
Abstract
Background
Postoperative delirium (POD) is a common surgical complication. However, the incidence and risk factors associated with postoperative delirium after revision total knee arthroplasty (rTKA) have not been comprehensively explored through extensive national databases.
Methods
Utilizing the National Inpatient Sample (NIS), the largest comprehensive U.S. hospital healthcare database, we undertook a retrospective investigation involving 127,400 patients who underwent rTKA between 2010 and 2019. We assessed various aspects, including patient demographics, hospital characteristics, pre-existing medical conditions, and perioperative complications.
Results
The overall incidence of postoperative delirium (POD) in patients undergoing rTKA between 2010 and 2019 was 0.97%. The highest incidence rate of 1.31% was recorded in 2013. Notably, this patient cohort demonstrated advanced age, increased burden of co-morbidities, prolonged hospital stays, increased hospitalization costs, and elevated in-hospital mortality rates (P < 0.001). Moreover, non-elective admissions, non-private insurance payments, and a preference for teaching hospitals were commonly observed among these patients. During their hospitalization, individuals who developed delirium subsequent to rTKA were more prone to experiencing certain perioperative complications. These complications encompassed medical issues like acute myocardial infarction, continuous invasive mechanical ventilation, postoperative shock, sepsis, stroke and other medical problems. Additionally, surgical complications including hemorrhage / seroma / hematoma, irrigation and debridement, prosthetic joint infection, periprosthetic fracture, and wound dehiscence / nonunion were noted. Several risk factors were found to be linked with the development of POD. These included advanced age (≥ 75 years), alcohol abuse, coagulation disorders, congestive heart failure, depression, fluid and electrolyte imbalances, and more. Conversely, female sex, having private insurance, and undergoing elective hospitalization emerged as protective factors against POD.
Conclusion
Our findings suggest that the general prevalence of POD in rTKA is relatively low according to NIS. There was a significant connection between the POD of rTKA and advanced age, prolonged length of stay (LOS), more in-patients’ costs, higher in-hospital mortality rate, increased comorbidities, postoperative medical complications and postoperative surgical complications. This study helps to understand the risk factors associated with POD to improve poor outcomes.
Similar content being viewed by others

Background
TKAs are performed more than 1,000,000 per year in the United States, remaining among the most successful modern surgical procedures to preserve the function of the joint and alleviate pain [1, 2]. However, as indicated by the NIS analysis, the demand for rTKA is projected to surge by 601%, soaring from 38,300 cases in 2005 to a staggering 268,200 cases by the year 2030 [2]. Furthermore, the projected burden for TKA revisions is anticipated to reach 7.2% by the year 2030. This revision burden is attributed to various factors, including aseptic loosening (29.8%), septic loosening (14.8%), pain (9.5%), wear (8.2%), and other causes [2, 3]. Additionally, a significant proportion of postoperative patients will develop postoperative complications.
Delirium is a neurological syndrome with complex and unclear etiology and pathogenesis, which is characterized by decreased cognitive function, consciousness or perception [4,5,6]. This acute alteration in mental status includes the inability to focus or keep attention and disorientation, and memory deterioration, which is associated with the brain’s maladaptive response to surgical stress [5,6,7,8]. POD remains a common complication for perioperative clinicians and geriatric patients, especially given its association with total joint arthroplasty (TJA) [1, 9, 10]. Notably, it is a significant source of progressive injury, higher mortality, long-term cognitive impairment, and incidence of complications, with a burdensome possession on patients, their family members, and society in all aspects [5, 11,12,13,14,15]. For nearly 2.4 billion elderly patients nationally, total direct 1-year health care costs attributable to delirium at the expense of between $143 billion and $152 billion annually because of increased morbidity and mortality, worse surgical outcomes, and more extended hospital stays [16,17,18,19]. Moreover, in addition to the acute episodes of POD, perioperative disturbances of cognition may also be manifested as postoperative cognitive decline (POCD) after hospital discharge [20]. Unlike POD, it is not a clinical diagnosis which is defined as a decline in performance on cognitive tests compared with preoperative performance [21]. POD has been reported to be a strong predictor of the development of POCD, so interventions to prevent delirium may help reduce the risk of POCD [22].
Therefore, to improve postoperative adverse outcomes and prevent other complications, it is vital to identify patients at high risk of POD preoperatively [1, 23, 24]. Advanced age, potential surgical risk factors, and the need for comprehensive pharmacological pain management interventions may be the driving factors for the occurrence of POD in orthopedic surgery [25,26,27,28,29]. Other risk factors reported in the literature contain a history of Parkinson’s disease or psychiatric disorders, cognitive impairment, depression, diabetes mellitus, and postoperative water and electrolyte disturbances [1, 23, 28, 30,31,32,33]. Besides, risk factors for POD in joint arthroplasty have been reported to include advanced age, diabetes, depression, fluid and electrolyte disorders, hypertension, neurological disorders, renal failure, weight loss, and other comorbidities in previous studies [34,35,36]. Nonetheless, up to now, there is no nationwide, large database research on the risk factors and incidence of POD following rTKA.
As a result, according to a large national database from the United States, our research aimed to inquire into delirium’s incidence and associated risk factors after rTKA. We hypothesized that the incidence of POD has generally trended downwards over the last decade, and additional risk factors will be identified in a large national database or by expanding the observational variables. This could help to identify patient groups that may require preoperative optimization.
Methods
Data source
This study used the largest US fully paid inpatient database, the NIS database, part of a Healthcare Utilization Project (HCUP) database. The HCUP is a series of databases funded by the Agency for Healthcare Research and Quality (AHRQ) that provides the most comprehensive American hospital data. The NIS collects stratified samples from more than 1,000 hospitals in 46 states, representing nearly 20% of the annual US hospital admissions [37]. We obtained information from the database on patient demographics, admission status, outcomes (including in-hospital mortality rate and LOS) for each sampled hospitalization, diagnoses, procedures, and comorbidities in the International Classification of Diseases (Ninth Edition) Clinical Modification (ICD-9-CM) and International Classification of Diseases (Tenth Edition) Clinical Modification (ICD-10-CM).
Data collection
We identified all patients in the NIS database who were 18 years of age or older from January 1, 2010, to December 31, 2019, with the ICD-9-CM rTKA procedure codes (00.80/00.81/00.82/00.83/00.84/81.55) and the ICD-10-CM rTKA procedure codes (0SWC/0SWD/0SWT/0SWU/0SWV/0SWW). Patients with delirium were diagnosed and selected according to ICD-9-CM diagnostic codes, including altered mental state (780.97), acute, subacute, and transient delirium (293, 293.0, 293.1, 293.8, 293.81, 293.82, 293.83, 293.84, 293.89, 293.9), and drug-induced delirium (292.81), as well as the ICD-10-CM diagnostic code (F05/R41.82/F06.0/F06.2). Exclusion criteria and the data collection process are outlined in Fig. 1. After rigorous screening, no outliers were found in the NIS database.

Analysis plan
We divided patients into two groups based on whether they developed POD. Their demographic data, such as age, race, sex, and outcome measurements, including admission mode, LOS, total hospitalization cost, insurance type, in-hospital mortality, and 29 variables of comorbidities (based on the NIS database), were analyzed (Table 1). The ICD-9-CM and ICD-10-CM diagnostic codes were used to obtain medical and surgical perioperative complications that may be independently related to POD before discharge. Perioperative medical complications included acute myocardial infarction, acute postoperative pain, acute renal failure, blood transfusion, cardiac arrest, continuous invasive mechanical ventilation, convulsions, deep venous thrombosis, pneumonia, postoperative shock, sepsis, stroke, and urinary tract infection. Perioperative surgical complications included hemorrhage/seroma/hematoma, irrigation and debridement, lower limb nerve injury, periprosthetic fracture, prosthesis joint dislocation, periprosthetic joint infection, and wound dehiscence/non-healing.
Data analysis
All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) version 25 (IBM SPSS Statistics, USA). The Kolmogorov-Wilk normality test was used for quantitative data such as age, LOS and total hospitalization cost, and it was found that they did not meet the normal distribution, so rank sum test was used instead of T-test. The two groups were compared using the Wilcoxon rank-sum test for continuous data and the chi-square test for categorical data. We developed univariate and multivariate logistic regression models (the Enter type) to evaluate the relationship between POD and perioperative complications. Then, binary logistic regression analysis (the Enter type) was applied to determine the independent risk factors of POD and its relationship with other complications. The regression analysis included all variables (Table 1). Given that other NIS studies have utilized substantial sample sizes, the statistical significance level was established at P ≤ 0.001 for alpha [38].
Results
Incidence of postoperative delirium in rTKA patients
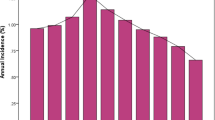
There were 127,400 rTKAs in the NIS database, of which 1232 patients developed POD, with an overall prevalence of 0.97% from 2010 through 2019 (Table 2). We observed that the incidence of delirium after rTKA increased yearly from 2010 (1.20%) to 2013 (1.31%). (Fig. 2 and Table 2), while from 2013 (1.31%) to 2019 (0.72%), the incidence of POD generally showed a downward trend, and at least to 2016 (0.61%) (Fig. 2 and Table 2).

Annual incidence of postoperative delirium in patients undergoing rTKA
Demographic and hospital characteristics of patients in the two groups
The age of patients with POD (66–80 years) was older than that of patients without POD (58–73 years), and the difference was statistically significant (P < 0.001). Otherwise, the difference in age distribution between the two groups was statistically significant, and the incidence of POD was significantly higher in patients older than 75. (P < 0.001) (Table 3). Conceivably, in-hospital mortality rate increased from 0.24% to 1.79% in patients with POD. Moreover, there was a significant difference in the number of comorbidities patients had, with a significantly higher incidence in patients with CCI ≥ 3 (97.48% vs. 81.74%) (Fig. 3C & D). The median LOS for patients with delirium was longer than those without POD (6 vs. 4 days), and the median total hospitalization cost increased by $26,691.5 ($100,480 vs. $73,788.5). In addition, the choice of insurance type was also different between the two groups, and POD patients preferred Medicare more significantly (82.39% vs. 59.08%). Patients with POD were also less likely to have elective admissions (58.60% vs. 81.35%) and were more likely to prefer teaching hospitals (67.05% vs. 61.67%). Beyond that, there was no significant difference in sex, race, hospital bed size, hospital location and region of hospital (Table 3 and Fig. 3E & F and Fig. 4).

Patient demographics and hospital characteristics between the two surgical groups. A Age distribution analysis of non-delirium patients. B Analysis of age distribution of patients with delirium. C Analysis of the number of comorbidities for non-delirium patients. D Analysis of the number of comorbidities for patients with delirium. E Racial distribution analysis of non-delirium patients. F Racial distribution analysis of delirium patients

Incidence of postoperative complications related to postoperative delirium. A Analysis of hospital regional distribution of non-delirium patients. B Analysis of hospital regional distribution of delirium patients. C Analysis of insurance types for non-delirium patients. D Analysis of insurance types for patients with delirium. E Analysis of the number of hospital beds for non-delirium patients. F Analysis of the number of hospital beds for patients with delirium
Relationship between other postoperative complications and postoperative delirium
The patient with POD receiving rTKA was possibly easier to suffer acute myocardial infarction (2.27%), acute renal failure (25.16%), blood transfusion (29.46%), continuous invasive mechanical ventilation (2.11%), deep vein thrombosis (2.84%), pneumonia (3.98%), postoperative shock (0.49%), sepsis (14.29%), stroke (2.19%), urinary tract infection (12.42%), hemorrhage/seroma/hematoma (3.57%), irrigation and debridement (3.08%), periprosthetic fracture (2.03%), prosthetic joint infection (29.62%), and wound dehiscence/non-healing (3.57%) than those without POD (P ≤ 0.001) (Fig. 5 and Table 4). On the side, multiple regression analysis suggested that POD was related to acute renal failure (OR = 2.72; CI = 2.34–3.17), blood transfusion (OR = 1.86; CI = 1.63–2.12),pneumonia (OR = 1.75; CI = 1.27–2.41), sepsis (OR = 1.81; CI = 1.49–2.19), stroke (OR = 2.57; CI = 1.71–3.85), urinary tract infection (OR = 2.35; CI = 1.96–2.83), fracture (OR = 2.10; CI = 1.39–3.16), periprosthetic and prosthetic joint dislocation (OR = 1.51; CI = 1.18–1.94), prosthetic joint infection (OR = 1.46; CI = 1.27–1.68) (Table 5).

Incidence of postoperative complications related to postoperative delirium
Risk factors related to postoperative delirium after rTKA
We used logistic regression analysis to explore risk factors related to POD, and the results were as follows (Table 5): advanced age (≥ 75 years, OR = 2.43; 95% CI = 2.13–2.79;P < 0.001), neurological disorders (OR = 18.05; CI = 15.97–20.41), psychoses (OR = 1.97; CI = 1.56–2.49), alcohol abuse (OR = 1.80; CI = 1.27–2.54), fluid and electrolyte disorders (OR = 1.79; CI = 1.56–2.06), pulmonary circulation disorders (OR = 1.69; CI = 1.28–2.21), and weight loss (OR = 1.66; CI = 1.29–2.13).coagulopathy (OR = 1.55; CI = 1.25–1.92), congestive heart failure (OR = 1.33; CI = 1.12–1.59), depression (OR = 1.28; CI = 1.11–1.48), On the other side, there were three protective factors related to POD, female sex (OR = 0.76; CI = 0.67–0.87, P < 0.001), elective admission (OR = 0.69; CI = 0.61–0.79, P < 0.001), and private insurance (OR = 0.62; CI = 0.51–0.75, P < 0.001).
Discussion
We illustrate the outcomes of a large health economic study of POD on patients undergoing rTKA. From 2010 to 2019, the incidence of POD increased yearly and decreased after 2013, ranging from 0.61 to 1.31% (Fig. 2). Noteworthily, the previous literature has yet to report such a trend. Two possible explanations exist for the increased incidence of POD in rTKA observed before 2013. First, this may have been caused by investigators’ increasing awareness of POD, since although the clinical definition of POD remains unchanged, its diagnosis (based on the ICD-9-CM) may vary according to their experience and recognition [38]. Another potential reason could be the increasing number of rTKA procedures as the population ages. However, inadequate knowledge of rTKA and management of medical interventions, immature anesthetic procedures, and even pain-relief protocols can lead to a higher incidence of POD. Since then, a growing amount of attention has been paid to POD, the continuous improvement of rTKA surgery, and the update of the ICD-10-CM code, which reversed this trend after 2013 [38, 39].
The overall incidence of POD in rTKA is 0.97% in this study, much lower than the incidence after TJA (5%-14.3%) reported in the literature [1]. Song et al. discovered a 14.6% incidence after rTKA in Seoul Sacred Heart General Hospital patients [40]. Moreover, Meyer et al. observed that, in Regensburg University Hospital, the incidence after rTKA was 22.4% [41]. We propose the following possible hypotheses to explain our significant differences. First, most previous studies have possessed the limitation of small sample sizes and an overrepresentation of elderly patients, which contributed to an overestimation of the POD incidence. Then, there are differences in the accuracy of POD diagnosis among different researchers and institutions, which will also affect the results [38, 39]. Finally, the hypoactive form of delirium is difficult to diagnose.
We observed that, in terms of demographics, patients with POD had a median age that was 8 years higher compared to those without POD (Table 3). Furthermore, we concluded from the logistic regression analysis that advanced age (≥ 75 years) was one of the independent risk factors for POD (Table 5). Coincidentally, in clinical work, it is not difficult to find that POD is a common complication in elderly patients. It has been previously reported that advanced age is a recognized predictor of POD, consistent with our data analysis results [42]. Nevertheless, the mechanisms by which advanced age leads to disturbance of consciousness and brain dysfunction need further investigation. A recent article reported that gut microbiota is connected with the pathogenesis of nervous system diseases. Anesthesia/surgery may promote the development of POD-like behavior in mice by inducing age-dependent changes in gut microbiota (reduction of lactobacillus). Therefore, the changes in intestinal flora in elderly patients after surgery may be an influencing factor leading to postoperative neurocognitive dysfunction [43].
The significantly higher comorbidity scores in POD patients are reasonable and justified because they may suffer from relatively poor preoperative health and more severe postoperative complications [1, 28]. We suggested an increased financial burden and a higher risk of POD, consistent with past documentation reports (Table 3). As noted above, POD increased the median LOS by 2 days at a total cost of US $26,691.5 per hospitalization. One possible explanation is a failure to manage and heal patients with POD according to guidelines [38]. Another possibility is that POD is often associated with postoperative perioperative complications, such as acute myocardial infarction, acute renal failure, continuous invasive mechanical ventilation, and deep vein thrombosis, which tend to delay discharge and prolong hospital stay (Table 4) [37].
Logistics regression showed that private insurance was considered a POD’s protective factor (Table 5). A possible explanation is that the purchase of private insurance symbolizes a good economic situation for the patient and plays a positive role in the prevention and treatment of POD. Additionally, we found a lower incidence of delirium in rTKA patients with elective admission (Table 3). Furthermore, logistic regression analysis showed that it was also a protective factor (Table 5). Patients admitted on an elective basis tend to be more physically fit or have received adequate preoperative evaluation and preparation [44]. Correspondingly, in emergency situations such as public health events and the sudden occurrence of prosthesis-related complications, the number of elective surgery patients will be greatly reduced [44, 45], which will increase the risk of postoperative complications such as delirium. As a result, in-hospital mortality is much higher among patients with delirium than among those without delirium. Otherwise, it is interesting that female sex was found to be a protective factor for reasons that are not known but have been reported previously (Table 5) [46]. One possible reason is that melatonin is considered helpful in preventing delirium, and female hormones have a modulatory effect on its secretion [47, 48].
Identifying the preoperative risk factors of POD for prevention and treatment is significant. Some studies on POD after TJA have pointed out that accurate screening, risk assessment, and proper management are beneficial to optimize the prognosis [1, 23]. The logistic regression analysis results used in this paper were consistent with those of previous literature. Other complications have been reported previously, such as alcohol abuse, depression, psychoses, fluid and electrolyte disorders and weight loss (Table 5) [31, 38, 49].
This study has the following limitations. First, the NIS database contains only information recorded before hospital discharge, which would lead to an underestimation of the incidence of POD. Because this limitation will impact the research on patients’ complications after discharge. Second, other known risk factors, such as a history of dementia, visual impairment, anesthesia method, sedation during recovery from anesthesia, and common perioperative medications (opioids, ketamine, and benzodiazepines), were not available in the NIS database [30, 33, 50]. In addition, coding and documentation may have discrepancies or errors as with other extensive databases. Administrative data are characterized by high specificity and low sensitivity for identifying adverse events. It may also have an impact on the findings [38, 39].
Conclusions
POD incidence increased yearly from 2010 (1.20%) to 2013 (1.31%) and then showed a downward trend to 2019 (0.72%), with a minimum of 0.61% in 2016. The occurrence of delirium after rTKA was related to increased LOS, total hospitalization cost, hospital mortality and number of comorbidities. POD was also associated with perioperative medical complications (e.g., acute myocardial infarction, pneumonia and stroke) and perioperative surgical complications (e.g., prosthetic joint infection, periprosthetic fracture, and wound dehiscence/non-healing). The risk factors were identified (e.g., advanced age (≥ 75 years), coagulopathy, and weight loss). Understanding risk factors connected with POD to ameliorate adverse outcomes and ensure appropriate management is conductive.
Availability of data and materials
This study is based on data provided by Nationwide Inpatient Sample (NIS) database, part of the Healthcare Cost and Utilization Project, Agency for Healthcare Research and Quality. The NIS database is a large publicly available full-payer inpatient care database in the United States and the direct web link to the database is https://www.hcup-us.ahrq.gov/db/nation/nis/nisdbdocumentation.jsp. Therefore, individual or grouped data cannot be shared by the authors.
Abbreviations
- POD:
-
Postoperative delirium
- rTKA:
-
Revision total knee arthroplasty
- NIS:
-
National Inpatient Sample
- LOS:
-
Length of stay
- CCI:
-
Charlson comorbidity index
- HCUP:
-
Healthcare Utilization Project
- ICD-9-CM:
-
International Classification of Diseases (Ninth Edition) Clinical Modification
- ICD-10-CM:
-
International Classification of Diseases (Tenth Edition) Clinical Modification
References
Bin Abd Razak HR. Yung WY: postoperative delirium in patients undergoing total joint arthroplasty: a systematic review. J Arthroplasty. 2015;30(8):1414–7.
Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780–5.
Sadoghi P, Liebensteiner M, Agreiter M, Leithner A, Böhler N, Labek G. Revision surgery after total joint arthroplasty: a complication-based analysis using worldwide arthroplasty registers. J Arthroplasty. 2013;28(8):1329–32.
Maclullich AM, Ferguson KJ, Miller T, de Rooij SE, Cunningham C. Unravelling the pathophysiology of delirium: a focus on the role of aberrant stress responses. J Psychosom Res. 2008;65(3):229–38.
Postoperative delirium in older adults. best practice statement from the American Geriatrics Society. J Am Coll Surg. 2015;220(2):136-148.e131.
Rengel KF, Pandharipande PP, Hughes CG. Postoperative delirium. Presse Med. 2018;47(4 Pt 2):e53–64.
Choi YH, Kim DH, Kim TY, Lim TW, Kim SW, Yoo JH. Early postoperative delirium after hemiarthroplasty in elderly patients aged over 70 years with displaced femoral neck fracture. Clin Interv Aging. 2017;12:1835–42.
Rai D, Garg RK, Malhotra HS, Verma R, Jain A, Tiwari SC, Singh MK. Acute confusional state/delirium: An etiological and prognostic evaluation. Ann Indian Acad Neurol. 2014;17(1):30–4.
Aranake-Chrisinger A, Avidan MS. Postoperative delirium portends descent to dementia. Br J Anaesth. 2017;119(2):285–8.
Zenilman ME. Delirium: An Important Postoperative Complication. JAMA. 2017;317(1):77–8.
Gottesman RF, Grega MA, Bailey MM, Pham LD, Zeger SL, Baumgartner WA, Selnes OA, McKhann GM. Delirium after coronary artery bypass graft surgery and late mortality. Ann Neurol. 2010;67(3):338–44.
Jankowski CJ, Trenerry MR, Cook DJ, Buenvenida SL, Stevens SR, Schroeder DR, Warner DO. Cognitive and functional predictors and sequelae of postoperative delirium in elderly patients undergoing elective joint arthroplasty. Anesth Analg. 2011;112(5):1186–93.
Fong TG, Jones RN, Marcantonio ER, Tommet D, Gross AL, Habtemariam D, Schmitt E, Yap L, Inouye SK. Adverse outcomes after hospitalization and delirium in persons with Alzheimer disease. Ann Intern Med. 2012;156(12):848–56, w296.
Saczynski JS, Marcantonio ER, Quach L, Fong TG, Gross A, Inouye SK, Jones RN. Cognitive trajectories after postoperative delirium. N Engl J Med. 2012;367(1):30–9.
Gleason LJ, Schmitt EM, Kosar CM, Tabloski P, Saczynski JS, Robinson T, Cooper Z, Rogers SO Jr, Jones RN, Marcantonio ER, Inouye SK. Effect of delirium and other major complications on outcomes after elective surgery in older adults. JAMA Surg. 2015;150(12):1134–40.
Leslie DL, Marcantonio ER, Zhang Y, Leo-Summers L, Inouye SK. One-year health care costs associated with delirium in the elderly population. Arch Intern Med. 2008;168(1):27–32.
Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet (London, England). 2014;383(9920):911–22.
Inouye SK, Marcantonio ER, Kosar CM, Tommet D, Schmitt EM, Travison TG, Saczynski JS, Ngo LH, Alsop DC, Jones RN. The short-term and long-term relationship between delirium and cognitive trajectory in older surgical patients. Alzheimer’s & dementia : the journal of the Alzheimer’s Association. 2016;12(7):766–75.
Rong X, Ding ZC, Yu HD, Yao SY, Zhou ZK. Risk factors of postoperative delirium in the knee and hip replacement patients: a systematic review and meta-analysis. J Orthop Surg Res. 2021;16(1):76.
Daiello LA, Racine AM, Yun Gou R, Marcantonio ER, Xie Z, Kunze LJ, Vlassakov KV, Inouye SK, Jones RN, Alsop D, et al. Postoperative Delirium and Postoperative Cognitive Dysfunction: Overlap and Divergence. Anesthesiology. 2019;131(3):477–91.
Feinkohl I, Janke J, Slooter AJC, Winterer G, Spies C, Pischon T. Metabolic syndrome and the risk of postoperative delirium and postoperative cognitive dysfunction: a multi-centre cohort study. Br J Anaesth. 2023;131(2):338–47.
Glumac S, Kardum G, Karanovic N. Postoperative Cognitive Decline After Cardiac Surgery: A Narrative Review of Current Knowledge in 2019. Med Sci Monit. 2019;25:3262–70.
Kalisvaart KJ, Vreeswijk R, de Jonghe JF, van der Ploeg T, van Gool WA, Eikelenboom P. Risk factors and prediction of postoperative delirium in elderly hip-surgery patients: implementation and validation of a medical risk factor model. J Am Geriatr Soc. 2006;54(5):817–22.
Nandi S, Harvey WF, Saillant J, Kazakin A, Talmo C, Bono J. Pharmacologic risk factors for post-operative delirium in total joint arthroplasty patients: a case-control study. J Arthroplasty. 2014;29(2):268–71.
Papaioannou A, Fraidakis O, Michaloudis D, Balalis C, Askitopoulou H. The impact of the type of anaesthesia on cognitive status and delirium during the first postoperative days in elderly patients. Eur J Anaesthesiol. 2005;22(7):492–9.
Bruce AJ, Ritchie CW, Blizard R, Lai R, Raven P. The incidence of delirium associated with orthopedic surgery: a meta-analytic review. Int Psychogeriatr. 2007;19(2):197–214.
Cox G, Tzioupis C, Calori GM, Green J, Seligson D, Giannoudis PV. Cerebral fat emboli: a trigger of post-operative delirium. Injury. 2011;42(Suppl 4):S6-s10.
Scott JE, Mathias JL, Kneebone AC. Incidence of delirium following total joint replacement in older adults: a meta-analysis. Gen Hosp Psychiatry. 2015;37(3):223–9.
Chen W, Ke X, Wang X, Sun X, Wang J, Yang G, Xia H, Zhang L. Prevalence and risk factors for postoperative delirium in total joint arthroplasty patients: a prospective study. Gen Hosp Psychiatry. 2017;46:55–61.
Oh ES, Li M, Fafowora TM, Inouye SK, Chen CH, Rosman LM, Lyketsos CG, Sieber FE, Puhan MA. Preoperative risk factors for postoperative delirium following hip fracture repair: a systematic review. Int J Geriatr Psychiatry. 2015;30(9):900–10.
Wang LH, Xu DJ, Wei XJ, Chang HT, Xu GH. Electrolyte disorders and aging: risk factors for delirium in patients undergoing orthopedic surgeries. BMC Psychiatry. 2016;16(1):418.
de Jong L, van Rijckevorsel V, Raats JW, Klem T, Kuijper TM, Roukema GR. Delirium after hip hemiarthroplasty for proximal femoral fractures in elderly patients: risk factors and clinical outcomes. Clin Interv Aging. 2019;14:427–35.
Huang J, Sprung J, Weingarten TN. Delirium following total joint replacement surgery. Bosn J Basic Med Sci. 2019;19(1):81–5.
Yang Q, Wang J, Huang X, Xu Y, Zhang Y. Incidence and risk factors associated with postoperative delirium following primary elective total hip arthroplasty: a retrospective nationwide inpatient sample database study. BMC Psychiatry. 2020;20(1):343.
Yang Q, Wang J, Chen Y, Lian Q, Shi Z, Zhang Y. Incidence and risk factors of postoperative delirium following total knee arthroplasty: A retrospective Nationwide Inpatient Sample database study. Knee. 2022;35:61–70.
Yang Q, Fu J, Pan X, Shi D, Li K, Sun M, Ding J, Shi Z, Wang J. A retrospective analysis of the incidence of postoperative delirium and the importance of database selection for its definition. BMC Psychiatry. 2023;23(1):88.
Newman JM, Sodhi N, Dalton SE, Khlopas A, Newman RP, Higuera CA, Mont MA. Does Parkinson Disease Increase the Risk of Perioperative Complications After Total Hip Arthroplasty? A Nationwide Database Study. J Arthroplasty. 2018;33(7s):S162-s166.
Fineberg SJ, Nandyala SV, Marquez-Lara A, Oglesby M, Patel AA, Singh K. Incidence and risk factors for postoperative delirium after lumbar spine surgery. Spine. 2013;38(20):1790–6.
Bozic KJ, Bashyal RK, Anthony SG, Chiu V, Shulman B, Rubash HE. Is administratively coded comorbidity and complication data in total joint arthroplasty valid? Clin Orthop Relat Res. 2013;471(1):201–5.
Song SJ, Kim KI, Bae DK, Park CH. Mid-term lifetime survivals of octogenarians following primary and revision total knee arthroplasties were satisfactory: a retrospective single center study in contemporary period. Knee surgery & related research. 2020;32(1):50.
Meyer M, Schwarz T, Renkawitz T, Maderbacher G, Grifka J, Weber M. Hospital Frailty Risk Score predicts adverse events in revision total hip and knee arthroplasty. Int Orthop. 2021;45(11):2765–72.
Peng J, Wu G, Chen J, Chen H. Preoperative C-Reactive Protein/Albumin Ratio, a Risk Factor for Postoperative Delirium in Elderly Patients After Total Joint Arthroplasty. J Arthroplasty. 2019;34(11):2601–5.
Liufu N, Liu L, Shen S, Jiang Z, Dong Y, Wang Y, Culley D, Crosby G, Cao M, Shen Y, et al. Anesthesia and surgery induce age-dependent changes in behaviors and microbiota. Aging. 2020;12(2):1965–86.
Yang QF, Lin ZM, Yang S, Wang PK, Chen R, Wang J. Incidence and Risk Factors of In-Hospital Prosthesis-Related Complications Following Total Knee Arthroplasty: A Retrospective Nationwide Inpatient Sample Database Study. Orthop Surg. 2021;13(5):1579–86.
Moldovan F, Gligor A, Moldovan L, Bataga T. An investigation for future practice of elective hip and knee arthroplasties during COVID-19 in Romania. Medicina (Kaunas). 2023;59(2):314. https://doi.org/10.3390/medicina59020314.
Stachon P, Kaier K, Zirlik A, Reinöhl J, Heidt T, Bothe W, Hehn P, Zehender M, Bode C, von Zur MC. Risk factors and outcome of postoperative delirium after transcatheter aortic valve replacement. Clinical research in cardiology : official journal of the German Cardiac Society. 2018;107(9):756–62.
de Jonghe A, van Munster BC, van Oosten HE, Goslings JC, Kloen P, van Rees C, Wolvius R, van Velde R, Levi MM, Korevaar JC, de Rooij SE. The effects of melatonin versus placebo on delirium in hip fracture patients: study protocol of a randomised, placebo-controlled, double blind trial. BMC Geriatr. 2011;11:34.
Campbell AM, Axon DR, Martin JR, Slack MK, Mollon L, Lee JK. Melatonin for the prevention of postoperative delirium in older adults: a systematic review and meta-analysis. BMC Geriatr. 2019;19(1):272.
Kang SY, Seo SW, Kim JY. Comprehensive risk factor evaluation of postoperative delirium following major surgery: clinical data warehouse analysis. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology. 2019;40(4):793–800.
Weinstein SM, Poultsides L, Baaklini LR, Mörwald EE, Cozowicz C, Saleh JN, Arrington MB, Poeran J, Zubizarreta N, Memtsoudis SG. Postoperative delirium in total knee and hip arthroplasty patients: a study of perioperative modifiable risk factors. Br J Anaesth. 2018;120(5):999–1008.
Acknowledgements
Not applicable.
Funding
This study received no direct funding from any third-party donor or funding institution in the public, commercial, or non-profit sectors.
Author information
Authors and Affiliations
Contributions
ZP, JW (Wu) and ZW contributed to the study design, data acquisition and analysis, interpretation of results, and writing and revising the manuscript. HX and JW (Wang) contributed to the study design, interpretation of results, and reviewing the manuscript. PZ contributed to data acquisition, data analysis, and reviewing of the manuscript. QY and YL contributed to the study design, interpretation of results, and reviewing the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable. This article does not contain any studies with human participants or animals performed by any of the authors. Additionally, this observational study used identified publicly available data, hence there was no requirement for consent to participate and it was deemed exempt by the Internal Review Board (IRB) of Southern Medical University Nanfang Hospital. So, there is no need to grant permission in the Ethics approval and consent to participate section. All methods are carried out following relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Peng, Z., Wu, J., Wang, Z. et al. Incidence and related risk factors for postoperative delirium following revision total knee arthroplasty: a retrospective nationwide inpatient sample database study. BMC Musculoskelet Disord 25, 633 (2024). https://doi.org/10.1186/s12891-024-07757-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07757-8