
Abstract
Background
The benefits of exclusive breastfeeding (EBF) have been universally documented, with evidence of positive impacts on a child’s optimal growth, development, and survival. However, EBF practices in Nepal have fluctuated and declined over the last 25 years. In addition to the individual factors of mothers and infants, EBF practices are affected by multiple community-level factors. Understanding these factors is essential for designing breastfeeding promotion programs to improve child nutritional status in Nepal. This study investigated the individual- and community-level determinants of EBF practices among young infants aged 0–5 months in Nepal.
Method
We used the dataset from the Nepal Demographic and Health Survey 2022. Information on EBF in the past 24 h was available for 540 infants aged 0–5 months. A multilevel mixed-effect logistic regression was used to identify individual- and community-level factors associated with EBF among infants aged 0–5 months in Nepal.
Results
The 24-hour prevalence of EBF among infants aged 0–5 months was 57.46% (95% confidence interval (CI): 52.18, 62.57). The infant’s age was inversely associated with EBF prevalence at the individual level. Compared with infants aged < 1 month, infants aged three months (adjusted odds ratio (AOR): 0.14, 95% CI: 0.05, 0.40), four months (AOR: 0.11, 95% CI: 0.04, 0.28), and five months (AOR: 0.07, 95% CI: 0.03, 0.20) were less likely to receive EBF. At the community level, community-level variables such as ≥ 4 ANC visits coverage, maternal employment status, and poverty level were generated by aggregating the individual characteristics in a cluster and were categorized using quartiles into low (“< 25%”), moderate (25–75%), and high (≥ 75%). Mothers from communities with moderate ≥ 4 ANC visits (AOR: 3.30, 95% CI: 1.65, 6.57) and high ≥ 4 ANC visits (AOR: 2.70, 95% CI: 1.40, 5.22) coverage had higher odds of EBF practices than did those from communities with low ≥ 4 ANC visits coverage. Similarly, communities with moderate (AOR: 2.67, 95% CI: 1.34, 5.30) and high (AOR: 2.34, 95% CI: 1.10, 4.99) levels of maternal employment status and moderate levels of poverty (AOR: 2.20, 95% CI: 1.13, 4.28) were associated with a higher likelihood of EBF practices. Subnational level variation was evident, with infants in Lumbini province having lower odds of EBF (AOR: 0.32, 95% CI: 0.13, 0.77) relative to Koshi province. Approximately 9% of the variation in EBF practices was observed among mothers while mapping across clusters in this study.
Conclusion
Various individual- and community-level factors influence the uptake of EBF in Nepal, underscoring the need to improve the approaches and strategies of EBF programs. This study highlighted the significant association of community-level factors (≥ 4 ANC visits coverage, poverty level, and maternal employment status) with EBF among infants under 6 months. It revealed approximately 9% variability in EBF across clusters. Future efforts to promote EBF should focus on older infants and communities with low poverty levels and low coverage of recommended ≥ 4 ANC visits. Furthermore, context-specific adaptation of such efforts might be required considering the variation observed between the communities in the present study.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
“Exclusive breastfeeding (EBF) refers to feeding an infant only breast milk for the first six months of life, without any additional food or drink, not even water, except for oral rehydration solutions, or drops/syrups of vitamins, minerals, or medicines” [1]. The benefits of EBF are well documented. EBF helps establish the infant gut microbiome, helps maintain body temperature, and provides immunity to a newborn [2]. Breastmilk is sufficient to provide all essential nutrients during the first six months of an infant’s life, and its nutritional benefits extend beyond this period. It boosts the immune system and protects against common childhood illnesses such as diarrhea, lower and upper respiratory tract infections, pneumonia and asthma, otitis media, and associated hospitalization [3,4,5]. Breastfeeding has also been associated with stronger bonding between mothers and babies and long-term benefits such as reducing the risk of overweight/obesity, type 2 diabetes, and chronic leukemia later in life [1, 6, 7]. EBF is considered the most effective intervention for reducing infant mortality and is estimated to prevent up to 13% mortality among children aged less than 5 years in low- and middle-income countries [LMICs] [8]. Furthermore, breastfeeding offers maternal benefits, including a reduced risk of postpartum depression, breast and ovarian cancer, and obesity. It also provides contraceptive benefits by inducing lactational amenorrhea. However, this approach is considered poor and unreliable [9].
The World Health Organization (WHO) recommends breastfeeding within an hour of birth, establishing and maintaining EBF practices for the first six months of a newborn’s life, and breastfeeding until two years [10, 11]. The prevalence of EBF among infants aged 0–5 months has reached 48% globally by 2023, close to the 2025 target of 50% [12]. However, there is wide variation in the prevalence of EBF practices across the continent, ranging from 26% in North America to 60% in South Asia. The WHO expects that all member states achieve EBF in the first six months of an infant’s life of 70% by the end of 2030 [12].
Nepal has set a target to achieve ≥ 90% EBF among infants aged 0–5 months by 2030 [13]. The prevalence of EBF among infants aged 0–5 months (i.e., infants under six months) varied significantly during different time periods. In 1996, the prevalence was relatively high at 75% [14]. By 2006, it had fallen sharply to 53%. The situation improved by 2011, with the prevalence increasing to 70%. This improvement was not sustained, as the rate dropped slightly to 66% in 2016 and markedly to 56% in 2022. Unless some major initiatives are implemented and sustained, it is unlikely that Nepal will reach the EBF target of ≥ 90% prevalence by 2030 [14]. The government of Nepal has made considerable efforts to promote, protect, and support breastfeeding, emphasizing several policies, strategies, acts, and programs. The government of Nepal enacted the Breast Milk Substitute (BMS) (Control of Sale and Distribution) Act in 1992 to regulate breast milk substitutes and the sale and distribution of infant foods [15, 16]. Following the WHO and UNICEF global initiatives of Baby Friendly and Hospital Initiative (BFHI) to protect, promote, and support breastfeeding in the 1990s, Nepal introduced BFHI activities in 1994 [17]. By 1996, under this initiative, health workers from 22 different hospitals nationwide were provided training [17]. However, only seven of the hospitals were accredited as baby-friendly hospitals following evaluation in 1997–1998 by the Nepal Pediatric Society [17]. Later, the Government of Nepal rolled out the Mother Baby Friendly Health Initiative (MBFHI) in 22 hospitals by November 2023, guided by the MBFHI guidelines endorsed almost a decade ago in 2017 [18, 19]. The MBFHI was on the initiation of the International Federation of Gynaecology and Obstetrics’ Safe Motherhood and Newborn Health Committee, which collaborated with the International Pediatric Association, the International Confederation of Midwives, the White Ribbon Alliance, and the WHO to develop criteria for certifying a facility as “Mother and Baby Friendly” and focused on labour, delivery, and postpartum practices in 2014 [20]. It is expected to be further scaled up in all provincial hospitals by 2025/2026, which began in 2019/2020 [21]. In addition to hospital-based initiatives, breastfeeding promotion activities are conducted at the community level via an extensive network of more than 48,000 female community health volunteers who receive training in promoting and supporting breastfeeding. The Ministry of Health and health facilities from the tertiary to the community level also conduct various activities during breastfeeding weeks [19]. Health workers working at community-level facilities are provided 7 days of comprehensive nutrition-specific intervention training, which includes a dedicated session on supporting mothers in breastfeeding their newborns. In addition, they receive community-based integrated management of neonatal and childhood illness, which includes focused training to support mothers in breastfeeding their newborns [22]. Despite these efforts, there has been fluctuation and decline in EBF over the past two decades [14, 23, 24].
The factors that influence EBF practices are multilayered. Several individual-level factors have been reported to influence EBF practices in LMICs: the infant’s age [25,26,27], household socioeconomic status [28, 29], maternal education [30, 31], preterm birth [28], maternal employment [30, 32], childbirth by cesarean Sects. [28, 33,34,35], parity [27, 36], antenatal and postnatal visits [28, 36, 37], place of childbirth [32, 38], provision of maternity leave [38], and ethnicity [34]. At the community level, EBF practices are influenced by the place of residence, maternal education, antenatal care (ANC) and postnatal care (PNC) visits, maternal employment status, poverty level, and media exposure [32, 35, 39,40,41,42]. Previous studies conducted in Nepal have examined the prevalence and predictors of EBF practices. Nevertheless, these studies were confined to specific geographical areas [35, 43, 44] or did not consider the influence of community-level factors (e.g., neighborhoods and municipalities) [27] where mother-child pairs were nested. The independent assumption of individuals within the cluster and equal variance in outcomes across the cluster is often violated in the hierarchical data of the Nepal Demographic and Health Survey (NDHS). Moreover, community-level factors are as important as individual factors are, and they provide insights into broader social, cultural, and environmental contexts that influence individual breastfeeding practices, which have not been previously identified via stronger statistical methods.
This study aimed to determine the individual- and community-level factors associated with EBF among infants under six months via multilevel mixed-effect logistic regression analysis. These findings will inform policymakers, implementers, and stakeholders about the individual- and community-level factors associated with low EBF and guide the development of context-specific targeted programs.
Methods
Data sources
The study used data from the NDHS 2022, a cross-sectional, population-based, and nationally representative study. The details of the NDHS 2022 can be obtained from the extant literature [14]. In the first stage, 476 primary sampling units (PSUs) were selected using probability proportional to size, with 248 PSUs from urban areas and 228 PSUs from rural areas covering all seven provinces. In the second stage, 30 households were selected systematically from each PSU, resulting in a total sample size of 14,280 households, consisting of 7,440 urban and 6,840 rural households. From these sampled households, 540 (unweighted) respondents (15–49 years old) whose youngest children lived with their mothers and aged 0–5 months were chosen as the analytical sample for this study. We used the children’s recode (KR) and individual’s recode (IR) datasets, which are publicly available [45], and followed the instructions from the DHS guide for analysis [46]. The response rate of the NDHS 2022 at the household level was 99%, and that at the women’s level was 97% [14].
Variables
Outcome variables
The NDHS defines EBF among infants aged 0–5 months as “an infant receiving only breast milk, no other liquids or solids are given, not even water, except oral rehydration solution or drops/syrups of vitamins, minerals or medicines.” The survey asked if the infant had breastfed breastmilk in the last 24 h, and a list of common food items was also read to assist mothers with their recall. If the mother reported providing breastfeeding only (except for ORS and medicine), it was classified as 1 = exclusive breastfeeding; otherwise, 0 = non-exclusive breastfeeding.
Explanatory variables
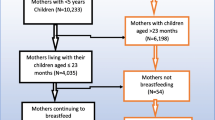
The evidence indicates the influence of multiple factors, such as individual, family, socioeconomic, and community factors, on breastfeeding practices [36, 47]. This study included two sets of explanatory variables (individual and community levels). The conceptual framework (Fig. 1) depicts the effects of these two levels of determinants on EBF practices. Different levels of factors considered for the study are explained briefly below.

Conceptual framework of determinants of exclusive breastfeeding among infants aged 0–5 months
Individual-level variables
Infant-related and maternal (sociodemographic, socioeconomic, obstetric, and maternal health service-related characteristics) variables were included in this study. Infant-related variables include the infant’s age, sex, birth weight, morbidities in the past two weeks, preceding birth interval, and breastfeeding initiation time. The maternal sociodemographic and socioeconomic variables used in the study were maternal age, caste/ethnicity, maternal employment, wealth index, media exposure, number of under-five children, household size, and maternal education. Maternal obstetrics and health service-related variables included parity, childbirth assistance, PNC check-ups within 2 days, and cesarean section childbirth. Details about the categories of individual-level variables are provided in Supplementary Table 1. The household wealth index used in the NDHS 2022 [14, 48] was further recategorized into three categories recommended by the World Bank Poverty Network and UNICEF [49] and used in an earlier similar study [50]. The bottom 40% of the households were referred to as poor, the next 40% as middle, and the top 20% as the richest.
Community-level variables
The study respondent’s place of residence, province, and ecological zone were nonaggregate community-level variables. Furthermore, community-level variables were generated by aggregating the individual characteristics in a cluster since NDHS does not directly gather data that can define the attributes of individual clusters except for the place of residence, province, and ecological zone. The aggregates were derived using the proportion of selected sub-categories of provided individual-level variables (maternal education, media exposure, ANC ≥ 4 visits, PNC check-up, maternal employment, infant morbidity). Since the aggregate values of all the generated variables were not normally distributed, they were categorized into groups (low, moderate, and high) based on the median value aligned with previously published studies [47].
Community antenatal care (ANC) coverage was the proportion of mothers within specific clusters who accomplished ≥ 4 visits. It was categorized using quartiles into low ANC using the community (when < 25% of mothers were attending ≥ ANC 4 visits), moderate ANC (when two of the middle quartiles (25–75%) of mothers were attending ≥ ANC 4 visits), and high ANC (when ≥ 75% of mothers were seeking ≥ ANC 4 visits) [47]. Community PNC check-up coverage was the proportion of mothers within specific clusters who received PNC within two days of childbirth. It was categorized into quartiles into low PNC service using the community (when < 25% of mothers were attending PNC check-ups within two days), moderate PNC service (when two of the middle quartiles (25–75%) of mothers were attending PNC check-up within two days), and high PNC service (when ≥ 75% of mothers were seeking PNC check-up within two days) [47].
The community level of media exposure was an aggregate respondent level exposure for different media types, which was categorized as “< 25%= Low,” “25–75% = Moderate,” and “≥ 75% = high” media using communities [47]. The community poverty level was the proportion of mothers within a specific cluster in either the poorest or poor wealth quintile. It was categorized based on quartiles: low poverty level (when < 25% of mothers were either poorest or poor), moderate poverty level (when two of the middle quartiles (25–75%) of mothers were either poorest or poor), and high poverty level (when ≥ 75% of the mothers were either poorest or poor) [47].
The community education level was the proportion of mothers within a specific cluster with secondary or higher education. It was categorized using quartiles into low education community (when < 25% of mothers had attended secondary or higher education), moderate education community (when two of the middle quartiles (25–75%) of mothers had attended either secondary or higher education), and high education community (when ≥ 75% of mothers had attended either secondary or higher education) [47]. The community maternal employment status was the proportion of mothers within a specific cluster currently engaged in work. It was causing quartiles into low maternal employment community (when < 25% of mothers were currently working), moderate maternal employment community (when two of the middle quartiles (25–75%) of mothers were currently working), and high maternal employment community (when ≥ 75% of mothers were currently working) [41, 47].
Statistical analyses
Descriptive statistics, including frequency, percent distribution, and the prevalence of EBF, were derived via the NDHS guidelines [14, 46]. To determine the factors associated with EBF, it is essential to consider the hierarchical structure of NDHS data, where individual children are nested within households and households within clusters/primary sample units. This hierarchical nature indicates that using a conventional logistic regression model may underestimate the standard error of the estimates [51, 52]. Furthermore, it is assumed that children’s socioeconomic characteristics from the same clusters are considered similar relative to those from another cluster. This violates the assumptions of conventional logistic regression models, such as the independence of observations and equal variance across clusters [51, 52]. Therefore, it was essential to account for cluster variability in this study. The multilevel logistic regression model was fitted to simultaneously estimate fixed (individual- and community-level effects) and random effects (cluster variation) [41, 51, 53].
Four models were considered in the multilevel logistic regression analysis to assess the model that fit the data well. Model 1 (null model), without any explanatory variables, was fitted to evaluate the null hypothesis that there were no cluster-level differences in EBF that specified only random intercepts and presented total variance in the EBF across clusters. Model 2 adjusted the explanatory variables individually, assuming that no cluster-level differences in EBF existed. Model 3 was adjusted for community-level factors by aggregating cluster-level differences in EBF practices. Model 4 considered both individual- and community-level variables simultaneously.
The log of the probability of EBF was modeled via a multilevel mixed-effect logistic regression model via the following equation [53]:
where \(\:i\) and \(\:j\) refer to levels 1 (individual) and 2 (community/cluster/PSU units), respectively. Clusters were considered using the previously established ward (community)-level categorization. \(\:\mathcal{X}\) and \(\:Z\) refer to individual- and community-level variables, respectively. \(\:{\pi\:}_{ij}\) is the probability of exclusive breastfeeding for \(\:{i}^{th\:}\)infants in the \(\:{j}^{th}\) community; \(\:\beta\:\) is the fixed effect coefficient. Whereas \(\:{\beta\:}_{0}\) represents the intercept, i.e., the effect on the probability of EBF in the absence of effects of explanatory variables, \(\:{\mu\:}_{j}\) represents the random effect (effect of community on EBF) for \(\:{j}^{th}\), and \(\:{e}_{ij}\) denotes the random error at the individual level. Each community/cluster/PSU is assumed to have a different intercept (\(\:{\beta\:}_{0})\) and fixed coefficient (\(\:\beta\:)\), hierarchical and clustered data, and variations within and between communities. The multilevel mixed effect logistic regression model used for analysis produced unexplained variation in EBF due to unobserved cluster factors called random effects. All four models incorporated a random intercept at the cluster level to reflect cluster heterogeneity.
The variation in EBF at the community level (random effect) was estimated by computing the intraclass correlation (ICC) coefficient, and an ICC value greater than 5% was considered sufficient for performing multilevel mixed-effect modeling [53]. The higher the ICC (ICC > 5%), the greater the importance the community-level variable has in understanding the individual-level variation in EBF practices [53]. We also calculated the median odds ratio (MOR) and proportional change in variance (PCV) to measure the variation in EBF practices across the community [51]. In our study, MOR represents the extent to which the characteristics of a residential area determine the individual probability of being exclusively breastfed. The PCV [PCV= (VA-VB)/VA*100] measures the total variation attributed to individual and community-level variables in multilevel modeling [51]. Variables with p value < 0.25 in the multilevel univariate analysis were further considered candidate variables for multivariable mixed-effect logistic regression analysis [54]. The predictive effects of explanatory variables (fixed effects) were measured via adjusted odds ratios (AORs) with 95% CIs. Akaike’s information criterion (AIC) and log-likelihood values were derived to assess the goodness of fit of each model, and the model with the lowest AIC and highest log-likelihood value was considered the best-fit model. The multicollinearity between explanatory variables was checked via the variance inflation factor (VIF); none of the variables demonstrated multicollinearity problems (VIF > 5) [55]. Details about the VIF are presented in the supplementary Table 2. All the statistical tests applied were two-sided and considered significant at p < 0.05, and analyses were performed using STATA 18 (Stata Corporation, College Station, Texas, USA).
Results
Descriptive summary
Table 1 summarises the distribution of background characteristics of mother-infant pairs at the individual level by EBF practices. The average age of the infants in the analytical sample was 2.63 months, with a standard deviation of 1.74 months. The largest proportion of infants, approximately 20.1%, were in the 5-month age group, and approximately half (49.7%) were female. Approximately four out of five mothers belonged to the poor (41.6%) and middle (40.7%) wealth quintiles. More than half of the mothers (55.4%) were currently employed. Similarly, 50.7% of the women had secondary education or higher—most households (57%) had 6 to 26 family members. Over eight out of ten mothers (81.6%) attended ≥ 4 ANC visits for antenatal care. Similarly, most mothers, approximately 81.6%, had their childbirth at health facilities. Approximately one in five mothers had a cesarean birth (18.6%).
Table 1 also presents the estimated percentage of infants aged 0–5 months who were EBF by selected individual-level infant and maternal determinants. The estimated prevalence of EBF was 57.46% (N = 527, weighted). The proportion of exclusively breastfed infants less than one month was 81.2%, 61.2% at one month, 68.3% at two months, 57.4% at three months, 42.6% at four months, and 40.6% at five months. EBF prevalence was lower among male infants, very low birth weight babies, those with a preceding birth interval of more than 24 months, and those who did not begin breastfeeding early. Conversely, EBF practices were more common among mothers less than 20 years of age, those in poor households, those with no education, those with PNC check-ups within two days, those with spontaneous childbirth, and those with ≥ 4 ANC visits during pregnancy. However, based on univariate multilevel mixed-effect modeling, infant age was significantly associated with EBF among all individual-level determinants.
Table 2 summarises the community-level characteristics of the mother-infant pairs by EBF practices included in the study. Approximately two-thirds of the respondents (68.7%) were from urban areas, and approximately a similar proportion (62.2%) were from the Terai region. The highest proportion, approximately 44.5%, were from communities with low poverty levels, and approximately one-third of mothers (34.4%) were from communities with low literacy rates. Similarly, over one-third of mothers (37.1%) were from communities with high ≥ 4 ANC visits coverage. Almost 42.7% of the mothers were from communities with high maternal employment status. The EBF prevalence was lowest in Lumbini and communities with low poverty levels, low maternal employment, and low ANC ≥ 4 visits coverage.
Determinants of exclusive breastfeeding
The fixed effects (measures of association) and random effects (measures of variation) for EBF are presented in Table 3. The initial null model (Model 1) did not include any explanatory variables. The second model (Model 2) incorporated individual-level factors related to the infant and mother. The third model (Model 3) included only community-level factors, whereas the fourth model combined individual- and community-level factors. The fourth and final model (Model 4), which had the lowest AIC and highest log-likelihoods, was chosen to explain the measures of association and variation, as it fits the data well. This final model significantly associated one individual and four community-level variables with EBF.
The infant’s age was significantly associated with EBF at the individual level. The odds of EBF decreased with increasing infant age. The odds of EBF were significantly lower among infants in the 2nd (AOR: 0.26; 95% CI: 0.09, 0.75), 3rd (AOR: 0.35; 95% CI: 0.13, 0.94), 4th (AOR: 0.14; 95% CI: 0.05, 0.40), 5th (AOR: 0.11; 95% CI: 0.04, 0.28), and 6th (AOR: 0.07; 95% CI: 0.03, 0.20) months than in the first month of birth.
At the community level, four variables were significantly associated with EBF: province, poverty level, ANC ≥ 4 visits coverage, and maternal employment status (Model 4). After adjustments were made for other individual- and community-level covariates (Model 4). Compared with those from Koshi Province, infants from Lumbini Province were less likely (AOR: 0.32; 95% CI: 0.13, 0.76) to be exclusively breastfed. In contrast, infants from Sudurpaschim Province were more likely (AOR: 2.20; 95% CI: 1.13, 4.28) to receive exclusive breastfeeding. A community with moderate and high ≥ 4 ANC visits coverage was positively associated with EBF practices. Compared with their counterparts with low coverage, infants from the community with moderate coverage of ≥ 4 ANC visits (AOR: 3.30; 95% CI: 1.65, 6.57) and high coverage of ≥ 4 ANC visits (AOR: 2.70; 95% CI: 1.40, 5.22) had greater odds of EBF. The community poverty level was positively associated with EBF practices. Compared with infants living in a community with low poverty, those belonging to a community with a moderate level of poverty had greater odds (AOR: 2.20; 95% CI: 1.13, 4.28) of EBF. Community maternal occupation status was positively associated with EBF practices. Compared with infants from the community with a low level of maternal employment, those living in a community with moderate (AOR: 2.64, 95% CI: 1.34, 5.23) and high (AOR: 2.33, 95% CI: 1.10, 4.94) maternal employment status were more likely to be exclusively breastfed.
This study investigated the influence of community characteristics on EBF practices among infants aged 0–5 months. Multivariable multilevel mixed effect logistic regression analysis revealed Model 4 as the best model to fit the data based on the lowest AIC and highest log-likelihood value. In the initial null model, the ICC was 0.29, exceeding the threshold of 5%, with a variance of 1.33. These findings suggest that community-level determinants accounted for 29% of the variation in EBF practices.
The full model (Model 4), which adjusted for individual- and community-level determinants, revealed that the variation in EBF practices across clusters decreased to 9% (ICC = 0.09) from 29% (ICC = 0.29) in the null model. This model demonstrated a greater PCV, with 75.18% of the variation in EBF practices explained by the combined factors at the individual and community levels. The MOR for the null and final models were 3.01 and 1.70, respectively. In the null model, the MOR of a cluster with a high proportion of EBF was 3.01 times greater than that of a cluster with a low EBF. In contrast, the MOR at a cluster with a high proportion of EBF was 1.73 times higher than that at a cluster with a low proportion of EBF in the final selected model. Including individual and community-level covariates in the final model resulted in reduced unexplained cluster heterogeneity. Thus, there was reduced variation between the clusters in the propensity for EBF practices in the Model 4.
Discussion
This study revealed that the prevalence of EBF among children aged 0–5 months was 57.46%, and only 40.6% of those aged 5th months were exclusively breastfed. In the past 10 years, EBF practices have decreased markedly from 70% in 2011 to 56% in 2022 [24]. The government of Nepal has endorsed and implemented multiple policies and programs such as the National Nutrition Strategy (2004), the Infant and Young Child Feeding (IYCF) strategy of 2014, and the Multi-Sector Nutrition Plan-III (2023–2030), which prioritizes the promotion, protection, and support of early, exclusive, and extended breastfeeding to improve maternal and child health and nutrition [19]. However, the prevalence of EBF in our study was lower than in South Asia (61%) [12] and India (65%) [56], but it was higher than in Pakistan (48%) [57]. The factors contributing to the declining rate of EBF in Nepal may include the aggressive marketing of BMS [58], poor quality antenatal care [59,60,61], lack of skilled breastfeeding counseling in health facilities [59, 62], and sociocultural beliefs favoring mixed feeding [27, 34]. This finding indicates that the existing programs for the promotion, protection, and support of EBF practices need urgent attention, as most child deaths are attributed to suboptimal breastfeeding [62].
This paper explored the associations between individual- and community-level determinants of EBF practices. We observed that infant age was significantly associated with EBF practices among infants aged 0–5 months. The odds of EBF practices decreased with increasing age in our study. Some previous studies in Ethiopia, Timor-Leste, Nepal, India, and Tanzania also reported that higher age groups were negatively associated with EBF practices [27, 56, 63,64,65]. The previous 2016 NDHS also revealed a decline in EBF with increasing age. A comparison between these two surveys regarding the pattern of drop in EBF revealed that the proportion of infants exclusively breastfed during the NDHS 2022 deteriorated in all months, excluding the first twenty-nine days and the latter six months (see supplementary Table 3). This could be due to incorrect perceptions among mothers and caretakers about the inadequacy and insufficiency of breast milk in meeting the nutrient requirements of growing infants [66]. Moreover, this could be attributed to a lack of knowledge about the adverse implications of the early introduction of complementary feeding [27, 34, 50, 56, 67]. Understanding the common age at which EBF gradually subsides and ultimately stops can help design effective interventions, considering the infant’s age as a key determinant. This allows for concentrated efforts to encourage EBF practices and ensure they continue until the infant is six months old, as recommended.
At the community level, province, poverty level, maternal employment status, and ANC ≥ 4 visits coverage affected EBF practices after adjusting for the effects of individual-level variables. Community-level ANC ≥ 4 visits coverage had a greater influence on promoting EBF practices at the individual level. Two distinct direct and indirect mechanisms could explain these differences in association. Under the direct mechanism, health service providers might have offered the mother appropriate information about using subsequent maternal health services (such as institutional delivery and postnatal care), further promoting EBF [67]. In an indirect mechanism, there might have been a spillover effect since women receiving these services might share knowledge and experience with other women, positively influencing the adoption of EBF [67]. In Nepal, people often stay in clusters based on ethnicity, education, and wealth status [68]. Subsequently, women within the specific cluster consistently use health services similar to those health workers provide. In contrast, women in another cluster may not have access to similar health services, resulting in differences in EBF practices. This could be a key factor for the cluster disparity detected in this study, consistent with previously published studies [27, 34, 67].
Maternal employment status positively influenced individual-level EBF practices, even after adjustments were made for other individual and community variables, which aligns with the findings of another Ethiopian study. This could be attributed to more mothers engaged in agricultural work (39%) than professional white-collar work (4.5%). Agricultural work often involves a flexible work schedule and proximity of the workplace to home, which is beneficial for the effective continuation of breastfeeding [69]. Conversely, some studies from Indonesia [30], Latin America [70], and Ethiopia [71] did not report findings similar to ours.
Mothers living in communities with moderate and high levels of poverty were more likely to practice EBF. This was consistent with previous studies in Nepal [72] and Vietnam [73]. In contrast, other studies have shown that mothers with the richest wealth index practice EBF relative to the poorest wealth index [41, 74]. The low practice of EBF in communities with moderate and high levels of poverty could be that relatively poor communities have less access to breastmilk substitutes [73, 75]. Alternatively, another reason could be that mothers in relatively wealthier provinces might be more frequently exposed to aggressive marketing by infant formula companies. These companies target affluent communities due to the larger market for their products [73].
At the community level, lower odds of EBF were found among infants from Lumbini province than those from Koshi Province. Geographical variability in EBF practices has also been reported in other studies [26,27,28, 50, 67]. Despite its access to roads and other social services, including a relatively better human development index, Lumbini province has performed poorly in terms of most maternal and child health indicators [14, 76, 77], and it is unclear why this province has underperformed, signaling the need for further research.
Some important public health implications can be drawn from our findings. This analysis quantified the variability in the proportion of EBF practices at the community level, implying that mothers in adjacent geographical areas may not have similar breastfeeding practices and that Nepal is heterogeneous regarding breastfeeding practices. This also reflected that there could be sociocultural differences in communities that often influence EBF practices. Hence, studies can be further designed to examine how this variation operates in smaller regions to increase the proportion of mothers practicing EBF. Moreover, targeted interventions in these smaller areas can be developed and rolled out to meet the nutrition-related SDG 2030 targets. It is essential to identify what works for whom and under what circumstances, as well as the mechanisms that make some breastfeeding promotion strategies and interventions successful and not others. Nepal’s restructuring after federalism involved autonomy in decision-making and implementation in the social development sector, including health and nutrition at the local level, providing an excellent opportunity to support such context-specific interventions.
Despite its strengths, our study has several limitations. First, this study could not include important explanatory variables crucial for determining EBF practices, such as breastfeeding problems, encouragement to breastfeed, and breastfeeding information, due to their unavailability in this round of the NDHS, which were included in a previously published study [35]. Including this variable could influence the estimates of EBF prevalence and shift the understanding of how sociodemographic factors could play a role. The findings could have also provided more precise guidance for designing targeted policies and programs to assist breastfeeding mothers. Second, this cross-sectional study could not establish a causal relationship between EBF and the explanatory variables considered in the study. Third, estimates of EBF were based on the 24-hour recall method, which might have overestimated the proportion of EBF in this study [78]. However, this method is still acceptable in LMICs [79]. Fourth, this study articulates promotion only. Standalone promotion efforts may not address all existing barriers to EBF in the community. These barriers could include cultural beliefs and lack of access to breastfeeding support, which require a comprehensive approach. Finally, we used a multivariable mixed-effect logistic regression model, accounting for the correlation of EBF within the specific cluster. However, using a qualitative approach, it can be further explored to precisely identify the contextual factors affecting EBF practices in a particular community. Nevertheless, our study demonstrated the existence of contextual factors through significant variation in EBF across communities. We quantified their influence on EBF practices, and this analysis could be further extended by incorporating spatial data for more detailed spatial analysis and employing small-area estimation through a Bayesian hierarchical model as used in previous studies [80, 81]. This approach would address the challenges of small sample sizes, often a drawback in frequentist inference.
Conclusion
EBF has recently declined in Nepal, with notable variations across different communities. The key factors associated with EBF were the infant’s age, community ANC coverage, community poverty level, community maternal employment, and provinces from which they belong. This empirical evidence could help policymakers, program implementers, and stakeholders at different levels of government understand the factors contributing to low levels of EBF practices and guide the formulation of context-specific, tailored breastfeeding support programs. Policy and programmatic efforts should focus on breastfeeding promotion and support programs during pregnancy, continue through childbirth, and extend beyond childbirth rather than only targeting mothers with infants aged 3–5 months. Further studies can be conducted to explore the factors that help improve EBF practices, particularly in Lumbini Province.
Data availability
Data used in this study are publicly available secondary data obtained from the DHS (https://dhsprogram.com/data/available-datasets.cfm) program.
Abbreviations
- AIC:
-
Akaike’s Information Criteria
- ANC:
-
Antenatal Care
- AOR:
-
Adjusted odds ratio
- BFHI:
-
Baby Friendly Hospital Initiative
- BMS:
-
Breast Milk Substitute
- CI:
-
Confidence Interval
- EBF:
-
Exclusive Breastfeeding
- ICC:
-
Intraclass Correlation
- IYCF:
-
Infant and Young Child Feeding
- LMICs:
-
Low and Middle-Income Countries
- MBFHI:
-
Mother and Baby Friendly Hospital Initiative
- MOR:
-
Median odds ratio
- NDHS:
-
Nepal Demographic and Health Survey
- PCV:
-
Proportional change in variance
- PNC:
-
Postnatal Care
- PSU:
-
Primary Sampling Unit
- SDG:
-
Sustainable Development Goal
- VIF:
-
Variance Inflation Factor
- WHO:
-
World Health Organization
References
World Health Organization. Exclusive breastfeeding for optimal growth, development, and health of infants. 2023. https://www.who.int/tools/elena/interventions/exclusive-breastfeeding. Accessed 1 June 2024.
Chichlowski M, van Diepen JA, Prodan A, Olga L, Ong KK, Kortman GAM, Dunger DB, Gross G. Early development of infant gut microbiota in relation to breastfeeding and human milk oligosaccharides. Front Nutr. 2023;10:1003032DOI. https://doi.org/10.3389/fnut.2023.1003032.
Horta BLVC. Short-term effects of breastfeeding: a systematic review on the benefits of breastfeeding on diarrhoea and pneumonia mortality. In. Geneva: WHO; 2013.
Frank NM, Lynch KF, Uusitalo U, Yang J, Lönnrot M, Virtanen SM, Hyöty H, Norris JM. The relationship between breastfeeding and reported respiratory and gastrointestinal infection rates in young children. BMC Pediatr. 2019;19(1):339. https://doi.org/10.1186/s12887-019-1693-2.
Lamberti LM, Zakarija-Grković I, Fischer Walker CL, Theodoratou E, Nair H, Campbell H, Black RE. Breastfeeding for reducing the risk of pneumonia morbidity and mortality in children under two: a systematic literature review and meta-analysis. BMC Public Health. 2013;13(3):S18. https://doi.org/10.1186/1471-2458-13-S3-S18.
Horta BL, Loret de Mola C, Victora CG. Long-term consequences of breastfeeding on cholesterol, obesity, systolic blood pressure and type 2 diabetes: a systematic review and meta-analysis. Acta Paediatr. 2015;104(S467):30–7. https://doi.org/10.1111/apa.13133. https://onlinelibrary.wiley.com/doi/abs/.
Kwan ML, Buffler PA, Abrams B, Kiley VA. Breastfeeding and the risk of Childhood Leukemia: a Meta-analysis. Public Health Reports®. 2004;119(6):521–35. https://doi.org/10.1016/j.phr.2004.09.002.
Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS. How many child deaths can we prevent this year? Lancet. 2003;362(9377):65–71. https://doi.org/10.1016/s0140-6736(03)13811-1.
Chowdhury R, Sinha B, Sankar MJ, Taneja S, Bhandari N, Rollins N, Bahl R, Martines J. Breastfeeding and maternal health outcomes: a systematic review and meta-analysis. Acta Paediatr. 2015;104(467):96–113. https://doi.org/10.1111/apa.13102.
Eidelman AI, Schanler RJ, Johnston M, Landers S, Noble L, Szucs K, Viehmann L. Breastfeeding and the use of human milk. Pediatrics. 2012;129(3):e827–41. https://doi.org/10.1542/peds.2011-3552.
World Health Organization. Breastfeeding; 2024. [https://www.who.int/health-topics/breastfeeding#tab=tab_2]. Accessed 11 June, 2024.
United Nations Children’s Fund. Breastfeeding; 2023. [https://data.unicef.org/topic/nutrition/breastfeeding/]. Accessed 12 June, 2024
National Planning Commission. FY 2023/24–2030/31. In: Singhdurbar, editor. Multisectoral Nutrition Plan - III. Kathmandu, Nepal: NPC; 2024. p. 146. https://www.mofaga.gov.np/detail/3198. Accessed 12 June 2024
Ministry of Health and Population, New Era, and ICF International. Nepal Demographic and Health Survey 2022. Kathmandu, Nepal: Ministry of Health and Population [Nepal]; 2023. https://www.dhsprogram.com/pubs/pdf/FR379/FR379.pdf
His Majesty Government of Nepal. Mother’s milk substitutes (control of sale and distribution) act, 2049(1992). Kathmandu: Government of Nepal; 1992. https://lawcommission.gov.np/en/?p=12745.
United Nations Children’s Fund. More than half of babies in Nepal are breastfed in the first hour of life; 2018. https://www.unicef.org/nepal/press-releases/more-half-babies-nepal-are-breastfed-first-hour-life#. Accessed 11 June 2024.
Shrestha P. Assessment and strengthening the implementation of the code on breast milk substitutes and the Baby Friendly Hospital Initiative (BFHI). Kathmandu: Department of Health Services; 2011.
Ministry of Health-MOH/Nepal. Mother and baby-friendly health facility initiative guideline – 2017. Department of Health Services. Kathmandu: Ministry of Health; 2017.
Ministry of Health and Population. Annual Health Report 2022/2023. Kathmandu: Ministry of Health and Population; 2024. http://dohs.gov.np/category/annual-report/.
International Federation of Gynaecology and Obstetrics. Mother-Baby friendly birthing facilities. Int J Gynaecol Obstet. 2015;128(2):95–9. https://doi.org/10.1016/j.ijgo.2014.10.013.
Ministry of Health and Population: Lactation Management Centre Guideline. Kathmandu: Family Welfare Division; 2022. https://fwd.gov.np/wp-content/uploads/2022/09/CLMC-Guideline-in-English.pdf
Ministry of Health and Population: Strategy for Infant and Young Child Feeding: Nepal 2014. Kathmandu: Family welfare division, Department of Health Services. 2014.https://www.exemplars.health/-/media/files/egh/resources/stunting/nepal/part-2/strategy-for-infant-and-young-child-feeding-nepal-2014.pdf
Ministry of Health and Population, New ERA, and ICF International. Nepal Demographic and Health Survey 2011. Calverton, Maryland; 2012. http://dhsprogram.com/pubs/pdf/FR257/FR257.pdf.
Ministry of Health and Population, New ERA, and ICF International. Nepal Demographic and Health Survey 2016. Calverton, Maryland; 2017. http://dhsprogram.com/pubs/pdf/FR336/FR336.pdf.
Yadanar MKS, Witvorapong N. Determinants of breastfeeding practices in Myanmar: results from the latest nationally representative survey. PLoS ONE. 2020;15(9):e0239515. https://doi.org/10.1371/journal.pone.0239515.
Chandhiok N, Singh KJ, Sahu D, Singh L, Pandey A. Changes in exclusive breastfeeding practices and its determinants in India, 1992–2006: analysis of national survey data. Int Breastfeed J. 2015;10(1):34. https://doi.org/10.1186/s13006-015-0059-0.
Khanal V, Sauer K, Zhao Y. Exclusive breastfeeding practices in relation to social and health determinants: a comparison of the 2006 and 2011 Nepal demographic and health surveys. BMC Public Health. 2013;13(1):958. https://doi.org/10.1186/1471-2458-13-958.
Sharma M, Anand A, Goswami I, Pradhan MR. Factors associated with delayed initiation and non-exclusive breastfeeding among children in India: evidence from national family health survey 2019-21. Int Breastfeed J. 2023;18(1):28. https://doi.org/10.1186/s13006-023-00566-0.
Patel A, Badhoniya N, Khadse S, Senarath U, Agho KE, Dibley MJ. Infant and young child feeding indicators and determinants of poor feeding practices in India: secondary data analysis of National Family Health Survey 2005-06. Food Nutr Bull. 2010;31(2):314–33. https://doi.org/10.1177/156482651003100221.
Laksono AD, Wulandari RD, Ibad M, Kusrini I. The effects of mother’s education on achieving exclusive breastfeeding in Indonesia. BMC Public Health. 2021;21(1):14. https://doi.org/10.1186/s12889-020-10018-7.
Neves PAR, Barros AJD, Gatica-Domínguez G, Vaz JS, Baker P, Lutter CK. Maternal education and equity in breastfeeding: trends and patterns in 81 low- and middle-income countries between 2000 and 2019. Int J Equity Health. 2021;20(1):20. https://doi.org/10.1186/s12939-020-01357-3.
Ahmed MS, Whitfield KC, Yunus FM. Trends and predictors of early initiation, exclusive and continued breast-feeding in Bangladesh (2004–2018): a multilevel analysis of demographic and health survey data. British Journal of Nutrition 2022, 128(9):1857–1867.https://www.cambridge.org/core/product/581922C41C0268BF87AB70FF5892D1FB
Patil DS, Pundir P, Dhyani VS, Krishnan JB, Parsekar SS, D’Souza SM, Ravishankar N, Renjith V. A mixed-methods systematic review on barriers to exclusive breastfeeding. Nutr Health. 2020;26(4):323–46. https://doi.org/10.1177/0260106020942967.
Wasti SP, Shrestha A, Dhakal P, Gc VS. The prevalence of exclusive breastfeeding practice in the first six months of life and its associated factors in Nepal: a systematic review and meta-analysis. Sex Reproductive Healthc. 2023;37:100863. https://www.sciencedirect.com/science/article/pii/S1877575623000538.
Karkee R, Lee AH, Khanal V, Binns CW. A community-based prospective cohort study of exclusive breastfeeding in central Nepal. BMC Public Health. 2014;14(1):927. https://doi.org/10.1186/1471-2458-14-927.
Bentley ME, Dee DL, Jensen JL. Breastfeeding among low income, African-American women: power, beliefs and decision making. J Nutr. 2003;133(1):s305–9. https://doi.org/10.1093/jn/133.1.305S.
Shitie A, Tilahun A, Olijira L. Exclusive breastfeeding practice and associated factors among mothers of infants age 6 to 12 months in Somali region of Ethiopia. Sci Rep. 2022;12(1):19102. https://doi.org/10.1038/s41598-022-22051-0.
Cozma-Petruţ A, Filip L, Banc R, Mîrza O, Gavrilaş L, Ciobârcă D, Badiu-Tişa I, Hegheş SC, Popa CO, Miere D. Breastfeeding practices and determinant factors of exclusive breastfeeding among mothers of children aged 0–23 months in Northwestern Romania. Nutrients. 2021;13(11). https://doi.org/10.3390/nu13113998.
Ahmmed F, Hossain MJ, Sutopa TS, Al-Mamun M, Alam M, Islam MR, Sharma R, Sarker MMR, Azlina MFN. The trend in exclusive breastfeeding practice and its association with maternal employment in Bangladesh: a multilevel analysis. Front Public Health. 2022;10. https://doi.org/10.3389/fpubh.2022.988016. https://www.frontiersin.org/journals/public-health/articles/.
Ogbo FA, Dhami MV, Awosemo AO, Olusanya BO, Olusanya J, Osuagwu UL, Ghimire PR, Page A, Agho KE. Regional prevalence and determinants of exclusive breastfeeding in India. Int Breastfeed J. 2019;14(1):20. https://doi.org/10.1186/s13006-019-0214-0.
Hagos A, Tsadik M, Belachew AB, Tesfahunegn A. Individual and community-level factors influencing optimal breastfeeding: a multilevel analysis from a national survey study of Ethiopia. PLoS ONE. 2021;16(4):e0241428. https://doi.org/10.1371/journal.pone.0241428.
Tsegaw SA, Ali Dawed Y, Tadesse Amsalu E. Exploring the determinants of exclusive breastfeeding among infants under-six months in Ethiopia using multilevel analysis. PLoS ONE. 2021;16(1):e0245034. https://doi.org/10.1371/journal.pone.0245034.
Dharel D, Dhungana R, Basnet S, Gautam S, Dhungana A, Dudani R, Bhattarai A. Breastfeeding practices within the first six months of age in mid-western and eastern regions of Nepal: a health facility-based cross-sectional study. BMC Pregnancy Childbirth. 2020;20(1):59. https://doi.org/10.1186/s12884-020-2754-0.
Dhakal PS, Bina; Ghimire PK, Wasti SP. Prevalence and factors influencing exclusive breastfeeding practice among breastfeeding mothers in Kathmandu, Nepal. J Health Allied Sci 2023, 12(1).https://jhas.org.np/jhas/index.php/jhas/article/view/411
ICF International. Standard NDHS, Dataset. Rockville, Maryland; 2023. https://dhsprogram.com/data/dataset/Nepal_Standard-DHS_2022.cfm?flag=0. Accessed 1 June 2024.
Croft TN, Allen CK, Blake W, et al. Guide to DHS statistics. Rockville, Maryland, USA: ICF; 2023. https://www.dhsprogram.com/pubs/pdf/DHSG1/Guide_to_DHS_Statistics_DHS-8.pdf.
Belachew AB, Kahsay AB, Abebe YG. Individual and community-level factors associated with introduction of prelacteal feeding in Ethiopia. Arch Public Health. 2016;74:6DOI. https://doi.org/10.1186/s13690-016-0117-0.
Rutstein SO, Staveteig S. Making the demographic and health surveys wealth index comparable. Volume 9. ICF international Rockville, MD; 2014. https://dhsprogram.com/pubs/pdf/MR9/MR9.pdf.
Filmer D, Pritchett LH. Estimating wealth effects without expenditure data–or tears: an application to educational enrollments in states of India. Demography. 2001;38(1):115–32. https://doi.org/10.1353/dem.2001.0003.
Agho KE, Dibley MJ, Odiase JI, Ogbonmwan SM. Determinants of exclusive breastfeeding in Nigeria. BMC Pregnancy Childbirth. 2011;11(1):2. https://doi.org/10.1186/1471-2393-11-2.
Merlo J, Chaix B, Ohlsson H, Beckman A, Johnell K, Hjerpe P, Råstam L, Larsen K. A brief conceptual tutorial of multilevel analysis in social epidemiology: using measures of clustering in multilevel logistic regression to investigate contextual phenomena. J Epidemiol Community Health. 2006;60(4):290–7. https://doi.org/10.1136/jech.2004.029454.
Larsen K, Merlo J. Appropriate Assessment of Neighborhood effects on Individual Health: integrating Random and fixed effects in Multilevel Logistic Regression. Am J Epidemiol. 2005;161(1):81–8. https://doi.org/10.1093/aje/kwi017.
Hox J, Moerbeek M, Van de Schoot R. Multilevel analysis: techniques and applications, Third Edition. 3rd ed. Routledge; 2017.
Agresti A. Categorical data analysis. Volume 792. Wiley; 2012. https://doi.org/10.1002/0471249688.
Kim JH. Multicollinearity and misleading statistical results. Korean J Anesthesiol. 2019;72(6):558–69. https://doi.org/10.4097/kja.19087.
Reddy NS, Dharmaraj A, Jacob J, Sindhu KN. Exclusive breastfeeding practices and its determinants in Indian infants: findings from the National Family Health Surveys-4 and 5. Int Breastfeed J. 2023;18(1):69. https://doi.org/10.1186/s13006-023-00602-z.
Riaz A, Bhamani S, Ahmed S, Umrani F, Jakhro S, Qureshi AK, Ali SA. Barriers and facilitators to exclusive breastfeeding in rural Pakistan: a qualitative exploratory study. Int Breastfeed J. 2022;17(1):59. https://doi.org/10.1186/s13006-022-00495-4.
Piwoz EG, Huffman SL. The impact of marketing of breast-milk substitutes on WHO-Recommended Breastfeeding practices. Food Nutr Bull. 2015;36(4):373–86. https://doi.org/10.1177/0379572115602174.
Kavle JA, LaCroix E, Dau H, Engmann C. Addressing barriers to exclusive breast-feeding in low- and middle-income countries: a systematic review and programmatic implications. Public Health Nutr. 2017;20(17):3120–34. https://doi.org/10.1017/s1368980017002531.
Joshi C, Torvaldsen S, Hodgson R, Hayen A. Factors associated with the use and quality of antenatal care in Nepal: a population-based study using the demographic and health survey data. BMC Pregnancy Childbirth. 2014;14:94. https://doi.org/10.1186/1471-2393-14-94.
Khanal V, Bista S, Mishra SR, Lee AH. Dissecting antenatal care inequalities in western Nepal: insights from a community-based cohort study. BMC Pregnancy Childbirth. 2023;23(1):521. https://doi.org/10.1186/s12884-023-05841-w.
Bhattacharjee NV, Schaeffer LE, Hay SI, Lu D, Schipp MF, Lazzar-Atwood A, Donkers KM, Abady GG, Abd-Allah F, Abdelalim A, et al. Mapping inequalities in exclusive breastfeeding in low- and middle-income countries, 2000–2018. Nat Hum Behav. 2021;5(8):1027–45. https://doi.org/10.1038/s41562-021-01108-6.
Muluneh MW. Determinants of exclusive breastfeeding practices among mothers in Ethiopia. PLoS ONE. 2023;18(2):e0281576. https://doi.org/10.1371/journal.pone.0281576.
Khanal V, da Cruz JL, Karkee R, Lee AH. Factors associated with exclusive breastfeeding in Timor-Leste: findings from demographic and Health Survey 2009–2010. Nutrients. 2014;6(4):1691–700. https://doi.org/10.3390/nu6041691.
Jahanpour OF, Okango EL, Todd J, Mwambi H, Mahande MJ. Role of clusters in exclusive breastfeeding practices in Tanzania: a secondary analysis study using demographic and health survey data (2015/2016). Front Pead. 2022. https://doi.org/10.3389/fped.2022.939706.
Gatti L. Maternal perceptions of insufficient milk supply in breastfeeding. J Nurs Scholarsh. 2008;40(4):355–63. https://doi.org/10.1111/j.1547-5069.2008.00234.x.
Rahman MA, Khan MN, Akter S, Rahman A, Alam MM, Khan MA, Rahman MM. Determinants of exclusive breastfeeding practice in Bangladesh: evidence from nationally representative survey data. PLoS ONE. 2020;15(7):e0236080. https://doi.org/10.1371/journal.pone.0236080.
Subedi M, Maharjan R. Caste or Class? Formation of Social Strata in Nepal; 2018.https://www.researchgate.net/publication/350125073_Caste_or_Class_Formation_of_Social_Strata_in_Nepal
Chen J, Xin T, Gaoshan J, Li Q, Zou K, Tan S, Cheng Y, Liu Y, Chen J, Wang H, et al. The association between work related factors and breastfeeding practices among Chinese working mothers: a mixed-method approach. Int Breastfeed J. 2019;14(1):28. https://doi.org/10.1186/s13006-019-0223-z.
Santos MN, Azeredo CM, Rinaldi AEM. Association between Maternal Work and exclusive breastfeeding in countries of Latin America and Caribbean. Matern Child Health J. 2022;26(7):1496–506. https://doi.org/10.1007/s10995-022-03390-w.
Tadesse F, Alemayehu Y, Shine S, Asresahegn H, Tadesse T. Exclusive breastfeeding and maternal employment among mothers of infants from three to five months old in the Fafan Zone, Somali regional state of Ethiopia: a comparative cross-sectional study. BMC Public Health. 2019;19(1):1015. https://doi.org/10.1186/s12889-019-7345-5.
Khanal V, Lee AH, Karkee R, Binns CW. Postpartum Breastfeeding Promotion and Duration of Exclusive Breastfeeding in Western Nepal. Birth. 2015;42(4):329–36.
Bui QT, Lee HY, Le AT, Van Dung D, Vu LT. Trends and determinants for early initiation of and exclusive breastfeeding under six months in Vietnam: results from the multiple Indicator cluster surveys, 2000–2011. Glob Health Action. 2016;9:29433DOI. https://doi.org/10.3402/gha.v9.29433.
Abegunde D, Hutchinson P, Anaba U, Oyedokun-Adebagbo F, Johansson EW, Feyisetan B, Mtiro E. Socioeconomic inequality in exclusive breastfeeding behavior and ideation factors for social behavioral change in three north-western Nigerian states: a cross-sectional study. Int J Equity Health. 2021;20(1):172. https://doi.org/10.1186/s12939-021-01504-4.
Thu HN, Eriksson B, Khanh TT, Petzold M, Bondjers G, Kim CNT, Thanh LN, Ascher H. Breastfeeding practices in urban and rural Vietnam. BMC Public Health. 2012;12(1):964. https://doi.org/10.1186/1471-2458-12-964.
Ministry of Health and Population NSO: National Population and Housing Census 2021. Nepal maternal mortality study 2021. Kathmandu: Ministry of Health and Population; National Statistical Office; 2022. https://mohp.gov.np/uploads/Resources/Final%20Report-26%20March-%202023-UPDATED.pdf.
Dulal TD. Status of Human Development Index with reference to Nepal. J Popul Dev. 2023;4(1):166–80. https://doi.org/10.3126/jpd.v4i1.64256.
Khanal V, Lee AH, Scott JA, Karkee R, Binns CW. Implications of methodological differences in measuring the rates of exclusive breastfeeding in Nepal: findings from literature review and cohort study. BMC Pregnancy Childbirth. 2016;16(1):389. https://doi.org/10.1186/s12884-016-1180-9.
World Health Organization. Indicators for assessing breastfeeding practices; 1991. https://www.who.int/publications/i/item/WHO_CDD_SER_91.14_Corr.1]. Accessed 16 June 2024
Ko S, Oh H, Subramanian SV, Kim R. Small Area Geographic estimates of Cardiovascular Disease Risk factors in India. JAMA Netw Open. 2023;6(10):e2337171–2337171. https://doi.org/10.1001/.
Haslett S, Jones G, Isidro M, Sefron A. Small area estimation of food insecurity and undernutrition in Nepal. Kathmandu, Nepal: Central Bureau of Statistics, National Planning Commissions Secreteriat, World Food Programme, UNICEF and World Bank; 2014.https://documents.wfp.org/stellent/groups/public/documents/ena/wfp277412.pdf?_ga=2.177582565.1196338768.1720522762-1757083935.1720522762
Acknowledgements
NA.
Funding
No funding was received for the development of this manuscript.
Author information
Authors and Affiliations
Contributions
BKS: Conceptualization, Data curation, Formal analysis, Methodology, Writing- original draft, Writing – review and editing, Visualization, Validation; RBK: Conceptualization, Methodology, Validation, Supervision, Writing – review and editing; SKS: Validation, Writing- review and editing; VK: Conceptualization, Methodology, Validation, Interpretation of results, Visualization, Writing – review & editing and Supervision.
Corresponding author
Ethics declarations
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Conflicts of interest
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as potential conflicts of interest.
Ethics approval and consent to participate
Not applicable. We used publicly accessible, deidentified datasets from the Demographic and Health Survey program (https://dhsprogram.com/data/available-datasets.cfm). The survey received ethical approval from the ICF Institutional Review Board in the USA and the Nepal Health Research Council, Nepal. Mothers provided informed consent both for themselves and for their children. Given that this research involved only a secondary analysis of completely anonymised data, there was no need for additional ethical clearance. The author (BKS) received approval to access and utilize the deidentified data.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Singh, B.K., Khatri, R.B., Sahani, S.K. et al. Determinants of exclusive breastfeeding among infants under six months in Nepal: multilevel analysis of nationally representative household survey data. BMC Public Health 24, 2456 (2024). https://doi.org/10.1186/s12889-024-19963-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19963-z