
Abstract
Background
Physical and mental health problems are becoming more serious among college students due to lifestyle changes and increased academic stress. Qigong exercise has been regarded as a potentially effective intervention to improve the physical and mental health of college students.
Methods
Eleven databases were searched from their respective inception dates to April 2022. Relevant randomized controlled trials (RCTs) were included. Physical and psychological conditions, including limb muscle strength, flexibility, cardiorespiratory endurance, vital capacity, blood pressure and heart rate, as well as depression, anxiety and mood, were evaluated. The risk of bias was assessed with the Cochrane Collaboration tool.
Results
Sixteen randomized controlled trials were included in the meta-analysis. Significant improvements in cardiorespiratory endurance (MD = 3.83, 95% CI: 0.99 to 6.67, P = 0.008) and flexibility (MD = 3.01, 95% CI: 1.21 to 4.81, P = 0.001) were observed. We also observed that Qigong exercise significantly reduced depression and anxiety symptoms (SMD=-0.89, 95% CI: -1.17 to -0.61, P < 0.00001; SMD=-0.78, 95% CI: -1.31 to -0.25, P = 0.004). Nevertheless, no significant effects on muscle strength, vital capacity, blood pressure, heart rate or mood were found.
Conclusion
Qigong exercise was advantageous for college students in terms of improving flexibility and cardiorespiratory endurance and alleviating depression and anxiety to some extent. However, due to the limited number of eligible trials and the low methodological quality, more well-designed RCTs are needed in the future.
Similar content being viewed by others


Introduction
With the number of cellphone users increasing dramatically [1], an increasing number of young people are spending a lot of time on electronic devices, resulting in a sedentary lifestyle being prevalent among college students worldwide. A report among East Asian college students indicated that physical inactivity is present in 7.2% in Singapore, 16.8% in Hong Kong, and 28.5% in South Korea [2]. In 2018, a study of 1.9 million participants from 168 countries revealed that more than a quarter of adults worldwide fail to achieve the recommended level of exercise [3]. Similarly, in the United States, fewer than 60% of students perform 30 min of moderate-intensity exercise a day [4]. Sedentary lifestyle is increasingly prevalent and has also been recognized as an important risk factor for chronic conditions such as cardiovascular disease, metabolic syndrome and diabetes [5,6,7,8].
Meanwhile, studies have shown that college students may have ‘worse’ mental health than the general population [9]. Compared with nonstudent groups of the same age, college students are more likely to suffer from a variety of mental health problems due to the influence of multiple pressures, such as academic challenges and competition with peers [10,11,12]. A survey of 14,175 college students in the United States revealed that the morbidity of depression was 17.3%, that of anxiety was 7.0%, that of suicidal ideation was 6.3%, and that of nonsuicidal self-harm was 15.3% [13]. In a 2017 global study, 35% of 13,984 college students surveyed worldwide were positive for at least one of the mental disorders when assessed [14]. In addition, the proportion of college students experiencing depressive and anxiety symptoms has been increasing over the past decade [15], and these psychological problems are associated with poorer academic performance, unstable intimate relationships, and even suicidal behaviour [16]. If mental health problems are ignored and untreated, they may lead to students suffering from dropping out of college, committing suicide, or engaging in other risky behaviours [17]. Due to the negative impact on individuals and society, the mental health of college students has received much attention from society in the past 20 years and has become a hot topic in the field of psychology.
Qigong is a traditional Chinese aerobic exercise for physical and mental health, based on Taoist philosophy and traditional Chinese medicine theory [18]. It is a total body and mind movement that coordinates body posture, movement and breathing and has been used for thousands of years in China to promote health [19–20]. As a mind-body exercise, the key elements of Qigong are body movement, spiritual guidance and controlled breathing [21–22], and there are various forms of Qigong in China, including Tai Chi [23],Wuqinxi, Baduanjin, Yijinjing, and Liuzijue [24]. Previous studies have indicated that Qigong can enhance the cardiorespiratory endurance and flexibility of college students, reduce anxiety, alter their state of mind, and improve the psychological well-being, thus promoting the development of their physical and mental health [4, 9, 25–26]. However, no previous review systematically assessed Qigong exercise for physical and mental health among college students. Although a narrative review analysed Tai Chi and Qigong for the treatment and prevention of mental disorders, it lacked a quantitative analysis [27]. A meta-analysis assessed the effect of Qigong exercise on psychological status in adolescents, but it was not based on RCTs and did not contain an analysis of physical functions [28]. Meanwhile, there are some studies containing meta-analyses of RCTs that have evaluated the effects of Qigong on physical [29–30] and mental health [31,32,33,34], but they focused mainly on middle-aged and elderly people with various diseases, with only a small part of them being young people. Therefore, this study aimed to conduct a comprehensive systematic review and meta-analysis to evaluate the effects of Qigong exercise on the physical and mental health of college students.
Methods
Search strategy
Original research articles published from database inception to April 2022 were identified with keywords such as “Qi gong”, “mindful exercise”, “college students” and “random” from the following 11 electronic databases: PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), Embase, Web of Science, Ovid, ClinicalTrials.gov, CINAHL (via EBSCOhost), EBSCO, China National Knowledge Information Database (CNKl), Chinese Scientific Journal Database (VIP) and WanFang Database. The journal languages were restricted to Chinese and English. The inclusion and exclusion criteria were as follows: (1) RCTs published in English and Chinese; (2) Qigong (including Tai Chi, Wuqinxi, Baduanjin, Yijinjing, and Liuzijue) as an intervention to improve physical and mental health; (3) Outcomes included commonly psychological indicators (depression, anxiety and mood) or physical fitness (limb muscle strength, flexibility, cardiorespiratory endurance, vital capacity, blood pressure and heart rate); and (4) participants were college students irrespective of health status. Those studies not focusing on Qigong or Qigong mixed with other interventions, with no full text and with insufficient information and data were excluded from our analysis. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to present detailed results. The PROSPERO registration number for this systematic review is CRD42021256823.
Study selection
Two reviewers independently screened all study titles and abstracts. The full text of the studies that potentially met the inclusion criteria was obtained, and all potentially relevant references were retrieved according to the predefined inclusion criteria. Disagreements were resolved through discussion and, if necessary, consultation with a third investigator to reach a consensus.
Data extraction
Two reviewers independently selected studies based on the inclusion and exclusion criteria. The following details of each study were extracted: (1) general information: study title, first author name and year of publication; (2) characteristics of participants: mean age, sample size; (3) characteristics of included studies: study type and design, interventions in experimental and control groups, duration of treatment; and (4) outcome measures and results: mean, SD (standard deviation). If data were missing from the included studies or the results were not reported as the mean and standard deviation, the authors were contacted by email for data.
Methodological Quality Assessment
The quality of each study was assessed independently by 2 reviewers according to the Cochrane Collaboration tool [35]; when the opinions of the 2 reviewers were inconsistent, a third reviewer was consulted, and a consensus was reached through discussion.
Statistics
Cochrane Collaboration Review Manager Software (RevMan version 5.3.0) was used for all data analyses. For continuous data, when the units or methods for evaluating the same outcome were consistent, the mean difference (MD) was used as the summary statistic; otherwise, standardized mean differences (SMD) were used when the units or methods for evaluating the same outcome were inconsistent. Heterogeneity was assessed by calculating I2 values. According to the study of Borenstein et al. 2010 and Handbook for Systematic Reviews,a random effects model was used to pool the data as taking variability between the included studies into consideration [36, 37]. P values < 0.05 were considered to be statistically significant. Funnel plot analysis was performed when at least 10 studies were included in the analysis [38].
Results
Study selection
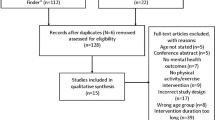
A total of 1721 relevant articles were retrieved from eleven electronic databases. After removing duplicate articles, 1217 articles remained. After reading the titles and abstracts, 1102 articles were excluded. After reading the full texts of the remaining 115 articles, 99 studies were further excluded for the following reasons: insufficient information and data (n = 22); no relevant outcomes (n = 14); no control group (n = 24); not a full article (n = 17); and other (n = 22). Finally, 16 studies were found to meet the study inclusion criteria and were pooled for meta-analysis [4, 9, 39−52]. The PRISMA flow diagram is illustrated in Fig. 1.

Flowchart of the search process for the articles
Study characteristics
The basic characteristics of the included studies are summarized in Table 1. A total of 1628 subjects in sixteen studies from thirteen Chinese [39–46, 48−52] and three English articles [4, 9, 47] were included in the final analysis. All these studies were conducted in China and published in Chinese and foreign language journals from 2015 to 2022. All participants were undergraduate or graduate students. The studies compared the effects of Qigong exercise with original sports exercise practices, muscle relaxation training or maintaining the original lifestyle without any intervention on the physical and mental health of college students. The intervention time in the Qigong group and the control group was the same, and interventions ranged from 8 weeks to 32 weeks, with most interventions being 12 weeks. All studies reported physical or psychological outcomes. Among them, in terms of psychological indicators, eleven studies evaluated depression by using the self-rating depression scale (SDS) [39, 41, 48, 50], SCL-90 Depression [42–43, 49, 51–52], center for epidemiologic studies depression scale (CES-D) [46] and hamilton depression scale (HAMD) [45]; eight studies used the self-rating anxiety scale (SAS) [39, 48, 50] and SCL-90 anxiety [42–43, 49, 51–52] to assess anxiety, and three studies used the profile of mood states (PMOS) [4, 47, 49] to assess mood. In the evaluation of physical indicators, seven studies reported vital capacity [4, 9, 40, 42,43,44, 52], five studies used a standing long jump to evaluate lower limb strength [4, 40, 42–43, 52], four studies reported hand grip force levels [4, 42–43, 52], five studies reported using the Sit-and-Reach test to assess flexibility [4, 9, 40, 42–43], five studies reported using the step test to assess cardiorespiratory endurance [4, 9, 42–43, 52], three studies reported blood pressure [4, 9, 44], and three studies reported heart rate [4, 9, 44].
Assessment of risk of bias
All 16 studies reported randomization, but only 3 trials reported randomizing the patients by using statistical software or a random number table to generate randomization sequences [4, 9, 50]. Two studies mentioned allocation concealment. The allocation sequence was concealed with password access files or kept with a project manager [4, 9]. For participant and personnel blinding, 16 studies were rated as high risk due to completely different intervention methods between the experimental and control groups [47, 52] and no intervention measures in control groups [4, 9, 39–46, 48−51]. Thus, it was unable to do blindness. Two studies reported dropouts during the clinical study, but all indicated reasons were unlikely to be related to the results [4, 9]. Therefore, the risk of bias for incomplete outcome data was assessed as low risk for all studies. Two studies were assessed as low risk with a protocol available [4, 9], while the remaining studies were unclear, as there was not enough information to judge. Two studies described the limitations of the study in the Discussion section and were therefore rated as high risk [45, 47] (Fig. 2).

Risk of bias summary and graph
Evaluation of physical outcomes
Flexibility
Five RCTs [4, 9, 42–43] analysed the scores of the Sit-and-Reach test as indicators of flexibility, including a total of 684 participants (336 in the Qigong group and 348 in the control group). The pooled results revealed a significant difference for the effect of Qigong exercise on the sit-and-reach index (MD = 3.01, 95% CI: 1.21 to 4.81, P = 0.001). However, due to the high heterogeneity among the studies (I2 = 70%) (Fig. 3A), a sensitivity analysis was conducted in which the included studies were excluded one by one. However, no matter which study was removed, the heterogeneity remained high. The Qigong group was also better than the control group (P < 0.05).

Meta-analysis of Qigong exercise on physical fitness (A:flexibility, B:cardiorespiratory endurance, C:hand grip force, D:standing long jump)
Cardiorespiratory endurance
The scores of the step test for cardiorespiratory endurance were analysed in five RCTs [4, 9, 42–43, 52] that included a total of 704 participants (346 in the Qigong group and 358 in the control group). Compared to the control group, the results of the pooled meta-analyses showed a significant improvement (MD = 3.83, 95% CI: 0.99 to 6.67, P = 0.008) in college students with Qigong exercise. Although the subgroup analysis also showed that Qigong significantly increased cardiorespiratory endurance, the heterogeneity remained high (I2 = 89%) (Fig. 3B). And heterogeneity did not obviously change after sensitivity analysis by removing any one of those studies.
Hand grip force
Four RCTs [4, 42–43, 52] analysed the effect of Qigong interventions on hand grip force levels, including a total of 506 participants (251 in the Qigong group and 255 in the control group). The pooled result showed no statistically significant difference between Qigong and control groups (SMD = 0.08, 95% CI: − 0.09 to 0.26, P = 0.34, I2 = 0%) (Fig. 3C). And the subgroup meta-analysis showed that there was no significant difference in neither no intervention control subgroup (P = 0.46) nor active control subgroup (P = 0.49).
Standing long jump
The standing long jump scores were analysed in five RCTs [4, 40, 42–43, 52] involving a total of 566 participants (281 in the Qigong group and 285 in the control group). The pooled results showed that the difference was not statistically significant (SMD = 0.16, 95% CI: − 0.08 to 0.40, P = 0.20, I2 = 48%) (Fig. 3D). And the subgroup meta-analysis showed that there was no significant difference in neither no intervention control subgroup (P = 0.21) nor active control subgroup (P = 0.81).
Vital capacity
Seven RCTs [4, 9, 40, 42,43,44, 52] reported the vital capacity of 712 participants (350 in the Qigong group and 362 in the control group), and the pooled result showed that the improvement of vital capacity in the Qigong groups was not significantly different from control groups (SMD = 0.07, 95% CI: -0.12 to 0.27, P = 0.46, I2 = 41%) (Fig. 4A). Subgroup analysis of both no intervention control and active control also showed no significant difference between the Qigong exercise and control groups (P = 0.55 and P = 0.47, respectively).

Meta-analysis of Qigong exercise on vital capacity,blood pressure and heart rate (A:vital capacity, B:systolic blood pressure, C:diastolic blood pressure, D:heart rate)
Systolic blood pressure
Systolic blood pressure scores were analysed in three RCTs [4, 9, 44] that included a total of 428 participants (208 in the Qigong group and 220 in the control group). Meta-analysis showed that there was no significant difference between the Qigong exercise and control groups (MD =− 0.70 95% CI: − 3.50 to 2.09, P = 0.62, I2 = 26%) (Fig. 4B).
Diastolic blood pressure
Diastolic blood pressure scores were analysed in three RCTs [4, 9, 44], including a total of 428 participants (208 in the Qigong group and 220 in the control group). The pooled results showed that compared with the control group, no significant difference was found in the Qigong group (MD=− 0.24, 95% CI: − 1.91 to 1.42, P = 0.77, I2 = 0%) (Fig. 4C).
Heart rate
Three RCTs [4, 9, 44] analysed heart rate scores that included a total of 428 participants (208 patients in the Qigong group and 220 in the control group). The pooled result showed that there was no significant difference between the Qigong exercise and control groups (SMD = 0.00, 95% CI: − 0.19 to 0.19, P = 1.00, I2 = 0%) (Fig. 4D).
Evaluation of psychological outcomes
Depression
Eleven RCTs [39, 41–43, 45−46, 48−52] analysed the effect of Qigong interventions on depression, including a total of 1098 participants (550 in the Qigong group and 548 in the Control group). The pooled results showed that the difference was statistically significantly (SMD=− 0.89, 95% CI: − 1.17 to − 0.61, P < 0.00001). On the subgroup meta-analysis, both no intervention control (P < 0.00001) and active control subgroup (P = 0.01) showed significant differences. However, due to the still substantive heterogeneity among the studies (I2 = 79%) (Fig. 5A), a sensitivity analysis was conducted in which the included studies were excluded one by one. The heterogeneity was significantly reduced (I2 = 58%, P < 0.00001) when the study of ChengX et al., 2016, was removed (Supplementary Fig. 1). The funnel plot shows almost bilateral symmetry and is less likely to be influenced by publication bias (Fig. 5).

Meta-analysis of Qigong exercise on psychological outcomes (A:depression, B:anxiety, C:mood)
Anxiety
Eight RCTs [39, 42–43, 48−52] analysed the anxiety of 972 participants (487 in the Qigong group and 485 in the Control group). The pooled meta-analysis showed that Qigong treated group had significantly lower anxiety than control group (SMD= − 0.78, 95% CI: − 1.31 to − 0.25, P = 0.004) with substantive heterogeneity (I2 = 93%) (Fig. 5B). Subgroup analysis also showed no significant effect in both the no intervention control (P = 0.01) and active control subgroup (P = 0.0005). But the heterogeneity in subgroup was still substantive (I2 = 94%). So sensitivity analysis was conducted and heterogeneity was significantly reduced when the study of LuoS et al., 2021 was removed (SMD= − 0.51, 95% CI: − 0.67 to − 0.35, P < 0.00001, I2 = 0%) (Supplementary Fig. 2).
Mood
Three RCTs [4, 47, 49] involving 448 participants (222 in the Qigong group and 226 in the Control group) analysed the effects of Qigong exercise on mood scores. The pooled results of the meta-analysis showed no significant changes between the Qigong exercise and control groups (MD=-7.79, 95% CI: -16.18 to 0.60, P = 0.07, I2 = 93%) (Fig. 6).
Subgroup analysis of no intervention control also showed no significant difference (P = 0.15, I2 = 62%), whereas the subgroup analysis of active control showed a significant improve in mood (P = 0.004).

Funnel plot about meta-analysis of Qigong exercise on depression
Sensitivity analyses
The results of sensitivity analysis were stable by model transformation between fixed effect model and random effects model and removing studies one by one.
Discussion
The purpose of this systematic review and meta-analysis was to investigate whether Qigong could improve limb muscle strength, flexibility, cardiorespiratory endurance, vital capacity, blood pressure and heart rate and alleviate depression, anxiety and mood changes in college students when these parameters were evaluated with commonly used physical fitness and psychological assessments. The meta-analysis showed significant improvements in cardiorespiratory endurance (measured by the step test) and flexibility (measured by the sit-and-reach test) with Qigong exercise. In addition, there was a significant reduction in depression and anxiety symptoms. However, there was no significant effect of Qigong exercise on vital capacity, blood pressure, heart rate, muscle strength (measured by the standing long jump test and hand grip force test) or mood.
The significant improvement in flexibility was also supported by Wehner C et al. [29]. Based on the included studies, twice a day, five days a week, for three months, Badujin and Yijinjing are recommended for improving trunk flexibility [42–43]. However, due to unexplained high heterogeneity of uncertain causes, we need to be cautious of this result.
We used step test to measure cardiorespiratory endurance. The meta-analysis showed that Qigong was beneficial for cardiorespiratory endurance. The included studies suggested that Yijinjing twice a day, more than 5 days a week for 3 months and Wuqinxi 5 days a week for 4 months are beneficial to improve the cardiopulmonary endurance of college students [42, 52]. However, given the unexplained high heterogeneity, we need to be cautious of these results.
Depression and anxiety have been widely studied in previous epidemiological studies looking at the relationship between exercise and mental health [53–54]. The results of this review are consistent with the conclusions of a previously published review suggesting that Tai Chi and Qigong exercises contribute to reducing anxiety and depression symptoms [26, 55–56]. Specifically, effect size estimates with respect to the effects of Qigong ranged from − 0.52 to − 1.94 for depression levels and from − 0.39 to − 0.78 for anxiety levels. The effective mechanism of Qigong may be attributed to Qigong training increasing excitation of the middle cerebral cortex, which has been shown to modulate the hypothalamic-pituitary-adrenal axis [57–58], monoamine neurotransmitter [57], brain-derived neurotrophic factor [57] and adiponectin [59] to alleviate severe psychological symptoms, such as anxiety and depression.
No significant changes in other physical outcomes, including limb strength, vital capacity, blood pressure and heart rate, were observed. One possible explanation for this result is that all participants enrolled in this trial were young (aged 18–25 years old) and apparently healthy college students. Ainsworth et al. [60] classified the intensity of Qigong, such as Tai Chi, as moderate intensity, equivalent to 4 metabolic equivalents, so Qigong may only be appropriate for people with chronic diseases and not for healthy people with relatively high baseline health levels. In addition, it is possible that the 12-week intervention period for Qigong exercise is not sufficient to identify significant differences in muscular strength, vital capacity, blood pressure or heart rate for an apparently healthy college student population.
The current meta-analysis mainly has the following shortcomings. First, considering that many Qigong studies originated in China and were published in Chinese, the research languages included were limited to English and Chinese, but this still inevitably leads to some omissions. Therefore, future research should include a wider range of learned languages. Second, in this meta-analysis, most of the included trials had flaws in methodological design, mainly including the method of randomization, allocation concealment, and insufficient reporting of blinding. Third, most of the included studies did not provide data on whether participants continued to practice Qigong after the intervention period. Due to a lack of follow-up data, the long-term effect of Qigong on the physical and mental health of college students is still unclear.
Conclusion
This systematic review and meta-analysis suggests that Qigong exercise is advantageous for college students in terms of improving physical fitness (flexibility and cardiorespiratory endurance) and alleviating depression and anxiety. However, given the low methodological quality, accurate conclusions cannot be drawn thus far, and the findings need to be interpreted with caution. More large, well-designed randomized controlled trials are needed in the future.
Data availability
All data are included in this manuscript and its supplementary files.
Abbreviations
- RCTs:
-
Randomized controlled trials
- MD:
-
Mean difference
- SMD:
-
Standardized mean differences
- SD:
-
Standard deviation
- CENTRAL:
-
Cochrane Central Register of Controlled Trials
- CNKl:
-
China National Knowledge Information Database
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- SDS:
-
Self-rating depression scale
- CES-D:
-
Center for epidemiologic studies depression scale
- HAMD:
-
Hamilton depression scale
- SAS:
-
Self-rating anxiety scale
- PMOS:
-
Profile of mood states.
References
Xiao T, Jiao C, Yao J, Yang L, Zhang Y, Liu S, Grabovac I, Yu Q, Kong Z, Yu JJ, Zhang J. Effects of Basketball and Baduanjin Exercise Interventions on Problematic Smartphone Use and Mental Health among College Students: A Randomized Controlled Trial. Evid Based Complement Alternat Med. 2021:8880716. https://doi.org/10.1155/2021/8880716.
Seo DC, Torabi MR, Chin MK, Huang SF, Chen CK, Mok MM, Wong P, Chia M, Lee CG, Wang C. A comparison of factors associated with physical inactivity among East Asian college students. Int J Behav Med. 2012;19(3):316–23. https://doi.org/10.1007/s12529-011-9167-4.
Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. 2018;6(10):e1077–86. https://doi.org/10.1016/S2214-109X(18)30357-7.
Li M, Fang Q, Li J, Zheng X, Tao J, Yan X, Lin Q, Lan X, Chen B, Zheng G, Chen L. The Effect of Chinese Traditional Exercise-Baduanjin on Physical and Psychological Well-Being of College Students: A Randomized Controlled Trial. PLoS ONE. 2015;10(7):e0130544. https://doi.org/10.1371/journal.pone.0130544.
Jingjie W, Yang L, Jing Y, Ran L, Yiqing X, Zhou N. Sedentary time and its association with risk of cardiovascular diseases in adults: an updated systematic review and meta-analysis of observational studies. BMC Public Health. 2022;22(1):286. https://doi.org/10.1186/s12889-022-12728-6.
Bai J, Wang Y, Zhang XF, Ouyang YF, Zhang B, Wang ZH, Du SF, Wang HJ. Associations of Sedentary Time and Physical Activity with Metabolic Syndrome among Chinese Adults: Results from the China Health and Nutrition Survey. Biomed Environ Sci. 2021;34(12):963–75. https://doi.org/10.3967/bes2021.132.
Macías N, Espinosa-Montero J, Monterrubio-Flores E, Hernández-Barrera L, Medina-Garcia C, Gallegos-Carrillo K, Campos-Nonato I. Screen-Based Sedentary Behaviors and Their Association With Metabolic Syndrome Components Among Adults in Mexico. Prev Chronic Dis. 2021;18:E95. https://doi.org/10.5888/pcd18.210041.
Cong XF, Liu SB, Xu TL, Wang WJ, Ma JX, Chen B, Li JH. [Relationship between sedentary time and incidence of type 2 diabetes in adults in China: a prospective cohort study]. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(9):1465–1470.Chinese. https://doi.org/10.3760/cma.j.cn112338-20190926-00705.
Zheng G, Lan X, Li M, Ling K, Lin H, Chen L, Tao J, Li J, Zheng X, Chen B, Fang Q. Effectiveness of Tai Chi on Physical and Psychological Health of College Students: Results of a Randomized Controlled Trial. PLoS ONE. 2015;10(7):e0132605. https://doi.org/10.1371/journal.pone.0132605.
Mikolajczyk RT, Brzoska P, Maier C, Ottova V, Meier S, Dudziak U, Ilieva S, El Ansari W. Factors associated with self-rated health status in university students: a cross-sectional study in three European countries. BMC Public Health. 2008;8:215. https://doi.org/10.1186/1471-2458-8-215.
Tosevski DL, Milovancevic MP, Gajic SD. Personality and psychopathology of university students. Curr Opin Psychiatry. 2010;23(1):48–52. https://doi.org/10.1097/YCO.0b013e328333d625.
Gore FM, Bloem PJ, Patton GC, Ferguson J, Joseph V, Coffey C, Sawyer SM, Mathers CD. Global burden of disease in young people aged 10–24 years: a systematic analysis. Lancet. 2011;377(9783):2093–102. https://doi.org/10.1016/S0140-6736(11)60512-6.
Eisenberg D, Hunt J, Speer N. Mental health in American colleges and universities: variation across student subgroups and across campuses. J Nerv Ment Dis. 2013;201(1):60–7. https://doi.org/10.1097/NMD.0b013e31827ab077.
Auerbach RP, Mortier P, Bruffaerts R, Alonso J, Benjet C, Cuijpers P, Demyttenaere K, Ebert DD, Green JG, Hasking P, Murray E, Nock MK, Pinder-Amaker S, Sampson NA, Stein DJ, Vilagut G, Zaslavsky AM, Kessler RC, WHO WMH-ICS Collaborators. WHO World Mental Health Surveys International College Student Project: Prevalence and distribution of mental disorders. J Abnorm Psychol. 2018;127(7):623–38. https://doi.org/10.1037/abn0000362.
Lattie EG, Adkins EC, Winquist N, Stiles-Shields C, Wafford QE, Graham AK. Digital Mental Health Interventions for Depression, Anxiety, and Enhancement of Psychological Well-Being Among College Students: Systematic Review. J Med Internet Res. 2019;21(7):e12869. https://doi.org/10.2196/12869.
Dyrbye LN, Thomas MR, Shanafelt TD. Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Acad Med. 2006;81(4):354–73. https://doi.org/10.1097/00001888-200604000-00009.
Cook LJ. Striving to help college students with mental health issues. J Psychosoc Nurs Ment Health Serv. 2007;45(4):40–4. https://doi.org/10.3928/02793695-20070401-09.
Jones BM. Changes in cytokine production in healthy subjects practicing Guolin Qigong:a pilot study. BMC Complement Altern Med. 2001;1:8. https://doi.org/10.1186/1472-6882-1-8.
Lee MS, Oh B, Ernst E. Qigong for healthcare: an overview of systematic reviews. JRSM Short Rep. 2011;2(2):7. https://doi.org/10.1258/shorts.2010.010091.
Huang J, Wang XY. [Review of centennial development of Qigong]. Zhonghua Yi Shi Za Zhi. 2012;42(4):201–7.
Koh TC. Qigong–Chinese breathing exercise. Am J Chin Med. 1982;10(1–4):86–91. https://doi.org/10.1142/S0192415X82000142.
Yeh ML, Chung YC. A randomized controlled trial of qigong on fatigue and sleep quality for non-Hodgkin’s lymphoma patients undergoing chemotherapy. Eur J Oncol Nurs. 2016;23:81–6. https://doi.org/10.1016/j.ejon.2016.05.003.
Lan C, Chen SY, Lai JS, Wong AM. Tai chi chuan in medicine and health promotion. Evid Based Complement Alternat Med. 2013;2013:502131. https://doi.org/10.1155/2013/502131.
Shi H, Liu T, Dong C, Zhen K, Wang Y, Liu P, Si G, Wang L, Wang M. Scientific Evidence of Traditional Chinese Exercise (Qigong) for Chronic Obstructive Pulmonary Disease: An Overview of Systematic Reviews and Meta-Analyses. Biomed Res Int. 2022;2022:7728973. https://doi.org/10.1155/2022/7728973.
Li K, Walczak-Kozłowska T, Lipowski M, Li J, Krokosz D, Su Y, Yu H, Fan H. The effect of the Baduanjin exercise on COVID-19-related anxiety, psychological well-being and lower back pain of college students during the pandemic. BMC Sports Sci Med Rehabil. 2022;14(1):102. https://doi.org/10.1186/s13102-022-00493-3.
Gao M. Experimental Study on the Effect of Taijiquan on the Physical Function and Mental Health of College Students. Appl Bionics Biomech. 2022;2022:7346946. https://doi.org/10.1155/2022/7346946.
Abbott R, Lavretsky H. Tai Chi and Qigong for the treatment and prevention of mental disorders. Psychiatr Clin North Am. 2013;36(1):109–19. https://doi.org/10.1016/j.psc.2013.01.011.
Liu X, Li R, Cui J, Liu F, Smith L, Chen X, Zhang D. The Effects of Tai Chi and Qigong Exercise on Psychological Status in Adolescents: A Systematic Review and Meta-Analysis. Front Psychol. 2021;12:746975. https://doi.org/10.3389/fpsyg.2021.746975.
Wehner C, Blank C, Arvandi M, Wehner C, Schobersberger W. Effect of Tai Chi on muscle strength, physical endurance, postural balance and flexibility: a systematic review and meta-analysis. BMJ Open Sport Exerc Med. 2021;7(1):e000817. https://doi.org/10.1136/bmjsem-2020-000817.
Zou L, SasaKi JE, Wang H, Xiao Z, Fang Q, Zhang M. A Systematic Review and Meta-Analysis Baduanjin Qigong for Health Benefits: Randomized Controlled Trials. Evid Based Complement Alternat Med. 2017;2017:4548706. https://doi.org/10.1155/2017/4548706.
Zou L, Yeung A, Quan X, Hui SS, Hu X, Chan JSM, Wang Guo L, Kong Z, Zhang Y. Qigong-Based Therapy for Treating Adults with Major Depressive Disorder: A Meta-Analysis of Randomized Controlled Trials. Int J Environ Res Public Health. 2019;16(5):826. https://doi.org/10.3390/ijerph16050826.
Zou L, Yeung A, Quan X, Hui SS, Hu X, Chan JSM, Wang C, Boyden SD, Sun L, Wang H. Mindfulness-Based Baduanjin Exercise for Depression and Anxiety in People with Physical or Mental Illnesses: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2018;15(2):321. https://doi.org/10.3390/ijerph15020321.
Li Z, Liu S, Wang L, Smith L. Mind-Body Exercise for Anxiety and Depression in COPD Patients: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2019;17(1):22. https://doi.org/10.3390/ijerph17010022.
Chang PS, Knobf T, Oh B, Funk M. Physical and Psychological Health Outcomes of Qigong Exercise in Older Adults: A Systematic Review and Meta-Analysis. Am J Chin Med. 2019;47(2):301–22. https://doi.org/10.1142/S0192415X19500149.
Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA, Cochrane Bias Methods Group; Cochrane Statistical Methods Group. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. https://doi.org/10.1136/bmj.d5928.
Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page M. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3, (2022). Available online at: https://training.cochrane.org/handbook.
Ang L, Song E, Lee HW, Lee MS. Herbal Medicine for the Treatment of Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Clin Med. 2020;9(5):1583. https://doi.org/10.3390/jcm9051583.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. https://doi.org/10.1371/journal.pmed.1000097.
Ke XJ, Cui YS, Zhang J. Influence of Health Gigong Baduanjin on Psychological Characteristics of College Students with Neck-Shoulder Syndrome. Chin Manipulation Rehabilitation Med. 2019;10(2):9–11. https://doi.org/10.19787/j.issn.1008-1879.2019.02.005.
Lai QY, Jing CX, Chen CJ, Jiao RY, Pan HS. Research on The Baduanjin on Health Promotion of Female College Students under the Background of Healthy China. Fujian Sports Science and Technology. 2018;37(1):44–6.
Wang M, Zhao QW, Wu H. Research on Huatuo Wuqinxi’s Intervention Treatment for College Students with Mild Psychological Problems.Journal of Jinzhou Medical University(Social Sci Edition). 2020;18(1):60–2. https://doi.org/10.13847/j.cnki.lnmu(sse).2020.01.017.
Wei QB, Zhao Q, Wu YC. Study of Yi Jin Jing on Mental health and Body Constitution in College Students. Shandong J Tradit Chin Med. 2017;36(8):654–56. https://doi.org/10.16295/j.cnki.0257-358x.2017.08.009.
Yan HJ, Wei QB. Study on the effect of Baduanjin on the psychological state and physical fitness of college students. Sports, 2017;(23):49–50.
Yuan MZ, Xue HH, Huang YM. The influence of 20 weeks Taijiquan exercise on the physical function of college students. J Military Phys Educ Sports. 2017;36(3):85–8.
Cheng X, Wang DM, Chen X, Wang W, Liu C, He T, He L, Qin QZ. Health Qigong Wuqinxi improves hydrogen proton magnetic resonance spectra in prefrontal cortex and hippocampus in college students with mild depression. J South Med Univ. 2016;36(11):1468–76.
Chen J, Li Y, Wu Y, Su X. Effects of Taijiquan exercise on depression and serum inflammatory factors in female college students. Chin J Sch Health. 2019;40(7):1065–68. https://doi.org/10.16835/j.cnki.1000-9817.2019.07.029.
Chen T, Yue GH, Tian Y, Jiang C. Baduanjin Mind-Body Intervention Improves the Executive Control Function. Front Psychol. 2017;7:2015. https://doi.org/10.3389/fpsyg.2016.02015.
Zhang YZ. An Empirical Study on the Effect of Health Qigong Baduanjin on College Students’ Depression and Anxiety. Wushu Stud. 2021;6(12):131–3. https://doi.org/10.13293/j.cnki.wskx.009327.
Wang B, Wang XL, Chang YJ, Mao Y, Peng J. Research on the impact of online Baduanjin on the mental health of college freshmen under the new crown pneumonia epidemic. Health Vocat Educ. 2021;39(23):155–9.
Luo SS. Research on the intervention effect of Taijiquan on sleep disorders of college students. Chin J Convalescent Med. 2021;30(12):1249–52. https://doi.org/10.13517/j.cnki.ccm.2021.12.004.
Guo TR. Experimental Research on the Effects of Baduanjin on College Students’ Mental Health. Study of Science and Engineering at RTVU. 2021;(2):76–8. https://doi.org/10.19469/j.cnki.1003-3297.2021.02.0076.
Jiao XX, Ji H, Chen J. Effects of traditional Wuqinxi on physical fitness and mental health of female college students. Chin J Sch Health. 2021;42(9):1323–27. https://doi.org/10.16835/j.cnki.1000-9817.2021.09.011.
Hendriks T, de Jong J, Cramer H. The Effects of Yoga on Positive Mental Health Among Healthy Adults: A Systematic Review and Meta-Analysis. J Altern Complement Med. 2017;23(7):505–17. https://doi.org/10.1089/acm.2016.0334.
Huang X, Wang X, Hu J, Xue Y, Wei Y, Wan Y, Song X, Wang R, Zhang B, Fang J, Zhang S. Inadequate Mental Health Literacy and Insufficient Physical Activity Potentially Increase the Risks of Anxiety and Depressive Symptoms in Chinese College Students. Front Psychiatry. 2021;12:753695. https://doi.org/10.3389/fpsyt.2021.753695.
Liu X, Li R, Cui J, Liu F, Smith L, Chen X, Zhang D. The Effects of Tai Chi and Qigong Exercise on Psychological Status in Adolescents: A Systematic Review and Meta-Analysis. Front Psychol. 2021;12:746975. https://doi.org/10.3389/fpsyg.2021.746975.
Liu X, Clark J, Siskind D, Williams GM, Byrne G, Yang JL, Doi SA. A systematic review and meta-analysis of the effects of Qigong and Tai Chi for depressive symptoms. Complement Ther Med. 2015;23(4):516–34. https://doi.org/10.1016/j.ctim.2015.05.001.
Tsang HW, Fung KM. A review on neurobiological and psychological mechanisms underlying the anti-depressive effect of qigong exercise. J Health Psychol. 2008;13(7):857–63. https://doi.org/10.1177/1359105308095057.
Tsang HW, Tsang WW, Jones AY, Fung KM, Chan AH, Chan EP, Au DW. Psycho-physical and neurophysiological effects of qigo ng on depressed elders with chronic illness. Aging Ment Health. 2013;17(3):336–48. https://doi.org/10.1080/13607863.2012.732035.
Chan JS, Li A, Ng SM, Ho RT, Xu A, Yao TJ, Wang XM, So KF, Chan CL. Adiponectin Potentially Contributes to the Antidepressive Effects of Baduanjin Qigong Exercise in Women With Chronic Fatigue Syndrome-Like Illness. Cell Transpl. 2017;26(3):493–501. https://doi.org/10.3727/096368916X694238.
Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, O’Brien WL, Bassett DR Jr, Schmitz KH, Emplaincourt PO, Jacobs DR Jr, Leon AS. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32(9 Suppl):498–504. https://doi.org/10.1097/00005768-200009001-00009.
Acknowledgements
We would like to thank the National Natural Science Foundation of China for financial support.
Funding
This work was funded by General project of National Natural Science Foundation of China (grant numbers 81973924 and 81874501) and Youth Project of National Natural Science Foundation of China (grant numbers 81904317).The funders had no role in study conception and design,data collection and analysis,decision making for publication,or writing of the manuscript.
Author information
Authors and Affiliations
Contributions
Research conception and design, LJP, CSQ and WSZ; Data Collection, GYF, GY, ZYX and YRS; Data analysis, LJP ,LM and GYF; Methodology, LJP and CSQ; Software, WSZ; Supervision, CSQ and WSZ; The manuscript draft, LJP and GYF; The manuscript revision, CSQ and WSZ; All authors have read and approved the manuscript for publication. LJP and GYF contributed equally to this work.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
not applicable (NA).
Consent for publication
NA.
Competing interests
All authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lin, J., Gao, Y.f., Guo, Y. et al. Effects of qigong exercise on the physical and mental health of college students: a systematic review and Meta-analysis. BMC Complement Med Ther 22, 287 (2022). https://doi.org/10.1186/s12906-022-03760-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12906-022-03760-5