
Abstract
Objective
The objective was to analyze the relationship between serum 25-hydroxy-vitamin D (25(OH)D) level and albuminuiria in middle-aged and older patients with type 2 diabetes of Gansu Province.
Methods
Data pertaining to 380 in-patients with type 2 diabetes were collected. Subjects were classified groups based on gender,age,25(OH)D,BMI and UACR.Serum 25(OH)D and other clinical characteristics among various UACR groups were compared.The relationship between albuminuiria and 25(OH)D was analyzed.
Results
Out of the 380 subjects, 83.4%were classified as vitamin D deficiency, 14.5%were classified as vitamin D insufficiency, while 2.1% were classified as vitamin D sufficiency. Among the participants,41% had albuminuria (microalbuminuria,28.7%;macroalbuminuria,12.3%).The prevalence of 25(OH)D deficiency in the albuminuria group(84.6%) was significantly higher than that in the normoalbuminuria group(82.6%)(Mann–Whitney U test:Z = -3.86,P = 0.000); patients with macroalbuminuria had the highest prevalence of 25(OH)D deficiency (91.5%; P < 0.01 versus normoalbuminuria).A binary logistic analysis demonstrated that 25(OH)D were protective factors for albuminuria.
Conclusions
The prevalence of vitamin D deficiency in patients with albuminuria was overtly higher than that in patients without albuminuria among middle-aged and older adults with type 2 diabetes.
Similar content being viewed by others


Introduction
The accelerated aging of the population has led to an increase in the number of older patients with type 2 diabetes mellitus (T2DM) [1]. Diabetic kidney disease (DKD) is one of the main consequences and a leading cause of death in people with type 2 diabetes, and its prevalence is rising globally as more middle-aged and older patients get the condition [2]. DKD has a significant impact on patients' quality of life and safety because it is the leading cause of disability and death in middle-aged and older people with type 2 diabetes [3]. Progressive albuminuria and a deterioration in renal function are the main clinical signs of DKD [4, 5]. DKD is characterized by podocyte destruction, interstitial fibrosis, and thickening of the glomerular basement membrane [6].The level of vitamin D in diabetic patients is lower than that in the normal population [7].Vitamin D deficiency may be involved in the occurrence and development of diabetic nephropathy [8,9,10]. A form of fat-soluble vitamin called serum vitamin D is crucial for maintaining bone health as it helps control the metabolism of calcium and phosphate [11]. In addition to causing problems with the way calcium and phosphorus are metabolized and with how bones are mineralized, a lack of vitamin D also hastens the onset of chronic renal disease [12].Numerous observational studies showed that patients with type 2 diabetes in Gansu Province, whether they had albuminuria or not, had vitamin D insufficiency or deficiency [13, 14]. Recent evidence from human and animal studies suggests that chronic kidney disease's traditional symptoms include low vitamin D levels and vitamin D resistance [15, 16]. Widespread use of serum 25-hydroxyvitamin D (25(OH)D) concentration as a diagnostic for vitamin D status [17]. Meanwhile,studies have confirmed that vitamin D deficiency is common in the adult population of Gansu Province [18].
Therefore, this study aims to evaluate the relationship between serum 25(OH)D and albuminuria in middle-aged and older patients with type 2 diabetes with or without albuminuiria of Gansu Province. Our findings may offer proof for the management and prevention of DKD in this area.
Objects and methods
Research objects
A total of 380 patients with type 2 diabetes (283 males and 97 females) who were hospitalized in the Department of Cadre Endocrinology of The People's Hospital of Gansu Province from October 2019 to December 2021. This cross-sectional research was carried out with an average age of (65.09 ± 8.20) years (55-92years).
(1) The following were the selection criteria: an endocrinologist determined the presence of type 2 diabetes mellitus based on the patient's medical history and high blood sugar levels. The following qualifications were required for exclusion:hepatorenal syndrome, hyperparathyroidism, malignant tumor, chronic digestive system disease, cancer, other special types of diabetes, acute complications of diabetes, inflammatory reaction, infection and recent surgery, estimated glomerular filtration rate (GFR) < 60mL/min,and vitamin D before hospitalization was excluded patients on complementary therapy. Our study protocol was approved by the ethics committee of hospital medicine. Written informed consent was obtained from each participant before data collection.
Research methods
General information
Collect general information of all patients, including name, age, gender, height, body mass index (BMI) = weight (kg)/height (m)2.
Laboratory measurements
Blood was drawn from the subjects fasting for 8–12 h,a random spot urine sample was collected. Fasting blood glucose (FBG), lipid profile, blood urea nitrogen (BUN), serum creatinine (Scr), calcium, phosphate, and HbA1c were among the laboratory markers. Using an automated analyzer called the Abbott C-1600, blood biochemical indicators were looked at.Using the glucose oxidase technique, FBG was found.Urinary albumin and creatinine concentrations were measured using a turbidimetric immunoassay with a Hitachi-7600 analyzer. Albuminuria was defined according to the creatinine,which was calculated by dividing the urinary albumin concentration (mg) by the urinary creatinine concentration (mg), which was urinary albumin-to-creatinine ratio (UACR).We determined serum 25(OH)D concentrations using using immunoassay chemiluminescence detection on Abbott ISR-2000 automatic analyzer.HbA1c was measured by ionic exchange high-performance liquid chromatography. Data support was provided by the Laboratory Department of The People's Hospital of Gansu Province.
Diagnostic categories
Categories was defined as follows.Based on the gender:283 males and 97 females.
Vitamin D status was divided into the following three categories based on serum 25(OH)D levels, as per the diagnostic criteria in the Application Guidelines for Vitamin D [19]: vitamin D sufficiency (> 30μg/L)(8); vitamin D insufficiency (> 20, ≤ 30μg/L)(55); and vitamin D deficiency(≤ 20μg/L)(317).Based on the levels of the level of urinary albumin-to-creatinine ratio (UACR),subjects were classified into three groups:UACR levels of 30 mg/g or less were classified as normoalbuminuria(224), whereas those of 30-300mg/g(≧30mg/g,and < 300mg/g)and above 300mg/g were classified as microalbuminuria(109) and macroalbuminuria(47), respectively. Based on their chronological ages, subjects were classified into three groups:young aged 55–64(204),middle-aged 65–74(120) and older over 75 years(56). Different UACR groups' serum 25(OH)D levels and other clinical traits were compared.Analysis was done on the connection between albuminuria and 25(OH)D.
Statistical analysis
The SPSS version 26.0 software utilized to carry out all statistical calculations. Continuous data with normal distribution are provided as mean standard deviation (SD), while continuous variables with non-normal distribution are shown as median interquartile range (IQR).The presentation of categorical variables is as frequency(percentage). For continuous variables with a non-normal distribution, between-group differences were evaluated using the Mann–Whitney U test.The correlation between the indicators was examined using Spearman correlation.Using binary logistic analysis, after taking into account potential confounding factors, the odds ratios (OR) and associated 95% confidence intervals (CI) for microalbuminuria and macroalbuminuria in connection to vitamin D status were determined. Two-sided P values of 0.05 or less were taken to indicate statistical significance across all analyses.
Results
General characteristics
Two hundred eighty-three (74.5%) of the 380 individuals were men, while 97 (25.5%) were women. Because more diabetic women were disqualified because of their propensity for urinary tract infections, which affect urine protein excretion, the percentage of females was lower. Out of the 380 subjects, the overall 25(OH)D level was 12.9 (9.9, 17.0)μg/L, patients had a considerably higher ratio of vitamin D deficiency and insufficiency(97.9%).
Among them, 317 (83.4%) were classified as vitamin D deficiency [25(OH)D ≤ 20 μg/L], 55 (14.5%) were classified as vitamin D insufficiency[25(OH)D > 20, ≤ 30 μg/L], while 8 (2.1%) were classified as vitamin D sufficiency [25(OH)D > 30 μg/L]. According to HbA1c levels, among the patients, 94 (24.7%) had HbA1c values below 7%, 213 (56.1%) had levels between 7 and 10%, and 73 (19.2%) had levels beyond 10%.
Clinical traits across different age groups compared:
The patients were divided into three groups according to age: young aged 55–64 years(204),middle-aged 65–74 years(120) and older over 75 years(56). Mann–Whitney U test results: there were significant differences in UACR between the middle-aged and the older aged group, p < 0.05.The test also showed that significant differences were observed between the young aged and the older aged group with respect to UACR and 25(OH)D, p < 0.05. (see Table 1).
Comparison of clinical characteristics among various UACR groups
Among the participants,156(41%) had albuminuria (microalbuminuria,28.7%;macroalbuminuria,12.3%). The prevalence of 25(OH)D deficiency in the albuminuria group(84.6%) was significantly higher than that in the normoalbuminuria group(82.6%)(Mann–Whitney U test:Z = -3.86,P = 0.000); the prevalence of 25(OH)D deficit was highest in patients with macroalbuminuria(91.5%; P < 0.01 versus normoalbuminuria). The Mann–Whitney U test showed that strong differences were found between the groups with macroalbuminuria and normoalbuminuria groups with respect to 25(OH)D,p < 0.001. Compared with the microalbuminuria and macroalbuminuria groups, the difference in 25(OH)D was statistically significant,p < 0.05. The differences in 25(OH)D between the microalbuminuria and the normoalbuminuria groups were statistically significant (p < 0.05). (see Table 2).
Correlation comparison
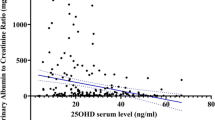
Spearman correlation analysis between 25(OH)D and albuminuiria in middle-aged and older diabetic patients
The studies that demonstrated a negative and substantial correlation between vitamin D and UACR(r = -0.233, p < 0.001), HbA1c(r = -0.223, p < 0.001).According to different age groups, in the young aged group(55-64years) and the middle-aged group(65-74years), 25(OH)D levels were negatively correlated with UACR(p < 0.05), and the middle-aged group was more significant (p < 0.001) (see Table 3).
Analysis of the risk factors for albuminuria in type 2 diabetes using binary logistic regression
With or without albuminuria as the dependent variable [without albuminuria (UACR < 30mg/g) = 0, with albuminuria(UACR≧30mg/g) = 1],and 25(OH)D as an independent variables(assigned value: measured value).The results showed that 25(OH)D was protective factor for albuminuria (See Table 4).
Discussion
We investigated the association of 25(OH)D with albuminuiria in the type 2 diabetes aged≧55y.In this observational study, we found that a low plasma 25(OH)D level was associated with a higher odds of having increased albuminuria.
The results of this study showed the middle-aged and older patients with type 2 diabetes who were treated in our hospital had obvious vitamin D deficiency, and the deficiency rate was 83.4%, which was similar to the proportion of vitamin D deficiency in the middle-aged and older people in Gansu (81.9%) previously reported [19]. These results showed that type 2 diabetes patients in China frequently have vitamin D deficiency or insufficiency. A large number of epidemiological studies at home and abroad [11] show that vitamin D shortage or insufficiency is relatively frequent throughout the world;with a deficiency rate of 39.6% to 57%, among which the older account for the majority [20]. It has been recently described in the literature that vitamin D has a strong protective role in chronic kidney disease [16, 17, 21]. One possible mechanism is that vitamin D protects against the development of DKD by inhibiting the activation of RAS by reducing renin expression [22,23,24]. In addition, 25(OH)D may act lowering oxidative stress by improving renal antioxidant capacity, preventing damage to podocytes by inhibiting hyperglycemia-induced apoptosis, promoting anti-inflammatory action, and improving endothelial function [15, 25, 26]. Kuhlmann et al. [27] found an animal study that vitamin D prevents podocyte damage, which lowers proteinuria and glomerulosclerosis. Meanwhile, another study showed that that lower 25(OH)D were linked to a higher prevalence of albuminuria in a sizable representative sample of adults with a variety of age, racial/ethnic, and diabetes status [28] (population). The conclusion agreed with what we found in the study. Regardless of the processes behind the link between a lack of vitamin D and albuminuria,numerous evidences point to vitamin D's major role in the prevalence of albuminuria and the existence of diabetic nephropathy [29].
In addition, we found that the serum 25(OH)D level of T2DM patients with albuminuiria was significantly lower than that of patients without albuminuiria. This study also showed that patients with micro or macro albuminuria had a higher prevalence of vitamin D insufficiency or deficiency compared to those with normoalbuminuria,and the difference between the groups was statistically significant.Our results agree with Ucak et al. [30], who discovered a link between individuals with low 25(OH)D levels and a higher incidence of microalbuminuria.
Further,elevated UACR level was associated with decreased 25(OH)D. Our study was also confirmed that vitamin D deficiency was more serious in older patients with type 2 diabetic nephropathy. The results confirmed that the level of 25(OH)D in patients aged 65–74 was more significantly correlated with UACR. Partial correlation (spearman) analysis showed that UACR level was significantly negatively correlated with 25(OH)D.In accordance with the our current study, binary logistic regression analysis found that 25(OH)D level was correlated with albuminuria.
Our investigation has the advantage of include a large sample of patients while eliminating those who had clearly compromised renal function (high serum creatinine levels), which would have interfered with 25(OH)D metabolism.Some limitations of our study should be acknowledged.Firstly,the lack of a control group of the same age and the influence of oral hypoglycemic drugs on bone metabolism are not excluded. Secondly, given that this was a cross-sectional study, the design makes it difficult to understand the causal relationship between serum vitamin D and proteinuria, which is a limitation of this research.The low vit D can give rise to albuminuria as easily as albuminuria can give low vitamin D,in compliance with albuminuria can give rise to low vitamin D carrier protein (alpha globulin) [ the protein is lost in the urine] hat in turn lowers totalvit D levels [31]. Finally, the impact of unmeasured confounders, such as exposure to direct sunlight, nutritional status, and smoking status, could not completely be ruled out even after we had controlled for several potential confounding factors.Therefore, more research and prospective cohort studies are needed to determine the exact cause of the link between vitamin D and protainuria.
In conclusion, we found that the low plasma 25(OH)D level was associated with a higher odds of having increased albuminuria.Vitamin D deficiency has become a global public health problem, especially for middle-aged and older patients, which is an important issue related to the future of mankind.
Therefore, vitamin D level monitoring should be carried out in patients with type 2 diabetes with or without albuminuiria, which not only helps to identify high-risk groups of diabetic nephropathy, but also provides a reference for judging the severity of diabetic nephropathy. In addition to establishing a 25(OH)D reference range specifically for middle-aged and older Chinese patients, more studies with adequate serum vitamin D are required, including randomized clinical trials, for a more forceful clinical practice among this population. Supplement the clinical value of vitamin D in preventing the occurrence of diabetes and preventing the progression of diabetic nephropathy is still worthy of further exploration.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
References
International Diabetes Federation, 2019. IDF Diabetes Atlas Brussels, Belgium ninth ed. www.diabetesatlas.org/. Accessed 11 Jun 2020.
Tuttle KR, Bakris GL, Bilous RW, et al. Diabetic kidney disease: a report from an ADA consensus conference. Diabetes Care. 2014;37:2864e2883.
Khatib ST, Hemadneh MK, Hasan SA, Khazneh E, Zyoud SH. Quality of life in hemodialysis diabetic patients:a multicenter cross-sectional study from Palestine. BMC Nephrol. 2018;19(1):49–49.
National Kidney Foundation. KDOQI Clinical Practice Guideline for Diabetes and CKD:2012 Update. Am J Kidney Dis. 2012;60(5):850–86. https://doi.org/10.1053/j.ajkd.2012.07.005.
Bonner R, Albajrami O, Hudspeth J, Upadhyay A. Diabetic Kidney Disease. Prim Care. 2020;47(4):645–59. https://doi.org/10.1016/j.pop.2020.08.004. (Epub 2020 Sep 23).
Lin YC, Chang YH, Yang SY, Wu KD, Chu TS. Update of pathophysiology and management of diabetic kidney disease. J Formos Med Assoc. 2018;117(8):662–75. https://doi.org/10.1016/j.jfma.2018.02.007. (Epub 2018 Mar 2).
JS Felıcio, Luz RM, de Melo FTC, de Souza Resende F, de Oliveira AF, Peixoto ́ AS, et al. Vitamin D on Early Stages of Diabetic Kidney Disease: A CrossSectional Study in Patients With Type 1 Diabetes Mellitus. Front Endocrinol. 2016;7:149.
De Boer IH, Sachs MC, Cleary PA, Hoofnagle AN, Lachin JM, Molitch ME, et al. Circulating Vitamin D Metabolites and Kidney Disease in Type 1Diabetes. J Clin Endocrinol Metab. 2012;97:4780–8.
S-h H, Kim YB, Choi HS, Jeong T-D, Kim JT, Sung YA. Association of vitamin D deficiency with diabetic nephropathy. Endocrinol Metab. 2021;36(1):106–13.
Senyigit A. The association between 25-hydroxy vitamin D deficiency and diabetic complications in patients with type 2 diabetes mellitus. Diabetes Metab Syndr. 2019;13(2):1381–6.
Holick MF. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev Endocr Metab Disord. 2017;18(2):153–65. https://doi.org/10.1007/s11154-017-9424-1.
Franca Gois P, Wolley M, Ranganathan D, Seguro A. Vitamin D Deficiency in Chronic Kidney Disease: Recent Evidence and Controversies. Int J Environ Res Public Health. 2018;15:1773.
Engelen L, Schalkwijk CG, Eussen SJPM, Scheijen JLJM, Soedamah-Muthu SS, Chaturvedi N, et al. Low 25-Hydroxyvitamin D2 and 25-Hydroxyvitamin D3 Levels Are Independently Associated With Macroalbuminuria, But NotWith Retinopathy and Macrovascular Disease in Type 1 Diabetes: The EURODIAB Prospective Complications Study. Cardiovasc Diabetol. 2015;14:67.
Felício JS, de Rider Britto HA, Cortez PC, et al. Association Between 25(OH)Vitamin D, HbA1c and Albuminuria in Diabetes Mellitus: Data From a Population-Based Study (VIDAMAZON). Front Endocrinol (Lausanne). 2021;12:723502.
Deng X, Cheng J, Shen M. Vitamin D Improves Diabetic Nephropathy in Rats by Inhibiting Renin and Relieving Oxidative Stress. J Endocrinol Investig. 2016;39:657–66.
Nakhoul N, Thawko T, Farber E, et al. The therapeutic effect of active vitamin D supplementation in preventing the progression of diabetic nephropathy in a diabetic mouse model. J Diab Res. 2020;2020:10 (Article ID 7907605).
Grant WB, Boucher BJ, Bhattoa HP, Lahore H. Why vitamin D clinical trials should be based on 25-hydroxyvitamin D concentrations. J Steroid Biochem Mol Biol. 2018;177:266–9.
Wenjuan Ma, Jing L, Lianhua W, et al. Serum vitamin D levels and related factors in healthy adults in Gansu Province [J]. Chin J Clin Nutr. 2017;25(4):6.
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, Murad MH, Weaver CM. Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911–30.
Mendes MM, Charlton K, Thakur S, et al. Future perspectives in addressing the global issue of vitamin D deficiency. Proc Nutr Soc. 2020;79:246–51.
Hong S, Kim YB, Choi HS, Jeong T-D, Kim JT, Sung YA. Association ofVitamin D Deficiency With Diabetic Nephropathy. Endocrinol Metab. 2021;36:106–13.
Tiryaki Ö, Usalan C, Sayiner ZA. Vitamin D Receptor Activation With Calcitriol for Reducing Urinary Angiotensinogen in Patients With Type 2Diabetic Chronic Kidney Disease. Ren Fail. 2016;38:222–7.
Li YC, Qiao G, Uskokovic M, Xiang W, Zheng W, Kong J. Vitamin D: ANegative Endocrine Regulator of the Renin-Angiotensin System and Blood Pressure. J Steroid Biochem Mol Biol. 2004;89–90:387–92.
Forman JP, Williams JS, Fisher NDL. Plasma 25-hydroxyvitamin D and regulation of the renin angiotensin system in humans. Hypertension. 2010;55(5):1283–8.
Li YC. Podocytes as Target of Vitamin D. Curr Diabetes Rev. 2010;7:35–40.
Doorenbos CRC, van den Born J, Navis G, de Borst MH. Possible Renoprotection by Vitamin D in Chronic Renal Disease: Beyond Mineral Metabolism. Nat Rev Nephrol. 2009;5:691–700.
Kuhlmann A, Haas CS, Gross M-L, et al. 1, 25-Dihydroxyvitamin D3 decreases podocyte loss and podocyte hypertrophy in the subtotally nephrectomized rat. Am J Physiol Renal Physiology. 2004;286(3):F526–33.
De Boer IH, Ioannou GN, Kestenbaum B, Brunzell JD, Weiss NS. 25-Hydroxyvitamin D levels and albuminuria in the Third National Health and Nutrition Examination Survey (NHANESIII). Am J Kidney Dis. 2007;50(1):69–77.
Felıcio JS, de Oliveira AF, Peixoto AS, de Souza ACCB, Abrahão Neto JF, de ́Melo FTC, et al. Albuminuria Reduction After High Dose of Vitamin D in Patients With Type 1 Diabetes Mellitus: A Pilot Study. Front Endocrinol. 2017;8:199.
Ucak S, Sevim E, Ersoy D, Sivritepe R, Basat O, Atay S. Evaluation of the Relationship Between Microalbuminuria and 25-(OH) Vitamin D Levels in Patients With Type 2 Diabetes Mellitus. Aging Male. 2019;22:116–20.
Speeckaert M, Huang G, Delanghe JR, Taes YE. Biological and clinical aspects of the vitamin D binding protein (Gc-globulin) and its polymorphism. Clin Chim Acta. 2006;372(1–2):33–42.
Acknowledgements
Not applicable.
Funding
This study was supported in part by grants from Gansu Provincial Youth Science and Technology Fund Program;Number: 21JR1RA008;this study also was supported by grants fromGansu Provincial People's Hospital In-hospital Fund Program;Number: 18GSSY1-4.
Author information
Authors and Affiliations
Contributions
Luyan Zhang: Conceptualization, Methodology, Software, Data curation, Writing-Original draft preparation. Qian Guo: Supervision. Yanjia Xu: Investigation. Wenzhen Wei: Investigation. Yu Wang: Investigation.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The experimental protocol was established, according to the ethical guidelines of the Helsinki Declaration and was approved by the Human Ethics Committee of the People's Hospital of Gansu Province.Written informed consent was obtained from each participant before data collection.Due to the impact of the epidemic, the upload of the original file was delayed.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, L., Guo, Q., Xu, Y. et al. Association between serum 25- hydroxyvitamin D and albuminuiria in middle-aged and older Chinese patients with type 2 diabetes. BMC Endocr Disord 23, 189 (2023). https://doi.org/10.1186/s12902-023-01440-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-023-01440-0