
Abstract
Background
Dental caries are common and troublesome and may affect individuals’ health conditions. It is crucial to comprehend the caries experience for prevention, management, and enhancing oral health. Techniques such as CAMBRA can help assess an individual’s risk factors for caries lesions. This study aims to assess the caries risk in five distinct regions of Saudi Arabia, utilizing the CAMBRA methodology.
Methods
This multiregional cross-sectional study was conducted at university dental clinics across the five regions of Saudi Arabia, using a Caries Management by Risk Assessment (CAMBRA) tool. This study used binary logistic regression analysis, the Pearson Chi-square test, and descriptive analysis as statistical methods.
Results
A total of 551 respondents participated in the study, with 59.7% being male and 40.3% being female. The age group with the highest proportion was 20–29, making up 31.6% of the participants. All participants exhibited at least one caries lesion (100%), with white spots (66.4%) and enamel lesions (56.1%) being the most prevalent. The moderate-risk category encompassed the largest proportion of participants, accounting for 60% of the total. High caries risk had a significant association with age group (P < 0.001), education (P < 0.001), profession (P < 0.001), and socio-economic status (P < 0.001). Furthermore, only age and socio-economic status showed a significant relationship with high caries risk in the multiple logistic regression.
Conclusion
The CAMBRA tool indicates a high prevalence of moderate risk across the five regions of Saudi Arabia, identifying age and socio-economic status as significant predictors of caries risk.
Similar content being viewed by others

Introduction
Dental caries poses a significant public health challenge due to its widespread prevalence, pain-inducing nature, high treatment costs, and potential to disrupt nutrition [1,2,3]. Dental caries harms about 100% of adults and between 60% and 80% of children worldwide, based on a 2012 oral health survey by the World Health Organization [4]. The multifaceted nature of dental caries, involving factors such as bacteria, nutrition, and host response, makes it a global concern despite ongoing advancements in scientific understanding [5, 6]. Addressing dental caries requires a comprehensive preventive approach, including the identification and evaluation of individuals susceptible to future caries using various assessment tools and models [5]. Several studies investigating the prevalence of dental caries have been conducted in the Kingdom of Saudi Arabia (KSA), revealing consistently high rates of caries in both adults and children [7]. Some of these studies, including systematic reviews have provided insights into the extent of caries over specific periods [8]. For instance, dental cavities affect 70% of children in permanent dentition and 80% of elementary school pupils in primary dentition [8]. Another study found that dental caries was common in the permanent dentition, with a mean DMFT of 3.34 in the primary dentition and 5.38 in the permanent dentition [9]. Similarly, Al-Ansari [10] reported mean DMFT values of 7.35 in adult permanent dentition and 7.34 in primary dentition. Studies across various regions of Saudi Arabia have demonstrated differing levels of dental caries prevalence [11,12,13]. However, a recent systematic review highlighted wide-ranging prevalence measures, extending from 21 to 100% in primary teeth as well as from 5 to 99% in permanent teeth [7]. Dental caries results from a variety of factors, encompassing oral microbiota, salivary production, and composition, as well as lifestyle factors like dietary habits, tooth brushing, and the use of fluoride-containing toothpaste [14,15,16,17,18]. Consequently, tailoring dental care plans to everyone’s specific risk factors is essential. To achieve this, many dental professionals advocate for the implementation of the evidence-based Caries Management by Risk Assessment (CAMBRA) technique used to evaluate and manage caries risk in children and adults [18]. People as young as six years old have their current risk of caries assessed using CAMBRA based on disease signs, risk factors, and protective factors [19]. CAMBRA has not been used as much as it may be to assess caries risk in Saudi Arabian citizens [6]. Therefore, the purpose of this study was to evaluate caries risk in five different regions of Saudi Arabian using the CAMBRA.
Methods
Design of study
This study used a cross-sectional survey technique, carried out within the university dental clinics affiliated with the dental colleges across five different regions of Saudi Arabia. The study utilized a CAMBRA tool [20]. Prior to obtaining formal informed consent, the research team ensured the voluntary participation of all participants and briefed them about the study’s purpose before obtaining written informed consent. For minors, we obtained informed consent from their parent or guardian. After completing survey forms, participants had an intra-oral examination and a bitewing radiography to determine how clean their teeth were and to look for any indications of caries.
Data collection
Participants were recruited from outpatient departments of university dental clinics in five regions, together with their partners (e.g., siblings, family members, or friends). Participants had to be at least six years old, fluent in both English and Arabic, and live in Saudi Arabia. A stratified simple random sampling technique, proportional to the population size, was employed to select participants from the five regions (i.e., north, west, south, east, and centre). The study was conducted from March 15, 2023, to December 15, 2023. The Ethical approval was taken from the Institutional Scientific Research and Bioethical Committee.
Study instrument
The study questionnaire consisted of a socio-demographic section and a CAMBRA caries risk assessment section. The sociodemographic section includes gender, age group, occupation, place of residence, region, educational level, and socio-economic status. The CAMBRA section includes four disease indicators (i.e., visible cavities or radiographic penetration of the dentin, radiographic approximal enamel lesions, white spots on smooth surfaces, restorations in the last three years), eight protective factors, and eight risk factors [20]. Additionally, this tool was tested and utilized among the Saudi Arabian population in a prior study [6].
Estimation of sample size
Based on the single proportion formula [21], we calculated the sample size and arrived at an initial estimate of 384 samples. This calculation was based on a presumed proportion (p) of 0.5, chosen to account for the highest possible variance and sample size [21], as no prior studies had been conducted across regions in Saudi Arabia. Furthermore, a significance level (z) of 1.96 and a margin of error (E) of 0.05 were used. After factoring in a 40% dropout rate to accommodate potential missing data and wrong data entry, the adjusted sample size was determined to be 640.
Data analysis
Initially, we conducted data cleaning to rectify missing values and erroneous data entries. Using Statistical Product and Service Solution (SPSS) version 27, the statistical analyses used in this study included binary logistic regression analysis, the Pearson Chi-square test, and descriptive analysis. Frequencies and percentages were presented using descriptive analysis. The relationship between sociodemographic traits and caries risk was examined using the Pearson Chi-square test. In order to determine the important variables connected to high-risk caries, we performed a binary logistic regression analysis. To find the crude odds ratio (COR) of predictors, basic logistic regression was used in the first stage of the logistic regression process. In order to calculate their adjusted odds ratio (AOR), factors with p-values less than 0.25 were deemed important and added to the multiple logistic regression analysis. The multiple logistic regression used both forward LR and backward LR approaches, and the entry method was used to execute the final model. Using analyses of variable interactions, Hosmer and Lemeshow tests, classification accuracy, and the area under the receiver operating characteristic curve (AUC), the final model’s suitability was evaluated.
Results
Table 1 presents the socio-demographic characteristics of the study respondents. A total of 551 respondents participated in the study, consisting of males (59.7%) and females (40.3%). Those aged 20–29 had the highest proportion (31.6%). The majority of the respondents were from urban areas (67.5%). The highest proportion of the participants were from the northern region (26.5%) and possessed a bachelor’s degree (29.9%). Furthermore, about half of the participants were of lower middle class (40.8%).
Table 2 illustrates the distribution of study participants based on disease indicators, risk factors, and protective factors. All participants exhibited at least one disease indicator (100%), with white spots (66.4%) and enamel lesions (56.1%) being the most prevalent. Among the identified risk factors, frequent snacks (62.1%) were the most commonly observed, followed by visible heavy plaque on teeth (56.1%). As for protective factors, fluoridated communities (61.0%) ranked highest, followed closely by fluoride toothpaste (60.6%).
Figure 1 shows that the ‘moderate’ risk category encompassed the largest proportion of participants, accounting for 60% of the total, whereas only 4% fell into the ‘extremely’ high-risk category of caries risk assessment.

Caries assessment
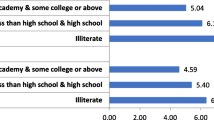
Table 3 presents the association between socio-demographic characteristics and caries risk. The results indicate that caries risk categories had a significant association with age group (P < 0.001), education (P < 0.001), profession (P < 0.001), and socio-economic status (P < 0.001). In terms of age, the prevalence of high risk was higher in individuals over 60 years old (71.4%) compared to the other age groups. Those with a PhD (100%) had a higher frequency of intermediate risk than the other groups. Among the professions, mechanics had the highest prevalence of extremely high risk (20%) when compared to other professions. In terms of socioeconomic position, the lower class had a higher prevalence of extremely high risk (8.1%), followed by the lower middle class (5.3%).
Table 4 presents the factors associated with high-risk caries using simple and multiple logistic regression analyses. In the multiple logistic regression analysis, only age and socio-economic status demonstrated a significant association with high caries risk. In terms of age groups, the 20–29-year-olds were 1.8 times more likely than the 6–19-year-olds to have a high caries risk (AOR = 1.82, P = 0.144). The 30-39-year-olds were 3 times more likely to have high-risk caries compared to the 6-19-year-olds (AOR = 3.04, P = 0.006); the 40–49 were 9.6 times more likely to have high-risk caries compared to the 6-19-year-olds (AOR = 9.59, P < 0.001); the 50-59-year-olds were 8.6 times more likely to have high-risk caries compared to the 6-19-year-olds (AOR = 8.56, P < 0.001); and those in the 60 + years were 34 times more likely to have high-risk caries compared to the 6-19-year-olds (AOR = 34.04, P < 0.001). In terms of socioeconomic status, those in lower middle status were 2.4 times less likely to have high-risk caries compared to those with lower status (AOR = 0.42, P = 0.006), those in middle status were 2.9 times less likely to have high-risk caries compared to those with lower status (AOR = 0.34, P = 0.001), and those in upper status were 4.5 times less likely to have high-risk caries compared to those with lower status (AOR = 0.22, P < 0.001).
Discussion
This study evaluated the caries risk across five regions of Saudi Arabia using CAMBRA tool. The study’s findings revealed that every participant (100%) exhibited at least one indication of caries, with 56.1% displaying clinically or radiographically confirmed dentin or enamel lesions. Additionally, 31.9% of individuals had undergone restorative treatment within the past three years. Consistent with prior research [6, 22,23,24,25], our study corroborates that visible cavities and white spot lesions constitute most lesions. The primary risk factors identified were plaque accumulation (56.1%) and frequent consumption of sugary foods (62.1%). Conversely, factors such as recreational drug use, orthodontic appliances, reduced salivary flow, exposed roots, and saliva-reducing conditions were less prevalent. These results align with earlier studies [6, 19, 22, 25], indicating a similar distribution of risk factors.
In this study, most participants (61.0%) reported fluoridated toothpaste as the primary protective factor, with over half (60.6%) indicating regular daily brushing. Less than half of the participants utilized calcium and phosphate paste, xylitol, fluoride varnish, or mouthwash. These findings align with previous research suggesting an increase in the high-risk caries group regardless of topical treatments or water fluoridation [6, 26]. Furthermore, clinical research by Featherstone et al. [27] demonstrated a significant reduction in caries with fluoride therapy and targeted antibacterial treatments.
The majority of participants in this study were classified as having a moderate risk of caries (60%), followed by those in the high caries risk category (23%). These results are consistent with prior studies [28, 29], although some studies have reported a higher prevalence of the high-risk group [23, 30, 31]. The recruitment of participants from a dental department, where individuals typically seek dental treatment, may explain the higher prevalence of caries risk in the present study. In this study, the prevalence of moderate risk was slightly higher among females (62.2%), the 20–29 years (70.1%), those residing in the western region (70.7%), individuals with a PhD (100%), and engineers (100%). These findings closely resemble those of studies by Iqbal et al., [6], where a higher prevalence of moderate risk was observed among females (16.7%). While no significant association between regions and caries risk was found in the present study, a notably higher prevalence of extremely high risk was observed in the northern region (7.5%). This observation is noteworthy, as previous studies have not extensively explored regional variations in CAMBRA.
Moreover, the results of this study suggest that age and socio-economic status are independently associated with a high risk of caries. Advanced age and lower socio-economic status were associated with an increased likelihood of high-risk caries. Age-related changes in oral hygiene habits, prolonged consumption of sugary foods and drinks, and possible reductions in saliva production—which naturally coats teeth—all contribute to an increased risk of dental problems [12, 32, 33]. In terms of socioeconomic position, people in lower socioeconomic brackets could have less access to preventive treatments, dental care, and information about good oral hygiene habits [34,35,36]. Additionally, because of factors like restricted access to healthy options or food instability, they can be more inclined to consume sugary foods and beverages [37].
A precise assessment of dental caries risk can enhance patient counselling and treatment plans. A proper risk analysis requires the use of patient-centric, easily understandable tools, like CAMBRA. With the aid of these tools, indicators of risk can be found, and then a customized treatment plan can be created for each patient. CAMBRA can improve a patient’s relationship with the dentist by involving them in the process of decision-making. Among the study’s shortcomings was its design. Including patients from the dental department may have influenced the study’s conclusions because the majority of participants were at higher risk and there was no control group to compare the results with. On the other hand, the results may have additional value because the study was carried out in all five regions of Saudi Arabia. Additionally, the research employed a self-report measure, which can introduce bias into the responses.
Conclusion
This study conducted a multi-regional survey utilizing the Caries Management by Risk Assessment (CAMBRA) to evaluate risk of caries among population of five regions of Saudi Arabia. The study findings reveal that age and socio-economic status are associated with a high risk of caries. We recommend future studies calibrate CAMBRA as a caries prediction tool or determine whether using it actually has a caries-controlling effect.
Data availability
The datasets generated and/or analyzed during the current studyare available from the corresponding author on reasonable request.
Abbreviations
- CAMBRA:
-
Caries Management By Risk Assessment
References
Gilchrist F, Marshman Z, Deery C, Rodd HD. The impact of dental caries on children and young people: what they have to say? Int J Pediatr Dent. 2015;25(5):327–38.
Martins LGT, Pereir KCR, Costa SXS, Traebert E, Lunardelli SE, Lunardelli AN et al. Impact of dental caries on quality of life of school children. Pesquisa Brasileira em Odontopediatria E Clínica Integrada. 2016;16(1).
Martins MT, Sardenberg F, Bendo CB, Abreu MH, Vale MP, Paiva SM, et al. Dental caries remains as the main oral condition with the greatest impact on children’s quality of life. PLoS ONE. 2017;12(10):e0185365.
Petersen PE. World Health Organization global policy for improvement of oral health-World Health Assembly 2007. Int Dent J. 2008;58(3):115–21.
Suneja ES, Suneja B, Tandon B, Philip NI. An overview of caries risk assessment: Rationale, risk indicators, risk assessment methods, and risk-based caries management protocols. Indian J Dent Sci. 2017;9(3):210–4.
Iqbal A, Khattak O, Chaudhary FA, Onazi MAA, Algarni HA, AlSharari T, et al. Caries risk assessment using the caries management by risk assessment (CAMBRA) protocol among the general population of Sakaka, Saudi Arabia—A cross-sectional study. Int J Environ Res Public Health. 2022;19(3):1215.
Alshammari FR, Alamri H, Aljohani M, Sabbah W, O’Malley L, Glenny A-M. Dental caries in Saudi Arabia: a systematic review. J Taibah Univ Med Sci. 2021;16(5):643–56.
Al Agili DE. A systematic review of population-based dental caries studies among children in Saudi Arabia. Saudi Dent J. 2013;25(1):3–11.
Khan SQ, Khan NB, ArRejaie AS. Dental caries. A meta analysis on a Saudi population. Saudi Med J. 2013;34:744–9.
Al-Ansari AA. Prevalence, severity, and secular trends of dental caries among various Saudi populations: a literature review. Saudi J Med Med Sci. 2014;2(3):142–50.
Alhabdan YA, Albeshr AG, Yenugadhati N, Jradi H. Prevalence of dental caries and associated factors among primary school children: a population-based cross-sectional study in Riyadh, Saudi Arabia. Environ Health Prev Med. 2018;23:1–14.
Alkarimi HA, Watt RG, Pikhart H, Sheiham A, Tsakos G. Dental caries and growth in school-age children. Pediatrics. 2014;133(3):e616–23.
Amin T, Al-Abad B. Oral hygiene practices, dental knowledge, dietary habits and their relation to caries among male primary school children in Al Hassa, Saudi Arabia. Int J Dental Hygiene. 2008;6(4):361–70.
Fejerskov O, Larsen MJ, Richards A, Baelum V. Dental tissue effects of fluoride. Adv Dent Res. 1994;8(1):15–31.
Gibson S, Williams S. Dental Caries in pre–school children: associations with Social Class, Toothbrushing habit and consumption of sugars and Sugar–Containing foods: further analysis of data from the National Diet and Nutrition Survey of children aged 1.5–4.5 years. Caries Res. 1999;33(2):101–13.
Leone CW, Oppenheim FG. Physical and chemical aspects of saliva as indicators of risk for dental caries in humans. J Dent Educ. 2001;65(10):1054–62.
Marsh PD. Microbiology of dental plaque biofilms and their role in oral health and caries. Dent Clin. 2010;54(3):441–54.
Kim J-M, Choi J-S, Choi Y-H, Kim H-E. Simplified prediction model for accurate assessment of dental caries risk among participants aged 10–18 years. Tohoku J Exp Med. 2018;246(2):81–6.
Chaffee BW, Cheng J, Featherstone JD. Non-operative anti-caries agents and dental caries increment among adults at high caries risk: a retrospective cohort study. BMC Oral Health. 2015;15:1–8.
Featherstone JD, Domejean-Orliaguet S, Jenson L, Wolff M, Young DA. Caries risk assessment in practice for age 6 through adult. J Calif Dent Assoc. 2007;35(10):703–13.
Taherdoost H. Determining sample size; how to calculate survey sample size. Int J Econ Manage Syst. 2017;2.
Almusawi M, Gosadi I, Abidia R, Almasawi M, Khan H. Potential risk factors for dental caries in type 2 diabetic patients. Int J Dental Hygiene. 2018;16(4):467–75.
MU M. Caries Risk Assessment and its Association with Socio-demographic factors among General Population of Lahore. Pakistan Biomed. 2019;35(3).
Khallaf YS, Hafez S, Shaalan OO. Evaluation of ICCMS versus CAMBRA caries risk assessment models acquisition on treatment plan in young adult population: a randomized clinical trial. Clin Cosmet Invest Dentistry. 2021:293–304.
Farsi N, Merdad L, Mirdad S. Caries risk assessment in preschool children in Saudi Arabia. Oral Health Prev Dent. 2013;11(3):271–80.
Featherstone J, Chaffee B. The evidence for caries management by risk assessment (CAMBRA®). Adv Dent Res. 2018;29(1):9–14.
Featherstone J, White J, Hoover C, Rapozo-Hilo M, Weintraub J, Wilson R, et al. A randomized clinical trial of anticaries therapies targeted according to risk assessment (caries management by risk assessment). Caries Res. 2012;46(2):118–29.
da Silva Jorge VC, Câmara JVF, da Silveira Pereira GD, Barbosa IF, de Carvalho Vianna RF, de Campos PRB, et al. Evaluation of caries risk in pre-school children using the CAMBRA protocol and CAST index. Brazilian J Dev. 2021;7(3):26944–54.
Muhson ZN, Thabit S, Al-ward FS, Al Shatari SA. Caries risk assessment of a sample of children attending preventive specialized dental center in Al Resafa, Baghdad. J Baghdad Coll Dentistry. 2020;32(4):17–24.
Sudhir KM, Kanupuru KK, Fareed N, Mahesh P, Vandana K, Chaitra NT. CAMBRA as a Tool for Caries Risk Prediction among 12-to 13-year-old Institutionalised Children-A Longitudinal follow-up study. Oral Health Prev Dent. 2016;14(4).
Rechmann P, Chaffee B, Rechmann B, Featherstone J. Changes in caries risk in a practice-based randomized controlled trial. Adv Dent Res. 2018;29(1):15–23.
Abbass MM, Mahmoud SA, El Moshy S, Rady D, AbuBakr N, Radwan IA et al. The prevalence of dental caries among Egyptian children and adolescences and its association with age, socioeconomic status, dietary habits and other risk factors. A cross-sectional study. F1000Research. 2019;8.
López R, Smith PC, Göstemeyer G, Schwendicke F. Ageing, dental caries and periodontal diseases. J Clin Periodontol. 2017;44:S145–52.
Kamate WI, Vibhute N, Baad R, Belgaumi U, Kadashetti V, Bommanavar S. Effect of socioeconomic status on dental caries during pregnancy. J Family Med Prim care. 2019;8(6):1976–80.
Ghasemianpour M, Bakhshandeh S, Shirvani A, Emadi N, Samadzadeh H, Moosavi Fatemi N, et al. Dental caries experience and socio-economic status among Iranian children: a multilevel analysis. BMC Public Health. 2019;19:1–8.
Naskova S, Iljovska S, Pavlevska M, Alimani-Jakupi J. Socio economic and nutritional status as dental caries risk factors in 12 year old children. IOSR J Dent Med Sci (IOSR-JDMS). 2016;15(14 (V)):106–14.
Srivastava P. To assess the Prevalence of Dental Caries and its association with body Mass Index, Socioeconomic Status, Dietary habits, and oral Hygiene among 6–12-year-old children in Faridabad. Int J Clin Pediatr Dentistry. 2023;16(4):626–32.
Acknowledgements
This research is funded by the Deanship of Graduate Studies and Scientific Research at Jouf University through the FastTrack Research Funding program.
Funding
The authors received no funding for this project.
Author information
Authors and Affiliations
Contributions
Conceptualization: MAO. Methodology AI, HAA. Investigation and analysis: MNSA. Writing-Original draft preparation: AI, MAO. Editing, Reviewing: SA, OK. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by Local Ethics Committee of Bioethics for Research at college of dentistry, Jouf University with the reference No 09-06-43.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Alonazi, M.A., Algarni, H.A., Alqarni, M.N.S. et al. Unmasking caries risk: a multi-regional study in Saudi Arabia. BMC Oral Health 24, 874 (2024). https://doi.org/10.1186/s12903-024-04665-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-024-04665-0