
Abstract
Background
Dental caries (DC) is highly prevalent condition affecting mostly young children. There has been no systematic review done on the prevalence of DC amongst 12-year -olds in Africa. Although some African countries have reported a decrease in DC prevalence, others have shown an increase and it is essential to measure current trends in order to identify strategies and programmes that could assist in reducing DC in Africa. The aim of this systematic review was to determine the prevalence of DC (condition) amongst the permanent dentition of 12-year-old children (population) in Africa (context).
Methods
A systematic review and meta-analysis was performed. Peer reviewed cross-sectional articles from January 2000 until December 2021 was searched and this included the following databases: Pubmed (Medline); SCOPUS; CINAHL (via EBSCOhost); Academic Search Complete (via EBSCOhost); Dentistry and Oral Sciences Sources (via EBSCOhost); and Science Direct. The search was last updated on the 10th January 2022. Joanna Briggs Institute critical appraisal tools were used to assess risk of bias. Prevalence figures were stratified by Urban/Rural status, country and time using a random-effects model. All studies performed on children 12-year-olds on the African continent were included. The prevalence of DC and the DMFT scores were the primary and secondary outcome measures, respectively. Only articles consisting of 12-year-old children who reside in Africa were included in this study. The systematic review was registered with Prospero CRD42021293666.
Results
18,080 participants were included in this review. A total of thirty studies were included in the review. The pooled effect size of dental caries severity was 1.09 (CI 0.91–1.27) and the overall prevalence was 36% (CI 29.4–41.7%). Eritrea (78%) had the highest prevalence of DC while Zambia had the lowest (11%); Eritrea also had the highest DMFT score (2.5) with Sudan having the lowest score (0.49). Urban cities had the highest DMFT score (1.32, CI 0.97–1.68), compared to rural cities (1.13, CI 0.86–1.4) and there was an increasing trend in DC prevalence over time from 28% (CI 23–34%) in 2000 to 2005 to 57% (CI 43–72%) in studies conducted after 2015. The risk of bias was very low where majority of the studies scored more than 50% in the JBI critical appraisal tool.
Conclusions
There was a wide discrepancy in the DC prevalence and scores across the different countries, settings (rural versus urban) and there was an increase in the prevalence over time. This review was self-funded.
Similar content being viewed by others


Introduction
Dental caries (DC) in children is a highly prevalent disease often resulting in pain and difficulty in mastication [1]. According to the Global Burden of Disease study, the prevalence of untreated DC in permanent teeth is 267 million [2].
The sequelae of untreated DC in children include poor school performance [3, 4]; high school absenteeism [3]; verbal bullying [5] and has shown to impact the Oral Health Related Quality of Life (OHRQoL) [6]. The prevalence of caries in 12-year-olds varies from country to country and even within continents. In Africa, the prevalence ranged from 42 to 78% [7,8,9,10,11,12].
DC share risk factors associated with obesity [14, 15]. Although aetiological factors have been described well in literature [16,17,18], there is still a very high prevalence rate across the globe. There are significant costs are associated with the management of DC and preventative measures, such as toothbrushing, are a much cheaper alternative [19]. However oral health literacy remains quite low [20].
Prevalence of DC in 12-year-olds have been reported in systematic review which highlighted that caries prevalence ranged between 41.9 and 69.4% in lower-middle and upper middle income countries [13]. A study conducted in Dominican Republic and Lithuania reported prevalence of 73% [21] and 85.5% [22]. However, an overall view of dental caries prevalence in 12-year-olds in Africa has not been conducted.
The aim of the systematic review was to determine the prevalence of dental caries (condition) in 12-year-olds (population) in Africa (context) using cross-sectional study designs. The results could assist in identifying public health programmes that can be implemented to manage and reduce the prevalence of DC.
Methodology
The Meta-Analysis of Observational Studies in Epidemiology (MOOSE) guideline was used to conduct this study [23]. A comprehensive search strategy was developed by a community dentistry specialist, a biostatistician and a clinical epidemiologist with a very good background in search strategy. Studies only in English were included. The authors (FKD and AB) conducted a pilot search strategy together before finalizing the ultimate search strategy that was going to be utilized for this study. Searching peer-reviewed articles from January 2000 until December 2021 was conducted and this included the following databases: Pubmed (Medline); SCOPUS; CINAHL (via EBSCOhost); Academic Search Complete (via EBSCOhost); Dentistry and Oral Sciences Sources (via EBSCOhost); and Science Direct. The search strategy for the African studies was obtained from a previous publication [15] and the terms used are listed in Table 1. Contact with authors was documented in the design of this study, but not performed as it was not deemed necessary.
We included children aged 12 years (plus or minus a year) [population], who had dental caries [condition] and who lived in Africa [context].
The search strategy for the African studies was obtained from a previous publication [24].
Hand-searching of eligible articles was also performed. All eligible articles were uploaded into Rayyan where all duplicate articles were removed [25].
Screening and selection criteria
Two authors (FKD and AB) screened titles and abstracts, independently. Full text selection was performed independently. If any disagreements were found in abstract or full text selection, they were discussed until consensus was reached. Only studies conducted in Africa on children who were 12-year-olds (give or take a year) were included in this review. If either the number of children with caries, or the number of the complete sample was missing, then the articles were not included for the prevalence component of the study. If the number of the complete sample, the mean and standard deviation of the mean DMFT was not included, then the article was also not included in the DC severity component of the study. The following articles were excluded: articles without the full text, dissertations, articles not published in English, conference proceedings, letters to the editor, grey literature, and published protocols. Based on inclusion and exclusion criteria, articles were sorted in Rayyan [25] and any disagreements between the authors were clarified through discussion.
Data extraction
Two authors (FKD and AB) extracted the data independently, if there were any disagreements, a consensus was reached through discussion. Although not necessary, the corresponding author could be contacted for any pertinent missing information from any included articles.
Author, year of publication, country of publication, study design, urban/rural status, diagnostic criteria, and the mean number of decayed, missing, and filled permanent teeth (DMFT) were recorded in Excel and uploaded into STATA for further examination.
Critical appraisal
The Joanna Briggs Institute (JBI) critical appraisal checklist for studies reporting prevalence data was used to determine the quality of the included studies [26]. The critical appraisal was performed independently by the two authors and any disagreements were discussed until a consensus was reached. There are nine criteria in the JBI critical appraisal tool and a maximum score of nine indicated a lower risk of bias.
Data synthesis
StataCorp. 2019. STATA Statistical Software: Release 17, College Station, TX: StataCorp LLC was used to conduct the meta-analyses. The I2 test and the Q test was used to determine statistical heterogeneity and subsequently random effects model was utilized due to the significant heterogeneity (I2 > 50%) results obtained. In addition the random /fixed effects model was chosen based on the Tufanaru article [27] which states that a minimum of 5 articles be used to run a random effects meta-analysis. Subgroup analysis was conducted for year of publication, urban/rural status, and country and the confidence intervals were set at 95%. A spatial representation of the distribution of pooled prevalence was carried out in QGIS software. Where possible subgroup analysis was performed per country, urban/rural status and year of publication. If the urban or rural status was unclear, a new category called, “urban/rural” was created.
Results
Search and selection
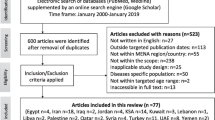
A total of 2097 articles, and a further 198 possible articles were identified before duplication was removed. After the 168 duplicate articles were removed, 2127 articles were screened, where a further 2047 articles were excluded by title and abstract. Thereafter, 80 articles were assessed by reading the full text for eligibility as described in the flow diagram (Fig. 1). Of these 80 articles, 30 articles met the criteria and were included. A total of 50 articles were excluded after reading the full texts and the reasons for their exclusion is shown in Table 2.

Flow diagram of article selection process
A total sample size of 18,080 participants were included in this review. Table 3 summarizes the findings from the included studies. There were 22 articles that determined prevalence and 21 articles which could be included for the DMFT meta-analysis. The overall prevalence was 36% (29.4–41.7) (Fig. 2). The overall mean DMFT was 1.09 (0.91–1.3) [4]. All the studies, except two, utilized the World Health Organization (WHO) criteria (III, IV or V) for the dental examination. The rural prevalence (31%) was lower than the urban prevalence (40%) Fig. 3.

Distribution of mean prevalence across the continent

Meta-Analysis of prevalence of dental caries for urban and rural settings
The overall prevalence of dental caries in 12-year -olds in Africa was 36% (29.4–41.7%) (Fig. 2). The highest prevalence was recorded in Eritrea in 2017 (78%; 95% CI 72.4–83.1%), followed by Sao Tome (73%, 95% CI 69.4–75.9%) with the lowest prevalence scores in Zambia (11%) and Nigeria (13%) (Table 4). Overall, the confidence intervals were relatively large indicating small sample sizes and a wide range within the results.
The mean DMFT score was the highest for Eritrea (2.5 (95% C.I.: 2.17–2.88)) followed by The Gambia (2.27 (95% C.I.: 1.93–2.61)) and Libya (2.11 (95% C.I.: 1.18–3.04)).
All of the studies were cross sectional in design and carried out by oral health personnel including dentists and dental therapists.
Diagnostic criteria is the method used to evaluate dental caries
The overall DMFT was 1.09 (95% C.I.: 0.91–1.27) (Table 3). The lowest DMFT scores were recorded in Sudan (0.49 (95% C.I.: 0.46–0.52)), Nigeria (0.60) and Burkina Faso (0.70 (95% C.I.: 0.37–0.83)) while the highest scores were obtained in Eritrea (2.50 (95% C.I.: 2.17–2.83)), the Gambia (2.27 (95% C.I.:1.93–2.61)) and Libya (2.11 (95% C.I.: 1.18–3.04)). In general, the confidence intervals were relatively large indicating small samples and a wide range within the results.
Urban cities had the highest pooled prevalence (40%, 95% C.I.: 23.3–57.4%) compared to rural cities (31%, 95% C.I.: 18.6–44.3%) (Fig. 3). Some studies did not indicate the setting and were pooled into a single group called urban/rural.
The mean DMFT in rural and urban settings were similar to the caries prevalence; urban settings recording a mean DMFT score of 1.32 (95% C.I.: 0.97–1.68) and rural settings recording a lower 1.13 (95% C.I.: 0.86–1.4) score (Fig. 4). Those studies which did not indicate the type of setting, reported a mean score of 1.00 (95% C.I.: 0.80–1.21. Again, similar to the other results, the confidence intervals were relatively large.

Meta-Analysis of mean DMFT scores for urban/rural settings. Note Weights and between-subgroup heterogeneity test are from random-effects model
The prevalence of dental caries in 12-year-old children in 2000–2004 was 28.2% (95% C.I.: 22.7–33.7), 2005–2009, 32.9% (95% C.I.: 11.1–54.8), 2010–2014 was 34.6% (95% C.I.:8.5–60.6) and in 2015 and above, it was 57.4% (95% C.I.:42.7–72.1) (Figs. 5 and 6). Although the confidence intervals were quite large, nevertheless the DC increased over time.

Meta-Analysis of prevalence of dental caries for different time periods

Meta-Analysis of DMFT scores during different time periods. NOTE: Weights and between-subgroup heterogeneity test are from random-effects mod
The mean DMFT scores was 0.99 (95% C.I.:0.73–1.26) in 2000–2004, 1.08 (95% C.I.:0.0–2.26) in 2005–2009, 0.58 (95% C.I.:0.32–0.84) in 2010–2014, and increased to 1.80 (95% C.I.:1.49–2.11) from 2015 to present (Fig. 6).
Pooled effect size of dental caries severity in Africa
The pooled effect size of dental caries severity was 1.09 (95% C.I .:0.914–1.27) (Fig. 3). The highest mean DMFT score was seen in Eritrea (2.5, 95% C.I.: 2.17–2.83), and the lowest was seen in Tanzania (0.61, 95% C.I.: 0.31–0.91). Urban cities had the highest mean DMFT score (1.32, 95% C.I.: 0.97–1.68), compared to rural cities (1.13, 95% C.I.: 0.86–1.4) (Fig. 5).
Critical appraisal
Twenty-eight studies found that the sampling frame was appropriately addressed to the target population and that the study participants were sampled in an appropriate way. In addition, 28 articles found valid methods to have been employed to identify dental caries. However, the study subjects were not described in detail in 22 studies, there was not a sufficient sample size for 23 of the studies and 18 studies found that appropriate statistical analysis was not used (Table 5).
Publication bias
Begg’s test and funnel plots were both significant which indicates that there was publication bias (p < 0.001). Publication bias was also assessed using Duval and Tweedies “Trim and Fill” method for prevalence (Fig. 7) and DMFT scores (Fig. 8). The prevalence was 35.4 (34.8–36.1), which indicated that zero studies were missing using a random effects model. Furthermore, the DMFT score was 0.47 (0.46–0.48), and indicated that 6 studies were missing. These results indicated that there was publication bias for the DMFT outcome but not for prevalence.

Publication bias for prevalence

Publication bias for dmft
The critical appraisal was done using the Joanna Briggs Institute (JBI) criteria and a maximum score of 9 indicated that there was minimal bias.
Discussion
This current study is the first of its kind evaluating the prevalence of DC in Africa for children of 12 years of age. The 12-year old age group is often neglected with many studies focussing on either the under 6-year olds and/or the 15-year olds. The 12-year-olds provide an ideal window to measure the impact of school based and fissure sealant programmes which are often undertaken when children are between the ages of 6 and 8 years old. In addition, the 12-year- olds also provide an opportunity to assess the status of the permanent teeth and the exfoliation of the primary dentition.
The current prevalence of DC was 36% (95% C.I.: 29.4–41.7%) which was lower than a study on 12-year -olds in Puerto Rico (39.3%) [103]. However, the caries prevalence was higher than that recorded on 12-year-old children in Haiti (31%) [104]. This discrepancy might be due to the differences in socio-economic status, the data collection indices, the educational levels and fluoride levels. These studies were individual studies while the current study is a systematic review of all African countries which could explain the difference in the results.
The mean DMFT was 1.09 which was much lower than the WHO goal of 12-year-old’s which estimates that the DMFT score be less than 3 [105]. Interestingly, the DMFT and caries prevalence was the highest in Eritrea (2.50 and 78% respectively). Eritrea has had many challenges including famines, recurrent wars and drought which has resulted in over 66% of the population living below the poverty line [106]. These factors could have impacted on the provision of dental services and education in the early years of these children which may have contributed to the high caries prevalence. The impact of war could have also decreased access to essentials such as toothbrushes and toothpaste which could have been partly responsible for the caries scores. Although Vasireddy [18]. reported that poverty could have a negative impact on dental caries prevalence, the impact of famine and war could have easily been responsible for the high caries scores.
The other country with a relatively high mean DMFT score was Libya (2.11). The study in Libya with the highest mean DMFT score was 2.66 and a possible reason for this was the setting. This study was carried put at a paediatric dental hospital and not a school setting. As a result, all those who attended required some sort of dental treatment and this could be the reason for the high score. This was confirmed by the second Libyan study which reported a mean DMFT score of 1.70 which could indicate the actual prevalence to be slightly lower.
The Gambia also recorded a high mean DMFT score (2.27). These results showed that rural children had a significantly higher mean DMFT score (2.84) compared to high socio-economic status urban children (1.69). The possible reasons for this high score was cited as a lack of access to services, poor diet and poor dental knowledge among young children. Preventive programs and educational programmes need to be implemented in general in African countries, especially in rural areas.
Countries with the lowest mean DMFT scores were in Sudan (0.49), Nigeria (0.60) and Burkina Faso (0.70). The Nigerian studies all cited the lower DMFT scores to the school programs, frequency of dental visits and brushing frequencies. This showed that a good environment can assist in the reduction of dental caries. The Sudanese study, although having a low mean DMFT score, reported that urban children and children of a high socioeconomic status had higher mean DMFT scores compared to rural children. The low mean DMFT score amongst the rural cohort was attributed to the diet and high level of oral hygiene.
A subgroup analysis showed that urban status resulted in a higher caries prevalence compared to rural status. This finding was corroborated by Al-Akwa [107] who also found that caries prevalence was higher in urban areas compared to rural areas. Urban poverty has also been linked to poor access to healthy eating and food insecurity [108]. The mean DMFT scores were also higher in urban cities compared to rural cities. This could be due to the diet in urban areas which usually comprise of refined carbohydrates rather than the rural diets which usually contain less sugars. It’s also possible that communities in rural areas utilise borehole water which tends to contain more fluoride compared to the urban areas which have a central water source that usually is derived from dams. The water derived from dams often has a much lower fluoride concentration.
Although the caries prevalence changed over time, the changes were not significant. It was expected that the caries prevalence would have decreased over time, but the results showed that the prevalence steadily increased. This could have been due to urbanization, access to refined carbohydrates, increase sugar intake and possibly a more urbanised diet compared to a more rural diet.
Twenty seven of the thirty articles presented with a critical appraisal of more than 50%. Eleven articles presented with a score of nine (Table 5).
Conclusions and recommendations
The mean DMFT and caries prevalence reported in this systematic review demonstrates that the WHO goal for 12-year-olds has been reached in Africa. We should however view these findings with great care because of the high heterogeneity between the studies and the high risk of bias. We would recommend that studies of high quality be conducted in Africa so that we can determine the mean DMFT scores and caries prevalence. Studies should include the setting of the sample (rural or urban) the socio-economic status, the indices used, the calibration of examiners, the appropriate statistical test and sample size and oral hygiene practices. This will allow studies to be pooled and compared to identify possible programmes that could impact on the dental disease burden.
Limitations
Many studies did not include all the data and in some of the studies, the data was collapsed and difficult to identify. This made the analysis more difficult. Studies that were not published in English were excluded as there is a great diversity in languages in Africa.
Given the different countries that were included, the times at which the data was collected and the settings, there was no inter-country calibration and as such the results need to be interpreted with caution.
Availability of data and materials
The datasets for this study can be made available on reasonable request to fkimmie@uwc.ac.za.
References
Gilchrist F, Marshman Z, Deery C, Rodd HD. The impact of dental caries on children and young people: What they have to say? Int J Paediatr Dent. 2015;25(5):327–38.
Bernabe, Marcenes W, Hernandez CR, Bailey J, Abreu LG, Alipour V, et al. Global, regional, and national levels and trends in burden of oral conditions from 1990 to 2017 a systematic analysis for the global burden of disease 2017 study. J Dent Res. 2020;362–73.
Karki S, Päkkilä J, Laitala ML, Humagain M, Anttonen V. Influence of dental caries on oral health-related quality of life, school absenteeism and school performance among Nepalese schoolchildren. Community Dent Oral Epidemiol. 2019;47(6):461–9.
Quadros LN, Rebelo MAB, de Queiroz AC, Pereira JV, Vettore MV, Rebelo Vieira JM. Clinical consequences of untreated dental caries and school performance in low-income adolescents. Int J Paediatr Dent. 2021;31(5):619–26.
Barasuol JC, Soares JP, Castro RG, Giacomin A, Goncalves BM, Klein D, et al. Untreated dental caries is associated with reports of verbal bullying in children 8–10 years old. Caries Res. 2017;51(5):482–8.
Faker K, Tostes MA, de Paula VAC. Impact of untreated dental caries on oral health-related quality of life of children with special health care needs. Braz Oral Res. 2018;32:1–9.
Mahesh Kumar P, Joseph T, Varma RB, Jayanthi M. Oral health status of 5 years and 12 years school going children in Chennai city—An epidemiological study. J Indian Soc Pedod Prev Dent. 2005;23(1):17–22.
Ravishankar PL, Jayapalan CS, Gondhalekar RV, Krishna BJ, Shaloob KMM, Ummer PF. Prevalence of dental caries and oral hygiene status among school going children: an epidemiological study. J Contemp Dental Pract. 2013;14(4):743–6.
Munjal V, Garewal R, Gupta A, Kaur P. Dental caries prevalence and treatment needs in 12 and 15-year-old school children of Ludhiana city. Indian J Oral Sci. 2013;4(1): 27.
Andegiorgish AK, Weldemariam BW, Kifle MM, Mebrahtu FG, Zewde HK, Tewelde MG, et al. Prevalence of dental caries and associated factors among 12 years old students in Eritrea. BMC Oral Health. 2017;17(1):1–6.
Simon C, Tesfaye F, Berhane Y. Assessment of the oral health status of school children in Addis Ababa. Addis Ababa University School of graduate studies; 2000.
Alraqiq H, Eddali A, Boufis R. Prevalence of dental caries and associated factors among school-aged children in Tripoli, Libya: a cross-sectional study. BMC Oral Health. 2021;21(1): 1–2.
Frencken JE, Sharma P, Stenhouse L, Green D, Laverty D, Dietrich T. Global epidemiology of dental caries and severe periodontitis—a comprehensive review. J Clin Periodontol. 2017;44:S94–105.
Manohar N, Hayen A, Fahey P, Arora A. Obesity and dental caries in early childhood: a systematic review and meta-analyses. Obes Rev. 2020;21(3): e12960.
Paisi M, Kay E, Bennett C, Kaimi I, Witton R, Nelder R, et al. Body mass index and dental caries in young people: a systematic review. BMC Pediatr. 2019;19(1):122.
Que L, Jia M, You Z, Jiang L-C, Yang C-G, Quaresma AA, et al. Prevalence of dental caries in the first permanent molar and associated risk factors among sixth-grade students in São Tomé Island. BMC oral health. 2021;21(1):483.
Pratyusha N, Vinay C, Uloopi KS, Rojaramya KS, Ahalya P, Devi C. Association of serum vitamin D and salivary calcium and phosphorus levels in 3–11-year-old schoolchildren with dental caries. J Indian Soc Pedod Prev Dent. 2021;39(3):240–5.
Vasireddy D, Sathiyakumar T, Mondal S, Sur S. Socioeconomic factors associated with the risk and prevalence of dental caries and dental treatment trends in children: a cross-sectional analysis of national survey of children’s health (NSCH) data, 2016–2019. Cureus. 2021;13(11): e19184.
Medina-Solis CE, Avila-Burgos L, Borges-Yanez SA, Irigoyen-Camacho ME, Sanchez-Perez L, Zepeda-Zepeda MA, et al. Ecological study on needs and cost of treatment for dental caries in schoolchildren aged 6, 12, and 15 years: Data from a national survey in Mexico. Medicine (Baltimore). 2020;99(7): e19092.
Baskaradoss JK. Relationship between oral health literacy and oral health status. BMC Oral Health. 2018;18(1):172.
Diaz-Nicolas J, Silva-Vetri MG, Rivas-Tumanyan S, Toro M, Elías-Boneta AR. Prevalence of dental caries in 12-year-olds in San Pedro de Macorís. DR Puerto Rico Health Sci J. 2020;39(2):210–5.
Milciuviene S, Bendoraitiene E, Andruskeviciene V, Narbutaite J, Sakalauskiene J, Vasiliauskiene I, et al. Dental caries prevalence among 12–15-year-olds in Lithuania between 1983 and 2005. Medicina (Lithuania). 2009;45(1):68–76.
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–12.
Pienaar E, Grobler L, Busgeeth K, Eisinga A, Siegfried N. Developing a geographic search filter to identify randomised controlled trials in Africa: finding the optimal balance between sensitivity and precision. Health Info Libr J. 2011;28(3):210–5.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5(210):1
Joanna Briggs I. Joanna Briggs Institute critical appraisal checklist for prevalence Ssudies.
Tufanaru C, Munn Z, Stephenson M, Aromataris E. Fixed or random effects meta-analysis? Common methodological issues in systematic reviews of effectiveness. Int J Evid Based Healthc. 2015;13(3):196–207.
Adeniyi A, Oyapero A, Ekekezie O, Braimoh M. Dental caries and nutritional status of school children in Lagos Nigeria-a preliminary survey caries. J West Afr Coll Surg. 2016;6(3):15.
Abbass MMS, Mahmoud SA, El Moshy S, Rady D, Abubakr N, Radwan IA, et al. The prevalence of dental caries among egyptian children and adolescences and its association with age, socioeconomic status, dietary habits and other risk factors. A cross-sectional study [version 1; referees: 1 approved, 2 approved with reservations]. F1000Research. 2019;8:1–19.
Abid A. Oral health in Tunisia. Int Dent J. 2004;54:389–94.
Adeniyi AA, Agbaje O, Onigbinde O, Ashiwaju O, Ogunbanjo O, Orebanjo O, et al. Prevalence and pattern of dental caries among a sample of Nigerian public primary school children. Oral Health Prev Dent. 2012;10(3):267–74.
Aidara AW, Bourgeois D. Prevalence of dental caries: national pilot study comparing the severity of decay (CAO) versus ICDAS index in Senegal. Odontostomatol Trop. 2014;37(145):53–63.
Ajayi DM, Abiodun-Solanke IF. Sociobehavioural risk factors of dental caries among selected adolescents in Ibadan. Niger Pediatr Dent J. 2014;24(1):33–8.
Arrish W, Altaher SA, Ahmed MA. Assessment of dental caries status among school children aged 9–12 years of Sebha city-Libya by using of dft/ DMFT & SiC indices. J Med Sci. 2020;15(1):31–7.
Awadia AK, Birkeland J, Haugejorden O, Bjorvatn K. Caries experience and caries predictors–a study of Tanzanian children consuming drinking water with different fluoride concentrations. Clin Oral Invest. 2002;6(2):98–103.
Azodo CC, Chukwumah NM, Enabulele JE, Adeghe HA. Relating dental caries experience with body mass index among Nigerian primary school children: a cross-sectional survey. J Educ Ethics Dent. 2012;2(1):28.
Berndt C, Meller C, Poppe D, Splieth CH. Fluorosis, caries and oral hygiene in schoolchildren on the Ombili foundation in Namibia. Oral Health Prev Dent. 2010;8(3):269–75.
Birkeland JM, Ibrahim YE, Ghandour IA, Haugejorden O. Severity of dental caries among 12-year-old Sudanese children with different fluoride exposure. Clin Oral Invest. 2005;9(1):46–51.
Blankson P-K, Amoah G, Thadani M, Newman-Nartey M, Amarquaye G, Hewlett S, et al. Prevalence of oral conditions and associated factors among schoolchildren in Accra, Ghana: a cross-sectional study. Int Dent J. 2021.
Carneiro LC, Kabulwa MN. Dental caries, and Supragingival plaque and Calculus among Students, Tanga. Tanzania ISRN Dent. 2012;2012:1–6.
Cheng J, Campbell K. Caries and dental erosion: Are soroti children and adolescents at risk from increased soft-drink availability in Uganda? Afr Health Sci. 2016;16(4):943–6.
Doumit M, Doughan B. Dental caries and fluorosis among children in Lebanon. Indian J Dent Res. 2018;29(3):317–22.
El-Sayed MEH, Osman KH, El Nour ALB. Prevalence of dental caries and its impact on the academic performance of Sudanese basic school children, AL-Sahafa residential area (2013–2014). J Am Sci. 2015;11(4):13–21.
Faye M, Sissoko B, Gueye Diagne MC, Tamba Fall A, Diop F, Yam AA. Relationship between oral health status of parents and that of their children. Odontostomatol Trop. 2009;32(125):5–10.
Folayan MO, El Tantawi M, Oginni O, Arowolo O. Is chronotype profile a risk indicator for caries in children and adolescents in sub-urban Nigeria? Int J Paediatr Dent. 2021;31(5):627–33.
Folayan MO, Kolawole KA, Onyejaka NK, Agbaje HO, Chukwumah NM, Oyedele TA. General anxiety, dental anxiety, digit sucking, caries and oral hygiene status of children resident in a semi-urban population in Nigeria. BMC Oral Health. 2018;18(1):1–10.
Folayan MO, Kolawole KA, Oziegbe EO, Oyedele TA, Agbaje HO, Onjejaka NK, et al. Association between family structure and oral health of children with mixed dentition in suburban Nigeria. J Indian Soc Pedod Prev Dent. 2017;35(2):134–42.
Folayan MO, Oginni O, Arowolo O, El Tantawi M. Association between adverse childhood experiences, bullying, self-esteem, resilience, social support, caries and oral hygiene in children and adolescents in sub-urban Nigeria. BMC Oral Health. 2020;20(1):1–11.
Gabroun E, Berbash A, Abusreweil S, Shetwi N. Dental caries experience among 6–14 years old Schoolchildren in Municipality of Tripoli Center, Libya *Ebtehal Gabroun **Amel Berbash ***Sara Abusreweil ****Najeha Shetwi. 2018:1–14.
Grobler SR, Louw AJ, Van W. Kotze TJ. Dental fluorosis and caries experience in relation to three different drinking water fluoride levels in South Africa. Int J Paediatr Dent. 2001;11(5):372–9.
Hirschowitz AS. Dental earies, gingival health and maloeelusion in 12-year-old urban Blaek sehoolehildren from Soweto, Johannesburg. 2000.
Hobdell M, Tsakos G, Sprod A, Ladrillo TE, Ross MW, Gordon N, et al. Using an oral health-related quality of life measure in three cultural settings. Int Dent J. 2009;59(6):381–8.
Kiwanuka SN, Åstrøm AN. Self-reported dental pain and associated factors in Ugandan schoolchildren. Norsk Epidemiologi. 2005;15(2):175–82.
Kolawole KA, Folayan MO, Agbaje HO, Oyedele TA, Oziegbe EO, Onyejaka NK, et al. Digit sucking habit and association with dental caries and oral hygiene status of children aged 6 months to 12 years resident in semi-urban Nigeria. PLoS ONE 2016.
Kumar N. Dental caries status among 6–14 years old school going children of Sebha city, Libya. 2016(March).
Lawal FB, Bankole OO. Impact of untreated dental caries on daily performances of children from low social class in an urban African population: the importance of pain. Pesquisa Brasileira em Odontopediatria e Clinica Integrada. 2019;19(1):1–9.
Mashoto KO, Åstrøm AN, David J, Masalu JR. Dental pain, oral impacts and perceived need for dental treatment in Tanzanian school students: a cross-sectional study. Health Qual Life Outcomes. 2009;7.
Mbawalla HS, Mtaya M, Masalu JR, Brudvik P, Astrom AN. Discriminative ability of the generic and condition-specific child-oral impacts on daily performances (Child-OIDP) by the Limpopo-Arusha school health (LASH) project: a cross-sectional study. BMC Pediatr. 2011;11:1–10.
Okoye LO, Chukweneke FN, Akaji EA, Folaranmi N. Caries experience among school children in Enugu, Nigeria. Okoye LO, Chukweneke FN, Akaji. J Coll Med. 2012;15(2).
Okullo I, Åstrøm AN, Haugejorden O, Rwenyonyi CM. Variation in caries experience and sugar intake among secondary school students in urban and rural Uganda. Acta Odontol Scand. 2003;61(4):197–202.
Olatosi OO, Oyapero A, Onyejaka NK. Disparities in caries experience and socio-behavioural risk indicators among private school children in Lagos, Nigeria. Pesquisa Brasileira em Odontopediatria e Clinica Integrada. 2020;20:1–13.
Oyedele T, Chukwumah N, Adeyemo Y. Dental caries experience and molar-incisor hypomineralisation in children: pattern and severity. Niger J Basic Clin Sci. 2020;17(2):103.
Oyedele TA, Fadeju AD, Adeyemo YI, Nzomiwu CL, Ladeji AM. Impact of oral hygiene and socio-demographic factors on dental caries in a suburban population in Nigeria. Eur Arch Paediatr Dent. 2018;19(3):155–61.
Robert K, Tejinder PS, Caren JF, Lisa HG. Assessment of dental caries and oral health challenges of school-age children in rhino camp refugee settlements in Arua, Uganda. Int J Oral Dent Health. 2019;5(2):1–4.
Rubin PF, Winocur E, Erez A, Birenboim-Wilensky R, Peretz B. Dental treatment needs among children and adolescents residing in an ugandan orphanage. J Clin Pediatr Dent. 2016;40(6):486–9.
Rugarabamu PGN, Poulsen S, Masalu JRP. A longitudinal study of occlusal caries among schoolchildren in Dar es Salaam, Tanzania. Community Dent Oral Epidemiol. 2002;30(1):47–51.
Simangwa LD, Johansson AK, Johansson A, Minja IK, Åstrøm AN. Oral impacts on daily performances and its socio-demographic and clinical distribution: a cross-sectional study of adolescents living in Maasai population areas. Tanzania Health Qual Life Outcomes. 2020;18(1):1–11.
Simangwa LD, Åstrøm AN, Johansson A, Minja IK, Johansson A-K. Oral diseases and socio-demographic factors in adolescents living in Maasai population areas of Tanzania: a cross-sectional study. BMC oral health. 2018;18(1):200.
Simushi N, Nyerembe SA, Sasi R, Siziya S. Dental caries on permanent dentition in primary school children—Ndola, Zambia, 2017. ZnphiCoZm. 2018;00002911:5–16.
Sofola OO, Folayan MO, Oginni AB. Changes in the prevalence of dental caries in primary school children in Lagos State. Nigeria Niger J Clin Pract. 2014;17(2):127–33.
Soroye M, Adegbulugbe C. Oral health status, knowledge of dental caries aetiology, and dental clinic attendance: a comparison of secondary school students in the rural and urban areas of Lagos. Port Harcourt Med J. 2016;10(2):42.
Ndanu TA, Aryeetey R, Sackeyfio J, Otoo G, Lartey A. Oral hygiene practices and caries prevalence among 9–15 years old ghanaian school children. J Nutrit Health Sci. 2015;1(4):1–8.
Teshome A, Gizachew M, Yitayeh A, Gizachew M. Prevalence of dental caries and associated factors among Finote Selam primary school students aged 12–20 years, Finote Selam Town, Ethiopia Group b streptococcus in enoates View project Systematic Review on Effectiveness of shoulder taping in Hemiplegia V. 2016(February).
Thema LK, Singh S. Epidemiological profile of patients utilising public oral health services in Limpopo province, South Africa. Afr J Prim Health Care Fam Med. 2017;9(1):e1–5.
van Wyk C, van Wyk PJ. Trends in dental caries prevalence, severity and unmet treatment need levels in South Africa between 1983 and 2002. SADJ. 2010;65(7):310.
Wandera M, Twa-Twa J. Baseline survey of oral health of primary and secondary school pupils in Uganda. Afr Health Sci. 2003;3(1):19–22.
Adekoya-Sofowora CA, Nasir WO, Oginni AO, Taiwo M. Dental caries in 12-year-old suburban Nigerian school children. Afr Health Sci. 2006;6(3):145–50.
Almerich-Silla JM, Montiel-Company JM. Influence of immigration and other factors on caries in 12- and 15-yr-old children. Eur J Oral Sci. 2007;115(5):378–83.
Bajomo AS, Rudolph MJ, Ogunbodede EO. Dental caries in six, 12 and 15 year old Venda children in South Africa. East Afr Med J. 2004;81(5):236–43.
Batwala V, Mulogo EM, Arubaku W. Oral health status of school children in Mbarara. Uganda Afr Health Sci. 2007;7(4):233–8.
Braimoh OB, Umanah AU, Ilochonwu NA. Caries distribution, prevalence, and treatment needs among 12–15-year-old secondary school students in Port Harcourt, Rivers State. Niger J Dent Surg. 2014;2014:1–6.
Brindle R, Wilkinson D, Harrison A, Connolly C, Cleaton-Jones P. Oral health in Hlabisa, KwaZulu/ Natal—a rural school and community based survey. Int Dent J. 2000;50(1):13–20.
Chukwumah NM, Folayan MO, Oziegbe EO, Umweni AA. Impact of dental caries and its treatment on the quality of life of 12- to 15-year-old adolescents in Benin. Niger Int J Paediatr Dent. 2016;26(1):66–76.
Denloye O, Ajayi D, Bankole O. A Study of dental caries prevalence in 12–14 year old school children in Ibadan. Niger Pediatr Dent J. 2005;15(2):147–51.
Elfseyie M, Alaskandrani R, Huew R, Huew R. Evaluation of health status of the first permanent molars of children aged 6 to 12 years in Benghazi. Libya Ijmsssr. 2020;2(4):110–6.
Fukuda H, Ogada CN, Kihara E, Wagaiyu EG, Hayashi Y. Oral Health status among 12-year-old children in a rural Kenyan community. J Dent Oral Hea. 2014;1:1–5.
Kikwilu EN, Mandari GJ. Dental caries and periodontal conditions among primary school children in morogoro municipality, Tanzania. East Afr Med J2001. 152–6.
Kosovic S, Nilsson-Andersson A. Survey of dental caries prevalence, dietary and oral hygiene habits among urban and rural 5 and 12-years old children in The Gambia. 2001(3):441–52.
Kutesa A, Kasangaki A, Nkamba M, Muwazi L, Okullo I, Rwenyonyi CM. Prevalence and factors associated with dental caries among children and adults in selected districts in Uganda. Afr Health Sci. 2015;15(4):1302–7.
Mafuvadze BT, Mahachi L, Mafuvadze B. Dental caries and oral health practice among 12 year old school children from low socio-economic status background in Zimbabwe. Pan Afr Med J. 2013;14:164.
Molete MM, Igumbor J, Stewart A, Yengopal V. Dental status of children receiving school oral health services in Tshwane. South Afr Dent J. 2019;74(4):171–7.
Msyamboza KP, Phale E, Namalika JM, Mwase Y, Samonte GC, Kajirime D, et al. Magnitude of dental caries, missing and filled teeth in Malawi: National Oral Health Survey. BMC Oral Health. 2016;16(1).
Muwazi LM, Rwenyonyi CM, Tirwomwe FJ, Ssali C, Kasangaki A, Nkamba ME, et al. Prevalence of oral diseases/conditions in Uganda. Afr Health Sci. 2005;5(3):227–33.
Mwakatobe AJ, Mumghamba EG. Oral health behavior and prevalence of dental caries among 12-year-old school-children in Dar-es-Salaam. Tanzania Tanzania Dent J. 2007;14(1):1–7.
Nkambule NR, Madiba TK, Bhayat A. Dental caries, body mass index, and diet among learners at selected primary schools in pretoria, Gauteng Province. South Afr J Contemp Dent Pract. 2019;20(11):1241–8.
Nurelhuda NM, Trovik TA, Ali RW, Ahmed MF. Oral health status of 12-year-old school children in Khartoum state, the Sudan; A school-based survey. BMC Oral Health. 2009;9(1):1–9.
Okoye L, Ekwueme O. Prevalence of dental caries in a nigerian rural community: a preliminary local survey. Ann Med Health Sci Res. 2011;1(2):187–95.
Owino RO, Masiga MA, Ng’Ang’A PM, Macigo FG. Dental caries gingivitis and the treatment needs among 12-year-olds. East Afr Med J. 2010;87(1):25–31.
Smit D, Barrie R, Louw A. The burden of dental caries in the western cape and a recommended turn-around strategy. South Afr Dent J. 2017;72(8):360–5.
van Wyk PJ, Louw AJ, du Plessis JB. Caries status and treatment needs in South Africa: report of the 1999–2002 National Children’s Oral Health Survey. SADJ. 2004;59(6):238.
Varenne B, Petersen PE, Ouattara S. Oral health status of children and adults in urban and rural areas of Burkina Faso. Africa Int Dent J. 2004;54(2):83–9.
Waweru LW, Opinya GN, Ng’Ang’A PM. Comparison of the prevalence of dental caries in 12–15 year-old children with dental fluorosis and those without dental fluorosis from juja in rural Kenya. East Afr Med J. 2016;93(9):416–20.
Elias-Boneta A, Toro MJ, Rivas-Tumanyan S, Murillo M, Orraca L, Encarnación-Burgos A, et al. Persistent oral health disparity in 12-year-old Hispanics_ a cross-sectional study. BMC Oral Health. 2016;16(10).
Psoter W, Saint Jean LP, Morse DE, Prophte SE, Joseph JE, Katz RV. Dental caries in twelve- and fifteen-year-olds_ results from the basic oral health survey in Haiti. J Publ Health Dent. 2005;65(4):209–14.
Aggeryd T. Goals for oral health in the year 2000: cooperation between WHO, FDI and the national dental associations. Int Dent J. 1983;33(1):55–9.
Rena R. Poverty in Eritrea_challenges and implications for development. Int Soc Sci J. 2009;60(197–198).
Al-Akwa AA, Al-Maweri SA. Dental caries prevalence and its association with fluoride level in drinking water in Sana’a. Yemen Eur J Dent. 2018;12:15–20.
Vilar-Compte M, Burrola-Mendez S, Lozano-Marrufo A, Ferre-Eguiluz I, Flores D, Gaitan-Rossi P, et al. Urban poverty and nutrition challenges associated with accessibility to a healthy diet: a global systematic literature review. Int J Equity Health. 2021;20(1):40.
Acknowledgements
The authors would like to thank Dr Dalia Elamien for assisting with the data collection and Mr Perseverance Savieri for the production of the GIS map.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Both, FKD and AB have contributed equally to this work and share first authorship. Both the authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing Interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kimmie-Dhansay, F., Bhayat, A. Prevalence of dental caries in the permanent dentition amongst 12-year-olds in Africa: a systematic review and meta-analysis. BMC Oral Health 22, 453 (2022). https://doi.org/10.1186/s12903-022-02489-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-022-02489-4