
Abstract
Backgroud
The relationship between serum uric acid (SUA) and 25-hydroxyvitamin D (25(OH)D) has been variably characterized in existing literature, with inconsistent results regarding its nature and implications in the Chinese population. This study aims to clarify this association, considering the potential impact of vitamin D levels on SUA.
Methods
This cross-sectional study involved 7,086 individuals from the Second Affiliated Hospital of Zhejiang University School of Medicine, screened throughout 2020. We collected data on 25(OH)D, SUA, and other metabolic markers. Logistic regression models adjusted for confounding factors were utilized to analyze the relationships.
Results
Our findings illustrate a statistically significant inverted U-shaped relationship between 25(OH)D and SUA. The identified threshold effect at 28.82 ng/ml is pivotal; with 25(OH)D levels below this point associated with an increased risk of hyperuricemia (odds ratio: 1.0146, p = 0.0148), and levels above it offering protective benefits (odds ratio: 0.9616, p = 0.0164).
Conclusions
Our findings confirm a nonlinear, inverted U-shaped correlation between 25(OH)D and SUA, emphasizing the importance of maintaining vitamin D levels within a specific range to effectively manage hyperuricemia. These results support the implementation of personalized vitamin D supplementation strategies to optimize metabolic health outcomes, highlighting the complex interplay between vitamin D status and uric acid levels.
Similar content being viewed by others


Introduction
Hyperuricemia has become a major public health problem in China. A Meta-analysis showed that the prevalence of hyperuricemia in Chinese adults was estimated to be 13.3% [1]. Elevated levels of serum uric acid (SUA) can lead to gout and are associated with increased risk of various metabolic disorders, including hypertension, diabetes, chronic kidney disease, and cardiovascular and cerebrovascular diseases [2]. Contrarily, some studies suggest that high SUA levels may protect against osteoporosis, indicating complex roles in human health [3, 4].
Vitamin D, a fat-soluble vitamin essential for calcium and phosphorus metabolism, is produced through skin exposure to sunlight and can also be ingested from dietary sources [5]. Insufficient levels of vitamin D are linked to numerous skeletal and chronic diseases, suggesting a multifaceted role in overall health maintenance [6,7,8,9]. Recent genome-wide association studies (GWAS) have indicated potential shared pathways between vitamin D metabolism and SUA regulation [10], yet the exact nature of their relationship remains poorly understood.
Therefore, interactions between vitamin D deficiency and hyperuricemia could have significant public health implications. Serum 25-Hydroxyvitamin D (25(OH)D) is considered the most stable and reliable indicator of vitamin D status [11]. Although several studies have suggested a mutual association between 25(OH)D levels and hyperuricemia, this relationship remains poorly defined and controversial [11,12,13]. A systematic review and meta-analysis have further supported the significant association between 25(OH)D levels and SUA, highlighting the need for detailed investigation into their interaction [14]. The nature of the correlation—whether simple and linear or more complex—deserves thorough investigation given the potential shared metabolic pathways between vitamin D and SUA.
To date, few studies have explored the relationship between serum uric acid (SUA) and vitamin D within the Chinese population. Our study aims to bridge this gap by employing logistic regression analysis in various models to examine and clarify the specifics of this association.
Materials and methods
Study population
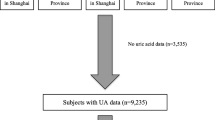
In this study, 88618 residents undergone physical examinations at the Health Management Center of Second Affiliated Hospital of Zhejiang University School of Medicine, whom were enrolled from January to December, 2020. All subjects are ≥ 18 years old. Of 88,618 subjects, 7482 had UA and vitamin D data. We excluded those who lacked history of person and present illness (n = 260), and had gouty arthritis (n = 50), chronic kidney disease (n = 14), pregnancy (n = 4) as well as anti-osteoporosis drug usage (n = 68). Ultimately, 7086 subjects were recruited in this study. The flow chart of the screening process was shown in Fig. 1. All participants provided informed consent. The study was approved by the ethics committee of local hospital.

Flowchart of this study. We totally collected 88,618 subjects. After excluding participants who without missing data or with specific states, ultimately, 7086 subjects were included
Data collection
All subjects were recorded in details for age, gender, and body mass index (BMI). Afterwards, serum was extracted and further used for biochemical analysis.
Laboratory measurements
Biochemical parameters, including SUA, total cholesterol (TC), triglycerides (TG), fasting plasma glucose (FPG), low-density lipoprotein (LDL), high-density lipoprotein (HDL), alanine transaminase (ALT), aspertate aminotransferase (AST) were determined via automated chemistry analyzer (Beckman/Power Processer Automation). Glycated hemoglobin A1c (HbA1c) was measured using high-performance liquid chromatography (HLC-732G8). Hyperuricemia was defined by SUA > 420µmol/L in adult men and > 360µmol/L in adult women [15]. Serum 25(OH)D measurement was performed using LC-MS/MS (Waters Xevo TQD). Vitamin D deficiency was defined as a 25(OH)D < 20ng/mL, insufficiency as 21-29ng/mL and sufficiency as at least 30ng/mL [16]. All methods were performed in accordance with the relevant guidelines and regulations.
Statistical analysis
Statistical analysis was conducted via Empower-Stats (www.empowerstats.com, X&Y Solutions, Inc., Boston, MA) and the statistical software package R (http://www.R-project.org, The R Foundation). Continuous variables that followed a normal distribution were expressed as the mean ± standard deviation (SD), and those that were not normally distributed were expressed as the median (quartile 1-quartile 3). Categorical variables were expressed as the frequency (percentage). The one-way ANOVA and chi-square test were employed as appropriate to evaluate the difference between hyperuricemia and non-hyperuricemia individuals. Results were considered statistically significant at a two-tailed P value of < 0.05.
The independent risk factors for hyperuricemia were determined via establishing univariate and multivariate logistics models. We selected these confounders on the basis of their associations with the HUA or a change in effect estimate of more than 10% [17]. A correlation matrix was used to assess the collinearity of all explanatory variables. Collinearity between variables was tested using the variance inflation factor (VIF) based on a multiple regression model [18]. The variables with VIF > 5 were considered to exhibit collinearity. Three different models were built: Model 1, with no adjustment for covariates; Model 2, adjusted for gender, age, drinking and smoking; and Model 3, adjusted for gender, age, drinking, smoking, HBP, BMI, AST, GLU, CR, TG, LDL, HbA1c and insulin.
To explore the nonlinear association between 25(OH)D and HUA, 25(OH)D of continuous independent variable was transformed into categorical variable based on tertiles. Moreover, we used a generalized additive model(GAM) to identify the nonlinear relationship between 25(OH)D and HUA. If the nonlinear relationship was found, the piece-wise linear regression model compute the threshold effect of 25(OH)D and HUA by the smoothing plot. Furthermore, the subgroup analysis were conducted and stratified via age, hypertension, sex, drinking, smoking, BMI, AST, Glu, CR, TG, LDL, HbA1C, and insulin.
Results
Baseline characteristics of subjects
In the survey, baseline characteristics of 7086 subjects between hyperuricemia and non-hyperuricemia were shown in Table 1. Among 7086 subjects, 5558 individuals had normal SUA, the remaining 1528 with hyperuricemia. Levels of SUA between hyperuricemia and normal group were 462.19 ± 56.18 nmol/L and 310.84 ± 62.72 nmol/L, respectively. The proportion of hyperuricemia was 21.56%. Of 5558 with normal SUA, 2961 was male, and 2597 was female (aged 46.24 ± 12.06 years). Of 1528 with hyperuricemia, 1260 was male, and 268 was female (aged 45.64 ± 12.94 years). Lipids (LDL, TC, TG), FPG, HbA1c, TBIL, ALT, AST, Cr, insulin and BMI in hyperuricemia group were significantly higher than the Non-hyperuricemia. Meanwhile, the hyperuricemia group had a significantly lower HDL than the Non-hyperuricemia. There was also a significantly difference in 25(OH)D in these two groups(19.15 ± 7.59 vs. 19.87 ± 7.02, P < 0.001) (Table 1).
Univariate analysis for hyperuricemia
The univariable logsitic regression for association between 25(OH)D and HUA was presented in Table 2. The 25(OH)D was risk factors for HUA. Moreover, the hypertension, male, smoking, drinking, BMI, TBIL, ALT, AST, GLU, CR, TC, TG, LDL, HbA1c, insulin, 25(OH)D can contribute to HUA as well. In contrast, the HDL were protective factors for HUA (Table 2).
Logistic regression analysis of HUA in different models
Model 1 was a crude model. This model showed that 25(OH)D was negatively related to the incidence of HUA. However, in Model 2, OR = 1.0046 95%CI: 0.9963–1.0129, P = 0.280 and in Model 3, OR = 1.004,95%CI: 0.995–1.013, P = 0.432. Thus, 25(OH)D and HUA may not be a simple linear correlation, and of which 25(OH)D should be further divided into trisection. In crude model, compared with the lowest concentration of 25(OH)D (T1), T2, T3 was associated with increased level of HUA(T2: OR = 1.389, 95%CI% :1.205- 1.600, T3: OR 1.382, 95%CI: 1.199–1.59), P for trend < 0.05 (Table 3). However, in Model 2 and Model 3, P for trend > 0.05, indicating the association between 25(OH)D and HUA were nonlinear.
Non- linear association between 25(OH)D and HUA
The GAM model with smoothing curve showed that the 25(OH)D and HUA were non- linear after multivariable adjustment (Fig. 2). According to the piece-wise linear regression analysis, there were threshold effects between 25(OH)D and HUA (Table 4), and we calculated that the turning points were 28.82ng/mL in 25(OH)D concentrations. On the left of turning points (25(OH)D < 28.82ng/mL), we observed a significantly positive association between 25(OH)D and HUA, with OR of 1.0146 (95 CI%: 1.0028, 1.0264, P < 0.05). Interestingly, we observed a significantly negative association between 25(OH)D and HUA, with OR of 0.9616 (95 CI%: 0.9313, 0.9929, P < 0.05) above the turning point (25(OH)D ≥ 28.82ng/mL).

The GAM model with smoothing curve showed that the 25(OH)D and HUA were non- linear after multivariable adjustment
Subgroup analysis
Table 5 showed the association between 25(OH)D and HUA in different subgroups. The results showed that there were no significant interaction effects of age, sex, HBP, drinking, smoking, BMI, AST, GLU, Cr, TG, LDL, HbA1c, insulin.
Discussion
We performed a cross-sectional study in the Chinese general population. In this study, the metabolism-related factors were significantly different between HUA and normal group, including 25(OH)D, LDL, TC, TG, FPG, HbA1c, TBIL, ALT, AST, Cr, insulin and BMI being significantly higher in hyperuricemia group. These findings were understandable. Furthermore, we found that BMI, ALT, TG and LDL may increase the risk of HUA, which were in consistent with some previous studies [19,20,21]. There are several limitations for the current study. Firstly, the study cohort only consisted of adults living in Zhejiang province. Therefore, the finding might not be representative of the whole Chinese population. Due to the cross-sectional study, the definitely causal relationship between 25(OH)D and uric acid could not be established. Notably, we did not account for important lifestyle factors such as diet, exercise, sunlight exposure, and vitamin D supplement use, which can significantly influence both vitamin D status and uric acid levels. These factors should be considered in future research to provide a more comprehensive understanding of the observed associations.
The previous studies found that Vitamin D has positive association with SUA [3, 11, 13]. However, some other studies demonstrated that Vitamin D deficiency might increase the risk of hyperuricemia [12, 22]. Han et al. showed that 25(OH)D have a negative association with SUA and hyperuricemia [23]. Therefore, there was a paradoxical relationship between 25(OH)D and SUA. Unexpectedly, an inverted U-shaped relationship between 25(OH)D and HUA was observed in our current study. We found that the level of 25(OH)D was negatively associated with hyperuricemia above the turning point (25(OH)D ≥ 28.82ng/mL), while significantly positive association when 25(OH)D < 28.82ng/mL. When we added multiple potential confounding factors, including age, hypertension, sex, drinking, smoking, BMI, AST, Glu, Cr, TG, LDL, HbA1C, insulin, the results were consistent in both crude and fully adjusted models. The sensitivity and stratification analysis of the association between 25(OH)D and HUA was relatively stable and revealed similar results across all subgroups without any indication of interaction.
Our findings identify a critical cutoff value for 25(OH)D at 28.82 ng/mL, below which the risk of hyperuricemia increases significantly. This threshold offers a practical target for clinicians to manage vitamin D levels more effectively. Considering the general recommendation for maintaining serum 25(OH)D concentrations above 30 ng/mL for optimal bone health in older adults, our study extends these guidelines by highlighting the potential metabolic risks associated with lower vitamin D levels. Given the controversial nature of vitamin D supplementation’s extra-skeletal benefits, as discussed in recent comprehensive reviews [24], our study suggests that maintaining serum 25(OH)D levels above our identified cutoff could not only support skeletal health but also mitigate hyperuricemia risk. This dual benefit reinforces the need for targeted vitamin D supplementation strategies, particularly in populations at risk for both bone diseases and elevated serum uric acid levels.
The exact mechanisms underlying the bidirectional relationship remain to be fully elucidated. however, they likely involve a complex interplay of renal function, hormonal balance, inflammation, oxidative stress, and genetic factors. First, Vitamin D plays a critical role in both renal function and inflammation, significantly impacting serum uric acid levels [14]. Optimal levels of 25(OH)D enhance renal function, facilitating efficient uric acid clearance and underscoring the importance of maintaining vitamin D within a specific range for optimal renal health. Concurrently, vitamin D’s anti-inflammatory properties regulate immune responses that can influence uric acid production. By maintaining proper vitamin D levels, inflammation is reduced, which can subsequently decrease uric acid synthesis [12]. Moreover, vitamin D influences hormonal pathways, including those involving parathyroid hormone and estrogen, which affect uric acid metabolism. Fluctuations in vitamin D levels can lead to hormonal imbalances, impacting uric acid concentrations [25]. And lastly, Vitamin D’s role in calcium and phosphorus homeostasis may affect uric acid levels through renal mechanisms. Additionally, genetic factors like variations in SLC2A9 and SLC17A3, which are involved in uric acid transport, could explain the variability in serum uric acid levels among individuals with different vitamin D statuses [26, 27]. These insights highlight the need for further research to elucidate how genetic predispositions and renal function interact with vitamin D to influence uric acid metabolism, potentially guiding more tailored interventions for managing related metabolic disorders.
To improve our interpretation of findings and produce more robust results, stratification of the association between 25(OH)D and HUA revealed similar finding among all subgroups. The previous study speculated that SUA have a beneficial effect on bone metabolism as an antioxidant in 7502 healthy postmenopausal women [28]. Moreover, we detected that there was a significant correlation between SUA and 25(OH)D, which clued the higher level of UA could help to prevent from the osteoporosis. Nabipour et al. also found that higher UA levels were associated with higher BMD at all skeletal sites and with a lower prevalence of vertebral and nonvertebral fractures in older men [3]. SUA reduction is a major risk factor for vitamin D deficiency in pregnant women. Estradiol (E2) may affect SUA through mechanisms involving renal clearance, secretion and reabsorption [29]. Recently, our findings are in line with recent research which also identified an inverted U-shaped relationship between serum vitamin D and serum uric acid levels in a pediatric cohort, further supporting the universality of this pattern across different age groups [30]. These findings further supported the current study.
In conclusion, our study demonstrated a nonlinear association between 25(OH)D and SUA. revealing that vitamin D levels influence uric acid metabolism in a concentration-dependent manner. Specifically, we found that the risk of hyperuricemia decreases when 25(OH)D levels are above the critical threshold of 28.82 ng/mL, while below this level, the risk increases significantly. This finding underscores the complexity of the relationship between vitamin D status and uric acid metabolism, and provides a clear guide for clinicians on how to adjust vitamin D therapy to optimize uric acid control.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.
References
Liu R, Han C, Wu D, Xia X, Gu J, Guan H, Shan Z, Teng W. Prevalence of hyperuricemia and gout in Mainland China from 2000 to 2014: a systematic review and meta-analysis. BioMed Res Int. 2015;2015:762820.
Bardin T, Richette P. Impact of comorbidities on gout and hyperuricaemia: an update on prevalence and treatment options. BMC Med. 2017;15(1):123.
Nabipour I, Sambrook PN, Blyth FM, Janu MR, Waite LM, Naganathan V, Handelsman DJ, Le Couteur DG, Cumming RG, Seibel MJ. Serum uric acid is associated with bone health in older men: a cross-sectional population-based study. J Bone Min Res. 2011;26(5):955–64.
Zhao DD, Jiao PL, Yu JJ, Wang XJ, Zhao L, Xuan Y, Sun LH, Tao B, Wang WQ, Ning G, et al. Higher serum uric acid is associated with higher bone mineral density in Chinese men with type 2 diabetes mellitus. Int J Endocrinol. 2016;2016:2528956.
Bikle DD. Vitamin D metabolism and function in the skin. Mol Cell Endocrinol. 2011;347(1–2):80–9.
Sahota O. Osteoporosis and the role of vitamin D and calcium-vitamin D deficiency, vitamin D insufficiency and vitamin D sufficiency. Age Ageing. 2000;29(4):301–4.
Wharton B, Bishop N. Rickets. Lancet. 2003;362(9393):1389–400.
Mitri J, Pittas AG. Vitamin D and diabetes. Endocrinol Metab Clin North Am. 2014;43(1):205–32.
Wang TJ. Vitamin D and cardiovascular disease. Annu Rev Med. 2016;67:261–72.
Thakkinstian A, Anothaisintawee T, Chailurkit L, Ratanachaiwong W, Yamwong S, Sritara P, Ongphiphadhanakul B. Potential causal associations between vitamin D and uric acid: bidirectional mediation analysis. Sci Rep. 2015;5:14528.
Chen Y, Cheng J, Chen Y, Wang N, Xia F, Chen C, Han B, Lu Y. Association between serum vitamin D and uric acid in the eastern Chinese population: a population-based cross-sectional study. BMC Endocr Disord. 2020;20(1):79.
Peng H, Li H, Li C, Chao X, Zhang Q, Zhang Y. Association between vitamin D insufficiency and elevated serum uric acid among middle-aged and elderly Chinese Han women. PLoS One. 2013;8(4):e61159.
Sipahi S, Acikgoz SB, Genc AB, Yildirim M, Solak Y, Tamer A. The association of vitamin D Status and Vitamin D Replacement Therapy with Glycemic Control, serum uric acid levels, and Microalbuminuria in patients with type 2 diabetes and chronic kidney disease. Med Princ Pract. 2017;26(2):146–51.
Isnuwardana R, Bijukchhe S, Thadanipon K, Ingsathit A, Thakkinstian A. Association between vitamin D and uric acid in adults: a systematic review and Meta-analysis. Horm Metab Res. 2020;52(10):732–41.
Multidisciplinary Expert Task Force on H, Related D. Chinese multidisciplinary expert consensus on the diagnosis and treatment of hyperuricemia and related diseases. Chin Med J (Engl). 2017;130(20):2473–88.
Alshahawey M, El Borolossy R, El Wakeel L, Elsaid T, Sabri NA. The impact of cholecalciferol on markers of vascular calcification in hemodialysis patients: a randomized placebo controlled study. Nutr Metab Cardiovasc Dis. 2021;31(2):626–33.
Jaddoe VW, de Jonge LL, Hofman A, Franco OH, Steegers EA, Gaillard R. First trimester fetal growth restriction and cardiovascular risk factors in school age children: population based cohort study. BMJ. 2014;348:g14.
Wax Y. Collinearity diagnosis for a relative risk regression analysis: an application to assessment of diet-cancer relationship in epidemiological studies. Stat Med. 1992;11(10):1273–87.
Chen SC, Huang YF, Wang JD. Hyperferritinemia and hyperuricemia may be associated with liver function abnormality in obese adolescents. PLoS One. 2012;7(10):e48645.
Li Q, Li R, Zhang S, Zhang Y, Liu M, Song Y, Liu C, Liu L, Wang X, Wang B, et al. Relation of BMI and waist circumference with the risk of new-onset hyperuricemia in hypertensive patients. QJM. 2022;115(5):271–8.
Peng TC, Wang CC, Kao TW, Chan JY, Yang YH, Chang YW, Chen WL. Relationship between hyperuricemia and lipid profiles in US adults. Biomed Res Int. 2015;2015:127596.
Takahashi S, Yamamoto T, Moriwaki Y, Tsutsumi Z, Yamakita J, Higashino K. Decreased serum concentrations of 1,25(OH)2-vitamin D3 in patients with gout. Metabolism. 1998;47(3):336–8.
Han Y, Han K, Zhang Y, Zeng X. Serum 25-hydroxyvitamin D might be negatively associated with hyperuricemia in U.S. adults: an analysis of the National Health and Nutrition Examination Survey 2007–2014. J Endocrinol Invest. 2022;45(4):719–29.
Bouillon R, Manousaki D, Rosen C, Trajanoska K, Rivadeneira F, Richards JB. The health effects of vitamin D supplementation: evidence from human studies. Nat Rev Endocrinol. 2022;18(2):96–110.
Johnson RJ, Kang DH, Feig D, Kivlighn S, Kanellis J, Watanabe S, Tuttle KR, Rodriguez-Iturbe B, Herrera-Acosta J, Mazzali M. Is there a pathogenetic role for uric acid in hypertension and cardiovascular and renal disease? Hypertension. 2003;41(6):1183–90.
Polasek O, Jeroncic I, Mulic R, Klismanic Z, Pehlic M, Zemunik T, Kolcic I. Common variants in SLC17A3 gene affect intra-personal variation in serum uric acid levels in longitudinal time series. Croat Med J. 2010;51(1):32–9.
Tu HP, Chung CM, Min-Shan Ko A, Lee SS, Lai HM, Lee CH, Huang CM, Liu CS, Ko YC. Additive composite ABCG2, SLC2A9 and SLC22A12 scores of high-risk alleles with alcohol use modulate gout risk. J Hum Genet. 2016;61(9):803–10.
Ahn SH, Lee SH, Kim BJ, Lim KH, Bae SJ, Kim EH, Kim HK, Choe JW, Koh JM, Kim GS. Higher serum uric acid is associated with higher bone mass, lower bone turnover, and lower prevalence of vertebral fracture in healthy postmenopausal women. Osteoporos Int. 2013;24(12):2961–70.
Yahyaoui R, Esteva I, Haro-Mora JJ, Almaraz MC, Morcillo S, Rojo-Martinez G, Martinez J, Gomez-Zumaquero JM, Gonzalez I, Hernando V, Soriguer F. Effect of long-term administration of cross-sex hormone therapy on serum and urinary uric acid in transsexual persons. J Clin Endocrinol Metab. 2008;93(6):2230–3.
Ma Z, Xiong T, Li Y, Kong B, Lu W, Zhang Z, Chen L, Tang Y, Yao P, Xiong J, et al. The inverted U-Shaped association between serum vitamin D and serum uric acid status in children and adolescents: a large cross-sectional and longitudinal analysis. Nutrients. 2024;16(10):1492.
Acknowledgements
We would like to thank participants.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
S.L and T.S conceived the study. S.L and F.N conducted the statistical analyses. S.L, Y.W, F.N, and T.S collected and interpreted the clinical data. S.L, Y.W drafted the manuscript. All authors contributed to the interpretation of the results and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The studies involving human participants were reviewed and approved by the ethics committee of The Second Affiliated Hospital of Zhejiang University School of Medicine (approval number: 2022-0043). All participants provided informed consent.
Consent for publication
Written informed consent for publication was obtained.
Competing interests
The authors declare no competing interests
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, ST., Wang, YL., Ni, FH. et al. Association between 25 hydroxyvitamin D and serum uric acid level in the Chinese general population: a cross-sectional study. BMC Endocr Disord 24, 187 (2024). https://doi.org/10.1186/s12902-024-01723-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-024-01723-0