
Abstract
Introduction
Earlier studies reported inconsistent findings for the association of childhood obesity with the risk of dental caries. In this systematic review and meta-analysis, we aimed to summarize earlier studies on the association of overweight and obesity with risk of dental caries in children.
Methods
Relevant studies published up to December 2023 were identified through searches in PubMed, MEDLINE, SCOPUS, EMBASE, and Google Scholar, using suitable keywords. All observational studies, including cross-sectional or cohort or case-control studies, about the association of each obesity index with risk of dental caries in children which reported odds ratio (OR), hazard ratio (HR), or relative risk (RR) and 95% CIs, were included. Studies involving adults, randomized clinical trials, studies on animals or pregnant women, and studies on other dental disorders were excluded. Risk of bias was assessed using standard methods for observational studies. A total of 22 studies including 40673 participants were included. Studies were pooled using the random-effect model, and results were synthesized with subgroup analyses and assessments of heterogeneity. Limitations included potential publication bias and heterogeneity among study designs. The quality of the included studies was assessed using the Newcastle–Ottawa scale (NOS).
Results
Children at the highest category of BMI were 44% more likely to have early childhood caries (ECC) than those at the bottom (OR: 1.44; 95% CI: 1.16 to 1.78). Moreover, combined analysis also showed no significant association between waist circumference (WC) and risk of dental caries in children. However, significant linear and non-linear associations were found between BMI and risk of childhood dental caries. No publication bias was found for the relationship between BMI and the risk of ECC based on visual inspection of a funnel plot and Egger's test.
Conclusions
This study showed a significant direct association between BMI and the risk of dental caries in children. Non-linear analysis showed higher risk of dental caries in children with higher BMI and also among underweight children. Further prospective studies are required to expand current knowledge in this issue.
Impact statement
The findings of this study have significant implications for public health and dental care, suggesting association between BMI and the risk of dental caries in children. This comprehensive meta-analysis is among the first to summarize earlier publications on the association of obesity with risk of dental caries in children, highlighting the need for more accurate methods of obesity assessment and further research to understand this relationship better. These findings can help inform public health policies and interventions to reduce the prevalence of childhood obesity and dental caries.
Similar content being viewed by others


Introduction
Obesity is a chronic disease characterized by excess or abnormal accumulation of fat in the body that might disturb a person’s health [1]. In 2016, it was reported that 1.9 billion adults 18 years old or above were overweight, of which over 600 million were obese [2]. The prevalence of obesity in children and adolescents is quickly increasing, such that more than 340 million children and adolescents aged between 5 to 19 are suffering from overweight or obese, worldwide [2].
Childhood obesity is linked with different chronic diseases, such as cardiovascular disease, certain types of cancers, type 2 diabetes, coronary heart disease, or hypertension in adulthood [3, 4]. Besides, it is positively linked to the development of various physical disabilities and diverse psychological problems [5]. Accordingly, obesity is considered as a critical threat to health‑care systems and imposes a substantial burden on countries [6].
Dental caries (known as tooth decay or dental cavity) is accounted as the most prevalent non-communicable diseases worldwide, often causing pain and infection, resulting in tooth extraction and altered quality of life [7, 8]. It has been estimated that near 5-10% of the health care annual budget in the developed countries is spent for the treatment of dental caries [9]. In addition, dental caries can threaten children's development and growth, especially those on a poor diet [10]. The association between obesity and dental caries might be related to low-socioeconomic status, high-sugar diet, low use of health services, and limited health literacy. These shared risk factors leads to higher prevalence of both conditions [11]. Many studies have examined association between obesity and dental caries in different locations; however, their findings are controversial. Several studies reached no remarkable association [12], while others found a positive or an inverse association between obesity and dental caries [13,14,15,16]. Earlier systematic reviews and meta-analyses also reported controversial findings [11, 14, 17, 18]. In addition, A recent meta-analysis suggested that obesity increases the risk of caries in older children, while it was equivocal in younger children [19], which highlights needs for a comprehensive analysis in this area. Those meta-analyses have substantial limitations, including focusing only on cross-sectional studies [11, 20, 21], lack of examination for the association in children under six years [11, 17, 21], and the majority of them had an incomplete search strategy in a small number of databases [11, 17, 19,20,21]. Furthermore, they did not separately analyze continuous and categorical effect sizes to reach a firm conclusion. Lack of different subgroup analyses is another limitation of those studies.
Given the aforementioned reasons and to address the knowledge gaps, current systematic review and meta-analysis was done to examine association between obesity indices and risk of dental caries in children.
Methods
This research was carried out in line with the PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines.
Search strategy
Relevant studies published up to December 2023 were searched through PubMed, MEDLINE, SCOPUS, EMBASE, and Google Scholar, using the following suitable MESH and non-MESH keywords: (("early childhood caries"[tiab] OR "Dental Care for Children"[tiab] OR "tooth decay"[tiab] OR "pediatric dentistry"[tiab] OR “dentistry”[tiab] OR “dental”[tiab] OR “teeth”[tiab] OR “tooth”[tiab] OR “caries”[tiab] OR "dental caries"[tiab] OR "Dental Decay"[tiab] OR “Teeth decay”[tiab]) AND (“child”[tiab] OR “kid”[tiab] OR “childhood”[tiab] OR “pediatric”[tiab] OR “paediatric”[tiab] OR "preschool children"[tiab]) AND (“weight”[tiab] OR "body mass index"[tiab] OR “BMI”[tiab] OR “waist circumference”[tiab] OR obesity[tiab] OR "overweight"[tiab] OR "Birth weight"[tiab])). No restrictions were done in terms of language or time of publication. Duplicate citations were removed. To avoid missing any publication, we also reviewed reference lists of all included studies and relevant review articles.
Inclusion criteria
All observational studies, including cross-sectional or cohort or case-control studies, that investigated the association of each obesity index with risk of dental caries in children. Eligible studies were required to report odds ratio (OR), hazard ratio (HR), or relative risk (RR) and 95% CIs, were included. In case of several publications with the same data set, we included only the most complete one. If data for specific subgroups were reported, results for the whole population were used. Studies on adults, randomized clinical trials, animal studies, those enrolled pregnant women, and studies assessed risk of other dental disorders in relation to obesity were not included in our systematic review and meta-analysis. We did not also include unpublished data and grey literatures, including dissertations, congress abstracts, and patents in the current meta-analysis.
Data extraction
Following data were extracted by two independent reviewers: first author’s name, publication year, location, study sample size, number of subjects in each group, participants’ age, participants' gender, study design, exposure, exposure assessment method, outcomes, outcome assessment methods, and any confounder adjusted for.
Statistical analysis
All statistical analyses were performed using STATA software version 14.0 (Stata Corp LP, College Station, TX). Statistical significance was set at p < 0.05. We focused on studies that reported odds ratios (ORs) for all-cause or early childhood caries across different BMI categories. A dose-response meta-analysis, following the method developed by Greenland and Longnecker [22] and further refined by Orsini et al. [23], was used to assess the trend from correlated log OR estimates across BMI categories. For each BMI category, the midpoint was considered the corresponding OR estimate. Open-ended categories were assumed to be of equal width to the adjacent categories.
A two-stage random-effects dose–response meta-analysis was employed to explore a potential non-linear relationship between BMI and early childhood caries risk. This involved modeling BMI with restricted cubic splines, with knots placed at the 10th, 50th, and 90th percentiles of the distribution, as described by Harrell et al. [24]. Using a generalized least-squares regression, we accounted for the correlation within each set of published ORs, combining the study-specific estimates with the restricted maximum likelihood method in a multivariate random-effects meta-analysis. The non-linearity probability was assessed by testing the null hypothesis that the coefficient of the second spline was zero.
For a linear dose-response relationship, we evaluated the impact of 1 kg/m2 increments in early caries on childhood using generalized least-squares trend estimation. We calculated pooled ORs and standard errors from all reported effect sizes and their 95% confidence intervals (CIs) using a random-effects model. Additionally, we applied a multivariate linear regression model to investigate the association between obesity indices and childhood dental caries risk, adjusting for potential confounders such as age, gender, socioeconomic status, and dietary habits.
Between-study heterogeneity was examined using the Cochrane Q test and I2 statistics, with I2 values over 50% indicating substantial heterogeneity. To identify sources of heterogeneity, we conducted subgroup analyses based on country population size (large vs. small), region (Asian vs. European vs. American countries), participants' age (≤7 years vs. >7 years), sample size (≤900 vs. >900), study design (cross-sectional, case-control, or cohort), and adjustments for age and gender. To assess publication bias, both the funnel plot and Egger's regression test were employed.
Quality assessment
The Newcastle Ottawa Scale (NOS), which is tailored for observational studies, was employed to evaluate the quality of the selected cohort, case-control and cross-sectional studies [25]. The NOS assigns up to ten points to each study: five for selection, two for comparability, and three for outcome assessment, with ten representing the highest quality. Any disagreements were resolved through discussion. In this study, publications scoring 5 or higher on the NOS were deemed high-quality (Supplementary Table 2).
PECO Framework
The study focused on the association between obesity indices (exposure), such as BMI and waist circumference, and the risk of dental caries (outcome) in children (population). Although the specific formulation of the PECO question was not explicitly stated, the study implicitly addressed these components to guide its research focus and parameters. Additionally, the comparator used was different levels of BMI (e.g., normal weight, overweight, obese). Detailed information on the PECO framework can be found in Supplementary Table 1.
Results
Systematic review
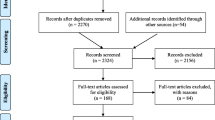
Flow-diagram of study selection has been shown in Fig. 1. Overall, 22 studies including 40673 participants were judged to be eligible for the current systematic review. Of these, 16 studies were included in the meta-analysis. Characteristics of these studies are summarized in Table 1. Included studies were published between 2007 and 2023; such that 8 studies were published before 2015 [12,13,14,15, 26,27,28,29] and 14 studies were published after that year [16, 30,31,32,33,34,35,36,37,38,39,40,41,42]. Included studies were done in Finland [30, 39], Brazil [26, 27, 37] , Sweden [32], Mexico [15], Germany[31, 35], Vietnam [16], China [29], UK [28, 34], India [13], Nepal [33], New Zealand [36], Belgium [38], Saudi Arabia [40], Tiwan [42] and USA [12, 14, 41]. They had case–control [30, 35, 38, 43], cross-sectional [13, 14, 16, 26, 27, 29, 31, 33, 34, 36, 40, 42, 44], or prospective cohort design [12, 15, 28, 32, 35, 37, 39, 41]. The sample size of these studies varied between 71 and 27333 and could be classified into two subgroups of less than 900 [13, 14, 26, 27, 29,30,31,32, 34, 35, 37,38,39, 42] and more thanf 900 [12, 15, 16, 28, 33, 36, 40, 41]. Moreover, study sample size was not reported in one of included papers [28]. The mean age of children in the included studies varied from 4 to 18 years. Fourteen studies were done on children aged <7 years [12, 14, 15, 27,28,29, 31, 32, 34,35,36,37, 40, 41], while 8 studies enrolled children between 7 and 15 years [13, 16, 26, 30, 33, 38, 39, 42]. All included studies were done on both genders.

Flow diagram of study selection
The measured exposures were BMI as a continuous [28, 29, 31, 34] or categorical [12,13,14,15,16, 26,27,28, 30, 32, 33, 36,37,38,39,40,41,42] variable and WC categories [29, 34]. Exposure assessment method was not reported in some studies [31], while the others directly measured participants’ weight and height to calculate BMI [12,13,14,15,16, 26,27,28,29,30, 32,33,34,35,36,37,38,39,40,41,42]. The outcome of interest was dental caries in most studies [12,13,14,15,16, 26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42]. Some other studies also reported odds ratio for erosive tooth wear [30, 31]. Assessment of outcomes was done by an experienced dentist in most included studies [12,13,14,15,16, 26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42]. In some studies findings were adjusted for participants’ gender [16, 26, 29, 30, 33, 36, 38,39,40,41,42]. In addition, some other studies adjusted their findings for the participants’ age [28, 30, 33, 37, 38, 41, 42]. Furthermore, a considerable number of included studies did not report any adjustment [13, 27, 31, 32, 34].
Meta-analysis
Combining data from 16 studies, we found a significant direct association between BMI and risk of ECC; such that those at the highest category of BMI had 44% higher risk of dental caries than those at the bottom category (OR: 1.44; 95% CI: 1.16 to 1.78, I2= 88.9 %) (Fig. 2). In our study, the subgroup analysis presented in Table 2 included articles that utilized consistent standards for defining both obesity and dental caries. When we did subgroup analysis by the predefined variables, the association significant relationship was found between BMI and risk of ECC among studies done in Asian countries (OR: 1.70; 95% CI: 1.25, 2.32), also among studies with cohort design (OR: 1.27; 95% CI: 1.07, 1.56) and cross-sectional design (OR: 1.58; 95% CI: 1.20, 2.08) and among studies done in participants’ age less than 7 years (OR: 1.59; 95% CI: 1.22, 2.07) (Table 2). Pooling data for the risk of dental caries in studies that entered BMI as a continuous variable in their analyses showed no significant association between increasing BMI and risk of dental caries in children (OR: 1.01; 95% CI: 0.99 to 1.03, I2= 3.5%.) (Fig. 3). Due to the limited number of included studies, we were unable to do subgroup analyses.

Forest plot for the association between BMI (categorical) and risk of childhood dental caries. Diamonds represent pooled estimates from random-effects analysis. Horizontal lines represent 95% CIs

Forest plot for the association between BMI (continuous) and risk of childhood dental caries. Diamonds represent pooled estimates from random-effects analysis. Horizontal lines represent 95% CIs
Furthermore, we found two studies about the association of waist circumference with risk of dental caries Combined analysis of these two studies showed no significant association between WC and risk of dental caries in children (OR: 1.8 95% CI: 0.90 to 1.30, I2= 47.7%) (Fig. 4).

Forest plot for the association of waist circumference with risk of childhood dental caries. Diamonds represent pooled estimates from random-effects analysis. Horizontal lines represent 95% CIs
In addition, our non-linear dose response analysis showed a significant non-linear association between body mass index and risk of dental caries (Fig. 5). Moreover, a significant linear association was found between each unit increment in BMI and risk of dental caries in children (Fig. 6).

The non-linear association meta-analysis between BMI and risk of childhood dental caries. BMI was modeled with restricted cubic splines in a multivariate random-effects dose-response model. The vertical axis is on a log scale. Horizontal lines represent 95% CIs

Forest plot for the linear association between each unit increment in BMI and risk of childhood dental caries
Publication bias was assessed through visual inspection of a funnel plot and Egger's test (significant at p< 0.05; Fig. 7). No evidence of publication bias was found for the relationship between BMI and the risk of early childhood caries (p = 0.170 with Egger's test).

Funnel plot for the association between BMI and the risk of ECC
Discussion
We found a significant direct association between BMI and risk of dental caries in children. In addition, a significant non-linear and linear associations were found between BMI and risk of ECC. To the best of our knowledge, this is among the first studies summarizing earlier publications about the association of obesity with risk of dental caries in children.
Childhood obesity is a growing problem around the world [45]. Obesity is associated with many acute health problems and difficulties during childhood [46]. In addition, childhood obesity might also leads to adult obesity and its associated comorbidities [47]. The prevalence of dental caries is increasing among children all over the world [48], affecting their normal growth and health [49]. Findings from a prospective cohort study in Sweden showed that obese children at age 6 year had higher prevalence of dental caries compared to those with normal weight [50]. In another cohort study conducted in UK, higher BMI was associated with slightly higher chance of dental caries, but this association was not as statistically significant [28]. Moreover, several systematic reviews have been done on this topic, but their findings are controversial [11, 18, 21].
In the current study, we found a significant association between BMI and risk of childhood dental caries. In line with our findings Hayden et al. found a significant relationship between childhood obesity and dental caries [51]. In a recent meta-analysis of observational studies, children with high BMI scores were more likely to experience dental caries comparing to children with normal weight [29]. However, another meta-analysis published in this field showed no significant differences in risk of both primary and permanent dental caries between children in different BMI categories [20]. It should be noted that findings of that study might be misleading because of including only cross-sectional and low-to-middle quality studies, different criteria for BMI classification, different indices and definitions of dental caries. They also included only studies from developing countries, which might affect their findings.
Our meta-analysis also showed a linear and non-linear association between BMI and risk of childhood dental caries. Our non-linear association showed higher risk of dental caries in children with higher BMI and also among underweight children. Looking the plot, it seems that changes in risk of dental caries is more pronounced in children with BMIs lower or higher than 15. With regards to those at BMI higher than 30, we had only one study and more investigations are needed. Furthermore, we found only two studies about the association of WC and risk of childhood dental caries[34, 52]. Although the association was not significant, limited number of included studies make it difficult to discuss.
There are common risk factors linking overweight or obesity to dental carries. For example, children consumed high calorie diets rich in sugar sweetened beverages (SSB) and high calorie dense snacks are vulnerable to overweight and obesity [53]. High-calorie diet can also be associated with dental carries due to high content of fermentable sugars [18, 54, 55]. In addition, socioeconomic factors might also play a role in the association of obesity with risk of childhood dental caries [20, 51]. Reduced physical activity by increases in body weight increases snacks consumption and also time spent for watching TV [18]. Furthermore, obesity is an inflammatory state characterized by increasing cytokine production, which can in turn, leads to dental caries (57). In fact, previous studies have shown that increased inflammation in the body will result to destructive attacks to dental enamel, such that earlier studies suggested significant links between production of tumor necrosis factor (TNF-a), interleukin-6 (IL-6), and interleukin-8 (IL-8) in saliva and risk of dental caries (58).
To the best if our knowledge, current study is a comprehensive updated meta-analysis on the association of obesity with risk of childhood dental caries; moreover, it is the first dose-response analysis in this area. Along with these strengths, the study also has some limitations. High-between study heterogeneity is a common concern in these meta-analyses. We tried to find probable sources of between-study heterogeneity by doing subgroup analyses. Assessment of obesity by different methods, applying different indices and definitions for diagnosis of dental caries and inconsistent adjustment for potential confounders were the major concerns. In addition, lack of studies in which obesity was assessed by updated and accurate methods, rather than BMI, is another limitation of the current meta-analysis. There are diet-related factors such as energy intake, macronutrients, and micronutrients that that most of the studies included in our study did not adjust for these factors.
In conclusion, in this systematic review and meta-analysis we found a significant direct association between BMI with risk of childhood dental caries. In addition, significant non-linear and linear associations were found between BMI and risk of ECC. Notably, the reviewed articles were of high quality, which strengthens the reliability of these findings. However, it is important to consider the potential risk of bias present in some studies. To further clarify these associations, additional longitudinal studies employing diverse obesity assessment tools are necessary.
Availability of data and materials
The datasets used and analysed during the current study available from the corresponding author on reasonable request
References
Ellulu MS, Patimah I, Khaza’ai H, Rahmat A, Abed Y. Obesity and inflammation: the linking mechanism and the complications. Arch Med Sci. 2017;13(4):851–63.
Organization WH, Organization WH. Obesity and overweight fact sheet. 2016. Department of Sustainable Development and Healthy Environments Available from: http://www.searo who int/entity/noncommunicable_diseases/media/non_communicable_diseases_obesity_fs pdf accessed June10. 2018.
Sadeghi A, Mousavi SM, Mokhtari T, Parohan M, Milajerdi A. Metformin therapy reduces obesity indices in children and adolescents: a systematic review and meta-analysis of randomized clinical trials. Childhood Obesity. 2020;16(3):174–91.
Fang X, Zuo J, Zhou J, Cai J, Chen C, Xiang E, et al. Childhood obesity leads to adult type 2 diabetes and coronary artery diseases: A 2-sample mendelian randomization study. Medicine (Baltimore). 2019;98(32): e16825.
Milajerdi A, Keshteli AH, Afshar H, Esmaillzadeh A, Adibi P. Dietary total antioxidant capacity in relation to depression and anxiety in Iranian adults. Nutrition. 2019;65:85–90.
Yusefzadeh H, Rahimi B, Rashidi A. Economic burden of obesity: A systematic review. Soc Health Behav. 2019;2:7–12.
Antonelli R, Massei V, Ferrari E, Gallo M, Pertinhez TA, Vescovi P, et al. Salivary Diagnosis of Dental Caries: A Systematic Review. Curr Issues Mol Biol. 2024;46(5):4234–50.
Frencken JE, Sharma P, Stenhouse L, Green D, Laverty D, Dietrich T. Global epidemiology of dental caries and severe periodontitis - a comprehensive review. J Clin Periodontol. 2017;44(Suppl 18):S94-s105.
Kandelman D, Arpin S, Baez RJ, Baehni PC, Petersen PE. Oral health care systems in developing and developed countries. Periodontology 2000. 2012;60(1):98-109.
Leong PM, Gussy MG, Barrow SYL, de Silva-Sanigorski A, Waters E. A systematic review of risk factors during first year of life for early childhood caries. International journal of paediatric dentistry. 2013;23(4):235–50.
Silva AER, Menezes AMB, Demarco FF, Vargas-Ferreira F, Peres MA. Obesity and dental caries: systematic review. Revista de Saúde Pública. 2013;47:799–812.
Hong L, Ahmed A, McCunniff M, Overman P, Mathew M. Obesity and dental caries in children aged 2–6 years in the United States: National Health and Nutrition Examination Survey 1999–2002. Journal of public health dentistry. 2008;68(4):227–33.
Honne T, Pentapati K, Kumar N, Acharya S. Relationship between obesity/overweight status, sugar consumption and dental caries among adolescents in South India. International journal of dental hygiene. 2012;10(4):240–4.
Marshall TA, Eichenberger-Gilmore JM, Broffitt BA, Warren JJ, Levy SM. Dental caries and childhood obesity: roles of diet and socioeconomic status. Community dentistry and oral epidemiology. 2007;35(6):449–58.
Vázquez-Nava F, Vázquez-Rodríguez EM, Saldívar-González AH, Lin-Ochoa D, Martinez-Perales GM, Joffre-Velázquez VM. Association between obesity and dental caries in a group of preschool children in Mexico. Journal of public health dentistry. 2010;70(2):124–30.
Pham TAV, Nguyen PA. Factors related to dental caries in 10-year-old Vietnamese schoolchildren. International dental journal. 2019;69(3):214–22.
Hooley M, Skouteris H, Boganin C, Satur J, Kilpatrick N. Body mass index and dental caries in children and adolescents: a systematic review of literature published 2004 to 2011. Systematic reviews. 2012;1(1):57.
Alshihri AA, Rogers HJ, Alqahtani MA, Aldossary MS. Association between dental caries and obesity in children and young people: a narrative review. International journal of dentistry. 2019;2019.
Paisi M, Kay E, Bennett C, Kaimi I, Witton R, Nelder R, Lapthorne D. Body mass index and dental caries in young people: a systematic review. BMC Pediatr. 2019;19(1):122.
Chen D, Zhi Q, Zhou Y, Tao Y, Wu L, Lin H. Association between dental caries and BMI in children: a systematic review and meta-analysis. Caries research. 2018;52(3):230–45.
Kantovitz KR, Pascon FM, Rontani RMP, Gavião MBD, Pascon FM. Obesity and dental caries--A systematic review. Oral health & preventive dentistry. 2006;4(2).
Greenland S, Longnecker MP. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am J Epidemiol. 1992;135(11):1301–9.
Orsini N, Bellocco R, Greenland S. Generalized least squares for trend estimation of summarized dose–response data. The stata journal. 2006;6(1):40–57.
Harre Jr FE, Lee KL, Pollock BG. Regression models in clinical studies: determining relationships between predictors and response. JNCI: Journal of the National Cancer Institute. 1988;80(15):1198-202.
Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute. 2011;2(1):1-12.
Frazao P, Benicio MH, Narvai PC, Cardoso MA. Food insecurity and dental caries in schoolchildren: a cross-sectional survey in the western B razilian A mazon. European journal of oral sciences. 2014;122(3):210–5.
Costa LR, Daher A, Queiroz MG. Early childhood caries and body mass index in young children from low income families. International journal of environmental research and public health. 2013;10(3):867–78.
Kay EJ, Northstone K, Ness A, Duncan K, Crean SJ. Is there a relationship between birthweight and subsequent growth on the development of dental caries at 5 years of age? A cohort study. Community dentistry and oral epidemiology. 2010;38(5):408–14.
Peng SM, Wong HM, King NM, McGrath C. Is dental caries experience associated with adiposity status in preschool children? Int J Paediatr Dent. 2014;24(2):122–30.
Marro F, De Smedt S, Rajasekharan S, Martens L, Bottenberg P, Jacquet W. Associations between obesity, dental caries, erosive tooth wear and periodontal disease in adolescents: a case-control study. European archives of paediatric dentistry : official journal of the European Academy of Paediatric Dentistry. 2020.
Tschammler C, Simon A, Brockmann K, Röbl M, Wiegand A. Erosive tooth wear and caries experience in children and adolescents with obesity. Journal of dentistry. 2019;83:77–86.
Boustedt K, Roswall J, Kjellberg E, Twetman S, Dahlgren J. A prospective study of perinatal and metabolic risk factors for early childhood caries. Acta paediatrica (Oslo, Norway : 1992). 2020.
Karki S, Päkkilä J, Ryhänen T, Laitala ML, Humagain M, Ojaniemi M, Anttonen V. Body mass index and dental caries experience in Nepalese schoolchildren. Community dentistry and oral epidemiology. 2019;47(4):346–57.
Paisi M, Kay E, Kaimi I, Witton R, Nelder R, Potterton R, Lapthorne D. Obesity and caries in four-to-six year old English children: a cross-sectional study. BMC Public Health. 2018;18(1):1–9.
Schüler IM, Haberstroh S, Dawczynski K, Lehmann T, Heinrich-Weltzien R. Dental Caries and Developmental Defects of Enamel in the Primary Dentition of Preterm Infants: Case-Control Observational Study. Caries Res. 2018;52(1–2):22–31.
Aung YM, Jelleyman T, Ameratunga S, Tin Tin S. Body mass index and dental caries in New Zealand pre-school children: A population-based study. J Paediatr Child Health. 2021;57(9):1432–7.
Feldens CA, Dos Santos IF, Kramer PF, Vítolo MR, Braga VS, Chaffee BW. Early-Life Patterns of Sugar Consumption and Dental Caries in the Permanent Teeth: A Birth Cohort Study. Caries Res. 2021;55(5):505–14.
Marro F, De Smedt S, Rajasekharan S, Martens L, Bottenberg P, Jacquet W. Associations between obesity, dental caries, erosive tooth wear and periodontal disease in adolescents: a case-control study. Eur Arch Paediatr Dent. 2021;22(1):99–108.
Methuen M, Kauppinen S, Suominen AL, Eloranta AM, Väistö J, Lakka T, et al. Dental caries among Finnish teenagers participating in physical activity and diet intervention: association with anthropometrics and behavioural factors. BMC Oral Health. 2021;21(1):333.
Mohamed RN, Basha S, Al-Thomali Y, AlZahrani FS, Ashour AA, Almutair NE. Association between early childhood caries and obesity among preschool children. Oral Health Prev Dent. 2022;20:113–8.
Piovesan É TA, Leal SC, Bernabé E. The Relationship between Obesity and Childhood Dental Caries in the United States. Int J Environ Res Public Health. 2022;19(23).
Yen CE, Lin YY, Hu SW. Anthropometric Status, Diet, and Dental Caries among Schoolchildren. Int J Environ Res Public Health. 2021;18(13).
Marro F, De Smedt S, Rajasekharan S, Martens L, Bottenberg P, Jacquet W. Associations between obesity, dental caries, erosive tooth wear and periodontal disease in adolescents: a case–control study. European Archives of Paediatric Dentistry.1-10.
Shivpuri A, Shivpuri A, Sharma S. Childhood obesity: Review of a growing problem. International Journal of Clinical Pediatric Dentistry. 2012;5(3):237.
Kelly AS, Barlow SE, Rao G, Inge TH, Hayman LL, Steinberger J, et al. Severe obesity in children and adolescents: identification, associated health risks, and treatment approaches: a scientific statement from the American Heart Association. Circulation. 2013;128(15):1689–712.
Lakshman R, Elks CE, Ong KK. Childhood obesity. Circulation. 2012;126(14):1770–9.
Chiu S-H, DiMarco MA, Prokop JL. Childhood Obesity and Dental Caries in Homeless Children. Journal of Pediatric Health Care. 2013;27(4):278–83.
Sheiham A. Dental caries affects body weight, growth and quality of life in pre-school children. British dental journal. 2006;201(10):625–6.
Alm A, Isaksson H, Fahraeus C, Koch G, Andersson-Gare B, Nilsson M, et al. BMI status in Swedish children and young adults in relation to caries prevalence. Swed Dent J. 2011;35(1):1–8.
Hayden C, Bowler JO, Chambers S, Freeman R, Humphris G, Richards D, Cecil JE. Obesity and dental caries in children: a systematic review and meta-analysis. Community dentistry and oral epidemiology. 2013;41(4):289–308.
Manohar N, Hayen A, Fahey P, Arora A. Obesity and dental caries in early childhood: A systematic review and meta-analyses. Obesity Reviews. 2020;21(3): e12960.
Sahoo K, Sahoo B, Choudhury AK, Sofi NY, Kumar R, Bhadoria AS. Childhood obesity: causes and consequences. J Family Med Prim Care. 2015;4(2):187–92.
Harris R, Nicoll AD, Adair PM, Pine CM. Risk factors for dental caries in young children: a systematic review of the literature. Community dental health. 2004;21(1):71–85.
Khademi Z, Milajerdi A, Larijani B, Esmaillzadeh A. Dietary intake of total carbohydrates, sugar and sugar-sweetened beverages, and risk of inflammatory bowel disease: A systematic review and meta-analysis of prospective cohort studies. Frontiers in Nutrition. 2021;8: 707795.
Abbasi F, Pourjalali H, do Nascimento IJB, Zargarzadeh N, Mousavi SM, Eslami R, Milajerdi A. The effects of exercise training on inflammatory biomarkers in patients with breast cancer: A systematic review and meta-analysis. Cytokine. 2022;149:155712.
Acknowledgments
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
Mohammad Reza Bakhoda (M.B), Mohammad mehdi Haghighat-Lari (M.M.H) and Alireza Milajedi (A.M) designed the study. Fatemeh Abbasi (F.A), Mohammad Reza Bakhoda (M.B) and Mohammad mehdi Haghighat-Lari (M.M.H) collected data. Fatemeh Abbasi (F.A) and Alireza Milajedi (A.M) analyzed data. Zeinab Khademi (Z.K) and Alireza Milajedi (A.M) wrote the manuscript. All authors read and approved the final manuscript. In addition, Mohammad mehdi Haghighat-Lari (M.M.H), Gholamreza Khosravi (G.K) and Alireza Milajedi (A.M) revised the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This section is not applicable because this study is a systematic review and Meta-analysis.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Bakhoda, M.R., Haghighat Lari, M.M., Khosravi, G. et al. Childhood obesity in relation to risk of dental caries: a cumulative and dose-response systematic review and meta-analysis. BMC Oral Health 24, 966 (2024). https://doi.org/10.1186/s12903-024-04733-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-024-04733-5