
Abstract
Background
Advanced Practice Nursing (APN) have been highly valued and an integral part of the health care system. Development and establishment of new APN roles is a complex process that has resulted from a wide variety of reasons, key component is a lack of a competency map delineation and role evaluation. Currently, however, competence framework has not been compared at an international level. In mainland China, APN have been introduced in some organizations but their competency domains have not yet been clearly defined, this study aimed to identify the core competencies for advanced practice nursing.
Methods
This study was performed in two phases: first, in-depth and semi-structured individual interviews with 46 participants from key stakeholders were carried out followed by a qualitative content analysis, then an item pool of core competencies was constructed by extracting data from the first phase and the results from previous studies, scales and documents; second, a Delphi technique was conducted with the participation of 28 experts from 7 areas of China to form the final core competency framework for advanced practice nursing.
Results
Through the qualitative phase, the core competency framework with six domains and 70 items emerged and then entered into the Delphi phase. Twenty-eight of 30 experts finished 2 rounds of Delphi approaches. The final core competencies for advanced practice nursing consisted of six domains with 61 items, including direct clinical nursing practice, research and evidence-based nursing practice, professional development, organization and management, mentoring and consultation, and ethical/legal practice.
Conclusion
This core competency framework consisted of six domains with 61 items can be used in competency-based education to cultivate advanced practice nurses as well as competency level assessment.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
With the increasing need for improved nursing services and outcomes, APN has spread and accepted worldwide and was proven to have advantages in improving access to care, decreasing waiting time, and cost containment of health care [1]. To date, approximately 70% of nations have some form of advanced practice nursing [2]. APN is the expanded healthcare services and interventions provided by nurses with an advanced capacity [3]. The advanced practice nurse is granted to a nurse who has completed additional education to acquire expert knowledge, complex decision-making skills, and the clinical competencies to provide expanded healthcare services within the context of nursing [4]. Identifying the definition of nursing competencies is the foundation of the conceptualization and development of advanced practice nursing roles [5, 6]. Nursing competency is a mastery of knowledge, clinical, interpersonal and technical skills, which is the basis for good performance in the clinical environment [7]. In 1996, Hamric had put forward core competencies for advanced practice nurses(APNs), which included seven domains that took clinical practice, nursing research, health coaching and education, collaboration, ethical decision making, and leadership into consideration [8]. In 2011, the American Association of Colleges of Nursing (AACN) designed six core competencies for master’s education in nursing, such as changes for quality care, culture of excellence, and translating evidence into practice [9]. In 2010, the Canadian Nurses Association published the core competency framework for nurse practitioners: clinical practice, collaboration, consultation and referral, research, and leadership [10]. In Australia, the Australian Nursing & Midwifery Council (ANMC) included three core competencies for nurse practitioners: dynamic practice, professional efficacy and clinical leadership [11]. In the UK, the Royal College of Nursing (RCN) established the core competency framework for APN [12].
Hong Kong is an area with early development of advanced practice nurses in China, the nurse specialist role was first piloted in 1993 and an advanced practice nursing role piloted in 2003. Nurse practitioner (NP) is the title of advanced practice nurse in Taiwan, who not only have a master's degree or doctor's degree, but also are registered nurses who have received the master's level education of nurse practitioner. Chinese mainland has established certified registered nurse and certified nurse systems to cultivate nurses with different competency levels under accompanying training and certification regulations. Although the current regulations for nurses, launched in 2008, did not have any APN roles or APN-related descriptions, Chinese researchers began to explore the localization of the role of advanced practice nurse based on the foreign concept model, and found that training advanced practice nurse from master level is the trend of the development of nursing specialization in recent years. By the end of March 2015, there were 84 clinical master's programs in nursing in China [13]. This resulted in a significant increase in the number of clinical nurses with master's degrees, which prompted China to establish an advanced practice specialty nursing program to prepare nurses for future work with medical specialists. Review of the literature revealed that advanced practice nurse role with higher consensus in china were clinical practitioner, manager, educator, researcher, coordinator and consultant [14]. This result is consistent with results of the international reasearech [15], but competences required for APN are wide heterogeneity, with a total of 16 was mentioned in the literature [14]. Clinical practice ability, research ability and management ability are higher consensus in the process of developing advanced practice in specialty areas, there is much confusion between Specialist Nurses(SN) and advanced practice nurses. Specialist nurses are probably those who can deal with situations in a specific area of practice. Advanced practice nurses not only perform proficiently and possess specialized knowledge, but also have original thinking, innovation and the ability to analyse complex situations in delivering services and leading changes [13]. APNs are at the frontier of their field and at the top of the clinical ladder [16]. The roles of Specialist Nurses(SN) have been defined and regulated in some organizations of mainland china. Some researchers have explored the core competencies of advanced practice nurses in different specialized fields, such as gastroenterology nursing specialists [6], oncology advanced practice nurses [17], critical care advanced practice nurses [18], and advanced midwifery practitioners [19]. In addition, previous studies in China did not provide a clear definition of specialist nurse or advanced practice nurse. The core competencies for APN role are not clearly defined, with confusion regarding the APN title more prevalent since delineation of the Specialized Nurse roles. Some intuitive or logical methods of categorization were used, with small convenience samples, resulting in validity and reliability. Under this condition, we aimed to identify a competency framework for APNs through sequential exploratory research.
The definition of advanced practice nurses(APN) used in our study is defined as a registered nurse with a master's degree or above and with at least 5 years of working experience who has received academic training and practical training, acquired the expert knowledge base, complex decision-making skills and clinical competencies for expanded practice.
Methods
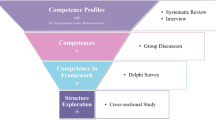
An exploratory sequential study was designed. We conducted a two-phase approach to develop the core competencies for advanced practice nursing: (1) Phase 1: a literature review and qualitative interviews were conducted to draft the initial competency framework; Phase2: The Delphi technique was used to identify the framework.
Phase 1: Semi-structured interviews with Key Stakeholders
This phase adopted a qualitative descriptive study to explore how APN’s core competencies are performed in clinical practice. An open-ended interview outline was constructed under the guidance of Hamric’s core competency framework.
Participants
This step involves identifying key stakeholders who would affect or be affected when the model of care changed and introduced an APN role. In our research, a mixed sampling strategy combining the purpose and snowball sampling method was used to recruit participants, including nursing managers, educators, experts from hospitals, government departments or associations related to health care, nursing education, and nurses with master of nursing specialist degrees. The inclusion criteria for nursing educators were as follows: (1) served as a supervisor of graduate nursing students and (2) had the title of associate professor above. The inclusion criteria for nursing managers from the hospital were as follows: (1) ever had postgraduate nursing employees; (2) served as a nursing manager for at least 1 year; (3) had clinical experience for 5 years or above; and (4) had a middle-level professional title or above. The inclusion criterion for experts from government departments or associations was to be familiar with nursing management and education policy in China. The inclusion criterion for nurses was having clinical experience of at least five years. A total of 46 participants volunteered to participate in face-to-face, semi-structured, and open-ended interviews. An interview framework was predefined to guide the interviews (Table 1).
Between March and September 2017, qualitative interviews were carried out at the study participants’ workplaces and/ or place of study. Forty-six in-depth individual interviews were conducted by the researcher, with the interview time ranging from one to two hours. The researcher had no relationships with these participants and promised the confidentiality of the interviews again before the interviews. During the interviews, the researcher listened to the participants and took notes of their tones, expressions, and body language to collect nonverbal information. At the end of the interviews, the participants were asked to verify the accuracy of the information. Each interview was audiotaped and then transcribed within 24 h after the interview.
Ethical considerations
This study was approved by the ethics committee of West China Hospital, Sichuan University (ID: 2017–177). Before starting the interviews, the researcher explained the purpose and procedure of the interviews in a private and quiet room and got the written informed consents from participants.
Data analysis
Conventional content analysis was adopted to analyse the transcripts through reading, coding, and thematising [20].
Trustworthiness
Some strategies were adopted to ensure the trustworthiness of this qualitative research process. Regarding credibility, the interview questions were designed to collect information that reflected the real experiences of the participants, and the researcher paraphrased all dialogues to ensure accurate interpretation of the participants’ opinions. Peer checking between two researchers was used to enhance the confirmability of this study. Regarding dependability, audit trials were taken by collecting, thematising and analysing data [21].
Phase 2: Delphi Process
In phase 2, for each initial competency domain, competencies relevant to each domain were drafted by combining the results of the literature review and interviews. Up to 83 competencies were formed at this stage. Then, five experts reviewed and refined the competencies by identifying redundancies, integrating related concepts, and removing competencies with a clinical focus interactively. The experts’ evaluation used the 4-point rating scale (1 = not relevant, 2 = somewhat relevant, 3 = quite relevant, and 4 = very relevant). The items were deleted when three or more experts gave 1 or 2, indicating redundancy with other items in the same category. Totally, 13 items were deleted.
The Delphi technique was used to identify competency domain delineation of the framework for APN and establish the content validity of the framework. The Delphi method was performed under the following principles: 1) including panels involving APN cultivation and potentially employers of APN; 2) incorporating an effective communicating method for the Delphi rounds through the email and web-based survey software; 3) using a structured approach built on previous results in the field; and 4) using adequate rounds to obtain consensus.
Participants
A purposive stratified sampling method was used to recruit Delphi panels. The 30 panels invited were from different fields, including nursing educators and managers. In the end, a total of 28 experts participated in the study, and two experts were too busy to participate throughout the entire study. All panels were required to be familiar with professional nursing practice and the requirements for the health service workforce, in addition to being credible within their professions.
We selected experts from 15 universities and 13 hospitals in 21 provinces, 4 municipalities and 3 autonomous regions of seven areas to ensure the representativeness of the sample. The inclusion criteria for nursing managers were as follows: (1) had a senior vice title or higher; (2) had worked at least 5 years, including at least 1 year of nursing management experience; and (3) had a bachelor’s degree or above. The inclusion criteria for nursing educators were as follows: (1) the institutions where the experts worked had a master of nursing specialist program (MNS); (2) served as a supervisor of MNS students; and (3) had the title of associate professor or above.
Instrument
The initial questionnaire of core competencies for APN developed based on the results from Phase 2 included three parts: (1) a cover letter introducing the study and instructing the completion of this questionnaire; (2) core competency framework for APN consisting of six dimensions with 70 items; and (3) experts’ sociodemographic information and their judgement and familiarity with the field of this questionnaire.
Data collection
The Delphi approaches were conducted from October 2017 to December 2017. We communicated with the Delphi panels through email, and all panelists were kept anonymous throughout the process. For each of our Delphi rounds, panelists were asked to indicate the importance of each domain and the related items within the domains described in the seed statement using a five-point Likert scale with scores ranging from 1 (highly unimportant) to 5 (highly important). Before the rating process, the panels were asked to give comments on the domain delineation. Each question had a blank for the experts to fill in their comments. The experts were asked to complete the questionnaire within 3 weeks. In the next round, panel members were sent the new version of the questionnaire attached to the panel’s comments. Two rounds were finally conducted to reach the final consensus.
Data analysis
All data were collected using a Web-based online survey and analysis software. The sociodemographic characteristics of the experts were described using appropriate methods. The mean, standard deviation (SD), coefficient of variation (CV), and content validity index (CVI) for each item were calculated. Items were removed if any item met the following criteria simultaneously: mean < 4, CV > 0.25, and CVI < 0.75 [22]; if any item met one or two criteria above, it was kept into the next Delphi round. The authority coefficient (Cr) and respondent rate of experts were also calculated. The authority coefficient was the mean of the sum of the content familiarity coefficient (Cs) and judgement coefficient (Ca), which we collected in the initial questionnaire. The judgement coefficient consisted of four dimensions: working experience, theory analysis, referring to literatures, and self-intuition. The working experience was defined as “great”, “medium” and “small” with a score of 0.5, 0.4 and 0.3 respectively. The theory analysis was defined as “great”, “medium” and “small” with a score of 0.3, 0.2 and 0.1 respectively. The referring to literatures and self-intuition were both defined as “great”, “medium” and “small” with a score of 0.1, 0.1 and 0.05 respectively. And the familiar coefficient ranged from 0.25 to 1.0, indicating “unfamiliar” to “very familiar” [23]. The Cr and respondent rate were acceptable if the value was over 0.7 [24]. Analyses in this phase were conducted in SPSS 23.0.
Ethical considerations
This study was performed in line with the principles of the Declaration of Helsinki and its later amendments or comparable ethical standards. We got informed consent from all the participants before taking the survey in the study. Approval for the study was granted by the Ethics committee of West China Hospital, Sichuan University (ID: 2017–177).
Results
Phase 1: semi-structured interviews with key stakeholders
Characteristics of participants
In Phase 1, a total of 22 experts took part in the interviews with a mean age of 47.9 ± 6.7 years old and a mean working time of 27.1 ± 9.1 years from fields of nursing education, management, clinical nursing practice and policy makers; 9 students of nursing specialist programs participated in the interviews with a mean age of 28.4 ± 5.4 years old; 15 nurses with a master of nursing specialist degree took part in the interviews with a mean age of 30.8 ± 3.2 years old and a mean working time of 6.2 ± 4.4 years.
Competency dimensions
The content analysis summarized six domains of nursing competencies for advanced practice nursing, including direct care practice competency, research competency, professional development competency, organization and management competency, mentoring and consultation competency, and legal/ethical practice (Table 2).
In phase 2: Delphi Process
After a series of iterations involving five members of our research team, six competency domains encompassing 70 items emerged.
Sociodemographic data of experts
In Phase 3, a total of 30 experts were initially invited, and 28 (93.3%) experts responded in the first round. The respondent rate in the second round was 100%. Table 3 displays the detailed information of the expert panels. Female experts accounted for the largest proportion (93%), with a mean age of 47.0 ± 6.7 years old. Over half of the experts had worked more than 20 years. Most of the experts served as supervisors for master’s or doctoral students (Table 3).
Reliability of experts
The authority coefficient (Cr), respondent rate, and Kendall’s coefficient of concordance (Kendall’ W) are usually used to evaluate the reliability of a Delphi approach [6, 25]. The content familiarity coefficient (Cs) and judgement coefficient (Ca) were 0.82 and 0.92, respectively. Therefore, the authority coefficient (Cr) was 0.87, which was acceptable. The response rate of both rounds was over 0.9, suggesting good initiative. The values of Kendall’s W were 0.296 and 0.178 for level 1 and level 2 items in the second round (p < 0.01), respectively.
The Core Competencies for APN
After two rounds of Delphi approaches, a consensual list of the core competencies for APNs was reached. For the six dimensions, 100% consensus was reached after modifying the description of the dimensions “Direct care practice” and “research” to “Direct clinical nursing practice” and “research and evidence-based nursing practice” (Table 4). Analysis of the importance score of competency citations by experts revealed that direct clinical nursing practice has more emphasis (Fig. 1).

Score on the six dimensions for APN
In the “direct clinical nursing practice” dimension, 6 items were modified and merged according to experts’ suggestions; 2 items that did not meet the selection criteria were deleted; and 1 new item proposed by experts was added. In the “research and evidence-based nursing practice” dimension, 3 items were merged, split, or modified, and 3 items that did not meet the item selection criteria were deleted. In the “professional development” dimension, 100% consensus was reached for all items. Regarding the “organization and management” dimension, 4 items that did not meet the item selection criteria were deleted, and 3 items were modified. Regarding the “mentoring and consultation” dimension, 2 items that did not meet the item selection criteria were deleted, and 1 item was split. In the “ethical and legal practice” dimension, only 1 item that did not meet the item selection criteria was deleted. Overall, 6 dimensions with 61 items remained (Table 4).
Discussion
The core competency framework with six domains and 61 items in this study provided evidence for the role development of APNs, which will prepare a cadre of nurses who have master’s degrees and are consistently ready to face health care delivery challenges and promote health. This study was a first attempt to define the scope of competency for APNs and may accelerate the maturation of the core competency framework for APNs in mainland China.
This study proposed an expert consensual list of the core competencies for APN, which contains six domains: direct clinical nursing practice, research and evidence-based nursing practice, professional development, organization and management, mentoring and consultation, and legal/ethical practice with 61 items. Compared to Hamric’s conceptual model and the ICN’s model, the core competency framework in this study had similar contents but also some differences.
The direct clinical nursing practice domain received the highest score among the six domains, as shown in Table 4, which indicated that providing clinical nursing care was the priority of nursing roles (Fig. 1). This finding was consistent with most previous studies [26, 27]. This domain consisted of patient-focused activities, including assessments, clinical nursing decision-making, nurse–patient relationship establishment and interpretation of data, which was consistent with previous studies [28, 29]. Nurse–patient relationships are critical to effectively implement nursing interventions [30]. The ability to establish therapeutic and collaborative nurse–patient relationships was also required in Hamric’s core competency model for APNs [8]. Comments about this domain led to the removal of ‘making a medical diagnosis’, ‘prescribing routine medications and routine examination for the patient’ as an activity, because nurse prescription has not yet been implemented widely in mainland China. If nurse prescription is widely allowed in the future, this activity should be included. Because nurse prescription has been an important responsibility to distinguish general nurses and nurses working in advanced positions in the USA. A total of 20 items were developed to describe the clinical nursing practice competency in detail.
The research and evidence-based nursing practice competency ranked second among all domains. This competency was also identified in some previous studies [31,32,33,34]. However, neither AMNC nor RCN is reflective of conducting research in their competency framework for APN [11, 12]. AACN only considered translating evidence to practice as a part of the core competencies without emphasizing the research ability of APN [9]. This discrepancy may result from the developing degree of nursing research between Western countries and China. The first master’s degree of nursing programme was not established until 1990 in China [35]. Although the enrolment of master of nursing specialist students has increased gradually since 2010, researchers, policy-makers, and educators think it is critical to have more expectations for the research competency of APNs to improve the nursing discipline in China. In this study, the 10 items in the dimension of research and evidence-based nursing practice pay more attention to the research on clinical problems and the translation of best evidence to clinical practice.
The third identified competency was professional development, which included the development of individuals and the nursing discipline. This confirmed previous results from Anna-Lena et al. [28] Krista et al. [27], and Finnbakk et al. [36]. With the development of health technologies, nurses are certainly required to keep up with the leading edge of specialized knowledge and new health care patterns. Moreover, advanced practice nurses are expected to take responsibility for the development of the nursing discipline. However, it may take a long time to make a difference in the acquisition of professional development competency.
Competency in organization and management was also required for APNs in this study. This competency contained two aspects: communicating and cooperating effectively with colleagues and participating in the organization and coordination of relevant elements of clinical nursing practice. This finding was slightly different from previous results, which only included collaborative or communicative ability [10, 28, 37] or only included mentoring and quality improvement activities [27, 32, 33]. Previous studies in China have found that communication is a time-consuming activity during the nursing process and directly relates to most conflicts and medical errors in the clinical environment [38, 39]. It was important for APN to conduct effective communication with patients, patients’ family members, and colleagues. The contents of this domain are more similar to professional leadership in Hamric’s advanced practice model.
This study also supported previous results, which stated that mentoring and consultation are required competencies for APNs [11, 32, 33, 40]. This competency generally involved health education to patients, professional guidance to peers, and specialized consultation to service subjects in this study, which was a complicated scenario to use clinical knowledge, learning principles, and education tools [41]. This domain covers a broad range of mentoring programs for patients, communities, clinicians, and students. However, the activity within this domain in our research included the large amount of “informal” teaching activities conducted by APN, similar to the result of Chang’s study [24]. It was critical to cultivate the mentoring and consultation competency of APNs to meet the demands of patients about disease management and health resource seeking as well as specialized issues from junior nurses [6].
The legal/ethical practice was another core competency identified in this study, which was rarely mentioned in most previous studies. Patient rights protection is a wide consensus around the world, and strengthening the occupational ethics and legal knowledge of nurses was proven to increase service quality and reduce medical disputes [42]. It is urgent to strengthen the ethical and legal practice competency of APNs in the complicated health environments of China [43].
This study identified some similarities with the competence framework of Hamric’s model, namely, six domains. However, there were several differences, such as the domain delineation and some items, due to the cultural and policy differences between China and Western countries. The engagement of stakeholders in all aspects of APN in this study was the distinguishing characteristic of this emerging field. This study also investigated the opinions of a heterogeneous sample, including nurses with master’s degrees, nursing managers and medical policymakers at multiple clinical sites, which helped to make the findings more reliable and generalizable.
Strengths, limitations and implications
The core competency framework for advanced practice nursing provided a benchmark in the implementation process of new advanced practice nursing roles in mainland China. The findings of this study may provide a framework for curriculum development and performance assessment in master of nursing specialist (MNS) education programe. Future research should focus on embedding these competencies in nursing curricula and how they impact patient outcomes.
This study explored the core competencies for APN in China. We recruited stakeholders including educators, employers, employees, nurses, and policy makers as participants, which provided rich perspectives of this issue. However, the gender of recruited participants disproportionately distributed because of the natural of nursing profession. In addition, in Phase 1, the participants mainly came from west China, which had a relatively lower economic and medical education level. These may affect the results in this study.
Conclusion
In this study, we identified six core competency domains required for APNs, including direct clinical nursing practice, research and evidence-based nursing practice, professional development, organization and management, mentoring and consultation, and ethical/legal practice. This competency framework can be used in competency-based education to cultivate advanced practice nurses to meet increasing nursing care needs. Additionally, this framework can be used for competency level assessment of APNs. A future study should examine how these competencies are incorporated into nursing curricula and how they affect patient outcomes.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy or ethical restrictions.
References
Goldsberry JW. Advanced practice nurses leading the way: Interprofessional collaboration. Nurse Educ Today. 2018;65:1–3.
Parker JM, Hill MN. A review of advanced practice nursing in the United States, Canada, Australia and Hong Kong Special Administrative Region (SAR), China. Int J Nurs Sci. 2017;4(2):196–204.
Hameic AB, Tracy, MF. Hamric and Hanson’s Advanced Practice Nursing: an Integrative Approach(6th ed ed). St. Louis, Missouri: Elsevier/Saunders, 2019.
International Council of Nurses. Guidelines of advanced practice nursing. 2020. Retrieved 05/22 from https://www.icn.ch/system/files/documents/2020-04/ICN_APN%20Report_EN_WEB.pdf.
Bryant-Lukosius D, Spichiger E, Martin J, Stoll H, Kellerhals SD, Fliedner M, De Geest S. Framework for evaluating the impact of advanced practice nursing roles. J Nurs Scholarsh. 2016;48(2):201–9.
Ren H, Liu C, Wang R, Zhang M, Li L. Core competencies required for gastroenterology nursing specialists in China. Gastroenterol Nurs. 2020;42:2.
Li Y, Lu H, Zhao Y, Ren L, Cao L, Pang D, Wang A. Core competencies of the midwifery workforce in China: a scoping review. J Nurs Manag. 2022;30(2):535–58.
Hamric AB, Hanson CM, Tracy MF, O’Grady ET. Advanced practice nursing: an integrative approach (5th ed ed). St. Louis, MO: Elsevier Health Sciences; 2014.
American Association of Colleges of Nursing. The Essentials of Master’s Education in Nursing. 2011. Available from: https://www.aacnnursing.org/Portals/42/Publications/MastersEssentials11.pdf.
Canadian Nurses Association, C. Canadian Nurse Practitioner: Core Competency Framework. 2010.Available from: https://www.cna-aiic.ca/-/media/cna/page-content/pdf-en/6---competency_framework_2010_e.pdf.
Gardner G, Carryer J, Dunn S, Gardner A. Nurse practitioner standards project: report to the Australian Nursing & Midwifery Council. 2004.
Royal College of Nursing. Advanced Level Nursing Practice Section 2: Advanced level nursing practice competencies. 2018. Available from https://www.rcn.org.uk/professional-development/publications/pub-006896.
Wong FKY. Development of advanced nursing practice in China: act local and think global. Int J Nurs Sci. 2018;5(2):101–4. https://doi.org/10.1016/j.ijnss.2018.03.003.
Guo HX, Li JP. Status of research on the advanced practice nurses role in China. Chin J Modern Nurs. 2023;29(6):827–34. https://doi.org/10.3760/cma.j.cn115682-20220726-03617.
Jokiniemi K, Pietilä AM, Kylmä J, Haatainen K. Advanced nursing roles: a systematic review. Nurs Health Sci. 2012;14(3):421–31. https://doi.org/10.1111/j.1442-2018.2012.00704.x.
Skills for health. Key elements of the career framework. 2010. Available from: http://www.skillsforhealth.org.uk/resources/guidance-documents/163-keyelements-of-the-career-framework.
Zhao YY, Ding Y, Pang D, Yang P, Jin SL, Lu Q. Building core competency framework of oncology advanced practice nurse (Original work published in Chinese). Chin Nurs Manag. 2011;11(8):27–30. https://doi.org/10.3969/j.issn.1671-315X.2011.06.004.
Zhong YP, Lu HJ, Xia HO, Jiang H. Study of Training Goals of ICU Advanced Practice Nurse. Nurs J Chin People’s Lib Army. 2013;30(4):9–12. https://doi.org/10.3969/j.issn.1008-9993.2013.04.003.
Gu CY, Li LL, Ding Y, Zhu XL, Xin SC, Wang XH. Job analysis and needs assessment of advanced midwifery practitioners in the hospital. Chin J Hosp Adm. 2016;32(7):534–8. https://doi.org/10.3760/cma.j.issn.1000-6672.2016.07.019.
Hsieh HF. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88. https://doi.org/10.1177/1049732305276687.
Chan ZCY. A qualitative study on communication between nursing students and the family members of patients. Nurse Educ Today. 2017;S0260691717302046. https://doi.org/10.1016/j.nedt.2017.08.017.
Lc A, Yw A, Sw B, Hz A, Cz A. Construction of evidence-based practice competencies for nurses in China: a modified Delphi study. Nurse Educ Today. 2021;102:104927. https://doi.org/10.1016/j.nedt.2021.104927.
Zeng G. Modern epidemiological methods and applications. Beijing: Beijing Medical University and China Medical University; 1994. p. 250–70.
Chang AM, Gardner GE, Duffield C, Ramis MA. A Delphi study to validate an Advanced Practice Nursing tool. J Adv Nurs. 2010;66(10):2320–30. https://doi.org/10.1111/j.1365-2648.2010.05367.x.
Chen F, Leng Y, Wang Y, Li J, Hematology DO. Construction of the scheme of specialty nurse training program using the Delphi method. J Nurs Sci. 2015;30(1):44–8. https://doi.org/10.1016/S2155-8256(15)30380-X.
Akamine I, Uza M, Shinjo M, Nakamori E. Development of competence scale for senior clinical nurses. Jpn J Nurs Sci. 2013;10(1):55–67. https://doi.org/10.1111/j.1742-7924.2012.00210.x.
Krista J, Riitta M, Anna-Maija P. Constructing content validity of clinical nurse specialist core competencies: exploratory sequential mixed‐method study. Scand J Caring Sci. 2018;1–9. https://doi.org/10.1111/scs.12588.
Anna-Lena N, Bodil M, Lisbeth F. Advanced practice nurses’ scope of practice: a qualitative study of advanced clinical competencies. Scand J Caring Sci. 2011;25(4):661–70. https://doi.org/10.1111/j.1471-6712.2011.00876.x.
Nieminen AL, Mannevaara B, Fagerström L. Advanced practice nurses’ scope of practice: a qualitative study of advanced clinical competencies. Scand J Caring Sci. 2011;25(4):661–70. https://doi.org/10.1111/j.1471-6712.2011.00876.x.
Feo R, Rasmussen P, Wiechula R, Conroy T, Kitson A. Developing effective and caring nurse-patient relationships. Nursing Stand. 2017;31(28):54–63. https://doi.org/10.7748/ns.2017.e10735.
Mick DJ, Ackerman MH. Advanced practice nursing role delineation in acute and critical care: application of the strong model of advanced practice. Heart Lung. 2000;29(3):210–21. https://doi.org/10.1067/mhl.2000.106936.
Sastre-Fullana P, Morales-Asencio JM, Sesé-Abad A, Bennasar-Veny M, Fernández-Domínguez JC, De Pedro-Gómez J. Advanced Practice Nursing Competency Assessment Instrument (APNCAI): clinimetric validation. BMJ Open. 2017;7(2):e013659. https://doi.org/10.1136/bmjopen-2016-013659.
Vaska M, Lori K, Sonia S, Virginia M, Cindy S, Linda B, Lexie K. University Health Network framework for advanced nursing practice: development of a comprehensive conceptual framework describing the multidimensional contributions of advanced practice nurses. Nurs Leadersh (Tor Ont). 2004;17(3):52–64. https://doi.org/10.12927/cjnl.2004.16231.
Zahran Z, Curtis P, Lloyd-Jones M, Blackett T. Jordanian Perspectives on Advanced Nursing Practice: An Ethnography. Int J Nurs Rev. 2012;59(2):222–9.
Ge S, Xi X, Guo GF. A systematic review of the impact of master’s-educated nurses on inpatient care. Int J Nurs Sci. 2015;2(4):414–21. https://doi.org/10.1016/j.ijnss.2015.10.003.
Finnbakk E, Wangensteen S, Skovdahl K, Fagerström L. The Professional Nurse Self-Assessment Scale: Psychometric testing in Norwegian long term and home care contexts. BMC Nurs. 2015;14(1):59. https://doi.org/10.1186/s12912-015-0109-3.
Darmody JV. Observing the work of the clinical nurse specialist. Clin Nurs Spec. 2005;19(5):260–8. https://doi.org/10.1097/00002800-200509000-00010.
Chen YY, Liu YH, Bin J, Ren XY, Liu WZ. Analyze the effect of therapeutic communication in clinical nursing: a review of recent 20 years literatures (Original work published in Chinese). J Nurs. 2014;13:970–2.
Zhu QM, Du L, Liu LY. Analysis of influencing factors of hospital nursing safety and management countermeasures (Original work published in Chinese). Chin Hosp Manag. 2013;7:71–2. https://doi.org/CNKI:SUN:YYGL.0.2013-07-038.
Kirk H. The role of advanced nursing practice in occupational health. Occup Med (Oxford, England). 2012;62(7):574–7. https://doi.org/10.1093/occmed/kqs144.
Bissett KM, Cvach M, White KM. Improving competence and confidence with evidence-based practice among nurses: outcomes of a quality improvement project. J Nurses Prof Dev. 2016;32(5):248–55. https://doi.org/10.1097/nnd.0000000000000293.
Hariharan S, Jonnalagadda R, Walrond E, Moseley H. Knowledge, attitudes and practice of healthcare ethics and law among doctors and nurses in Barbados. BMC Med Ethics. 2006;7:E7. https://doi.org/10.1186/1472-6939-7-7.
Lancet T. Violence against doctors: Why China? Why now? What next? Lancet. 2014;383(9922):1013–1013. https://doi.org/10.1016/S0140-6736(14)60501-8.
Acknowledgements
The authors thank all the content experts and nurses for their indispensable contribution to this study.
Funding
This work was supported by the West China Nursing Discipline Development Special Fund Project, Sichuan University (grant number HXHL21003), and project of Technology and Training of Sichuan Province under grant number 2021JDKP0043.
Author information
Authors and Affiliations
Contributions
Study conception and design,HXG, JPL. Data collection,WZ, HXG. Data analysis and interpretation,WZ, HXG. Drafting of the article,WZ, HXG. Critical revisions of the article,WZ, JPL. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was performed in line with the principles of the Declaration of Helsinki and its later amendments or comparable ethical standards. We got informed consent from all the participants before taking the survey in the study. Approval for the study was granted by the Ethics committee of West China Hospital, Sichuan University (ID: 2017–177).
Consent for publication
Not applicable
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Guo, H., Zhu, W. & Li, J. Developing a core competency framework for advanced practice nursing in mainland China: a sequential exploratory study. BMC Nurs 22, 179 (2023). https://doi.org/10.1186/s12912-023-01335-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-023-01335-4