
Abstract
Objective
To evaluate the effects of different attachment configurations with and without buccal root torque on expansion movements achieved with aligners through finite element analysis (FEA).
Methods
FEA modelling was done with 0.25 mm buccal expansion force application to the maxillary molars with different attachment configurations: Eight models were tested (1) no attachment (NA), (2) horizontal attachment (HA), (3) gingivally beveled horizontal attachment (GHA), and (4) occlusally beveled horizontal attachment (OHA), as well as models with 6obuccal root torque, (5) no attachment (TNA), (6) horizontal attachment (THA), (7) gingivally beveled horizontal attachment (TGHA), and (8) occlusally beveled horizontal attachment (TOHA).
Results
The first and second molars exhibited buccal tipping in all models. The highest amount of buccal tipping for the molars was observed in the NA (6CMB, 0.232 mm; 6CMP, 0.246 mm; 7CMB, 0.281 mm; 7CMP, 0.312 mm) and GHA (6CMB, 0.230; 6CMP, 0.245; 7CMB, 0.279 mm; 7CMP, 0.311 mm) models, respectively, while the least tipping was observed in the TOHA model (6CMB, 0.155 mm; 6CMP, 0.168 mm; 7CMB, 0.216 mm; 7CMP, 0.240 mm). In all groups, the buccal tipping of the second molars was higher than that of the first molars.
Conclusion
This FEA study showed that expansion with aligners tip maxillary molars buccally and the use of occlusally beveled attachments and addition of buccal root torque reduces uncontrolled buccal tipping.
Similar content being viewed by others


Background
Clear aligners, have gained popularity over traditional orthodontic appliances, due to aesthetics, ease of use and requiring fewer dental visits [1,2,3,4,5]. In spite of its popularity, studies have shown that aligners are not as effective as fixed appliances and fail to produce adequate occlusal contacts. The most predictable movements achieved with aligners are buccolingual crown tipping and lingual constriction. Movements such as rotations, incisor intrusion and torque control are difficult and less than 50% accurate [1, 2, 6, 7]. Over time, different aligner materials and attachment types were introduced to improve effectiveness of clear aligner treatment (CAT).
There are several methods of achieving maxillary expansion and arch development, that range from rapid maxillary expanders, quad-helix, and archwires, to aligners, all with different indications and biomechanical capabilities. Since one of the easier movements to achieve with aligners is buccolingual tipping, aligners are used in patients with mild to moderate amount of dentoalveolar expansion need [8, 9]. By using aligners to expand arches in non-growing individuals, the correction takes place with buccal tipping of posterior teeth, which causes the palatal cusps to move occlusally. To minimize this and to achieve bodily tooth movement, torque compensation with addition of buccal root torque was suggested [10, 11]. A recent systematic review showed that expansion, with clear aligners was not completely predictable, and the rate of expansion decreased from anterior to posterior teeth.
Most common type of research methodology used to assess aligner effectiveness is superimposing posttreatment scans over the final simulated digital models to determine the differences between the predicted and achieved movements. Another commonly utilized method is Finite element analysis (FEA). FEA is a computer-aided engineering method used in dentistry to analyze mechanical behavior of structures [4, 6, 12]. In comparison to in-vitro studies, the advantage of using FEA, is the ability to estimate the stresses generated within the alveolar bone, periodontal ligament (PDL), and teeth with different orthodontic appliances, as well as determining the loading and displacement patterns.
Previous studies on different attachment designs showed that horizontal rectangular attachments with or without bevels are the most favored type for various tooth movements, such as incisor extrusion and mesiodistal movement during space closure [7, 13, 14]. A study conducted by Dasy et al. [15] stated that the utilization of rectangular beveled attachments also had a substantial positive impact on aligner retention. The application of horizontal rectangular attachments to posterior teeth was suggested as one of the ways to improve arch expansion with aligners [8]. Zhang et al. [10] utilized FEA to study effects of additional torque and concluded that it was effective in controlling tipping, but also reduced the efficiency of maxillary arch expansion. Yao et al. [11] investigated different attachment designs ranging from ball shaped to cuboid to cylinder and compensatory torque during expansion with clear aligners. They found that torque expression was not linear and the most effective attachment type was the cylinder among the tested. However, this is not a commonly used attachment design.
There is a scarcity of information in the literature regarding the effects of attachment configurations and torque compensation on maxillary arch expansion with aligners. Therefore, this study aimed to evaluate the effects of different attachment configurations with and without compensatory buccal root torque on molar teeth during maxillary expansion with aligners using FEA.
Materials and methods
Model creation
Three-dimensional (3D) finite element models were created using cone beam computed tomography (CBCT) data. Finite element stress analysis was performed using HP workstations that were equipped with INTEL Xeon E-2286 processors operating at a 2.40 GHz clock speed and 64 GB ECC memory. A 3D model in .stl format was generated from the CBCT data utilizing 3DSlicer software.
Reverse engineering and 3D CAD activities were carried out with the ANSYS SpaceClaim software, while adaptation of solid models to the analysis environment and creation of optimized mesh activities were performed with the ANSYS Workbench software. The LS-DYNA solver was used to solve the created finite element models.
Material properties
Linear material properties were used in the analysis given the elastic modulus and Poisson ratio. The material properties of the analyzed model are defined numerically in Table 1.
Cortical bone, trabecular bone, teeth, and periodontal ligament
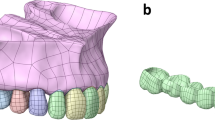
The bone model was reconstructed with a section thickness of 0.1 mm. The CBCT data obtained from the reconstruction was transferred to the 3DSlicer software in DICOM (.dcm) format. The data was segmented based on the relevant Hounsfield values in the 3DSlicer program and transformed into a 3D model through segmentation. The models were exported in .stl format and then transferred to the ANSYS SpaceClaim software, where the maxilla cortical bone and tooth geometry were modeled. A 3D maxillary model with adjustable thickness trabecular bone was obtained by taking the inner surface of the cortical bone as a reference. Periodontal ligaments with a thickness of 0.25 mm were modeled using the outer surface of the teeth as a reference. The modeling process was completed by placing all the prepared models in the correct coordinates in 3D space in the ANSYS SpaceClaim software (Fig. 1).

Eight model groups. (1) NA, (2) HA, (3) GHA, (4) OHA, (5) TNA, (6) THA, (7) TGHA, (8) TOHA
Obtaining mathematical models
Upon completion of the modelling procedure, 3D models were created using ANSYS Workbench software. The created mathematical models were transferred to the LS-DYNA solver for analysis (Fig. 2). The aligners and attachments utilized in the study were designed using ANSYS SpaceClaim, with dimensions derived from the product catalogue of the XXX Company, which was modelled in the software. The thickness of the aligner was adjusted to 0.750 mm, and rectangular attachments with dimensions of 3 mm x 2 mm x 1 mm (width x depth x height) were utilized.

Mathematical Model
Model grouping
Eight groups were created according to the attachment configuration, with and without compensatory buccal root torque (Fig. 1):
Group 1: No attachment (NA).
Group 2: Rectangular horizontal attachment (HA).
Group 3: Gingivally beveled rectangular horizontal attachment (GHA).
Group 4: Occlusally beveled rectangular horizontal attachment (OHA).
Group 5: No attachment and buccal root torque (TNA).
Group 6: Rectangular horizontal attachment and buccal root torque (THA).
Group 7: Gingivally beveled rectangular horizontal attachment and buccal root torque (TGHA).
Group 8: Occlusally beveled rectangular horizontal attachment and buccal root torque (TOHA).
Quantitative model information
Table 2 presents the quantity of nodes and elements within each model.
Loading and boundary conditions
To measure the 3D displacement, two points were selected at the cusp tip level of the maxillary right first and second molars (mesiobuccal (CMB) and mesiopalatal (CMP)) and two points at the root apex level (mesiobuccal (AMB) and palatal (AP)). In this study, an activation force of 0.25 mm was applied to the maxillary first and second molars in the opposite direction of the expansion movement in all groups. The forces created by the aligner on each tooth were calculated, and applied to the model in buccal direction. Furthermore, for Groups 5–8, a 6° torque compensation was utilized in addition to the aligner activation force. Eight nonlinear analyses were conducted on the models, in accordance with the prescribed force and boundary conditions.
The X-axis in the 3D co-ordinate system represented the buccopalatal direction. A positive value on the X-axis indicated movement towards the palatal direction, whereas a negative value indicated buccal movement. The Y-axis represented a mesiodistal direction. While a positive value on the Y-axis indicated movement in the distal direction, a negative value indicated mesial movement. The Z-axis represented the occlusogingival direction. A positive value on the Z-axis indicated movement in the gingival direction and a negative value indicated occlusal movement.
System combination and interconnection of components
A nonlinear friction contact with a coefficient of µ = 0.2 was set at the aligner-tooth and aligner-attachment interfaces. The tooth-PDL, tooth-attachment, and cortical and trabecular bone-PDL contact areas were designated as bonded-type contact.
Results
Aligner deformation
The maximum deformation was observed on the palatal cusps of the second maxillary molar tooth occlusal surface in NA model, whereas the smallest deformation was observed on the buccogingival surface of the maxillary first molar in TOHA model (Table 3; Fig. 3). Among the models without torque, the highest degree of deformation was observed in the NA model (0.3388 mm), followed by the GHA (0.3381 mm), HA (0.3285 mm), and OHA (0.3253 mm) models. Among the models with torque, the maximum deformation occurred in TNA (0.2926 mm), followed by TGHA (0.2875 mm), THA (0.2772 mm), and TOHA (0.2721 mm).

Aligner deformation. (1) NA, (2) HA, (3) GHA, (4) OHA, (5) TNA, (6) THA, (7) TGHA, (8) TOHA
Stress distribution
The PDL stress distribution values and regions are presented in Table 4; Fig. 4. In all models, maximum stress values were observed at the palatal root of the maxillary second molar followed by the first molar. The NA model displayed the highest PDL stress distribution, whereas the TOHA model had the lowest.

Maximum principal stress distribution of PDL in eight models (MPa); (1) NA, (2) HA, (3) GHA, (4) OHA, (5) TNA, (6) THA, (7) TGHA, (8) TOHA. (A) Palatal view of upper first molar, (B) Palatal view of upper second molar
Tooth displacement
The first and second molar 3D displacements are illustrated in Fig. 5 along with the corresponding findings reported in Tables 5 and 6, respectively.

Displacements of upper first and second molar teeth in x (A), y (B), z (C) axes. (1) NA, (2) HA, (3) GHA, (4) OHA, (5) TNA, (6) THA, (7) TGHA, (8) TOHA
In the transverse (X-axis) dimension, the cusp points of the first and second molars were displaced in the buccal direction, and the apex points were displaced palatally. The models with the greatest buccal crown movement for the first and second molars respectively were NA (6CMB, 0.232 mm; 6CMP, 0.246 mm; 7CMB, 0.281 mm; 7CMP, 0.312 mm) and GHA (6CMB, 0.230; 6CMP, 0.245; 7CMB, 0.279 mm; 7CMP, 0.311 mm). In all groups, the degree of buccal tipping on the second molar was higher than on the first molar tooth.
In the anteroposterior (Y-axis) dimension, the first and second molars showed mesial tipping in all models. The highest mesial tipping for the first molar was observed in the NA (6CMB, 0.059 mm; 6CMP, 0.028 mm) and GHA (6CMB, 0.059; 6CMP, 0.027) models, respectively, while the least mesial crown movement was observed in the TOHA model (6CMB, 0.044 mm; 6CMP, 0.014 mm). The highest mesial tipping for the second molar was observed in the NA (7CMB, 0.058 mm; 7CMP, 0.031 mm), while the least mesial tipping was observed in the TOHA model (7CMB, 0.050 mm; 7CMP, 0.016 mm) (Tables 5 and 6; Fig. 5B).
In the vertical (Z-axis) dimension, all buccal cusp measurement points relocated gingivally, while the palatal cusp points were displaced occlusally in all groups. The greatest vertical movement of the first and second molars was observed in the NA and GHA models, while the least vertical movement was observed in the TOHA model. In all groups, the degree of vertical movements on the second molar was higher than on the first molar tooth (Tables 5 and 6; Fig. 5C).
Discussion
In recent years, there has been a notable interest in CAT which are perceived as an aesthetic and comfortable treatment option [1, 19]. With more adult patients seeking CAT, the scope of treatments provided with aligners have changed. Expansion of the dental arches by buccal tipping of posterior teeth can be achieved with CAT for mild-moderate discrepancies with moderate predictability [9, 20]. The efficacy of various movement types have significantly enhanced by the application of various attachment configurations [2]. To improve outcomes and reduce side effects during expansion with aligners, utilization of rectangular horizontal attachment and torque compensation were suggested [8, 10, 11]. The objective of this study was to evaluate the effect of different attachment configurations with or without compensatory buccal root torque on molar teeth during maxillary expansion with CAs using FEA.
Aligner deformation has a significant impact on the results of CA therapy [3, 6]. According to the results of our study, the highest degree of aligner deformation was on the palatal cusp of the second molar tooth, while the least was on the buccogingival surface of the first molar tooth, in direct proportion to the increasing PDL stress values. This finding is similar to Cortona et al. [6] This is also in line with the finding that the highest degree of crown tipping also took place at the second molar in the NA group. Nevertheless, the deformation was found to be less pronounced in the presence of the attachments, as observed in the study by Fan et al. [3].
Similar to the study by Gomez et al., [18] in which tooth movement was evaluated in models with and without attachments, this study also found more tipping in the model without attachments, due to the increase in tipping movement. Another model with the highest PDL stress is GHA, which may be related to the decrease in aligner thickness in the gingival area and the resulting decrease in movement predictability [21,22,23].
When the displacement of the teeth in the buccolingual (X-axis) direction was analysed, the models that displayed the greatest buccal tipping were the NA and GHA models, similar to Gomez et al. [18] The occlusally beveled horizontal attachment and torque compensation were identified to effectively control the buccal tipping. These findings emphasize the importance of attachment presence, configuration, and torque compensation in controlling tooth movement. In addition, the results of this study supported previous research findings that the use of occlusally beveled rectangular attachments reduced tipping by increasing the effective force transferred to the tooth surface and aligner retention [15, 21, 24].
In the mesiodistal direction (Y-axis), similar to the findings of Mao et al., [22] this study also observed a straightening tendency of the aligners, buccal movement, and mesial displacement of the molar teeth due to shortening and widening of the appliances with a more flattened dental arch curve. When the movement in the occlusogingival direction (Z-axis) was evaluated, due to tipping, there was gingival displacement of the buccal cusps while the palatal cusps moved occlusally. This was noted in all models after expansion [25]. In the no-attachment model, the greatest movement in the vertical direction also indicated a greater tendency for uncontrolled tipping [18]. The occlusally beveled attachment and torque compensation were found to reduce tipping movements [21]. In addition, similar to the findings of prior studies, the increase in movement inconsistencies from first molar to second molar observed in this study may be related to a decrease in aligner retention in the posterior region and an increase in the width and flexibility of the aligner-tooth gap [22, 26].
This study has several limitations. These effects and values reflect one timepoint and the differences between models are small and may be considered clinically insignificant. Accumulative effects of these with every aligner change is not tested. Additionally, only the molar teeth were evaluated and the effects of expansion on other teeth should be investigated in future studies. We also did not investigate the effect of initial torque value or different values of compensatory torque on the behavior of molars. Furthermore, as with any FEA study, this study did not evaluate the effects under in vivo conditions, aligner wear protocol, and associated factors related to masticatory function. Therefore, these results need to be further tested with clinical studies.
Conclusion
This FEA study showed that expansion with aligners results in buccal and mesial tipping of the maxillary molar teeth. The amount of buccal tipping exhibited an increase from the first to the second molars. The addition of occlusally beveled attachments and buccal torque compensation resulted in a significant decrease in the incidence of uncontrolled buccal tipping.
Data availability
The data will be available on reasonable request from the corresponding author.
References
Ke Y, Zhu Y, Zhu M. A comparison of treatment effectiveness between clear aligner and fixed appliance therapies. BMC Oral Health. 2019;19:1–10.
Costa R, Calheiros FC, Ballester RY, Gonçalves F. Effect of three different attachment designs in the extrusive forces generated by thermoplastic aligners in the maxillary central incisor. Dent Press J Orthod. 2020;25:46–53.
Fan D, Liu H, Yuan CY, Wang SY, Wang PL. Effectiveness of the attachment position in molar intrusion with clear aligners: a finite element study. BMC Oral Health. 2022;22:474.
Wang Q, Dai D, Wang J, Chen Y, Zhang C. Biomechanical analysis of effective mandibular en-masse retraction using class II elastics with a clear aligner: a finite element study. Prog Orthod. 2022;23:23.
Kawamura J, Ojima K, Nanda R. Effect of attachment type on distal bodily movement of the maxillary canine in aligner orthodontics: a finite element study. Angle Orthod. 2023;93:566–71.
Cortona A, Rossini G, Parrini S, Deregibus A, Castroflorio T. Clear aligner orthodontic therapy of rotated mandibular round-shaped teeth: a finite element study. Angle Orthod. 2020;90:247–54.
Laochahaiaroon P, Samruajbenjakun B, Chaichanasiri E. Initial displacement and stress distribution of upper central incisor extrusion with clear aligners and various shapes of composite attachments using the finite element method. Dent J. 2022;10:114.
Tai S. Clear aligner technique. 2018. 26p.
Zhou N, Guo J. Efficiency of upper arch expansion with the Invisalign system. Angle Orthod. 2020;90:23–30.
Zhang Y, Hui S, Gui L, Jin F. Effects of upper arch expansion using clear aligners on different stride and torque: a three-dimensional finite element analysis. BMC Oral Health. 2023;23(1):891.
Yao S, Jiang W, Wang C, He Y, Wang C, Huang L. Improvements of tooth movement efficiency and torque control in expanding the arch with clear aligners: a finite element analysis. Front Bioeng Biotechnol. 2023;11:1120535.
Rossini G, Schiaffino M, Parrini S, Sedran A, Deregibus A, Castroflorio T. Upper second molar distalization with clear aligners: a finite element study. Appl Sci. 2020;10:7739.
Savignano R, Valentino R, Razionale AV, Michelotti A, Barone S. D’anto V. Biomechanical effects of different auxiliary-aligner designs for the extrusion of an upper central incisor: a finite element analysis. J Healthc Eng. 2019;2019:9687127.
Dai FF, Xu TM, Shu G. Comparison of achieved and predicted tooth movement of maxillary first molars and central incisors: first premolar extraction treatment with Invisalign. Angle Orthod. 2019;89(5):679–87.
Dasy H, Dasy A, Asatrian G, Rózsa N, Lee HF, Kwak JH. Effects of variable attachment shapes and aligner material on aligner retention. Angle Orthod. 2015;85(6):934–40.
Cheng Y, Gao J, Fang S, Wang W, Ma Y, Jin Z. Torque movement of the upper anterior teeth using a clear aligner in cases of extraction: a finite element study. Prog Orthod. 2022;23:26.
Liu X, Cheng Y, Qin W, Fang S, Wang W, Ma Y, Jin Z. Effects of upper-molar distalization using clear aligners in combination with class II elastics: a three-dimensional finite element analysis. BMC Oral Health. 2022;22:546.
Gomez JP, Peña FM, Martínez V, Giraldo DC, Cardona CI. Initial force systems during bodily tooth movement with plastic aligners and composite attachments: a three-dimensional finite element analysis. Angle Orthod. 2015;85:454–60.
Elkholy F, Mikhaiel B, Repky S, Schmidt F, Lapatki BG. Effect of different attachment geometries on the mechanical load exerted by PET – G aligners during derotation of mandibular canines: an in vitro study. J Orofac Orthop. 2019;80:315–26.
Boyd RL. Esthetic orthodontic treatment using the invisalign appliance for moderate to complex malocclusions. J Dent Educ. 2008;72:948–67.
Jones ML, Mah J, O’Toole BJ. Retention of thermoformed aligners with attachments of various shapes and positions. J Clin Orthod. 2009;43:113–7.
Mao B, Tian Y, Li J, Zhou Y. Expansion rebound deformation of clear aligners and its biomechanical influence: a three-dimensional morphologic analysis and finite element analysis study. Angle Orthod. 2023;93:572–9.
Palone M, Longo M, Arveda N, et al. Micro-computed tomography evaluation of general trends in aligner thickness and gap width after thermoforming procedures involving six commercial clear aligners: an in vitro study. Korean J Orthod. 2021;51:135–41.
Groody JT, Lindauer SJ, Kravitz ND, Carrico CK, Madurantakam P, Shroff B, Darkazanli M, Gardner WG. Effect of clear aligner attachment design on extrusion of maxillary lateral incisors: a multicenter, single-blind randomized clinical trial. Am J Orthod Dentofac Orthop. 2023;164(5):618–27.
Camcı H, Salmanpour F. Effect of sinus proximity, alveolar bone level, and initial buccolingual inclination on behavior of maxillary first molar under expansion force: a finite element analysis. J World Fed Orthod. 2022;11:60–7.
Edelman A, English JD, Chen SJ, Kasper FK. Analysis of the thickness of 3-dimensional-printed orthodontic aligners. Am J Orthod Dentofac Orthop. 2020;158:91–8.
Acknowledgements
We acknowledge Orthero Aligner Company and Tinus Technology for technical support and analysis assistance.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
NK and MA wrote the main manuscript, designed the research.IO prepared the figures.HG: Checked the main manuscript.OD: Designed the research.All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Karslı, N., Ocak, I., Akyıldız, M. et al. Evaluation of the effect of different attachment configurations on molar teeth in maxillary expansion with clear aligners – a finite element analysis. BMC Oral Health 24, 921 (2024). https://doi.org/10.1186/s12903-024-04544-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-024-04544-8