
Abstract
Objective
This study sought to determine the incidence and risk factors of blood transfusion among patients undergoing total knee revision (TKR) using a nationwide database.
Methods
A retrospective data analysis was conducted based on the Nationwide Inpatient Sample (NIS), enrolling patients who underwent TKR from 2010 to 2019 with complete information. The patients were divided into two groups based on whether they received blood transfusion or not. The demographic characteristics (race, sex, and age), length of stay (LOS), total charge of hospitalization, hospital characteristics (admission type, insurance type, bed size, teaching status, location, and region of hospital), hospital mortality, comorbidities, and perioperative complications were analyzed. Finally, we conducted univariate and multivariate logistic regression to identify factors that were associated with TKR patients to require blood transfusion.
Results
The NIS database included 115,072 patients who underwent TKR. Among them, 14,899 patients received blood transfusion, and the incidence of blood transfusion was 13.0%. There was a dramatic decrease in the incidence over the years from 2010 to 2019, dropping from 20.4 to 6.5%. TKR patients requiring transfusions had experienced longer LOS, incurred higher total medical expenses, utilized Medicare more frequently, and had increased in-hospital mortality rates (all P < 0.001). Independent predictors for blood transfusion included advanced age, female gender, iron-deficiency anemia, rheumatoid disease, chronic blood loss anemia, congestive heart failure, coagulopathy, uncomplicated diabetes, lymphoma, fluid and electrolyte disorders, metastatic carcinoma, other neurological diseases, paralysis, peripheral vascular disorders, pulmonary circulation disorders, renal failure, valvular disease, and weight loss. In addition, risk factors for transfusion in TKR surgery included sepsis, acute myocardial infarction, deep vein thrombosis, pulmonary embolism, gastrointestinal bleeding, heart failure, renal insufficiency, pneumonia, wound infection, lower limb nerve injury, hemorrhage/seroma/hematoma, wound rupture/non healing, urinary tract infection, acute renal failure, and postoperative delirium.
Conclusions
Our findings highlight the importance of recognizing the risk factors of blood transfusion in TKR to reduce the occurrence of adverse events.
Similar content being viewed by others


Introduction
Total knee arthroplasty (TKA) is a widely practiced and effective approach for treating advanced knee joint diseases in clinical settings [1, 2]. Although the therapeutic effect of total knee arthroplasty has been established, complications, including periprosthetic joint infection, prosthesis loosening, dislocation, periprosthetic fracture, and pain can lead to the failure of primary joint replacement and demand of revision treatment [3,4,5]. Total knee revision (TKR) requires the removal of the previously replaced prosthesis and re-implantation of the new prosthesis. Approximately over 100,000 TKR procedures are carried out annually in the United States [6].
TKR surgery is intricate and often results in significant blood loss. Consequently, the need for blood transfusions during TKR is more frequent. Nevertheless, blood transfusions come with potential risks, including transfusion reactions, infections, immunosuppression, and surgical site infections [3]. Furthermore, blood transfusion increases medical resources consumption, length of stay (LOS), hospitalization expenses, complications, and even death [7, 8]. Hence, it is crucial to identify how often patients undergoing TKR require blood transfusions and the factors that increase this risk to minimize the necessity for blood transfusions.
Reports indicate that the occurrence of blood transfusions in total knee arthroplasty varies between 3.2% and 18.1%, while for TKR, it ranges from 9.8 to 19.8% from 2010 to 2015 [9]. The preoperative lower level of hemoglobin (Hb), female, extended operative duration and increased blood loss during surgery have been reported to be independently associated with blood transfusion in total joint arthroplasty (TJA) [10, 11]. However, no study has hitherto examined the occurrence and risk factors of blood transfusion in patients undergoing TKR with a substantial sample size. Therefore, this study aims to explore the frequency and factors contributing to blood transfusions following TKR, harnessing data from a nationwide database.
Materials and methods
Data source
This study drew upon data from the Nationwide Inpatient Sample (NIS) database, a component of the Healthcare Cost and Utilization Project facilitated by the Agency for Healthcare Research and Quality. In the United States, NIS stands out as the most extensive all-payer database encompassing hospital admissions. Sampling from over 1000 hospitals, NIS gathers data from about 20% of annual hospitalizations in the country [12,13,14]. Data for this study were extracted from the database, encompassing patient demographics (age, sex, and race), hospital characteristics (insurance type, admission type, hospital bed size, teaching status, location, and region), LOS, economic indicators, and diagnostic and procedural codes derived from the International Classification of Diseases (ninth and tenth revisions) Clinical Modification (ICD-9-CM and ICD-10-CM). This research study did not require approval from an ethics board since it used anonymous data that is publicly accessible.
Data collection
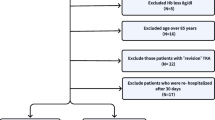
Data spanning from 2010 to 2019 was collected from the Nationwide Inpatient Sample database. The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and The International Classification of Diseases, tenth Revision, Clinical Modification primary procedure coding ICD-10-CM) indicative of total knee revision were used (Supplement 1) [6].The occurrence of blood transfusion was determined based on ICD-9-CM or ICD-10-CM diagnostic codes. Patients under 18 years old and those using anticoagulants, antiplatelets, antithrombotic, non-steroidal, and aspirin drugs were excluded (Fig. 1).

Exclusion process for patients undergoing total knee revision with blood transfusion
The patients included in the study were separated into two groups based on whether they received a blood transfusion. We evaluated patient demographics, hospital characteristics, and outcome measures such as LOS, economic indicators, and in-hospital mortality. Information about preoperative comorbidities and perioperative complications was extracted from the database using diagnostic codes from ICD-9-CM and ICD-10-CM (Table 1). Perioperative complications included: sepsis, acute myocardial infarction, deep vein thrombosis, convulsion, pulmonary embolism, gastrointestinal bleeding, heart failure, renal sufficiency, pneumonia, respiratory disease, urinary tract infection, acute renal failure and postoperative delirium, wound infection, lower limb nerve injury, hemorrhage/seroma/hematoma, wound rupture/non healing.
Data analysis
Analysis was conducted using Statistical Package for the Social Sciences (SPSS) 25.0 statistical software. Independent t-tests were applied to assess continuous data, while chi-square tests were used for comparing categorical data. Logistic regression analysis was employed to identify potential risk factors associated with blood transfusion. The regression analysis included all variables from NIS, covering patient demographics, hospital characteristics, and comorbidities (Table 1). Odds ratios (OR) and 95% confidence intervals (CI) were calculated after the logistic regression. Given the substantial sample size, statistical significance was considered for p-values less than 0.001.
Results
Incidence of blood transfusion after TKR
From 2010 to 2019, a total of 139,098 TKR cases were identified in the NIS database. After excluding the patients who did not meet the criteria, there were 115,072 patients undergoing TKR, among which 14,899 patients received blood transfusion, and the incidence of blood transfusion was 13.0% (Table 2). The data revealed a gradual decrease in the incidence of blood transfusion each year from 2011 to 2019, dropping from 20.4 to 6.5% (Fig. 2).

Annual incidence of blood transfusion in total knee revision
Patient demographics between the two groups
A notable difference was observed in the occurrence of blood transfusions during hospitalization between the two genders, with a higher proportion of transfusions observed in females (64.1% vs. 35.9%, P < 0.001) (Table 2). Overall, patients who required blood transfusions were relatively older (67.4 years vs. 64.7 years, P < 0.001). Consistently, the age distribution between the two groups differed, with a higher proportion of patients aged 71 years and older in the blood transfusion group (41.4% vs. 30.2% P < 0.001) (Table 2). Meanwhile, a significant difference was detected in races, with the Black occupying slightly larger proportions in the transfusion group.
Hospital characteristics of two groups
The significantly more cases of TKR requiring blood transfusions were observed in large hospitals than in small hospitals (P < 0.001) (Table 2). Patients who received a blood transfusion were less likely to have undergone elective admission compared to those in the non-transfusion group (P < 0.001) (Table 2). Additionally, teaching and urban hospitals exhibited a lower incidence of blood transfusion after TKR (P < 0.001). In terms of geographical location, in-hospital blood transfusion was more likely in the South and Midwest or North Central regions, while less likely in the Northeast and West (P < 0.001) (Table 2).
Adverse impact of blood transfusion in TKR
The significantly more deaths (at least 3-fold) were observed among patients receiving blood transfusion than those who did not require blood transfusion (0.2% vs. 0.8%; P < 0.001) (Table 2). The median length of hospital stay was extended by three days in the presence of blood transfusion (6 days vs. 3 days; P < 0.001) (Table 2). Consequently, the occurrence of blood transfusion was associated with an increase in medical expenses. Notably, there was a substantial rise of $34,731 in total hospital charges associated with blood transfusions ($121,039 vs. $86,308, P < 0.001) (Table 2).
Risk factors of blood transfusion for TKR
Logistic regression analysis was utilized to explore factors associated with blood transfusion, revealing the following indicators: advanced age (≥ 71 years, odds ratio [OR] = 1.49; 95% confidence interval [CI] = 1.38–1.61; P < 0.001), female (OR = 1.25; CI = 1.21–1.30), black (OR = 1.45; CI = 1.37–1.53), hispanic (OR = 1.380; CI = 1.28–1.47), large hospital (OR = 1.16; CI = 1.11–1.22) (Table 3), iron-deficiency anemia (OR = 2.43; CI = 2.32–2.55), rheumatoid arthritis/collagen vascular diseases (OR = 1.29; CI = 1.20–1.38), chronic blood loss anemia (OR = 2.72; CI = 2.42–3.06), congestive heart failure (OR = 1.40; CI = 1.31–1.50 ), coagulopathy (OR = 1.90; CI = 1.75–2.05), uncomplicated diabetes (OR = 1.15; CI = 1.10–1.20), lymphoma (OR = 2.00; CI = 1.59–2.51), fluid and electrolyte disorders (OR = 1.84; CI = 1.76–1.93), metastatic cancer (OR = 1.99; CI = 1.47–2.68), other neurological disorders (OR = 1.39; CI = 1.25–1.45), paralysis (OR = 1.72; CI = 1.39–2.17), peripheral vascular disorders (OR = 1.31; CI = 1.20–1.44), pulmonary circulation disorders (OR = 1.36; CI = 1.22–1.53), renal failure (OR = 1.45; CI = 1.37–1.54), valvular disease (OR = 1.24; CI = 1.15–1.34), weight loss (OR = 1.96; CI = 1.76–2.17) (Table 4). Interestingly, protective factors included private insurance (OR = 0.83; CI = 0.80–0.88), elective admission (OR = 0.511; CI = 0.49–0.53), teaching hospital (OR = 0.810; CI = 0.78–0.84), urban hospital (OR = 0.90; CI = 0.83–0.96), hospital in the Midwest or North Central (OR = 0.63; CI = 0.59–0.66), South (OR = 0.87; CI = 0.86–0.91), West (OR = 0.72; CI = 0.68–0.76) (Table 3) regions, and Obesity (OR = 0.81; CI = 0.78–0.84) (Table 4).
Factors associated with blood transfusions during TKR
Blood transfusions occurred more frequently in sepsis, acute myocardial infarction, deep vein thrombosis, convulsion, pulmonary embolism, gastrointestinal bleeding, heart failure, renal insufficiency, pneumonia, respiratory disease, wound infection, lower limb nerve injury, hemorrhage/seroma/hematoma, wound rupture/non healing, urinary tract infection, acute renal failure, postoperative delirium (P < 0.001) (Table 5). During multivariate analysis, blood transfusion was associated with sepsis (OR = 1.23; CI = 1.13–1.33), acute myocardial infarction (OR = 1.79; CI = 1.50–2.15), deep vein thrombosis (OR = 1.79; CI = 1.52–2.09), pulmonary embolism (OR = 1.55; CI = 1.24–1.94), gastrointestinal bleeding (OR = 3.13; CI = 2.39–4.10), heart failure (OR = 1.99; CI = 1.85–2.14), renal insufficiency (OR = 3.18; CI = 1.65–6.12), pneumonia (OR = 1.67; CI = 1.45–1.92), wound infection (OR = 1.57; CI = 1.35–1.83), lower limb nerve injury (OR = 1.67; CI = 1.51–1.85), hemorrhage/seroma/hematoma (OR = 2.36; CI = 2.13–2.62), wound rupture/non healing (OR = 1.44; CI = 1.30–1.60), urinary tract infection(OR = 2.09; CI = 1.94–2.26), acute renal failure (OR = 2.33; CI = 2.20–2.48), and postoperative delirium (OR = 1.85; CI = 1.61–2.14).
Discussion
This investigation presents a comprehensive health-economic analysis of patients undergoing in-hospital blood transfusion following total knee revision. Because of an increased focus on enhancing surgical techniques, component design, and the implementation of strict transfusion guidelines, clinical protocols for maintaining minimum preoperative Hb levels, as well as the implementation of new drugs, hemostatics and devices for hemostatics [15,16,17,18,19,20], there was a gradual decrease in blood transfusion rates from 2010 to 2019 (from 20.4 to 6.5%) (Fig. 2). The overall infection rate after TKA was 1.1% at 3 months and 1.6% at 1 year [21]; increased infections were associated with increased TKR rates. Effective management of TKR typically involves debridement, with or without implant removal, resulting in a complex and prolonged procedure and extended hospital stays [22]. In comparison to TKA, the transfusion rate in TKR is higher. Therefore, understanding the risk factors for transfusion in TKR is crucial for effective control [23, 24].
There is an increasing consensus suggesting that both older age and being female are linked to increased blood transfusion risk in the context of total knee revision [24,25,26]. In our investigation, older age (≥ 71 years) and being female emerged as independent risk factors for blood transfusion (Fig. 3A and B). This correlation may be attributed to older individuals having a higher prevalence of comorbidities and weakened hematopoietic function [25, 27]. Additionally, women are more prone to anemia, experience longer postoperative recovery cycles, and are at a heightened risk of complications [28]. During logistic regression analysis, compared to White individuals, the Black and Hispanic have a higher incidence of blood transfusions following TKR (Fig. 3C and D). Both Black and Hispanic patients have been shown to have lower levels of health literacy. Complex factors contribute to disparities, including diminished access to care that results in delayed patient presentations, substandard care, impaired clinician-patient communication, and insufficient post-hospital support systems [29]. Conversely, blood transfusions were less frequent in Asians or Pacific Islanders. This disparity may be attributed to higher rates of anemia, lower mean corpuscular volume, and lower serum transferrin saturation in this population, suggesting that racial or genetic heterogeneity might contribute to the likelihood of requiring blood transfusion [30, 31].

Patient demographics between the two surgical groups. A: Age distribution analysis of blood transfusion patients. B: Analysis of age distribution of patients without blood transfusion. C: Racial distribution analysis of blood transfusion patients. D: Racial distribution analysis of patients without blood transfusion
The literature has consistently reported that blood transfusion in the context of TKR is associated with extended length of stay, increased medical costs, and higher mortality rates [21, 32]. Consistent outcomes were found in the present study (Table 2). In the presence of blood transfusion, the median length of stay was extended by 3 days, and the total hospital charge per admission increased by $34,731, this may be due to blood transfusion itself, LOS and complications associated with blood transfusion [33,34,35]. Patients undergoing TKR via elective admission were less likely to experience blood transfusion, possibly because most elective cases involve individuals with relatively healthier conditions or adequate pre-operative preparations, while emergent cases tend to be more severe [36]. The likelihood of blood transfusion was higher in large hospitals but lower in small hospitals (Fig. 4A, B), potentially related to the complexity of surgeries and the higher volume of surgical patients [24]. In addition, teaching and urban hospitals emerged as protective factors against blood transfusion, possibly due to their standardized blood management practices, the use of drugs and equipment for bleeding control and blood management, and the skilled surgical techniques employed by their surgeons [37]. In-hospital mortality was three times higher in patients affected by blood transfusion compared to those unaffected. Regarding the hospital’s region, the Midwest or North Central, South, and West regions correlated with lower blood transfusion rates after TKR (Fig. 4C and D). However, the reasons for this remain unclear and are likely multifactorial [35].

Hospital characteristics between the two surgical groups. A: Analysis of the number of hospital beds for blood transfusion patients. B: Analysis of the number of hospital beds for patients without blood transfusion. C: Analysis of hospital regional distribution of blood transfusion patients. D: Analysis of hospital regional distribution of patients without blood transfusion
Numerous studies focusing on blood transfusion following TKA have emphasized the importance of pre-screening, risk stratification, and appropriate management to enhance outcomes [24, 38]. Consequently, to prevent the need for blood transfusion, it is crucial to comprehensively understand the preoperative risk factors. The utilization of logistic regression in our study yielded results consistent with prior research. As anticipated, iron deficient anemia and chronic blood loss anemia were identified as factors that can elevate the risk of blood transfusion, possibly linked to lower preoperative hemoglobin levels in patients [37, 39]. Maempel et al. [40] revealed that undergoing total knee arthroplasty were associated with a 6-fold increase in transfusion rates. However, patients with coagulopathy may experience significant blood loss during TKR, potentially leading to the necessity for blood transfusion [41].
Patient-related factors associated with blood transfusion in our study encompassed rheumatoid arthritis (RA)/collagen vascular diseases and uncomplicated diabetes (Fig. 5), both of which are systemic autoimmune disorders. This association may be attributed to the heightened susceptibility of these patients to preoperative anemia and low protein levels [42]. Congestive heart failure and valvular disease, known for inducing organ hypoxia, ischemia, and inadequate blood volume, were identified as factors increasing the likelihood of blood transfusion. However, the underlying cause of this relationship remains unknown. In our investigation, risk factors for blood transfusion included lymphoma, metastatic cancer, and weight loss (Fig. 5), indicating a relatively poor health condition that might be further exacerbated by intraoperative blood loss [43].

Incidence of preoperative comorbidities related to blood transfusion
Our results indicate that sepsis, acute myocardial infarction, deep vein thrombosis, pulmonary embolism, gastrointestinal bleeding, heart failure, renal insufficiency, pneumonia, urinary tract infection, acute renal failure, postoperative delirium, wound infection, lower limb nerve injury, hemorrhage/seroma/hematoma, wound rupture/non-healing were linked with blood transfusion (Fig. 6).

Incidence of postoperative complications related to blood transfusion
Consistent with the literature, our findings indicate that blood transfusion after TKR was associated with venous thromboembolism and pneumonia [44]. In TKR, patients experience loss of whole blood but are transfused with concentrated blood, potentially contributing to the higher viscosity of the transfused blood. Another explanation could be that the transfusion of stored erythrocytes itself influences the coagulative process [45]. It is widely thought that transfusion of red blood cell units stored for more than 20 days increases the venous thromboembolism risk [46]. Stored red blood cell units have been associated with reduced nitric oxide levels, leading to vasoconstriction, elevated lactate levels causing a decrease in pH, and the release of proinflammatory factors, all of which can impact coagulation and enhance hypercoagulability [47, 48].
Our study revealed that blood transfusion after TKR was associated with perioperative infectious complications including sepsis, wound infection, wound rupture/non-healing, urinary tract infection and pneumonia. In line with the findings of prior research, adverse effects occurred in blood transfusions [49, 50]. The effect of transfusions may have been in part related to low-dose bacterial contamination from the phlebotomy site and methods of blood handling and storage [51]. According to clinical experience, the infection patients are more likely to receive blood transfusions. Probably because infection with greater circulatory dysfunction, greater susceptibility to anemia and blood transfusions [52].Post-blood transfusion, there is an increased likelihood of renal insufficiency and acute renal failure, potentially stemming from that blood transfusions may increase the amount of circulating free iron and exacerbate the stress injury during surgery, which associated with renal organ damage [53]. However, red blood cell production and erythrocyte lifespan may be diminished in acute renal failure, resulting in anaemia and blood transfusion [54]. Additionally, blood transfusions was associated with acute myocardial infarction and heart failure, possibly due to changes in blood viscosity leading to an increased circulating blood volume and subsequent cardiac strain [55].And in patients with acute myocardial infarction, sustaining an elevated haemoglobin level may enhance clinical outcomes, potentially leading to transfusions, by enhancing oxygen delivery to the susceptible myocardium [45].The blood transfusions and complications that is an association and does not prove causality. The inference of causality between blood transfusion and adverse outcomes remains difficult due to methodological limitations of observational and database studies. Transfused patients are likely to have a higher degree of comorbidity, or postoperative complications, which may be the cause of the adverse outcome rather than the transfusion itself. Despite attempts to control for this confounding, causation cannot be proved. Thus, further validation through prospective studies is still needed for the given results [35].”
Our study has several limitations. Firstly, patient information was recorded only up to the point of discharge, suggesting that complications occurring after discharge are not recorded in the Nationwide Inpatient Sample database. Secondly, being a retrospective observational study, our investigation shares the limitations inherent in such designs. The NIS database lacks specific details, such as the volume of blood loss, pre-, peri-, postoperative hemoglobin values, or the number of units of blood transfused [7] and using of hemostatics. These limitations highlight that our results should be interpreted with caution, given that only data available in the NIS database could be analyzed. Indeed, certain well-established risk factors were not accessible in the Nationwide Inpatient Sample database, including details such as the type of anesthesia, duration of the operation, commonly used perioperative medications (opioids, benzodiazepines, and ketamine), sedation during anesthesia recovery, and functional impairment. Additionally, administrative data tends to exhibit high specificity (low false-positive rate) but low sensitivity (high false-negative rate) in identifying adverse events. This characteristic may lead to an underestimation of the incidence of blood transfusion following total knee revision [27].
Conclusion
Our findings indicate that the incidence of blood transfusion in TKR continued to decrease with an overall incidence of 13.0% between 2010 and 2019. Notwithstanding advancements, transfusions continue to transpire, with a higher incidence observed in female patients, older patients (≥ 71), patients afflicted with particular situation (e.g., iron deficiency anemia, chronic blood loss anemia, lymphoma, metastatic cancer, weight loss). Nevertheless, obesity was recognized as a protective factor. Additionally, gastrointestinal bleeding, renal insufficiency, urinary tract infection, hemorrhage/seroma/hematoma, and acute renal failure were all linked to blood transfusions. There is an association between blood transfusions and increased hospital costs and duration of stay. It is recommended that comprehensive preoperative assessment and medical optimization be performed on these patients, in addition to preoperative anemia management strategies, in order to reduce the likelihood of perioperative transfusion.
Data availability
The datasets are available at https://www.ahrq.gov/data/hcup/index.html.
Abbreviations
- Total knee arthroplasty:
-
TKA
- Total knee revision:
-
TKR
- Length of stay:
-
LOS
- Total joint arthroplasty:
-
TJA
- Nationwide inpatient sample:
-
NIS
- International classification of diseases:
-
ICD
- Figure:
-
Fig
- Statistical package for the social sciences:
-
SPSS
- Odds ratios:
-
OR
- Confidence intervals:
-
CI
- Rheumatoid arthritis:
-
RA
- Acquired immunodeficiency syndrome:
-
AIDS
References
Bin Abd Razak HR, Yung WYA. Postoperative delirium in patients undergoing total joint arthroplasty: a systematic review. J Arthroplasty. 2015;30(8):1414–7.
Carr AJ, Robertsson O, Graves S, Price AJ, Arden NK, Judge A, Beard DJ. Knee replacement. Lancet. 2012;379(9823):1331–40.
Blanco JF, Díaz A, Melchor FR, da Casa C, Pescador D. Risk factors for periprosthetic joint infection after total knee arthroplasty. Arch Orthop Trauma Surg. 2020;140(2):239–45.
Rodriguez-Merchan EC, Delgado-Martinez AD. Risk factors for Periprosthetic Joint Infection after primary total knee arthroplasty. J Clin Med 2022, 11(20).
Postler A, Lützner C, Beyer F, Tille E, Lützner J. Analysis of total knee arthroplasty revision causes. BMC Musculoskelet Disord. 2018;19(1):55.
Yang Q-F, Lin Z-M, Yang S, Wang P-K, Chen R, Wang J. Incidence and risk factors of In-Hospital prosthesis-related complications following total knee arthroplasty: a Retrospective Nationwide Inpatient Sample Database Study. Orthop Surg. 2021;13(5):1579–86.
Mistry JB, Gwam CU, Naziri Q, Pivec R, Abraham R, Mont MA, Delanois RE. Are allogeneic transfusions decreasing in total knee arthroplasty patients? National Inpatient Sample 2009–2013. J Arthroplasty. 2018;33(6):1705–12.
Kim JL, Park J-H, Han S-B, Cho IY, Jang K-M. Allogeneic blood transfusion is a significant risk factor for Surgical-Site infection following total hip and knee arthroplasty: a Meta-analysis. J Arthroplasty. 2017;32(1):320–5.
Kimball CC, Nichols CI, Vose JG. Blood transfusion trends in Primary and Revision Total Joint Arthroplasty: recent declines are Not Shared equally. J Am Acad Orthop Surg. 2019;27(20):e920–7.
Everhart JS, Sojka JH, Mayerson JL, Glassman AH, Scharschmidt TJ. Perioperative Allogeneic Red Blood-Cell Transfusion Associated with Surgical site infection after total hip and knee arthroplasty. J Bone Joint Surg Am. 2018;100(4):288–94.
Frisch N, Wessell NM, Charters M, Peterson E, Cann B, Greenstein A, Silverton CD. Effect of body Mass Index on blood transfusion in total hip and knee arthroplasty. Orthopedics. 2016;39(5):e844–9.
Gwam CU, Mistry JB, Mohamed NS, Thomas M, Bigart KC, Mont MA, Delanois RE. Current Epidemiology of Revision Total Hip Arthroplasty in the United States: National Inpatient Sample 2009 to 2013. J Arthroplasty. 2017;32(7):2088–92.
Menendez ME, Ring D, Barnes CL. Inpatient Dislocation after primary total hip arthroplasty. J Arthroplasty. 2016;31(12):2889–93.
Fineberg SJ, Nandyala SV, Marquez-Lara A, Oglesby M, Patel AA, Singh K. Incidence and risk factors for postoperative delirium after lumbar spine surgery. Spine (Phila Pa 1976). 2013;38(20):1790–6.
Ackerman SJ, Tapia CI, Baik R, Pivec R, Mont MA. Use of a bipolar sealer in total hip arthroplasty: medical resource use and costs using a hospital administrative database. Orthopedics. 2014;37(5):e472–81.
Aguilera X, Martinez-Zapata MJ, Bosch A, Urrútia G, González JC, Jordan M, Gich I, Maymó RM, Martínez N, Monllau JC, et al. Efficacy and safety of fibrin glue and tranexamic acid to prevent postoperative blood loss in total knee arthroplasty: a randomized controlled clinical trial. J Bone Joint Surg Am. 2013;95(22):2001–7.
Randelli F, D’Anchise R, Ragone V, Serrao L, Cabitza P, Randelli P. Is the newest fibrin sealant an effective strategy to reduce blood loss after total knee arthroplasty? A randomized controlled study. J Arthroplasty. 2014;29(8):1516–20.
Suh DW, Han S-B, Park J-H, Cheong K, Kyung BS. Intravenous iron supplementation with intra-articular administration of tranexamic acid reduces the rate of allogeneic transfusions after simultaneous bilateral total knee arthroplasty. Blood Transfus. 2017;15(6):506–11.
Helito CP, Bonadio MB, Sobrado MF, Giglio PN, Pécora JR, Camanho GL, Demange MK. Comparison of Floseal® and Tranexamic Acid for Bleeding Control after total knee arthroplasty: a prospective Randomized Study. Clin (Sao Paulo). 2019;74:e1186.
Kim E, Kim S, Kwon YW, Seo H, Kim M, Chung WG, Park W, Song H, Lee DH, Lee J et al. Electrical stimulation for therapeutic approach. Interdisciplinary Med 2023, 1(2).
Rhee C, Lethbridge L, Richardson G, Dunbar M. Risk factors for infection, revision, death, blood transfusion and longer hospital stay 3 months and 1 year after primary total hip or knee arthroplasty. Can J Surg. 2018;61(3):165–76.
Daines BK, Dennis DA, Amann S. Infection prevention in total knee arthroplasty. J Am Acad Orthop Surg. 2015;23(6):356–64.
López-Contreras J, Limón E, Matas L, Olona M, Sallés M, Pujol M. Epidemiology of surgical site infections after total hip and knee joint replacement during 2007–2009: a report from the VINCat Program. Enferm Infecc Microbiol Clin. 2012;30(Suppl 3):26–32.
Jeschke E, Citak M, Halder AM, Heller K-D, Niethard FU, Schräder P, Zacher J, Leicht H, Malzahn J, Günster C, et al. Blood transfusion and venous thromboembolism trends and risk factors in primary and aseptic revision total hip and knee arthroplasties: a nationwide investigation of 736,061 cases. Orthop Traumatol Surg Res. 2022;108(1):102987.
Slover J, Lavery JA, Schwarzkopf R, Iorio R, Bosco J, Gold HT. Incidence and risk factors for blood transfusion in total joint arthroplasty: analysis of a Statewide Database. J Arthroplasty 2017, 32(9).
To J, Sinha R, Kim SW, Robinson K, Kearney B, Howie D, To LB. Predicting Perioperative Transfusion in Elective hip and knee arthroplasty: a validated predictive model. Anesthesiology. 2017;127(2):317–25.
Song K, Pan P, Yao Y, Jiang T, Jiang Q. The incidence and risk factors for allogenic blood transfusion in total knee and hip arthroplasty. J Orthop Surg Res. 2019;14(1):273.
Cao G, Huang Z, Huang Q, Zhang S, Xu B, Pei F. Incidence and risk factors for blood transfusion in simultaneous bilateral total joint arthroplasty: a Multicenter Retrospective Study. J Arthroplasty. 2018;33(7):2087–91.
Upfill-Brown A, Paisner N, Sassoon A. Racial disparities in post-operative complications and discharge destination following total joints arthroplasty: a national database study. Arch Orthop Trauma Surg. 2023;143(4):2227–33.
Roth TM, Gustilo-Ashby T, Barber MD, Myers ER. Effects of race and clinical factors on short-term outcomes of abdominal myomectomy. Obstet Gynecol. 2003;101(5 Pt 1):881–4.
Rogers MAM, Blumberg N, Heal JM, Langa KM. Utilization of blood transfusion among older adults in the United States. Transfusion. 2011;51(4):710–8.
Hart A, Khalil JA, Carli A, Huk O, Zukor D, Antoniou J. Blood transfusion in primary total hip and knee arthroplasty. Incidence, risk factors, and thirty-day complication rates. J Bone Joint Surg Am. 2014;96(23):1945–51.
Sherrod BA, Baker DK, Gilbert SR. Blood transfusion incidence, risk factors, and Associated complications in Surgical Treatment of Hip Dysplasia. J Pediatr Orthop. 2018;38(4):208–16.
Carson JL, Sieber F, Cook DR, Hoover DR, Noveck H, Chaitman BR, Fleisher L, Beaupre L, Macaulay W, Rhoads GG, et al. Liberal versus restrictive blood transfusion strategy: 3-year survival and cause of death results from the FOCUS randomised controlled trial. Lancet. 2015;385(9974):1183–9.
Browne JA, Adib F, Brown TE, Novicoff WM. Transfusion rates are increasing following total hip arthroplasty: risk factors and outcomes. J Arthroplasty. 2013;28(8 Suppl):34–7.
Yang Q, Wang J, Xu Y, Chen Y, Lian Q, Zhang Y. Incidence and risk factors of in-hospital prosthesis-related complications following total hip arthroplasty: a retrospective Nationwide Inpatient Sample database study. Int Orthop. 2020;44(11):2243–52.
Viola J, Gomez MM, Restrepo C, Maltenfort MG, Parvizi J. Preoperative anemia increases postoperative complications and mortality following total joint arthroplasty. J Arthroplasty. 2015;30(5):846–8.
Khan H, Dhillon K, Mahapatra P, Popat R, Zakieh O, Kim WJ, Nathwani D. Blood loss and transfusion risk in robotic-assisted knee arthroplasty: a retrospective analysis. Int J Med Robot. 2021;17(6):e2308.
Newman JM, Webb MR, Klika AK, Murray TG, Barsoum WK, Higuera CA. Quantifying blood loss and transfusion risk after primary vs Conversion Total Hip Arthroplasty. J Arthroplasty. 2017;32(6):1902–9.
Maempel JF, Wickramasinghe NR, Clement ND, Brenkel IJ, Walmsley PJ. The pre-operative levels of haemoglobin in the blood can be used to predict the risk of allogenic blood transfusion after total knee arthroplasty. Bone Joint J. 2016;98–B(4):490–7.
Clevenger B, Mallett SV. Transfusion and coagulation management in liver transplantation. World J Gastroenterol. 2014;20(20):6146–58.
Ravi B, Croxford R, Hollands S, Paterson JM, Bogoch E, Kreder H, Hawker GA. Increased risk of complications following total joint arthroplasty in patients with rheumatoid arthritis. Arthritis Rheumatol. 2014;66(2):254–63.
Azmy MC, Pinto J, Patel NM, Govindan A, Kalyoussef E. Risk factors for blood transfusion with Neck Dissection. Otolaryngol Head Neck Surg. 2019;161(6):922–8.
Thurn L, Wikman A, Lindqvist PG. Postpartum blood transfusion and hemorrhage as independent risk factors for venous thromboembolism. Thromb Res. 2018;165:54–60.
Carson JL, Brooks MM, Chaitman BR, Alexander JH, Goodman SG, Bertolet M, Abbott JD, Cooper HA, Rao SV, Triulzi DJ, et al. Rationale and design for the myocardial ischemia and transfusion (MINT) randomized clinical trial. Am Heart J. 2023;257:120–9.
Spinella PC, Carroll CL, Staff I, Gross R, Mc Quay J, Keibel L, Wade CE, Holcomb JB. Duration of red blood cell storage is associated with increased incidence of deep vein thrombosis and in hospital mortality in patients with traumatic injuries. Crit Care. 2009;13(5):R151.
Lelubre C, Vincent J-L. Relationship between red cell storage duration and outcomes in adults receiving red cell transfusions: a systematic review. Crit Care. 2013;17(2):R66.
Esmon CT. The impact of the inflammatory response on coagulation. Thromb Res. 2004;114(5–6):321–7.
Schoettker P, Marcucci CE, Casso G, Heim C. Revisiting transfusion safety and alternatives to transfusion. Presse Med. 2016;45(7–8 Pt 2):e331–40.
Husted H, Holm G, Jacobsen S. Predictors of length of stay and patient satisfaction after hip and knee replacement surgery: fast-track experience in 712 patients. Acta Orthop. 2008;79(2):168–73.
Vamvakas EC, Blajchman MA. Blood still kills: six strategies to further reduce allogeneic blood transfusion-related mortality. Transfus Med Rev 2010, 24(2).
Cao X, Liu X, Zhang X, Zhang K, Chen C, Yang Q, Wang J, Li X, Wei L. Risk factors for perioperative blood transfusion in patients undergoing total laparoscopic hysterectomy. BMC Womens Health. 2024;24(1):65.
Vincent J-L, Lelubre C. Preoperative transfusions to limit the deleterious effects of blood transfusions. Anesthesiology. 2012;116(3):513–4.
Oppert M, Jörres A. Transfuse or not transfuse in acute renal failure? This is the question. Intensive Care Med. 2005;31(11):1469–70.
Ducrocq G, Gonzalez-Juanatey JR, Puymirat E, Lemesle G, Cachanado M, Durand-Zaleski I, Arnaiz JA, Martínez-Sellés M, Silvain J, Ariza-Solé A, et al. Effect of a restrictive vs liberal blood transfusion strategy on Major Cardiovascular events among patients with Acute myocardial infarction and Anemia: the REALITY randomized clinical trial. JAMA. 2021;325(6):552–60.
Acknowledgements
None.
Funding
This work was supported by the President Foundation of Nanfang Hospital, Southern Medical University [2021]33 and the Guangdong Provincial Department of Education [2021]29.
Author information
Authors and Affiliations
Contributions
Visualization, Writing - Original Draft, Data Curation: XL, HX. Validation: JW, ZS, QY. Resources: LB. Writing - Review: SL. Conceptualization, Methodology, Writing - Review & Editing, Supervision: LB, QL, QY.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, X., Xie, H., Liu, S. et al. Analysis of the incidence and risk factors of blood transfusion in total knee revision: a retrospective nationwide inpatient sample database study. BMC Musculoskelet Disord 25, 225 (2024). https://doi.org/10.1186/s12891-024-07331-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07331-2