
Abstract
Background
Medial tibial stress syndrome (MTSS) is a running-related injury of the lower extremities. After returning to competition, there are often recurring episodes of MTSS. Therefore, it is important to prevent the onset and recurrence of MTSS among long-distance runners. This case–control study aimed to compare the kinematics and kinetics of runners with and without previous MTSS during running to clarify the biomechanical characteristics of the lower extremity of runners with previous MTSS.
Methods
Thirteen male long-distance runners aged over 18 years and asymptomatic at the time of measurement were divided into an MTSS group and a non-MTSS group based on their history of MTSS as reported in a questionnaire. The kinetics and kinematics of running were analyzed when participants ran at a speed of 2.0 ± 0.2 m/s by a three-dimensional motion analysis system and two force plates. Data regarding the joint angles, moments, and powers of the ankle, knee, and hip during the stance phase while running were extracted and compared between the two groups using the Mann–Whitney U test.
Results
Of the 13 participants, 5 and 8 were included in the MTSS (10 legs) and non-MTSS (16 legs) groups, respectively. The ankle maximum eversion moment was significantly larger in the MTSS group than in the non-MTSS group (p = 0.04). There were no significant differences in other parameters.
Conclusions
This study found that the ankle maximum eversion moment during the stance phase of running was larger in the MTSS group than in the non-MTSS group. Even after the disappearance of the symptoms of MTSS, the running biomechanics of participants with previous MTSS differed from those of participants without previous MTSS.
Similar content being viewed by others
Background
Many adult long-distance runners (19–92%) have experienced a running-related injury of the lower extremities [1]. Medial tibial stress syndrome (MTSS) accounts for 5–10% of runners [2, 3]. This injuries occurs at 0.01 per 1000 km in elite runners [4]. Runners may require prolonged periods of rest and cessation of running, ranging from 2 to 6 weeks on average [2]. After returning to competition, MTSS often recurs [3]. MTSS incidence in runners with an MTSS history in one season is about twice that of runners without such a history [4, 5]. Therefore, prevention of the onset and recurrence of MTSS in long-distance runners is important. Previous findings demonstrate the multifactorial development of MTSS, involving passive range of motion, muscle strength, plantar pressure distributions, and both proximal and distal kinematics [6]. A study involving 146 college athletes showed that 87% had a history of MTSS [7]. A history of MTSS is a risk factor for MTSS recurrence [2, 8, 9].
Compared to runners with no previous injuries, including MTSS or stress fractures, runners with previous injuries have biomechanical characteristics including greater hip flexion or pelvic tilt angles in the frontal plane and lesser knee flexion angles in the stance phase of running [10, 11]. Therefore, even after MTSS symptoms have disappeared, the biomechanics affecting recurrence of MTSS may remain.
A study that analyzed running in individuals with a previous running injury looked at ground reaction forces and joint angles, but not joint moments or power [10, 11]. These kinematic variables are important for estimating the load on muscles and joints during motion. Previous reports [10, 11] have assessed multiple running disorders of the shanks and thighs. The kinematic factors of running injuries such as MTSS differ from those of injuries of the thigh. However, no study has analyzed MTSS-related kinetics data during running.
We aimed to compare the kinematics and kinetics of runners with and without previous MTSS during running to clarify the biomechanical characteristics of runners with previous MTSS. Excessive traction stress to the soleus fascia and tibial periosteum during running is involved in MTSS onset [12, 13]. Thus, we hypothesized that runners with and without previous MTSS have different eversion angles and moments, both of which are associated with increased traction stress on the soleus fascia and tibial periosteum [12].
Methods
Study design and oversight
This was a case-control study that followed the guidelines of the 1975 Declaration of Helsinki. Our study were performed in accordance with relevant guidelines and regulations. Ethical approval was granted by our institutional review board (approval number, M 2000-2069), and all participants provided written informed consent before participation.
Participants
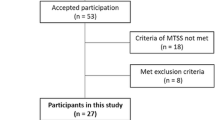
Male long-distance runners aged 18–30 years were included who (i) specialized in long-distance running competitions at the university level or higher; (ii) participated in training ≥ 3 times per week; and (iii) reported no pain in their lower extremities at the time of the assessment. Participants who had not participated in practice sessions for more than one week within the last six months due to injury or illness were excluded. Thirteen participants (age, 24.1 ± 1.8 years; height, 170.1 ± 5.7 cm; weight, 55.3 ± 4.2 kg; body mass index, 19.1 ± 0.6 kg/m2) who met the criteria were included. A leg was counted as one sample [14,15,16] in investigating the kinetics and kinematics of a leg with an MTSS history.
Questionnaire
Participants described their mileage and MTSS history in the self-administered questionnaire. The MTSS history was defined according to a previous diagnosis of MTSS by a doctor who ruled out a tibial stress fracture or exertional compartment syndrome via diagnostic imaging. The running mileage was defined as the total distance travelled by the participant during practice or in competitions in the last week before the assessment [11].
Measurement of motion
All participants wore identical athletic attire comprising spandex shirts, shorts, and shoes without air cushions (step101, Lucky Bell, Kobe, Japan). Participants were assessed using a three-dimensional motion analysis system (Motive; Acuity Inc., Tokyo, Japan) with eight cameras operating at a sampling rate of 100 Hz and two force plates (TF-406; Tec Gihan Co, Kyoto, Japan) at a sampling rate of 1,000 Hz. Sixteen infrared reflective markers (9 mm spheres) were attached to anatomical landmarks using the Plug-in-Gait model (Oxford Metrics LTD, Oxford, United Kingdom). Markers were placed over both anterior superior iliac spines and the posterior superior iliac spine, lateral thigh, lateral condyles of the thigh, lateral shank, lateral malleolus, posterior calcaneus, and second metatarsal heads. The motor task was running on a track at a speed of 2.0 ± 0.2 m/s for approximately 10 m [17, 18]. Before the running task, participants warmed up by stretching or running for 5 min and practicing running at a predetermined speed. A successful measurement occurred when the patient’s entire foot was placed on the force plate surface.
Analysis
The three-dimensional data were smoothed by a second-order Butterworth-type low-pass filter with a cut-off frequency of 10 Hz and imported to analysis software (SKYCOM; Acuity Inc, Tokyo, Japan). A lower extremity model of the pelvis, thighs, shanks, and foot segments was created using this software. Additionally, using this model, the kinematics and kinetics of the hip, knee, and ankle on the sagittal and frontal planes were analyzed (Table 1). The eversion or inversion moment is the external moment when a foot segment is applied outward or inward to the direction of progression. Joint moments were calculated as external joint moments and were normalized to the body weight (Nm/kg). Furthermore, joint powers were normalized to body weight (W/kg).
Grouping according to MTSS history
The participants who reported an MTSS history were asked to provide more details. The survey asked, "In which leg did you previously experience MTSS?" and "How many times did you experience MTSS?".
Legs reported to have previous MTSS were included in the MTSS group, and those without reported MTSS history were included in the non-MTSS group.
Statistical analysis
Participant demographics and questionnaire results were descriptively summarized. Data normality was confirmed using the Shapiro–Wilk test. An unpaired t-test was used to compare normally distributed data between the groups. Finally, the Mann–Whitney U test was used to compare the non-normally distributed data between groups, and the effect size (d) or (r) was calculated. All statistical analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). All statistical significance was set at p < 0.05.
An a priori sample size calculation was conducted using G* Power software 3.1.9.4 [19]. Based on a previous study [6] that analyzed the kinematics of the ankle, the minimum number of participants was calculated with an α value of 0.05 and β of 0.8, and 12 paired samples in each group were indicated.
Results
Demographic data
Of the 13 participants, 5 had a history of MTSS (10 legs; MTSS group), and 8 did not (16 legs; non-MTSS group). All five MTSS participants had a history of MTSS in both legs. In the motion analysis, 10 MTSS legs and 16 non-MTSS legs (total: 26 legs) were analyzed. No participants had previous tibial stress fractures, and no significant differences were found in participant demographics between the two groups (Table 2). In the MTSS group, the median time of the previous MTSS onset was 1.5 [4.0] years (median [interquartile range]).
Biomechanical data
Biomechanical data of the lower extremities are shown in (Tables 3, 4 and 5), and (Figs. 1, 2 and 3). No significant difference was found in the maximum eversion angle between the groups (p = 0.77). However, the maximum eversion moment was significantly larger in the MTSS group than in the non-MTSS group (p = 0.03) (Table 3). No differences were found in the knee and hip biomechanical data during the stance phase of running (Tables 4 and 5).

Joint angle during running in the stance phase. The solid line and dashed line represent the MTSS group and Non-MTSS group, respectively. A Ankle joint dorsi ( +)/planter flexion angle (-); B Knee joint flexion ( +)/extension (-) angle; C Hip joint flexion ( +)/extension (-) angle; D Ankle joint eversion ( +)/inversion (-) angle; E Knee joint varus ( +)/valgus (-) angle; F Hip joint adduction ( +)/abduction (-) angle. MTSS, medial tibial stress syndrome

Joint moments during running in the stance phase. The solid line and dashed line represent the MTSS group and Non-MTSS group, respectively. A Ankle joint dorsi ( +)/planter (-) flexion moment; B Knee joint flexion ( +)/extension (-) moment; C Hip joint flexion ( +)/extension (-) moment; D Ankle joint eversion ( +)/inversion (-) moment; E Knee joint varus ( +)/valgus (-) moment; F Hip joint adduction ( +)/abduction (-) moment.MTSS, medial tibial stress syndrome

Joint power during running in the stance phase. The solid line and dashed line represent the MTSS group and Non-MTSS group, respectively. A Ankle joint power on the sagittal plane; B Knee joint power on the sagittal plane; C Hip joint power on the sagittal plane; D Ankle joint power on the frontal plane; E Knee joint power on the frontal plane; F Hip joint power on the frontal plane. MTSS, medial tibial stress syndrome
Discussion
This study found that the maximum eversion moment during the stance phase of running was larger in runners with an MTSS history than in those without an MTSS history. This finding partially supports the hypothesis of the study.
The maximum eversion moment in the MTSS group was significantly larger than that in the non-MTSS group (Table 3). Since no previous research has analyzed the joint moment and power in runners with an MTSS history, it is difficult to compare our results with previous reports. Therefore, our results will be discussed based on the MTSS etiology. MTSS is caused by a bone stress reaction to the impact of walking and running in the tibial cortex [18, 20]. Elongational stress on the soleus, flexor digitorum longus, and tibialis posterior muscles increases strain on the tibial fascia [18, 20]. Traction stress on the soleus and posterior tibial muscles is greater during movement and induces a large external eversion moment. In this study, traction stress on the soleus and posterior tibial muscles appeared relatively large in the MTSS group due to the large maximum eversion moment during running. Although no specific joint motion was observed in the MTSS group, they may not control the eversion moment.
One reason for the difference in the eversion moment between the two groups may be variations in the trajectory of the center of pressure (COP) during running. The stance phase COP during the gait, in those without MTSS, passed from the heel to the lateral forefoot and then to the medial toes. In runners who developed MTSS, the COP was transmitted directly from the heel to the medial toes [20, 21]. In the MTSS group, the COP might have passed through the medial sole, shortening the eversion moment lever arm. Since the COP trajectory during running was not analyzed in this study, future studies should explore a detailed kinematic analysis of the foot pressure distribution during running.
No significant intergroup differences were found in the maximal eversion and inversion angles and eversion-inversion angle excursion. The foot abduction, eversion, is considered to positively correlate with eversion in the subtalar because it is one of the pronation-in-subtalar-movement components [22, 23]. The soleus muscle and its fascia are more stretched during calcaneal inversion than during pronation [12]. However, our results do not support this hypothesis. Previous studies reported that athletes and military personnel with MTSS had a greater hindfoot eversion angle during running than those without MTSS [7, 24, 25]. A possible explanation for our results not supporting the hypothesis may be due to differences in foot definitions during the motion analysis and participant demographics. We defined the foot based on markers for the calcaneus, lateral malleolus of the fibula, and the second metatarsal head. Therefore, the forefoot and hindfoot were considered a single segment. However, another study defined the forefoot and hindfoot as separate segments [7]. They targeted athletes from several sports (for example, short-track running, tennis, and basketball). In contrast, our study targeted only long-distance runners. The onset mechanism of MTSS may differ between the above-mentioned sports and long-distance running.
The maximum ankle dorsiflexion angle did not differ significantly between the two groups. Okunuki [7] reported no significant differences in the foot dorsiflexion angle between MTSS and control groups. Interestingly, our results support this finding. The maximum dorsiflexion angle of the ankle during running appeared unrelated to the history or the symptoms of MTSS.
We found no significant intergroup differences in the maximum knee and hip angles during running. However, it has been reported that runners who experienced injuries demonstrated lesser knee flexion and greater hip adduction angles in the early stance phase than those without such a history [11, 26]. Other studies reported that runners with a history of bone stress injury (tibial stress fractures and shin splints) had greater hip flexion angles than runners without such a history [10, 26]. Our results did not support these findings, possibly because running injuries other than MTSS were included as target injuries in two of these studies [10, 26]; in the third study, participants were grouped according to the presence or absence of medial tibial pain [11]. Another reason may be that the analyzed running phases differ [22]. However, no study has analyzed joint moment and power in runners with MTSS or a history of running-related injuries. Our data suggest that knee and hip joint angles, moments, and powers during running were unrelated to the MTSS history.
In this study, a statistical difference was found in the ankle eversion moment and hip maximum absorptive power on the frontal plane; however, no difference was found in the other angles and moments on the frontal plane. Therefore, it is possible that the trunk movement, including the head and arms, contributed to the ankle eversion moment. However, this study did not measure it; therefore, it was difficult to prove.
Our biomechanical data partially describe the kinetics and kinematics in runners with previous MTSS. Therefore, the foot kinetics and kinematics in runners with an MTSS history should be evaluated to prevent recurrence after MTSS symptoms disappear.
This study had some limitations. First, this study’s results may not apply to female runners or runners of other categories because the participants were all male long-distance runners at the university level or higher. Second, since this was a case–control study, it is unclear whether the differences in the eversion moment caused MTSS or resulted from MTSS. Moreover, we cannot show that participants in the MTSS group acquired pain-avoidance movements from a previous MTSS, as the MTSS onset in the MTSS group was approximately 1.5 years before the study initiation. Therefore, future follow-up studies and prospective trials are warranted. Third, all MTSS participants had a bilateral MTSS history, and these results may not apply to individuals with a unilateral MTSS history. Additionally, this study did not analyze the difference between the dominant and non-dominant legs. This was because the dominant and non-dominant legs during running did not differ [27]. Fourth, parameters where p > 0.05 had a large effect size; therefore, type II errors were possible. This study had a small sample size; therefore, it might also have had a type II error. A post hoc power analysis revealed that, with an alpha value of 0.05 and effect size 1.10 (Maximum ankle joint eversion moment), this study had a power of 84.3% for the difference between the two groups. Lastly, kinetics and kinematics vary during fast motion [17, 28]. Although we set the running speed to 2.0 ± 0.2 m/s, our results may not be applicable at higher running speeds. Therefore, biomechanical data at different running speeds require further investigation.
Conclusions
This study compared lower extremity kinetic and kinematic variables during running between a population of young adult male runners with or without an MTSS history. Our findings revealed that foot kinematics during the stance phase of running differed between individuals with and without a history of MTSS. Therefore, our findings suggest that running kinematics in runners with and without an MTSS history were different even after symptom disappearance.
Availability of data and materials
All data generated or analyzed during this study are included in this article.
Abbreviations
- COP:
-
Center of pressure
- MTSS:
-
Medial tibial stress syndrome
References
van Gent RN, Siem D, van Middelkoop M, van Os AG, Bierma-Zeinstra SM, Koes BW. Incidence and determinants of lower extremity running injuries in long distance runners: a systematic review. Br J Sports Med. 2007;41:469–80 discussion 80.
Galbraith RM, Lavallee ME. Medial tibial stress syndrome: conservative treatment options. Curr Rev Musculoskelet Med. 2009;2:127–33.
Thacker SB, Gilchrist J, Stroup DF, Kimsey CD. The prevention of shin splints in sports: a systematic review of literature. Med Sci Sports Exerc. 2002;34:32–40.
Plisky MS, Rauh MJ, Heiderscheit B, Underwood FB, Tank RT. Medial tibial stress syndrome in high school cross-country runners: incidence and risk factors. J Orthop Sports Phys Ther. 2007;37:40–7.
Reinking MF, Austin TM, Richter RR, Krieger MM. Medial tibial stress syndrome in active individuals: a systematic review and meta-analysis of risk factors. Sports Health. 2017;9(3):252–61.
Becker J, Nakajima M, Wu WFW. Factors contributing to medial tibial stress syndrome in runners: a prospective study. Med Sci Sports Exerc. 2018;50:2092–100.
Okunuki T, Koshino Y, Yamanaka M, Tsutsumi K, Igarashi M, Samukawa M, et al. Forefoot and hindfoot kinematics in subjects with medial tibial stress syndrome during walking and running. J Orthop Res. 2019;37:927–32.
Knobloch K, Yoon U, Vogt PM. Acute and overuse injuries correlated to hours of training in master running athletes. Foot Ankle Int. 2008;29:671–6.
Hubbard TJ, Carpenter EM, Cordova ML. Contributing factors to medial tibial stress syndrome: a prospective investigation. Med Sci Sports Exerc. 2009;41:490–6.
Lachniet PB, Taylor-Haas JA, Paterno MV, DiCesare CA, Ford KR. Altered sagittal plane hip biomechanics in adolescent male distance runners with a history of lower extremity injury. Int J Sports Phys Ther. 2018;13:441–52.
Loudon JK, Reiman MP. Lower extremity kinematics in running athletes with and without a history of medial shin pain. Int J Sports Phys Ther. 2012;7:356–64.
Michael RH, Holder LE. The soleus syndrome. A cause of medial tibial stress (shin splints). Am J Sports Med. 1985;13:87–94.
Bouché RT, Johnson CH. Medial tibial stress syndrome (tibial fasciitis): a proposed pathomechanical model involving fascial traction. J Am Podiatr Med Assoc. 2007;97:31–6.
Beach A, Regazzola G, Neri T, Verheul R, Parker D. The effect of knee prosthesis design on tibiofemoral biomechanics during extension tasks following total knee arthroplasty. Knee. 2019;26:1010–9.
Niki Y, Nagura T, Nagai K, Kobayashi S, Harato K. Kinematically aligned total knee arthroplasty reduces knee adduction moment more than mechanically aligned total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2018;26:1629–35.
Nagura T, Niki Y, Harato K, Mochizuki T, Kiriyama Y. Analysis of the factors that correlate with increased knee adduction moment during gait in the early postoperative period following total knee arthroplasty. Knee. 2017;24:250–7.
Keller TS, Weisberger AM, Ray JL, Hasan SS, Shiavi RG, Spengler DM. Relationship between vertical ground reaction force and speed during walking, slow jogging, and running. Clin Biomech (Bristol, Avon). 1996;11:253–9.
Schnohr P, O’Keefe JH, Marott JL, Lange P, Jensen GB. Dose of jogging and long-term mortality: the Copenhagen City Heart Study. J Am Coll Cardiol. 2015;65:411–9.
Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–91.
Klein P, Mattys S, Rooze M. Moment arm length variations of selected muscles acting on talocrural and subtalar joints during movement: an in vitro study. J Biomech. 1996;29:21–30.
Kinoshita K, Okada K, Saito I, Saito A, Takahashi Y, Kimoto M, et al. Alignment of the rearfoot and foot pressure patterns of individuals with medial tibial stress syndrome: a cross-sectional study. Phys Ther Sport. 2019;38:132–8.
Naderi A, Degens H, Sakinepoor A. Arch-support foot-orthoses normalize dynamic in-shoe foot pressure distribution in medial tibial stress syndrome. Eur J Sport Sci. 2019;19:247–57.
Nester CJ. Rearfoot complex: a review of its interdependent components, axis orientation and functional model. Foot. 1997;7:86–96.
Messier SP, Pittala KA. Etiologic factors associated with selected running injuries. Med Sci Sports Exerc. 1988;20:501–5.
Viitasalo JT, Kvist M. Some biomechanical aspects of the foot and ankle in athletes with and without shin splints. Am J Sports Med. 1983;11:125–30.
Bramah C, Preece SJ, Gill N, Herrington L. Is there a pathological gait associated with common soft tissue running injuries? Am J Sports Med. 2018;46:3023–31.
Brown AM, Zifchock RA, Hillstrom HJ. The effects of limb dominance and fatigue on running biomechanics. Gait Posture. 2014;39:915–9.
Andriacchi TP, Ogle JA, Galante JO. Walking speed as a basis for normal and abnormal gait measurements. J Biomech. 1977;10:261–8.
Acknowledgements
We would like to thank the members of our institution for their assistance and Editage (www.editage.jp) for English language editing.
Funding
This work was supported by the JSPS KAKENHI [grant number 18K17822].
Author information
Authors and Affiliations
Contributions
All authors made significant contributions to the conception and design, acquisition of data, or analysis and interpretation of data. All authors made significant contributions to drafting the manuscript or revising it critically for intellectual content. TO participated in the conception and design, analysis, and interpretation of data, and in writing the manuscript. JA, KH, and SO participated in the design, acquisition and interpretation of data, and revision of the manuscript. SM, TO and KY participated in the acquisition of data, interpretation of data, and revision of the manuscript. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was granted by our institutional review board (Tokyo Medical and Dental University Hospital) (approval number, M 2000–2069). All participants provided written informed consent before participation.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ohmi, T., Aizawa, J., Hirohata, K. et al. Biomechanical characteristics of the lower extremities during running in male long-distance runners with a history of medial tibial stress syndrome: a case control study. BMC Musculoskelet Disord 24, 103 (2023). https://doi.org/10.1186/s12891-023-06216-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-06216-0