
Abstract
The need for equitable access to primary healthcare services in the current global context has attracted widespread attention, prompting nations to continuously enhance their grassroots medical service levels. In response, China launched the "Healthy China" initiative, which prioritizes the enhancement of national health as a core goal of the healthcare system and uses this opportunity to deepen reforms aimed at strengthening primary care. However, in remote and rural areas, the optimization of medical resource allocation and the achievement of balanced service development remain critical challenges owing to limited resources. This study selected Liannan Yao Autonomous County, which is situated in the northwestern corner of Guangdong Province, as a case study due to its remote mountainous location, underdeveloped economy, and minority region characteristics. Through field research and interviews, this study thoroughly explored the needs of both supply and demand, factoring in elements such as the service capability of healthcare facilities and residents' travel thresholds to enhance the two-step floating catchment area model, thus making it more applicable to remote villages. By integrating electric bikes and cars, which are the primary means of transportation in rural areas, this study conducted a thorough analysis and comparison of the accessibility of medical services in Liannan Yao Autonomous County (Liannan County) . The results reveal significant disparities in healthcare accessibility, an uneven distribution of medical resources, and varying impacts of transportation conditions and facility service capabilities on accessibility. Notably, the study revealed that improving transportation conditions alone has limited effects in rural areas; the key lies in balancing medical service capabilities and the rationality of overall layouts. From the perspectives of equity and efficiency, this study employs the equitable coverage model and the efficiency-driven model to construct two scenarios, comparing accessibility changes in Liannan County under both conditions and proposing strategies to improve the spatial layout of local healthcare facilities. This research not only deepens the understanding of healthcare service accessibility in rural areas but also provides a scientific basis for optimizing resource allocation and enhancing primary medical services, offering valuable guidance and reference for Liannan County and other similar rural regions.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
In the current global context, there is a growing recognition of the significance of primary health care, now a shared focus among countries. Various nations have implemented measures to provide high-quality and inclusive primary health care services aimed at safeguarding the health and well-being of their populations [1]. In 2015, the WHO released a draft for consultation on the WHO Framework on Integrated People-Centred Health Services [2], which outlined a global strategy to strengthen health systems through more integrated, people-focused health services. In line with this, China introduced the national strategy "Healthy China", primarily aimed at enhancing the overall health of its citizens [3]. This strategy initiated comprehensive reforms of the healthcare system, particularly emphasizing the strengthening of primary health care services. However, China currently faces challenges in terms of the distribution and allocation of healthcare resources, with only about 30% of these resources being available in towns and townships, and even fewer in remote and rural areas [4]. Addressing these issues and find solutions to optimize resource allocation and enhance the quality and efficiency of medical services are crucial, especially given the limited availability of resources.
Against this background, research on the accessibility of healthcare facilities has become a crucial approach to addressing this issue [5]. The accessibility of healthcare facilities is not only directly related to the health status of residents but also serves as an important indicator for measuring social welfare and equity in a region [6]. In recent years, with the rapid development of Geographic Information System (GIS) technology, research on the accessibility of healthcare facilities has deepened, focusing on several key aspects [7]. Firstly, in terms of concepts and definitions, accessibility, as a spatio-temporal concept, reflects the ease or difficulty of overcoming various barriers to communication between a starting point and an endpoint in space and time, while also emphasizing the interconnection and interaction among all elements. Since Hansen first introduced the concept of accessibility in 1959 [8], its meaning has been continuously enriched. For example, Penchansky and Thomas (1981) broke down the broad and somewhat vague concept of accessibility into five dimensions: accessibility, availability, acceptability, affordability, and accommodation [9]. Khan categorized accessibility into two primary dimensions: potential and revealed (or realized). Each of these dimensions is further divided into spatial and aspatial aspects, resulting in four categories of accessibility [10]. Although spatial accessibility has long been the core of research, recent years have seen a gradual increase in studies focusing on non-spatial factors, greatly enriching the meaning and application scope of accessibility [11].
Secondly, in terms of research methods and application models, researchers have introduced various innovations and improvements based on classical models. They have refined and adjusted their approaches to accommodate different groups, research unit scales, modes of transportation, time factors, and types and levels of healthcare facilities [12]. Common methods for measuring spatial accessibility include the provider-to-population ratio (PPR), distance to the nearest provider, average distance to a group of providers, and gravity models [13,14,15,16,17]. Among these, the two-step floating catchment area (2SFCA) method is the most commonly used approach [1, 24], and it has been chosen for this study. The 2SFCA method was initially proposed by Radke et al [18] and later refined and formally named by Luo et al. [19, 20]. Its ease of understanding and operability has led to widespread attention and development [21,22,23], culminating in various extended formulas such as the enhanced 2SFCA[25], Gaussian 2SFCA [26], kernel density 2SFCA [27], and gravity 2SFCA [28]. The improvement of these models and the integration of multi-source data have significantly enhanced research accuracy and expanded their application scenarios [29].
Furthermore, key factors influencing the accessibility of healthcare facilities have been extensively explored. Factors such as population density, the distribution of medical resources, transportation convenience, quality of medical services, and socioeconomic status all profoundly impact the distribution of healthcare resources and residents' convenience in seeking medical care [31]. In-depth research into these factors contributes to a comprehensive understanding of the current state and challenges related to healthcare facility accessibility [32].
However, despite significant progress in the three areas mentioned above, the strategies and recommendations for improving healthcare facility accessibility remain relatively underdeveloped. Current research primarily focuses on status analysis and problem diagnosis, with a greater need for specific improvement strategies. Future studies should focus more on integrating interdisciplinary knowledge and combining it with practical applications.
It is worth noting that existing accessibility studies are mostly concentrated in developed coastal cities and plain areas, with insufficient attention to remote rural and mountainous regions [33]. Current research is largely limited to the analysis of geographical data and lacks in-depth investigation and consideration of actual conditions. Although the amount of data for rural areas is not large, the real-life complexity and limited availability of online information necessitate using surveys and interviews to study these regions. This approach ensures that the parameters in accessibility evaluation models align more closely with the actual conditions of remote and rural areas, reflecting the primary goal of this study.
Moreover, most existing studies assume that residents rely on a single mode of transportation to access healthcare facilities. This study examines cars and electric bikes—the two most common means of transportation in rural southern China—and analyzes their impact on the accessibility of medical services. It then uses the results of this accessibility evaluation to propose effective recommendations for optimizing the layout of healthcare facilities, representing another innovative effort by this research.
Simultaneously, to address the shortcomings of existing research in providing strategies and recommendations for improving healthcare facility accessibility, this study expands further in this direction. By designing and constructing different development scenarios, this study simulates various resource allocation schemes to predict and evaluate the effects of policy interventions.
In summary, this study has three objectives: (1) To adopt both quantitative analysis and social surveys based on the unique context of remote rural areas and from both the supply and demand perspectives, comprehensively considering factors such as the service capacity of healthcare facilities and residents' travel thresholds, and to improve the accessibility model to more accurately reflect and be applicable to the actual conditions of remote rural areas; (2) To explore the spatial differences in the accessibility of medical resources in Liannan County based on various modes of transportation and healthcare service thresholds, and to analyze the impact of transportation and service capabilities on accessibility through comparative analysis; (3) To design and construct two scenarios based on the current development and future trends of Liannan County, determining which strategy more effectively enhances the accessibility of medical resources through comparative analysis. Based on these findings, targeted strategies and recommendations are proposed to support decision-making for improving the spatial layout of local healthcare facilities. This research not only seeks to increase the standard of medical services in the rural areas of Liannan County, enhancing convenience and efficiency for local residents, but also aims to provide valuable insights for the development of rural healthcare in other similar regions.
Methods and data sources
This article examines Liannan County in China as a case study utilizing the gravity-based two-step floating catchment area (2SFCA) method for assessing accessibility. In presenting the results of the accessibility assessment, the inverse distance weighting interpolation technique is utilized for grading [35]. Subsequently, based on the accessibility outcomes and their distribution characteristics, two scenarios were designed: one for balanced coverage and the other for enhancing a single core. Correspondingly, the maximization coverage model and the core service capability enhancement calculation are employed to simulate changes in accessibility. This targeted approach proposes optimization strategies for improving medical services in Liannan County (Fig. 1).

Method workflow
Study area
This study focuses on Liannan County, located in Qingyuan city, Guangdong Province, in the northwestern corner of the province. It is among the least economically developed counties in Guangdong Province (Fig. 2). Geographically, it spans from 24°17′16″N to 24°56′2" N in latitude and from 112°2′2″E to 112°29′1" E in longitude. The county administers seven towns—Sanjiang, Sanpai, Zhaigang, Daping, Xiangping, Guoshui, and Damaishan-which comprise 69 administrative villages and 2 communities, totaling 71 residential demand points. In 2022, the county had a total population of 177,521, with more than half comprising the Yao ethnic group. More than 88% of the county's area is mountainous, featuring 161 high mountains exceeding 1000 meters in altitude (Fig. 3). Many residents, especially those from the Yao community, maintain the traditional habit of living in mountainous areas, which results in inconvenient transportation for many residential areas (Fig. 4). The county experiences a high degree of aging, with 16.74% of the population aged 60 and above. The distributions of the population density and healthcare facilities within the region are illustrated in Table 1 and Fig. 2, respectively.

Location map and distribution of population and healthcare facilities in Liannan County

Typical terrain of Liannan County

Typical Yao ethnic village in Liannan County
The selection of Liannan County as the focus of this study is based on three main considerations: (1) Liannan County, located in the remote mountainous area of northwestern Guangdong Province, is a typical representative of remote and rural areas.Its unique geographical location and socioeconomic conditions provide a rare case study for researching healthcare accessibility in remote, rural areas. As a region predominantly inhabited by ethnic minorities, Liannan County also faces the challenge of an aging population, making the study of healthcare services in this area more relevant and urgent; (2) Liannan County not only represents remote areas but also reflects the general insufficiency of healthcare resources in rural China, particularly regarding their uneven distribution. This imbalance is especially pronounced in Liannan County, making it an ideal subject for studying healthcare resource allocation in remote and rural areas. This research will conduct a thorough investigation and analysis of data to examine healthcare accessibility and resource allocation issues in this typical area in depth; (3) Against the backdrop of China's ongoing healthcare reform and the implementation of the "Healthy China" strategy, Liannan County, a remote mountainous area that has achieved significant success in healthcare service reform, provides valuable empirical evidence for this study. By taking Liannan County as a representative of remote and rural areas, this study delves into its healthcare accessibility. This approach not only helps improve the quality and accessibility of healthcare services in the local area and other similar remote rural regions but also offers valuable experiences and insights for healthcare reform and resource allocation in remote rural areas globally.
The distribution of medical resources in China is uneven, with significant disparities between rural areas and cities. Cities have ample medical resources, while rural areas are relatively underserved. In rural areas of China, the healthcare system operates as a three-tiered medical service system comprising county hospitals, town health centers (THCs), and village clinics [34]. China has not yet established a comprehensive hierarchical medical system, permitting residents to seek treatment at any level of medical institution when ill. County hospitals typically represent the highest level of medical care in a county, and many residents, particularly those living nearby, choose to go directly to them. THCs serve as hubs of rural medical network services, providing primary healthcare and public health services while also overseeing and managing village clinics. Every village in Liannan County has a health room, usually within a 15-minute walk, thereby offering good accessibility with little variation among villages. These village health rooms, with their basic equipment, cater to minor ailments of local residents, who generally visit town health centers or the Liannan County People's Hospital for more serious conditions. Hence, this study exclusively focused on the 8 THCs and 1 county hospital in Liannan County, excluding village health rooms. To facilitate the use of medical health facilities and residential demand point locations within geographic information systems(GIS), these locations were digitized into latitudinal and longitudinal points based on points of interest (POI).
Data collection
Population and healthcare-related data were obtained from the Liannan Yao Autonomous County Statistics Bureau and the Liannan Yao Autonomous County Health Bureau. To better understand the healthcare-seeking behavior of rural residents and the practices of doctors, a survey was designed for this study. The survey consisted of two parts: 218 questionnaires for local residents and 42 for healthcare professionals, aiming to gather their opinions and insights. A total of 270 questionnaires were distributed (see Supplementary Files 1 and 2), with 260 valid responses received, resulting in a response rate of 96%. The survey participants comprised local residents and healthcare personnel. Residents were required to be at least 18 years old and to have lived in Liannan County for more than one year. Healthcare personnel comprised doctors, nurses, and other medical staff who had been working in various medical institutions in Liannan County for more than six months. This study employed a random sampling method, with the number of questionnaires distributed controlled according to the population proportion of each town, ensuring that the collected data adequately represented the actual situation of the area.
Gravity-based two-step movement search method
Overall model
In the traditional 2SFCA method, the first step entails establishing a healthcare supply point \(j\) as the center and utilizing a service threshold \({d}_{0}\) as the radius to delineate the catchment area for that supply point. All demand points \(k\) within this catchment area are then identified and analyzed to calculate the supply-demand ratio \({R}_{j}\) for supply point \(j\). In the second step, attention shifts to demand point \(i\). Using the same service threshold \({d}_{0}\) as the service radius, this phase involves calculating the sum of the supply-demand ratios \({R}_{j}\) within the radius of the demand point. This sum determines the accessibility \({A}_{i}\) at demand point \(i\). The formula is as follows:
Where \(i\) represents the demand point; \(j\) represents the supply point;\({A}_{i}\) represents the accessibility of demand point \(i\) calculated based on the 2SFCA method; \({d}_{ij}\) represents the distance between demand point \(i\) and supply point \(j\); \({R}_{j}\) represents the ratio of the facility size of supply point \(j\) to the population served within the search radius (\({d}_{0}\)); \({S}_{j}\) represents the supply size of supply point \(j\); \({P}_{k}\) represents the demand size of demand point \(k\) [36].
The gravity-based 2SFCA method applies the distance decay function of the gravity model within the search domain of the 2SFCA method, thereby transforming the discrete distance decay function into a continuous one [19, 30]. When the distance is short, accessibility decreases rapidly; as the distance increases, the rate of decline slows, aligning better with the actual conditions of the study area. The formula for the gravity-based 2SFCA method can be expressed as follows, incorporating the decay function into the basic formula (1):
where \({A}_{i}\) represents the accessibility of demand point \(i, f({d}_{ij})\) is the distance decay functions, and \(\upbeta\) is the distance decay parameter.
Evaluation of the service capacity of healthcare facilities \({S}_j\)
Past studies have typically relied on a single indicator to evaluate the service capacity \({\text{S}}_{\text{j}}\) [37, 38] of healthcare facilities, thus failing to capture the variability in service capabilities based on the actual conditions of rural areas. This study initially conducted field observations and questionnaires to collect indicators that represent the service capabilities of healthcare facilities and are in line with the current national medical reform and development trends. For example, indicators such as the number of medical visits and number of patients under family doctor contracts reflect a significant portion of a rural doctor's regular duties. After collecting a set of indicators, these indicators were refined based on data availability and consultations with healthcare professionals. Given the requirements of the SPSS factor analysis, which stipulates that the number of indicators must not exceed the number of supply points, the final selection comprised seven indicators of healthcare service capacity, as listed in Table 2.
After integrating all the indicator data into the raw dataset, Kaiser–Meyer–Olkin (KMO) and Bartlett's tests were performed to determine whether the original variables were suitable for factor analysis. Generally, a KMO measure above 0.5 and a Bartlett's test p value below 0.05 indicate that factor analysis is appropriate. The results, as shown in Table 3, confirm that the factor analysis is appropriate.
Based on eigenvalues greater than 1 and a cumulative contribution rate exceeding 85%, two common factors, F1 and F2, were extracted from the seven evaluation variables; these factors are stastistically independent. The cumulative contribution rate of 99.117% demonstrated that the two extracted factors accounted for 99.117% of the variance in the original seven healthcare service capability indicators, providing a comprehensive explanation of the raw data. The factor loading matrix underwent orthogonal rotation, and the factors were subsequently named and interpreted. As shown in Table 4, variables such as the number of beds, number of practicing physicians, number of medical treatments in 2022, number of nurses, other medical technicians, and number of hospitalizations in 2022 exhibit high loadings on Factor F1, which is interpreted as the level of comprehensive medical resources. This factor had the largest variance contribution rate at 82.311%, indicating that it was the primary influencing factor. The number of family doctor contracts displays a high loading on Factor F2, while the number of nurses also demonstrates a smaller positive correlation with F2, interpreted as primary healthcare service management. This factor contributed 16.806% of the variance, making it a secondary influencing factor.
Finally, to accurately analyse the medical service capabilities of the eight healthcare facilities, the original data were entered into the formula derived from the factor score coefficients, as detailed in Table 5. Weighted calculations are then conducted using the following factor score functions for Factors F1 and F2:
By utilizing these factor score functions for weighted calculation, comprehensive scores \({S}_{j}\) representing the service capabilities for each healthcare facility were derived, as presented in Table 6.
Selection of the distance decay coefficient value \(\beta\)
The distance decay coefficient \(\upbeta\) reflects the pattern by which the influence between demand points and supply points diminishes as distance increases. The selection of \(\upbeta\) significantly impacts the outcomes of the gravity-based 2SFCA method. Ideally, this value should be derived from a regression analysis of a large dataset that considers various conditions at supply points. However, the required volume of data for practical verification is substantial, and the associated costs are high, making implementation challenging. According to the literature, the range of values for \(\upbeta\) varies between 0.9 and 2.29 [39,40,41,42], with common practice setting it at 1.0, 1.2, 1.5, 1.8, or 2.0 [43,44,45,46,47]. To determine the most suitable value, this study conducts a gravity-based 2SFCA model simulation for each of these five values. The travel background is set as car trips, with a healthcare service threshold of 90 minutes, as longer car travel times can better reflect changes in \(\upbeta\). Finally, the accessibility statistics for different values of are compared to determine the most appropriate value for calculating the accessibility of healthcare facilities in Liannan County (see Table 7).
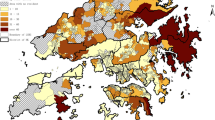
As shown in Fig. 5, as the value of \(\upbeta\) increases, the high-accessibility areas in Liannan County expand gradually, while the low-accessibility areas shrink correspondingly. This change is particularly evident in the northern and southern peripheral regions of the county. These geographically remote areas, which lack healthcare resources, are more sensitive to changes in the \(\upbeta\) value. In contrast, in the central part of the county, where healthcare facilities are relatively concentrated and residents have more access to medical services, the response of accessibility to changes in the β value is more gradual. Additionally, we conducted an accessibility analysis based on minimum impedance during the study, but due to space limitations, it is not detailed in this paper. This analysis further highlights the significant impact of road distance on motor vehicle travel accessibility. In Liannan County, road conditions directly affect the speed and ease with which residents can reach healthcare facilities. Considering this practical situation, we selected a relatively larger β value to ensure that the accessibility assessment accurately reflects the impact of road distance on accessibility. By comparing the visualized spatial distribution of accessibility under different \(\upbeta\) values, we found that when \(\upbeta\)=1.8, the accessibility assessment results best match the actual conditions. This conclusion is supported not only by the intuitive observation of spatial distribution but also by statistical data analysis. Therefore, we chose β=1.8 as the appropriate distance decay coefficient for assessing healthcare accessibility in Liannan County.

Spatial distribution map of accessibility with different \(\upbeta\) values
Traffic data
Traffic speed
The survey results indicated that electric bikes and cars are the most common means of transport for rural residents seeking medical care. The shortest travel times from healthcare facilities to administrative villages, and vice versa, can be calculated using the origin-destination (OD) cost matrix function in the network analyst extension and the built-in calculator in GIS.
The basic transportation data for Liannan County, including highways and primary, secondary, tertiary, and quaternary roads, were obtained from the National Geomatics Center of China and digitized in accordance with the requirements of the GIS network model. Based on actual road conditions and the speed regulations for different road types as stipulated in China's "Highway Route Design Regulations" (JTG D20-2017) [48], the simulated driving speeds in GIS are detailed in Table 8.
Estimation of healthcare service threshold values
In the survey, the thresholds for acceptable travel time to County People's Hospital and THCs were established at intervals of less than 30 minutes, 30 minutes, 45 minutes, 60 minutes, and more than 90 minutes. The majority of respondents selected "30 minutes" and "over 90 minutes" (Fig. 6). Consequently, this study determined the search radius to be 30 minutes and 90 minutes.

Proportional distribution of residents' willingness regarding travel time to different healthcare facilities
Maximized coverage model
During the layout optimization simulation, the Maximization Coverage Model is employed. This model focuses on selecting a specified number of facility locations from a set of potential candidate sites, ensuring that each is strategically placed within the required service radius of the facilities. The primary goal of the maximization coverage model (maximum covering location problem) is to maximize the coverage of facilities. Concerning the distance from demand points to healthcare facilities, the model assumes that any demand point within the service radius receives adequate services. The formulas are as follows:
Where i represents the set of demand points; j represents the set of candidate points; m represents the total number of demand points; n represents the total number of candidate points; p represents the total number of facility points; d represents the distance from demand point i to supply point j; s represents the defined service radius; \({x}_{j}\) is the location variable, indicating whether a healthcare facility is established at candidate point j (if established, \({x}_{j}\)=1; otherwise, \({x}_{j}\)=0); \({y}_{i}\) is the allocation variable, indicating whether demand point i receives service from a community health service center (if received, \({y}_{i}\)=1; otherwise, \({y}_{i}\)=0). The variable \({y}_{j}\) indicates whether candidate point j is selected as a healthcare facility point (if selected, \({y}_{j}\)=1; otherwise, \({y}_{j}\)=0).
Where i represents the set of demand points; j represents the set of candidate points; p represents the total number of facility points; d represents the distance from demand point i to supply point j; s represents the designated service radius; and \({x}_{j}\) is the location variable indicating whether a healthcare facility is established at candidate point j. If established, \({x}_{j}\)=1; otherwise, \({x}_{j}\)=0; and \({y}_{i}\) is the allocation variable indicating whether demand point i accepts services from the community health service center. If accepted, \({y}_{i}\)=1; otherwise, \({y}_{i}\)=0.
Results
Results of overall accessibility
Figure 7 illustrates the spatial distribution of healthcare service accessibility via electric bikes, while Fig. 8 depicts accessibility via cars. The "Inverse Distance Weighting (IDW)" method in GIS classifies accessibility scores into nine levels, with each cell shaded in a different color according to its level. In ArcGIS, the "Inverse Distance Weighting (IDW)" method was used to classify accessibility scores into nine levels, with higher levels indicating better accessibility. Each cell is colored differently according to its level. Within this classification framework, Level 5 represents a relatively balanced state, indicating a medium level of healthcare service accessibility—neither the best nor the worst. This middle level reflects the current situation in Liannan County, where healthcare facilities are limited and unevenly distributed. Therefore, Level 5 can be considered representative of the overall average level of healthcare service accessibility in the region, providing a relatively objective benchmark for evaluation.Although the absolute values in each figure differ, our analysis does not directly compare the specific values of Level 5 in each figure, but rather focuses on their relative positions and meanings across the figures. This approach provides a simple and clear framework for comparison, particularly when basic parameters (such as geographical location, traffic conditions, etc.) are consistent. Adjusting certain parameters (such as service capacity or thresholds) allows for an intuitive observation of the impact of changes in accessibility. Thus, despite the differences in specific values between the figures, this classification method enables a clear comparison of accessibility changes under different scenarios, making horizontal comparisons more straightforward.

Spatial distribution of healthcare service accessibility by electric bike. a 30 min. b 90 min

Spatial distribution of healthcare service accessibility by car. a 30 min. b 90 min
The adopting of a nine-level classification is primarily based on the unique terrain and distribution characteristics of medical resources in Liannan County. In previous studies, classifications exceeding six levels are rare. However, in this study, due to the relatively dispersed distribution of healthcare facilities in Liannan County, it was found through experimentation that dividing accessibility into nine levels more clearly reveals the differences and contrasts between regions, making the trends more evident. This refined classification method not only improves the resolution of the analysis but also significantly enhances the scientific validity and comparability of the research results.
Table 9 details the proportion of healthcare services accessible to residents within different thresholds in Liannan County and the percentage of healthcare facilities throughout the county meeting or exceeding Level 5 accessibility standards. Regardless of the mode of transportation or threshold setting, the proportion of areas in Liannan County achieving above Level 5 is less than 60%, with minimal differences among the four modes of transportation, indicating that the impact of transportation modes on accessibility is relatively limited.
The results revealed a significant disparity between the maximum and minimum values of accessibility within Liannan County, underscoring substantial inequalities in healthcare service accessibility across the region and an uneven distribution of medical resources. Accessibility declines from the central part of the county towards the southwest, exhibiting distinct north‒south and east‒west gradients. The northern and eastern parts of the county demonstrate notably better accessibility compared to the southern and western areas, indicating a more adequate distribution of medical and healthcare facilities in these regions.
The impact of transportation
Extending travel distances with electric bikes has a negligible impact on enhancing accessibility, particularly in regions that are initially the most underserved. These areas, notably the northwestern part of the county, which includes sections of three towns, and the southern area of Damaishan Town, are characterized by low population density, considerable distances between healthcare facilities, substandard medical service capabilities, and limited coverage. Consequently, residents frequently must traverse significant distances within the county to access treatment from hospitals with superior service capabilities. Even after extending the threshold to 90 minutes, no noticeable improvement was observed in these highly underserved areas. Instead, the area of poor accessibility expanded, extending beyond the regions previously calculated for a 30-minute travel time. This demonstrates that increasing the travel distance for electric bikes fails to enhance accessibility in the most disadvantaged areas.
Regarding sensitivity to threshold changes—specifically, the difference in calculated results before and after adjustments in the threshold—electric bikes surpass conventional cars within a certain range. However, beyond a specific threshold, electric bikes prove less effective than conventional cars. A comparison of four maps reveals that within the town domain, the differences in simulated travel outcomes for electric bikes are significant; however, beyond the town domain—especially across two towns—the variations in conventional car travel simulations become considerably more pronounced, particularly in the county’s most peripheral areas.
The impact of service capability
The imbalance in regional accessibility significantly impacts the area and does not necessarily improve with increased travel distances. In this study, changes in the threshold demonstrated polarization in geographic areas, typically causing further deterioration in worse-off areas, while better-served areas improved. The top four healthcare facilities ranked by service capability are all located on the eastern side of the county, resulting in Xiangping Town on the far west becoming the area most affected by the uneven distribution of medical services. The superior medical services accessible to Xiangping Town are the farthest away, so even with an increased threshold, the accessibility around the Xiangping Health Center remains the worst. In contrast, the area around the Zhaigang Health Center on the eastern side consistently boasts the greatest accessibility, which further increases with increasing threshold. This underscores the critical importance of balancing regional service capabilities.
From the maps, the certian areas exhibit a clear improvement in accessibility with increased thresholds, while others experience a reduction in accessibility levels due to the higher threshold. The areas with significant improvements are those with access to the two most robust services—County People's Hospital and Zhaigang Health Center—particularly in Damaishan Town in the southern part of the county. Interviews conducted in Shangdong village and neighboring villages in Damaishan town revealed that with adequate transportation conditions, the majority of villagers opt to travel to the superior Zhaigang Health Center as travel distances increase. Therefore, with the increased service threshold, the accessibility rating for this area improved from Level 5 to Level 6 or higher, closely aligning with actual conditions. In areas where the accessibility rating decreased due to the increased threshold, the cause was exposure to lower-quality resources than before due to the expanded threshold, which lowered the average level of medical services and thus decreased the accessibility results accordingly.
Discussion
Based on the evaluation of accessibility using various thresholds and transportation methods, it is clear that in remote and rural areas, improvements in transportation alone have a limited effect on enhancing accessibility. Instead, the equitable distribution of medical service capabilities and the optimization of the overall spatial layout are crucial. Given these findings, this paper proposes two improvement scenarios tailored to the specific conditions in Liannan County. Considering the existing economic constraints, the likelihood of adding new healthcare facilities remains low. Therefore, under the premise of maintaining the current number of facilities, this study constructs two scenario simulations designed to explore strategies that enhance accessibility.
The first scenario prioritizes equity. This research identified significant impacts resulting from regional imbalances, necessitating county-wide consideration of balance. Field research has revealed that many health centers consider their locations to be suboptimal and express a desire to relocate. Thus, we use the maximal coverage model to simulate scenarios aimed at maximizing service coverage and fairness.
The second scenario emphasizes efficiency. From an accessibility perspective, the core parameters in the model are transportation and service capability. The proposed hypothesis is that concentrating limited financial resources on a particular medical facility could significantly enhance accessibility. According to previous measurements, Zhaigang and County People's Hospital exert the most substantial impact. Coupled with the county government's three-year development plan, which aims to further enhance the service capacity of Zhaigang Health Center, this facility was selected for the simulation to assess the strategy’s effectiveness.
Regardless of whether they travel by electric bikes or cars, residents can reach at least one healthcare facility within 90 minutes. Therefore, regarding optimization adjustments, we focus solely on ensuring that residents can access at least one primary healthcare service within a 30-minute service radius.
Optimization of the maximum coverage model
To enhance accessibility without increasing public resource investment, this hypothesis is based on the premise that the total number of nine healthcare service facilities remains unchanged, with resources distributed among 71 village residential points as potential new locations. We conducted a simulation analysis using GIS, with specific parameter settings detailed in Fig. 9. The results show a significant improvement in overall accessibility within the county, regardless of whether travel is by electric bike or car. Specifically, the maximal coverage model for electric bike travel shows that three healthcare facility locations remain unchanged. Prior to the simulation, an accessibility analysis indicated that 11 residential points lacked access to medical services within a 30-minute threshold. However, postsimulation, this number dramatically decreased to only two points: Junliao village in Daping town and Shanlian village in Zhaigang town (Fig. 10a). Similarly, the maximal coverage model for car travel indicates that two healthcare facility locations remain unchanged under this model setting. Under this hypothetical model, all residential points fall within the service range, whereas the presimulation accessibility analysis identified four villages without service (Fig. 10b). These results confirm that by optimizing the distribution of existing resources without increasing the number of healthcare facilities, overall accessibility to medical services can be significantly enhanced.

Parameter Settings for the Maximal Coverage Model

Results from the maximal coverage model simulation. a electric bike. b car
Additionally, the simulation results demonstrate high consistency with real-world conditions, thus providing considerable reference value. In simulations that included both modes of transportation, Baimang village and Guoshui village were identified as new sites. This outcome aligns closely with field research and in-depth interviews with the heads of health centers in these towns, and both locations are considered ideal for their respective town health centers. These site selection recommendations are not only theoretically sound but also strongly supported by practical considerations, thus providing important references for future structural adjustments in the county's healthcare service system.
Optimization of the multicore and multiring models
According to the "Liannan Yao Autonomous County Healthcare Service System Plan (2021—2025)", as published by the government, projections indicate that by 2025, the composite ratio of key indicators between primary healthcare facilities and county hospitals will reach 1.7 to 2.4. These data provide a basis for assigning weight to the service capacity expansion at Zhaigang Health Center. The estimated service capability score post-expansion was calculated and is detailed in Table 10.
The resimulation of the accessibility within a 30-minute travel radius by electric bike demonstrates that with the enhanced service capability of the Zhaigang Health Center (Fig. 11) , there has been a significant improvement in the accessibility tiers in the southeastern region, covering nearly one-third of Liannan County's total area. In this region, most areas previously rated as Level 5 have been upgraded to Level 6, signifying that residents can now access healthcare services more easily, particularly in remote villages on the outskirts of Liannan County. This significant improvement considerably alleviates the issue of insufficient medical services.

Simulated spatial distribution of healthcare service accessibility by electric bike. a current situation. b projected
Similarly, the accessibility within a 30-minute travel radius by car was resimulated, as shown in Fig. 12. The results indicate that the expansion of service capacity at Zhaigang Health Center predominantly affected the southeastern region, which accounts for approximately one-third of Liannan County's area. Notably, given that the time differences in car travel are less significant at short distances, residents closer to Zhaigang Health Center did not exhibit a marked advantage in accessibility assessments. Therefore, improvements in car travel accessibility become more apparent when considering a broader road network and longer driving distances. This finding aligns with the research results mentioned in the Results section, indicating that within a certain range, changes in car travel accessibility are not as pronounced as those with electric bikes.

Simulated spatial distribution of healthcare service accessibility by car. a current situation. b projected
In summary, the model results clearly demonstrate that the enhanced service capacity of the Zhaigang Health Center has positively impacted the accessibility of healthcare services in the southeastern region, underscoring its critical role in Liannan County’s healthcare service network. Although the southeastern region has experienced significant improvements in accessibility, other areas have not experienced comparable enhancements. This suggests that planning the healthcare service network in Liannan County must fully consider regional differences, as reliance on a single central health center is insufficient. Furthermore, future plans should include the establishment of additional central health centers to enhance the accessibility of healthcare services throughout the country.
Conclusion
The quality of medical services in remote and rural areas, a critical component of the primary healthcare system, has long been underemphasized in academic research. This study employs a multifaceted approach by integrating GIS, field research, and expert interviews and enhances the 2SFCA method to conduct empirical research in Liannan County. The goal is to explore the current layout and optimization strategies of primary healthcare facilities in remote and rural areas, focusing on accessibility. By assessing the impacts of various transportation methods and thresholds, our study shows that simple improvements in transportation modes, such as the use of electric vehicles and cars, have certain limitations in enhancing the accessibility of healthcare services in remote and rural areas. Furthermore, the imbalance in regional development is a key factor limiting the improvement of healthcare service quality, requiring a comprehensive strategy to address, including but not limited to enhancing transportation infrastructure and service capacity. Based on the current development status of Liannan County, we propose two optimization strategies that provide practical suggestions for enhancing regional medical services. This research not only guides the spatial layout and resource optimization of healthcare facilities in Liannan County but also establishes new research paths and methodologies for studying healthcare facilities accessibility in remote and rural areas. We hope these results will serve as valuable references for improving rural medical services and promoting the health and well-being of rural residents.
At the innovation level, we achieved the following results: First, we refined the traditional 2SFCA model based on the unique characteristics of remote rural areas, allowing for a more accurate reflection of the actual supply and demand situation in these regions. Second, by effectively integrating qualitative and quantitative research, we successfully overcame the challenges of data collection in remote areas, ensuring that the evaluation criteria are both comprehensive and precise. Third, we conducted an innovative comparative analysis of multiple transportation modes, offering a broader perspective for the optimal allocation of healthcare resources. Lastly, by integrating multidisciplinary knowledge, we expanded the scope of the research further and, through scenario simulation and strategy optimization, provided robust scientific support for decision-makers.
This study is predicated on the assumption that residents exclusively seek medical treatment within Liannan County and that local medical resources are dedicated solely to those within the specified research area. However, it does not consider the medical practices of residents in bordering areas or the impact of neighboring regions on the accessibility of medical services. Additionally, the behaviors associated with seeking medical treatment across administrative boundaries have not been thoroughly examined. Future research should investigate these questions more deeply. Furthermore, subsequent in-depth studies should monitor and validate the actual effects of the two proposed recommendations, undertaking more extensive analyzes that integrate various geographic and socioeconomic factors. Such an approach would enhance the theoretical foundation and practical guidance necessary for optimizing global rural medical services.
Availability of data and materials
The basic transportation data for Liannan Yao Autonomous County were obtained from the National Geomatics Center of China(NGCC): https://www.ngcc.cn/. Population and healthcare-related data were sourced from the Liannan Yao Autonomous County Statistics Bureau and the Liannan Yao Autonomous County Health Bureau. However, restrictions apply to the availability of these data, which were used under licence for the current study and so are not publicly available. The data are, however, available from the authors upon reasonable request and with the permission of the Liannan Yao Autonomous County Statistics Bureau and the Liannan Yao Autonomous County Health Bureau.
Abbreviations
- WHO:
-
World Health Organisation
- 2SFCA:
-
Two-step floating catchment area
- THC:
-
Town Health Center
- GIS:
-
Geographic Information System
- POI:
-
Points of Interest
References
Allan DP. Catchments of general practice in different countries– a literature review. Int J Health Geograph. 2014;13(32). https://doi.org/10.1186/1476-072X-13-32.
World Health Organization. WHO global strategy on integrated people-centred health services 2016-2026 Executive Summary. Available at: https://iris.who.int/bitstream/handle/10665/180984/WHO_HIS_SDS_2015.20_eng.pdf?sequence=1%20. Accessed 22 Apr 2024.
Wu C, Tu Y, Li Z, et al. An early assessment of the County Medical Community reform in China: a case study of Zhejiang province. J Chinese Gov. 2021;6(4):463–85.
Yao Q, Liu C, Ferrier JA, et al. Urban‒rural inequality regarding drug prescriptions in primary care facilities – a pre-post comparison of the National Essential Medicines Scheme of China. Int J Equity Health, 2015.
Liu L, Zhao Y, Lyu H, Chen S, Tu Y, Huang S. Spatial Accessibility and Equity Evaluation of Medical Facilities Based on Improved 2SFCA: A Case Study in Xi’an, China. Int J Environ Res Public Health. 2023;20(3):2076.
Liu S, Qin Y, Xu Y. Inequality and Influencing Factors of Spatial Accessibility of Medical Facilities in Rural Areas of China: A Case Study of Henan Province. Int J Environ Res Public Health. 2019;16(10):1833.
Marwal A, Silva E. Literature review of accessibility measures and models used in land use and transportation planning in last 5 years. J Geograph Sci. 2022;32(3):560–84.
Hansen W. How Accessibility Shapes Land Use. J Am Plan Assoc. 1959;25(2):73–76.
Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. 1981;19(2):127–40.
Khan AA. An integrated approach to measuring potential spatial access to health care services. Socio-Econ Plan Sci. 1992;26(4):275–87.
Yang L, Liang Y, He B, Yang H, Lin D. COVID-19 moderates the association between to-metro and by-metro accessibility and house prices. Transportation Research Part D-Transport and Environment, 2023, 114.
Guo C, Liang J. Accessibility analysis of medical facilities based on multiple transportation modes of network map. J Geo-information Sci, 2022,24(3):483-494(In Chinese).
Guagliardo MF. Spatial accessibility of primary care: concepts, methods and challenges. Int J Health Geograph, 2004, 3(3).
Hu R, Dong S, Zhao Y, et al. Assessing potential spatial accessibility of health services in rural China: a case study of Donghai county. Int J Equity Health. 2013;12(35). https://doi.org/10.1186/1475-9276-12-35.
Li P, Hua L, Yu Q. Theoretical and methodological review of urban accessibility research. Urban Issues. 2005;01:69–74.
Koenig J.G. Indicators of urban accessibility: Theory and application. Transportation, 1980,9(2)(In Chinese).
Yang T, Guo X. New Concept of Urban Travel Accessability and its Application. China J Highway Transport. 1995;02:25–30 (In Chinese).
Radke J, Mu L. Spatial Decompositions, Modelling and Mapping Service Regions to Predict Access to Social Programs. Annals of GIS. 2000;6(2):105–12.
Luo W, Wang F. Measures of Spatial Accessibility to Health Care in a GIS Environment: Synthesis and a Case Study in the Chicago Region. Environment and Planning B: Planning and Design. 2003;30(6):865–84.
Wachs M, Kumagai TG. Physical accessibility as a social indicator. Socio-Econ Plann Sci. 1973;7(5):437–56.
Joseph AE, Bantock PR. Measuring potential physical accessibility to general practitioners in rural areas: a method and case study. Soc Sci Med (1982). 1982;16(1):85–90.
Ding Q, Zhu L, Luo J. Analysing spatial accessibility to residential care facilities in Wuhan. Human Geography. 2016;31(02):36–42 (In Chinese).
Song Z, Chen W, Zhang G, Zhang L. Spatial Accessibility to Public Service Facilities and Its Measurement Approaches. Progress in Geography. 2010;29(10):1217–24 (In Chinese).
Zhang J, Han P, Sun P, Zhao J, Yang L. Assessing Spatial Accessibility to Primary Health Care Services in Beijing. China: Int J Environ Res Public Health; 2021;18(24): 13182.
Luo W, Qi Y. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians. Health Place. 2009;15(4):1100–7.
Dai D. Racial/ethnic and socioeconomic disparities in urban green space accessibility: Where to intervene?. Landscape and Urban Plann. 2011;102(4):234–44.
Dai D, Wang F. Geographic Disparities in Accessibility to Food Stores in Southwest Mississippi. Environment and Planning B: Planning and Design, 2011, 38(4).
Wang F, Tang Q. Planning toward Equal Accessibility to Services: A Quadratic Programming Approach. Environment and Planning B: Planning and Design. 2013;40(2):195–212.
Xing L, Liu Y, Wang B, Wang Y, Liu H. An environmental justice study on spatial access to parks for youth by using an improved 2SFCA method in Wuhan, China. Cities. 2020, 96.
Wang F. Measurement, Optimization, and Impact of Health Care Accessibility: A Methodological Review. Annals Assoc Am Geographers. 2012;102(5):1104–12.
Lu C, Zhang Z, Lan X. Impact of China's referral reform on the equity and spatial accessibility of healthcare resources: A case study of Beijing. Soc Sci Med. 2019:1-9.
Cheng J, Cheng J, Lu Y, Huang Z, Cao F. Spatial inequity in access to healthcare facilities at a county level in a developing country: a case study of Deqing County, Zhejiang, China. Int J Equity Health, 2015.
Liu Y, Gu H, Shi Y. Spatial Accessibility Analysis of Medical Facilities Based on Public Transportation Networks. International J Environ Res Public Health. 2022;19:16224.
Gu X, Zhang L, Tao S, Xie B. Spatial Accessibility to Healthcare Services in Metropolitan Suburbs: The Case of Qingpu, Shanghai. Int J Environ Res Public Health. 2022;16:225.
Wang X, Yang H, Duan Z, et al. Spatial accessibility of primary health care in China: A case study in Sichuan Province. Soc Sci Med. 2018;209:14–24.
Liu G, Wang Y, Wang Y. Impact of inverse distance weighted interpolation factors on interpolation error. China Sciencepaper, 2010,5(11):879-884(In Chinese).
Tao Z, Chen Y, Dai T. Measuring spatial accessibility to residential care facilities in Beijing. Progress in Geography. 2014;33(05):616–24 (In Chinese).
Hang J, Chen M, Li Y, Peng M. The Evaluation and Optimization of the Quality of Medical and Health Service Facilities in Wuhan Based on Optimal Path Analysis and Two-Step Floating Catchment Area Method. Modern Urban Res. 2019;08:25–34 (In Chinese).
Xu B, Qin Q, Wei X, Li J, Lin Y, et al. Spatial Accessibility to the Primary Healthcare Services of Community Healthcare Centers in Nanning City: Gaussian Two-step Floating Catchment Area Approach. Chin J Health Stat. 2021;38(06):852–9 (In Chinese).
Berens W, Körling FJ. Estimating road distances by mathematical functions. Eur J Operational Res. 1985;21(1):54–6.
Brimberg J, Love RF. General Considerations on the Use of the Weighted lp Norm as an Empirical Distance Measure. Transportation Sci. 1993;27(4):341–9.
Peeters D, Thomas I. Distance predicting functions and applied location-allocation models. J Geograph Syst. 2000;2(2):167–84.
Love RF, Morris JG. Mathematical Models of Road Travel Distances. Manag Sci. 1979;25(2):130–9.
Wang F . Quantitative methods and applications in GIS. Commercial Press, 2009 (In Chinese).
Siegel M, Koller D, Vogt V, et al. Developing a composite index of spatial accessibility across different health care sectors: A German example. Health policy (Amsterdam). 2016;120(2):205–12.
Wang Q. Accessibility analysis of medical services in Shanghai based on improved two-step mobile search method. Natural Geography of Wuhan University, 2019 (In Chinese).
Tao H, Chen X, Li X. Research on Spatial Accessibility to Health Service——A Case Study in the Haizhu District of Guangzhou. Geomatics & Spatial Information Technology. 2007;01:1–5 (In Chinese).
Ministry of Transport of the People’s Republic of China. Design Specification for Highway Alignment Available at:https://xxgk.mot.gov.cn/2020/jigou/glj/202006/t20200623_3312660.html. Accessed 22 Apr 2024 (In Chinese).
Acknowledgements
Not applicable.
Funding
This research was supported by the philosophy and social science foundation of Guangdong province, China[grant number GD22CGL33], Office of the Guangzhou Social Science Planning Leadership Group, China[grant number 2024GZYB22] and Guangzhou Municipal Science and Technology Bureau, China [grant number 202201011084]. The funding bodies did not influence this paper in any way prior to circulation.
Author information
Authors and Affiliations
Contributions
LL Conceptualized and wrote the first and final draft of the article. YC designed the research methods, analysed the data and wrote the first draft. HX revised the manuscript and reviewed all the literature. JZ and YX participated in field finds and data collection. PZ and LW participated in designing the figures and tables. YS revised the manuscript. All authors read and approved the paper.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Our study was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Guangdong Pharmaceutical University [Ethics approval number: (2024) IIT (30)]. The ethics committee reviewed and approved the request for a waiver of written informed consent. All methods were used in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, L., Chen, Y., Xiang, H. et al. Measuring and optimizing the spatial accessibility of primary health care in remote and rural areas: a case study of Liannan Yao Autonomous County in China. BMC Health Serv Res 24, 1100 (2024). https://doi.org/10.1186/s12913-024-11556-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-024-11556-1