exercises to improve flexibility.
Beneficial effects on emotional competence
Based on previous research, this study controlled for age and gender variables to provide a clearer understanding of how the interventions impacted the children’s emotional competence and social behavior.Intragroup comparisons showed no significant effects in social competence, anger aggression, and anxietywithdrawal in the three groups after the intervention compared with baseline data. However, anger aggression in the HS group was significantly lower than in the FP group after intervention. Further, the anxious-withdrawal score was significantly different among the three groups, with the scores of the HS and FP groups showing a significant decrease compared to the OPE group. Previous research has focused on the impact of interventions on young children’s social competence and socio-emotional competence; for example, studies have reported that structured play-based activities during recess have a positive impact on the development of preschool children’s social skills [61, 62] and that physical training has a significant positive effect on preschoolers’ social skill level [63, 64]; on the other hand, social-emotional competence refers to emotional and social competence working together towards adaptive behaviour [65]. No significant changes in social competence were found in this study, which may be due to insufficient intervention time, or excessive emphasis on safe social distancing in both teaching strategies and the daily health care atmosphere during the pandemic, which affected children’s social development. Rodrigues et al.‘s [41] systemic review suggested that there was an absence of research evidence on the effects of exercise on anger/aggression and anxiety/withdrawal, and highlighted that of all the body-oriented interventions, play programmes received the most research attention and exhibited the highest efficacy in fostering social-emotional development. Free play is a prevalent form of play that enables children to explore their bodies and experience emotional changes [41]. In contrast, pretend play, which involves children taking on different roles and scenarios, is thought to develop emotion comprehension and regulation and prosocial behaviour [66, 67]. Pretend play is considered an activity that is more often engaged in by 5-year-olds in the context of free play [66]. In our FP group, free play, including pretend play and other spontaneous activities, was the main form of physical activity for children and occurred in a more relaxed environment, which may be beneficial for reducing anxiety and withdrawal. However, similar to Chinekesh et al.‘s study [68], structured group games in the HS groups also improved emotional abilities. It has been proposed that motor skill levels in infancy and early childhood predict anxiety levels during the school-age period [69]. Children with higher levels of motor skills may exhibit greater self-belief. The research further indicates that motor skills intervention can enhance children’s self-beliefs, consequently reducing psychological issues such as anxiety [70]. This, to some extent, explains the potential reasons behind the HS intervention.
Broadly, this study compared three mainstream PE models in Chinese preschools to evaluate their impact on child physical health and emotional competence development. The strengths of this study included its quasi-experimental design, which allowed for a more controlled comparison of the different interventions, reflecting real-world applicability. Additionally, the comprehensive assessment of both physical fitness and emotional competence provided a holistic view of the children’s development. Moreover, focusing on a preschool population highlighted the critical period for development and underscored the potential long-term benefits of early physical education interventions.However, several limitations must be addressed: (1) the subjective scale (SCBE-30) can be influenced by social desirability biases or inaccurate perceptions; (2) the study did not extensively account for potential confounding factors that may influence the outcomes, such as prior exposure to physical education or variations in teaching quality among different educators; (3) the long-term sustainability and durability of the observed benefits have not been thoroughly explored; and (4)this study focuses on a specific region in China, it may be limited in generalisability to other populations or settings. Long-term follow-up studies would provide more insight into the lasting effects of the intervention and reveal the underlying mechanism. Additionally, investigating the integration of effective physical exercise programmes into preschool curricula holds the potential for promoting holistic development.
Conclusions
In summary, this study compared three mainstream physical education models in Chinese preschools, focusing on the efficacy of the “Hello Sunshine” physical education program. The results indicate that structured ball skills training not only promotes physical health but also significantly reduces anxiety in children. This finding underscores the potential of integrating effective physical exercise programs into preschool curricula to foster holistic development.
Data availability
The data are available from the corresponding author upon reasonable request.
Abbreviations
- PA:
-
Physical activity
- FMS:
-
Fundamental movement skills
- PE:
-
Physical education
- HS group:
-
“Hello Sunshine” programme group
- OPE group:
-
Ordinary physical education group
- FP:
-
Free play group
- SCBE:
-
Social competence and behavior evaluation scale
References
GBD 2015 Obesity Collaborators. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377:13–27.
World Health Organization, Obesity. and overweight. 2021. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 16 May 2023.
Ortega FB, Ruiz JR, Castillo MJ, Sjöström M. Physical fitness in childhood and adolescence: a powerful marker of health. Int J Obes (Lond). 2008;32:1–11.
Corbin CB, Castelli DM, Sibley BA, Masurier GCL. Fitness for life. 7th edition. CHAMPAIGN, USA: Human Kinetics; 2021.
Fühner T, Kliegl R, Arntz F, Kriemler S, Granacher U. An update on secular trends in physical fitness of children and adolescents from 1972 to 2015: a systematic review. Sports Med. 2021;51:303–20.
Reilly JJ, Aubert S, Brazo-Sayavera J, Liu Y, Cagas JY, Tremblay MS. Surveillance to improve physical activity of children and adolescents. Bull World Health Organ. 2022;100:815–24.
Tu C, Pan Q, Jiang C, Tu Y, Zhang S. Trends and predictions in the physical shape of Chinese preschool children from 2000 to 2020. Front Public Health. 2023;11:1148415.
Li F, Yin L, Sun M, Gao Z. Examining relationships among Chinese preschool children’s meeting 24-hour movement guidelines and fundamental movement skills. JCM. 2022;11:5623.
China Institute of Sport Science. Fifth National Physical Fitness Monitoring Bulletin. 2021. https://www.ciss.cn/zhxw/info/2021/32028.html. Accessed 14 May 2023.
Serrano-Gallén G, Arias-Palencia NM, González-Víllora S, Gil-López V, Solera-Martínez M. The relationship between physical activity, physical fitness and fatness in 3–6 years old boys and girls: a cross-sectional study. Transl Pediatr. 2022;11:1095–104.
Li Y, Zhou T, Lu Y, Sang M, Liu J, He X, et al. The association between the health-related physical fitness and inhibitory control in preschool children. BMC Pediatr. 2022;22:106.
Wick K, Kriemler S, Granacher U. Associations between measures of physical fitness and cognitive performance in preschool children. BMC Sports Sci Med Rehabil. 2022;14:80.
Kirschbaum S, McCollister C, Drake-Croft J, O’Neal L. Social and emotional competence– why it’s vital for life success. United States: Tennessee Commission on Children and Youth; 2018.
Li Q, Liu P, Yan N, Feng T. Executive function training improves emotional competence for preschool children: the roles of inhibition control and working memory. Front Psychol. 2020;11:347.
Denham SA, Blair KA, DeMulder E, Levitas J, Sawyer K, Auerbach-Major S, et al. Preschool emotional competence: pathway to social competence? Child Dev. 2003;74:238–56.
LaFreniere P, Masataka N, Butovskaya M, Chen Q, Auxiliadora Dessen M, Atwanger K, et al. Cross-cultural analysis of social competence and behavior problems in preschoolers. Early Educ Dev. 2002;13:201–20.
Chen Q, Jiang Y. Social competence and behavior problems in Chinese preschoolers. Early Educ Dev. 2002;13:171–86.
Bart O, Hajami D, Bar-Haim Y. Predicting school adjustment from motor abilities in kindergarten. Infant Child Dev. 2007;16:597–615.
Trentacosta CJ, Izard CE. Kindergarten children’s emotion competence as a predictor of their academic competence in first grade. Emotion. 2007;7:77–88.
Alwaely SA, Yousif NBA, Mikhaylov A. Emotional development in preschoolers and socialization. Early Child Dev Care. 2021;191:2484–93.
Kendziora K, Osher D. Promoting children’s and adolescents’ social and emotional development: district adaptations of a theory of action. J Clin Child Adolesc Psychol. 2016;45:797–811.
Eime RM, Young JA, Harvey JT, Charity MJ, Payne WR. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: informing development of a conceptual model of health through sport. Int J Behav Nutr Phys Act. 2013;10:98.
Ransford CP. A role for amines in the antidepressant effect of exercise: a review. Med Sci Sports Exerc. 1982;14:1–10.
Voss MW, Nagamatsu LS, Liu-Ambrose T, Kramer AF. Exercise, brain, and cognition across the life span. J Appl Physiol (1985). 2011;111:1505–13.
Chan JSY, Liu G, Liang D, Deng K, Wu J, Yan JH. Special issue - therapeutic benefits of physical activity for mood: a systematic review on the effects of exercise intensity, duration, and modality. J Psychol. 2019;153:102–25.
Chaddock L, Erickson KI, Prakash RS, Kim JS, Voss MW, VanPatter M, et al. A neuroimaging investigation of the association between aerobic fitness, hippocampal volume, and memory performance in preadolescent children. Brain Res. 2010;1358:172–83.
Di Bartolomeo G, Papa S. The effects of physical activity on social interactions: the case of trust and trustworthiness. J Sports Econ. 2019;20:50–71.
Schoemaker MM, Kalverboer AF. Social and affective problems of children who are clumsy: how early do they begin? Adapted Phys Activity Q. 1994;11:130–40.
Piek JP, Bradbury GS, Elsley SC, Tate L. Motor coordination and social–emotional behaviour in preschool-aged children. Int J Disabil Dev Educ. 2008;55:143–51.
Chen C, Ahlqvist VH, Henriksson P, Magnusson C, Berglind D. Preschool environment and preschool teacher’s physical activity and their association with children’s activity levels at preschool. PLoS ONE. 2020;15:e0239838.
Brown WH, Googe HS, McIver KL, Rathel JM. Effects of teacher-encouraged physical activity on preschool playgrounds. J Early Intervention. 2009;31:126–45.
Krombholz H. The impact of a 20-month physical activity intervention in child care centers on motor performance and weight in overweight and healthy-weight preschool children. Percept Mot Skills. 2012;115:919–32.
Wang G, Zeng D, Zhang S, Hao Y, Zhang D, Liu Y. The effect of different physical exercise programs on physical fitness among preschool children: a cluster-randomized controlled trial. Int J Environ Res Public Health. 2023;20:4254.
Zhou L, Liang W, He Y, Duan Y, Rhodes RE, Lippke S, et al. A school-family blended multi-component physical activity program for Fundamental Motor Skills Promotion Program for obese children (FMSPPOC): protocol for a cluster randomized controlled trial. BMC Public Health. 2023;23:369.
Zhou Z, Ren H, Yin Z, Wang L, Wang K. A policy-driven multifaceted approach for early childhood physical fitness promotion: impacts on body composition and physical fitness in young Chinese children. BMC Pediatr. 2014;14:118.
Wick K, Kriemler S, Granacher U. Effects of a strength-dominated exercise program on physical fitness and cognitive performance in preschool children. J Strength Cond Res. 2021;35:983–90.
Robinson LE, Veldman SLC, Palmer KK, Okely AD. A ball skills intervention in preschoolers: the CHAMP randomized controlled trial. Med Sci Sports Exerc. 2017;49:2234–9.
Popović B, Cvetković M, Mačak D, Šćepanović T, Čokorilo N, Belić A et al. Nine months of a structured multisport program improve physical fitness in preschool children: a quasi-experimental study. Int J Environ Res Public Health. 2020;17.
Mačak D, Popović B, Babić N, Cadenas-Sanchez C, Madić DM, Trajković N. The effects of daily physical activity intervention on physical fitness in preschool children. J Sports Sci. 2022;40:146–55.
Dias Rodrigues A, Cruz-Ferreira A, Marmeleira J, Veiga G. Effects of body-oriented interventions on preschoolers’ social-emotional competence: a systematic review. Front Psychol. 2021;12:752930.
Dias Rodrigues A, Cruz-Ferreira A, Marmeleira J, Laranjo L, Veiga G. Which types of body-oriented interventions promote preschoolers’ social-emotional competence? A systematic review. Healthc (Basel). 2022;10:2413.
Wang X, Xiong W. Physical education in early childhood education and care in China. In: Antala B, Demirhan G, Carraro A, Oktar C, Oz H, Kaplánová A, editors. Physical Education in Early Childhood Education and Care researches -Best practices -Situation. Bratislava, Slovakia: Slovak Scientific Society for Physical Education and Sport and FIEP; 2019.
Barnett LM, Stodden D, Cohen KE, Smith JJ, Lubans DR, Lenoir M, et al. Fundamental movement skills: an important focus. J Teach Phys Educ. 2016;35:219–25.
Seefeldt V. Developmental motor patterns. Implications for elementary school physical education. In: Nadeau CH, Halliwell WR, Newell KM, Roberts GC, editors. Psychology of motor behavior and sport. Champaign: Human Kinetics(Verlag); 1980. pp. 314–23.
Donath L, Faude O, Hagmann S, Roth R, Zahner L. Fundamental movement skills in preschoolers: a randomized controlled trial targeting object control proficiency. Child Care Health Dev. 2015;41:1179–87.
Altunsöz IH, Goodway JD. SKIPing to motor competence: the influence of project successful kinesthetic instruction for preschoolers on motor competence of disadvantaged preschoolers. Phys Educ Sport Pedagogy. 2016;21:366–85.
Westendorp M, Houwen S, Hartman E, Mombarg R, Smith J, Visscher C. Effect of a ball skill intervention on children’s ball skills and cognitive functions. Med Sci Sports Exerc. 2014;46:414–22.
Wu H, Eungpinichpong W, Ruan H, Chen W, Yang Y, Dong X. Towards sustainable early education practices: a quasi-experimental study on the effects of kindergarten physical education programs on fundamental movement skills and self-regulation in Haikou city. China Sustain. 2024;16:1400.
Liu Y, Song Y, Liang Z. Evaluation of social competence and behavior of urban children in China. J Southeast Univ (Med Sci Edi). 2012;31:268–73.
State Sport General Administration. The National Physical Fitness Measurement Standards Manual (Preschool children Version). 2003. http://www.sport.gov.cn/n16/n41308/n41323/n41345/n41426/n42527/n42587/171330.html. Accessed 26 Feb 2020.
LaFreniere PJ, Dumas JE. Social competence and behavior evaluation in children ages 3 to 6 years: the short form (SCBE-30). Psychol Assess. 1996;8:369–77.
Goldfield GS, Harvey A, Grattan K, Adamo KB. Physical activity promotion in the preschool years: a critical period to intervene. Int J Environ Res Public Health. 2012;9:1326–42.
Lima RA, Bugge A, Ersbøll AK, Stodden DF, Andersen LB. The longitudinal relationship between motor competence and measures of fatness and fitness from childhood into adolescence. Jornal De Pediatria (Versão em Português). 2019;95:482–8.
State Council Gazette No. 12 of 2016. Kindergarten Work Regulations. https://www.gov.cn/gongbao/content/2016/content_5067918.htm. Accessed 30 Jul 2024.
Roth K, Kriemler S, Lehmacher W, Ruf KC, Graf C, Hebestreit H. Effects of a physical activity intervention in preschool children. Med Sci Sports Exerc. 2015;47:2542–51.
Liu J, Gao F, Yuan L. Effects of diversified sports activity module on physical fitness and mental health of 4–5-year-old preschoolers. Iran J Public Health. 2021;50:1233–40.
Behan S, Belton S, Peers C, O’connor NE, Issartel J. Exploring the relationships between fundamental movement skills and health related fitness components in children. Eur J Sport Sci. 2022;22:171–81.
Liu C, Cao Y, Zhang Z, Gao R, Qu G. Correlation of fundamental movement skills with health-related fitness elements in children and adolescents: a systematic review. Front Public Health. 2023;11:1129258.
Lubans DR, Morgan PJ, Cliff DP, Barnett LM, Okely AD. Fundamental movement skills in children and adolescents: review of associated health benefits. Sports Med (Auckland NZ). 2010;40:1019–35.
Stodden DF, Goodway JD, Langendorfer SJ, Roberton MA, Rudisill ME, Garcia C, et al. A developmental perspective on the role of motor skill competence in physical activity: an emergent relationship. Quest. 2008;60:290–306.
Loukatari P, Matsouka O, Papadimitriou K, Nani S, Grammatikopoulos V. The effect of a structured playfulness program on social skills in kindergarten children. Int J Instruction. 2019;12:237–52.
Tersi M, Matsouka O. Improving social skills through structured playfulness program in preschool children. Int J Instruction. 2020;13:259–74.
Lobo YB, Winsler A. The effects of a creative dance and movement program on the social competence of Head Start preschoolers. Soc Dev. 2006;15:501–19.
Ozyurek A, Ozkan I, Begde Z. N.F.Yavuz. Effects of physical training on social skill levels of preschool children. JSS. 2015;3:282–9.
Ma R, Lin M, Song H, Pang J, Ma D, Zhang L, et al. Effects of movement skill development on behavioral self-regulation ability of preschool children. China Sport Sci. 2019;39:40–7.
Richard S, Gay P, Clerc-Georgy A, Gentaz É. Evaluation of a training program based on pretend play designed to promote the development of socioemotional skills in five-year-old children: an exploratory study. L’Année Psychologique. 2019;119:291–332.
Richard S, Baud-Bovy G, Clerc-Georgy A, Gentaz E. The effects of a pretend play-based training designed to promote the development of emotion comprehension, emotion regulation, and prosocial behaviour in 5- to 6-year-old Swiss children. Br J Psychol. 2021;112:690–719.
Chinekesh A, Kamalian M, Eltemasi M, Chinekesh S, Alavi M. The effect of group play therapy on social-emotional skills in pre-school children. Glob J Health Sci. 2014;6:163–7.
Piek JP, Barrett NC, Smith LM, Rigoli D, Gasson N. Do motor skills in infancy and early childhood predict anxious and depressive symptomatology at school age? Hum Mov Sci. 2010;29:777–86.
Bremer E, Cairney J. Fundamental movement skills and health-related outcomes: a narrative review of longitudinal and intervention studies targeting typically developing children. Am J Lifestyle Med. 2016;12:148–59.
Acknowledgements
The authors would like to extend their heartfelt gratitude to the children, their teachers and testers for their involvement and cooperation in this study. We would also like to extend our gratitude to Associate Professor Zhou Junmei from the School of Mathematics and Statistics, Hainan Normal University, for her diligent efforts in creating the forest plot for this article. We would like thanks to Asst. Prof. Dr. Kurusart Konharn of the faculty of Associated Medical Sciences of Khon Kaen University for his valuable advice.
Funding
This research was funded by the Fundamental Fund of KhonKaen University and has received funding support from the National Science, Research and Innovation Fund (NSRF). Project No.SD-65-023 and Hainan Province Philosophy and Social Science Planning Project (HNSK(YB)23–57).Informed consent was obtained from all subjects involved in the study.
Author information
Authors and Affiliations
Contributions
H.W.:conceptualization, methodology, writing—original draft; H.R.: preparation, data curation; W.E.: conceptualization, reviewing; W.L.: investigation and data collection.All authors have read and agreed to the published version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Institutional Review Board Statement: We confirm that informed consent was obtained from the legally authorized representatives (LARs) or next of kin of all minors (less than 16 years of age) who participated in the study. The LARs or next of kin were provided with detailed information about the study, including its purpose, procedures, risks, and benefits, and gave their voluntary and informed consent on behalf of the minors. All LARs or next of kin were informed that participation in the study was entirely voluntary and that they could withdraw their consent at any time. The study was conducted in accordance with the Declaration of Helsinki and approved by KhonKaen University Ethics Committee for Human Research (HE642100).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wu, H., Ruan, H., Eungpinichpong, W. et al. The effects of physical exercise on fitness and emotion in Chinese preschoolers. BMC Public Health 24, 2407 (2024). https://doi.org/10.1186/s12889-024-19895-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19895-8