
Abstract
Metabolic dysfunction-associated steatotic liver disease (MASLD), previously termed nonalcoholic fatty liver disease (NAFLD), poses a significant global health challenge due to its increasing prevalence and strong association with cardiovascular disease (CVD). This comprehensive review summarizes the current knowledge on the MASLD-CVD relationship, compares analysis of how different terminologies for fatty liver disease affect cardiovascular (CV) risk assessment using different diagnostic criteria, explores the pathophysiological mechanisms connecting MASLD to CVD, the influence of MASLD on traditional CV risk factors, the role of noninvasive imaging techniques and biomarkers in the assessment of CV risk in patients with MASLD, and the implications for clinical management and prevention strategies. By incorporating current research and clinical guidelines, this review provides a comprehensive overview of the complex interplay between MASLD and cardiovascular health.
Similar content being viewed by others

Introduction
Nonalcoholic fatty liver disease (NAFLD), a manifestation of metabolic syndrome (MS), is now one of the leading causes of chronic liver disease worldwide. It affects approximately 25% of the global population [1], and this figure is expected to increase to 38% by 2023 [2]. In 2020, NAFLD was redefined as “metabolic-associated fatty liver disease” (MAFLD), characterized by liver steatosis evident through biopsy, imaging or elevated liver enzymes, as well as obesity/overweight, type 2 diabetes mellitus (T2DM) or metabolic disorders [3, 4]. Afterwards, in 2023, three major international hepatology organizations advocated for a nomenclature shift, recommending that the term “metabolic dysfunction-associated steatotic liver disease (MASLD)” be adopted in lieu of NAFLD as the preferred term currently used in the field, the term “non-alcoholic steatohepatitis” has been superseded by “metabolic dysfunction-associated steatohepatitis (MASH)” [5].
MASLD includes a spectrum of liver conditions, ranging from simple steatosis (fat in > 5% of hepatocytes) to MASH, advanced fibrosis, cirrhosis and hepatocellular carcinoma [6]. Recently, MASLD has been considered a multisystemic disease with interorgan connections to extrahepatic conditions [7,8,9,10]. Increasing evidence suggests that cardiovascular disease (CVD) is a significant concern in individuals with MASLD [11], with a greater risk of CVD-related deaths than liver-related deaths [12, 13]. This is due to shared pathophysiological mechanisms such as insulin resistance (IR), endothelial dysfunction, oxidative stress (OS), and systemic inflammation [12, 14, 15].
MASLD and CVD interactions are associated with common metabolic disorders such as obesity, hypertension, dyslipidemia and diabetes [16, 17]. The preferred term MASLD has been used to reflect the independence of MAFLD patients from metabolic risk factors. Although both MAFLD and MASLD are associated with different atherosclerotic cardiovascular disease (ASCVD) risks, MAFLD predicts ASCVD risk better than MASLD does [18]. However, empirical confirmation regarding the superior predictive efficacy of MAFLD over MASLD in forecasting CVD events remains elusive [19]. Since cardiovascular death has overtaken liver-related deaths and is the most common cause of death in MASLD patients, the link between MASLD and CVD has attracted the attention of clinicians, and it is crucial to identify MASLD patients at greater risk of fibrosis and disease progression and to effectively prevent and manage cardiovascular(CV) risk [20]. This review aimed to provide an overview of the current understanding of MASLD and its impact on cardiovascular health.
Comparative analysis of CV risk across different terminologies of fatty liver diseases
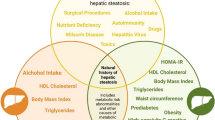
In recent years, as the understanding of fatty liver disease deepens, the diagnostic criteria for NAFLD, MAFLD, MASLD have gradually evolved, reflecting a deeper understanding of the relationship between metabolism and liver health. At the same time, a new category, outside pure MASLD, termed metabolic and alcohol related/associated liver disease (MetALD), was selected to describe those with MASLD who consume greater amounts of alcohol per week (140 g/week and 210 g/week for females and males respectively) [5]. The variations in these criteria not only affect the diagnosis of liver disease but also have a substantial impact on the assessment of CV risk.
The diagnostic criteria for NAFLD are based on liver imaging (such as ultrasound, CT or MRI) showing more than 5% fat deposits in the liver, and exclude alcoholic liver disease (daily alcohol intake > 20 g for men, > 10 g for women) and other causes (such as drugs, viral hepatitis, hereditary liver disease, etc.) [21]. Its criteria emphasize the presence of fat accumulation, but the lack of attention to metabolic factors may lead to insufficient CV risk assessment for certain metabolic high-risk populations (such as obese patients).
The diagnostic criteria of MAFLD encompass the detection of fatty liver, complemented by at least one additional criterion from the trio of overweight or obesity, type T2DM, or manifestations of metabolic imbalance [3]. The criteria for MAFLD place more emphasis on metabolic factors and can more comprehensively identify CV risks associated with metabolic syndrome (MS), suggesting MAFLD may be a better nomenclature than NAFLD in clinical practice [22, 23]. By identifying metabolic abnormalities, patients’ CV risks can be assessed earlier and more targeted interventions can be developed.
The diagnostic criteria for MASLD are similar to those for MAFLD, with the cardiometabolic criteria adjusted to incorporate one cardiometabolic factor [5].Compared with MAFLD, MASLD further refines the role of metabolic dysfunction in liver disease, has more specific diagnostic criteria, and emphasizes CV risk factors. Although emerging data indicate a remarkably high concordance between the diagnoses of NAFLD and MASLD, with approximately 99% of individuals classified with NAFLD also fulfilling the criteria for MASLD [24]. Definition of MASLD provides more flexibility in assessing CV risk and can cover a wider population, including those who may not be identified under the definition of NAFLD, thereby improving the understanding and management of CVD risk. In a recent comparative analysis evaluating the relationship between MASLD and MAFLD with coronary artery calcification (CAC), highlighting a distinct link between MASLD and the severity of CAC, with MASLD being uniquely associated with advanced stage of CAC [25]. This association suggests that MASLD could potentially serve as a more robust indicator of increased ASCVD risk compared to MAFLD. However, another study intriguingly found that while both MASLD and MAFLD exhibit associations with varying risks of ASCVD, MAFLD demonstrates superior predictive capability for ASCVD risk compared to MASLD [18]. In addition, a recent study underscores the enhanced predictive capability of MAFLD in pinpointing patients at an elevated risk for liver fibrosis and disease progression [20]. Therefore, conducting validation studies to ascertain the reliability and consistency of the classification criteria for MAFLD and MASLD is crucial, as this will prevent ambiguity and ensure the global relevance of these newly adopted terminologies.
Nonetheless, such a comparison may not conclusively dictate the clinical utility of these diagnostic classifications. A recent meta-analysis evaluating the association of MASLD and MetALD with clinical outcomes showed that both MASLD and MetALD had increased CVD incidence compared with participants without SLD. In addition, MetALD was associated with a significantly increased risk of cardiovascular death [26]. Current evidence suggests that patients with MetALD have a more unfavorable prognosis compared with patients with MASLD. Moreover, a community cohort study with a 20-year follow-up suggested that the risk of CVD increased in the order of no SLD, MASLD, and MetALD [27], shedding light on critical implications for clinical practice and further research based on different terminology.
Pathophysiological mechanisms linking MASLD to CVD
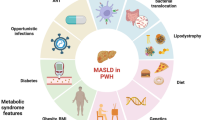
As MASLD and CVD share many common risk factors, the pathophysiological mechanisms linking MASLD to an increased risk of CVD are complex and multifaceted and include multiple mechanisms (Fig. 1).

Pathophysiological mechanisms linking MASLD to CVD (Created with BioRender.com). IR: insulin resistance, MASLD: metabolic dysfunction-associated steatotic liver disease, CVD: cardiovascular disease
Insulin resistance
IR is a condition in which cells become less responsive to insulin, a hormone essential for regulating blood glucose levels. Normally, insulin stimulates tissues to absorb glucose and convert it into glycogen while also inhibiting liver glucose production. However, in IR, this regulatory mechanism is compromised [28]. IR is a central feature in the onset of MASLD and MS, impacting lipid metabolism and contributing to a range of metabolic disorders [29]. The liver takes up excess free fatty acids (FFAs), which contribute to fat accumulation in hepatocytes; this process is known as hepatic steatosis or fatty liver [30]. This occurs due to increased FFAs release from adipose tissue and reduced excretion, resulting in increased circulating FFAs concentrations. Under normal insulin conditions, the liver synthesizes triglycerides (TGs) from FFAs and packages them into very low-density lipoprotein (VLDL) particles for storage or export. However, IR impairs this process, causing lipid accumulation in liver cells and exacerbating hepatic steatosis [29]. Lipid imbalance also fosters atherosclerosis development. Atherogenic dyslipidemia combined with other MS- and MASLD-related factors, such as hypertension, inflammation and hyperglycemia, escalates the risk of ASCVD [31]. Consequently, individuals with IR are at a notably greater risk for heart attacks, strokes and other cardiovascular events, even without overt diabetes. Overall, IR initiates a cascade of metabolic disorders, predisposing individuals to liver disease and significantly increasing CVD risk.
Inflammation
The association of MASLD with systemic inflammation is a critical factor in disease progression [32]. Inflammation extends beyond the liver, significantly impacting other organ systems, particularly the cardiovascular system [7, 33]. In MASLD, there is increased release of inflammatory cytokines and chemokines, with tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) being key mediators. One article indicated that in mice model, TNFα is a key regulator of liver inflammation and IR associated with the development of early non-obese MASH, and is a key factor in the development of MASLD [34]. Meanwhile, TNF-α secretion is predominantly linked to hepatic inflammation and steatosis. By engaging the nuclear factor kappa-B(NF-κB) signaling cascade, TNF-α orchestrates the upregulation of a cadre of pro-inflammatory mediators. Furthermore, TNF-α initiates monocyte activation, facilitating their transformation into foam cells, a pivotal event in the pathogenesis of atherosclerosis [35].While IL-6 initiates the JAK/STAT signaling cascade, culminating in the transcriptional upregulation of acute-phase reactants, including C-reactive protein (CRP) and serum amyloid A (SAA), which in turn amplify the hepatic inflammatory response, as well as systemic effects outside the liver [36,37,38]. Chronic low-level inflammation is a hallmark of MASLD and plays a pivotal role in atherosclerosis development. Atherosclerosis is characterized by arterial plaque formation. In MASLD, elevated levels of proinflammatory cytokines such as TNF-α and IL-6 may exacerbate this process through endothelial dysfunction, plaque instability and arterial wall injury, further triggering atherosclerosis progression and coronary artery events [39, 40].
Oxidative stress
OS arises from an imbalance between the production of reactive oxygen species (ROS) and the body’s antioxidant defenses. It is intricately connected to the pathophysiology of MASLD and CVD risk [32]. In MASLD, excessive fat accumulation in the liver increases ROS production, leading to cellular damage and promoting inflammation and fibrosis. This can further intensify IR—a defining feature of MASLD—and escalate metabolic dysregulation [41]. In the context of CVD, OS promotes atherosclerosis by damaging the endothelium, inciting inflammation and oxidizing lipids, which can result in arterial plaque formation [42]. Elevated OS can also impair cardiovascular function by attacking heart muscle cells and blood vessels, potentially leading to hypertension, myocardial infarction (MI), and heart failure [43]. In addition, obesity, a prevalent condition in both MASLD and CVD, triggers OS through the production of nutrients that increase VLDL and LDL levels and promote lipid peroxidation, thereby increasing the risk of CVD [44].
Endothelial dysfunction
Endothelial dysfunction is a crucial factor in the pathogenesis of CVD and is intimately linked to MASLD. The endothelium, which lines blood vessels, is essential for maintaining vascular homeostasis by regulating blood flow, tone and coagulation. It typically produces mediators that induce vasodilation and prevent platelet aggregation and smooth muscle cell proliferation [45]. In MASLD, this equilibrium is disturbed, resulting in endothelial dysfunction and an elevated risk of cardiovascular events [46]. Nitric oxide (NO), a critical endothelium-derived relaxing factor, is vital for endothelial health, promoting vasodilation and inhibiting platelet aggregation and smooth muscle cell proliferation [47]. However, in MASLD, NO production is often compromised by heightened OS and inflammation, which diminishes NO availability. Asymmetric dimethylarginine (ADMA), an endogenous inhibitor of endothelial NO synthase (eNOS), significantly contributes to endothelial dysfunction in both MASLD and CVD patients. Elevated ADMA levels, which are prevalent in MASLD, inhibit eNOS and consequently NO production. This reduction in NO leads to diminished vasodilation, increased vasoconstriction, and consequently increased vascular resistance and blood pressure. The increase in ADMA associated with MASLD is attributed to enhanced methylation in the liver and prevalent OS and inflammation, which further suppresses NO synthesis and exacerbates endothelium-dependent vasodilation [48]. This suppression also results in increased arterial stiffness and increased thrombosis risk, underscoring the role of ADMA as a mediator between vascular dysfunction in MASLD and increased CVD risk. Furthermore, endothelin-1 (ET-1), a potent vasoconstrictor, is frequently overproduced in MASLD due to proinflammatory and oxidative conditions. Although ET-1 is crucial for regulating vascular tone under normal circumstances, its excessive production in MASLD leads to pathological vasoconstriction and proliferation of vascular smooth muscle, exacerbating endothelial dysfunction and atherosclerosis [49]. Therefore, addressing the imbalance caused by ADMA and ET-1 is crucial for ameliorating endothelial dysfunction in MASLD patients and mitigating the risk of CVD.
Altered lipoprotein metabolism
In MASLD, dyslipidemia characterized by elevated small dense low-density lipoprotein (sdLDL) and reduced high-density lipoprotein (HDL) cholesterol is a key driver of atherosclerosis and CVD. The ability of sdLDL particles to penetrate the endothelium and transform into oxidized low-density lipoprotein (ox-LDL) triggers inflammatory pathways pivotal to atherosclerotic plaque development. Their reduced clearance due to their lower affinity for LDL receptors intensifies their atherogenic effects [50]. Concurrently, diminished HDL levels impair reverse cholesterol transport and curtail the antioxidant and anti-inflammatory roles of HDL, hindering excess cholesterol breakdown. The impaired lipid regulation in the liver results in an overabundance of VLDL and a reduction in HDL functionality, fostering a pro-atherosclerotic lipid profile [51]. The uptake of sdLDL by macrophages leads to foam cell formation, exacerbating endothelial dysfunction and OS, which promotes atherosclerosis progression. The interaction between altered sdLDL and HDL levels in MASLD substantially accelerates atherosclerotic CVD, highlighting the crucial role of lipoprotein metabolism in the vascular complications of MASLD.
Increased thrombogenicity
MASLD increases the risk of cardiovascular and vascular events by promoting a hypercoagulable state. It is linked to elevated levels of coagulation factors such as factor VIII, fibrinogen, and von Willebrand factor, which shift the balance toward hypercoagulability and can lead to the production of dysfunctional coagulation proteins [52]. IR and inflammation in MASLD patients enhance platelet reactivity, increasing the risk of thrombosis through aggregation and vascular endothelium damage, potentially leading to acute events such as MI or stroke. Additionally, elevated plasminogen activator inhibitor-1 (PAI-1) in MASLD disrupts fibrinolysis, slowing blood clot breakdown and intensifying a prothrombotic state [53]. Endothelial dysfunction due to reduced NO production and increased adhesion molecule levels further favors a thrombogenic environment in MASLD patients. The cumulative effect of these factors indicates the probability of thrombus formation, predisposing individuals to ischemic events in coronary arteries and other vascular territories that can result in heart attacks, strokes or peripheral arterial disease [54]. Overall, the impact of MASLD on coagulation, platelet function, fibrinolysis and endothelial health collectively elevates the risk of thromboembolic events.
Imbalance of adipokines
Adipokine dysregulation significantly influences systemic metabolism and inflammation in the pathogenesis of MASLD. The level of adiponectin, an adipokine with anti-inflammatory properties that enhances insulin sensitivity, is typically reduced in individuals with MASLD. This decrease is linked to IR and an elevated CV risk, and it can exacerbate hepatic steatosis and the progression of NASH [55]. Conversely, leptin, which normally suppresses appetite and regulates energy expenditure, is increased in individuals with MASLD. High leptin levels are associated with liver fibrosis and inflammation and contribute to atherosclerosis through proinflammatory effects, OS, and endothelial dysfunction [56, 57]. In addition to adiponectin and leptin, the dysregulation of other adipokines, such as resistin, visfatin, and chemerin, which affect IR, inflammation, and metabolic pathways, has been observed in MASLD patients [58]. The perturbed adipokine profiles in MASLD contribute to liver pathology and increase the risk of metabolic disorders, including IR, T2DM, and CVD, emphasizing the importance of adipose tissue-derived factors in metabolic health.
Ectopic fat deposition
Ectopic fat deposition in MASLD involves the abnormal accumulation of fat in non-adipose organs such as the liver, pancreas, heart and skeletal muscle, leading to metabolic complications [59, 60]. The liver’s capacity to store fat is overwhelmed by factors such as IR, excessive dietary fat intake and genetic predispositions, resulting in hepatic steatosis [61]. This can progress from simple steatosis to MASH, fibrosis and cirrhosis and increase the risk of liver failure and hepatocellular carcinoma [62]. The heart is particularly susceptible to ectopic fat deposition, with excess fatty acids potentially accumulating in the myocardium or peripheral blood vessels. These lipotoxic effects can impair cardiac function through OS, endoplasmic reticulum stress, mitochondrial dysfunction, and inflammatory responses [59]. These changes can manifest as changes in myocardial structure and function, cardiac arrhythmias, and increased susceptibility to myocardial ischemia. Cardiac fat accumulation is correlated with an elevated risk of CVD, a major cause of mortality in MASLD patients [63]. One study demonstrates a positive correlation between elevated pericardial adipose tissue and the propensity for heart failure, with a pronounced effect observed in the female cohort. The findings advocate for the acknowledgment of pericardial fat as an emergent risk factor in the etiology of heart failure [64]. Another study among Chinese middle-aged and elderly patients demonstrates that periaortic fat volume (PAFV) is significantly associated with coronary artery atherosclerosis and severe CAD, independent of general obesity and clinical risk factors. Visceral adipose tissue (VAT) is found to be associated with severe CAD, highlighting the potential of ectopic fat measurement as a clinical indicator for coronary atherosclerosis risk assessment [65].Thus, ectopic fat deposition in MASLD patients is a significant concern, necessitating attention to prevent adverse cardiovascular outcomes.
Genetic susceptibility
Genetic predisposition significantly influences the onset of MASLD and CVD, with identified risk factors including specific genetic polymorphisms. A notable example is the single nucleotide polymorphism (SNP) rs738409 in the patatin-like phospholipase domain-containing protein 3 (PNPLA3) gene, which encodes a liver-expressed protein involved in lipid metabolism [66]. The isoleucine to methionine at position 148 (I148M) substitution caused by this SNP is linked to heightened liver fat accumulation and an increased risk of progressive liver disease, including cirrhosis and hepatocellular carcinoma, irrespective of traditional risk factors [67]. Although the direct impact of the PNPLA3 I148M variant on CVD risk is complex, it may contribute to atherogenic dyslipidemia, potentially increasing CVD risk through an unfavorable lipid profile [68]. In addition to PNPLA3, variants in genes such as transmembrane 6 superfamily member 2 (TM6SF2) and membrane-bound O-acyltransferase domain 7 (MBOAT7) are associated with MASLD progression [69]. Another study indicated that the TM6SF2 E167K gene variant is associated with an increased susceptibility to MASH and liver fibrosis but is paradoxically protective against cardiovascular events, suggesting a complex interplay between liver disease severity and CV risk [70]. Polymorphisms in glucokinase (GCKR) and sterol regulatory element-binding protein 1 (SREBP-1) genes, which are involved in fat content and lipid metabolism, may also influence CVD risk [71]. Understanding these genetic susceptibilities is pivotal for personalized medicine, enabling targeted approaches to screening, prevention, and treatment of MASLD and associated CVD risk.
Changes in the gut microbiota
Emerging research highlights the intricate connections between the gut microbiota, MASLD, and CVD risk, indicating a significant role for the gut microbiome in the development and progression of these diseases. Gut dysbiosis, an imbalance in the microbiota, is linked to metabolic disorders such as MASLD. The gut-liver axis is pivotal, with bacteria modulating liver metabolism through the production of beneficial short-chain fatty acids (SCFAs) and potentially harmful metabolites [72]. Dysbiosis also enhances intestinal permeability, promoting the translocation of noxious bacterial products and inciting liver inflammation. The microbiota further impacts bile acid composition and influences lipid and glucose metabolism, as well as energy balance [73]. The role of the gut microbiota in cardiovascular health is multifaceted. Specifically, gut bacteria convert dietary choline and L-carnitine to trimethylamine (TMA), which is then metabolized to trimethylamine N-oxide (TMAO) in the liver. Furthermore, as a metabolite derived from the gut microbiota, TMAO is potentially linked to endothelial dysfunction through the modulation of critical vasocrine factors, including NO and adhesion molecules, which may confer an elevated risk of atherosclerosis, MI, and stroke [74, 75]. Additionally, systemic inflammation incited by dysbiosis and microbial product translocation into the bloodstream may foster endothelial dysfunction and atherosclerosis, key contributors to CVD [76]. Microbial metabolites and their engagement with the host immune system can also affect blood pressure regulation, impacting cardiovascular health [77]. One study uncovers a significant link between gut microbiota dysbiosis, characterized by reduced richness and diversity, and elevated serum urate levels across two cohorts. The study indicates that gut microbiota imbalance may influence urate metabolism, offering new insights into the development of associated metabolic conditions [78]. Given the dual role of the gut microbiota in MASLD and CVD, dysbiosis is a common contributor to the pathogenesis of both conditions.
Effect of MASLD on traditional CV risk factors and its relationship to CVD
MASLD is intricately linked to CV risk factors and is characterized by the co-occurrence of hepatic steatosis and metabolic disorders associated with several traditional CV risk factors, including atherogenic dyslipidemia, hypertension, obesity and T2DM (Fig. 2). The association with CVD risk factors has been explained by current studies (Table 1). And the correlated CVD complications will be described below.

Effect of MASLD on traditional cardiovascular risk factors (Created with BioRender.com). MASLD: metabolic dysfunction-associated steatotic liver disease
MASLD and obesity
Obesity, characterized by excessive fat accumulation, particularly in the abdominal region, is strongly correlated with MASLD. This central obesity leads to fat deposits in the liver, potentially causing liver cell damage and inflammation, which are hallmarks of MASLD development [79]. Obesity is also an established risk factor for CVD, and its co-occurrence with MASLD can exacerbate CVD risk factors, leading to a significant increase in CVD risk. As a central feature of MS, obesity is recognized as a primary diagnostic criterion for MASLD and serves as a significant link between MASLD and CVD risk. Recent research has supported the notion that addressing obesity can ameliorate MASLD and mitigate CVD risk [80]. However, a study among the MASLD population in the United States revealed that nonobese individuals with MASLD constituted half of the affected population, and these nonobese individuals exhibited higher all-cause mortality rates than did their obese counterparts [81]. Overall, obesity is a pivotal factor connecting MASLD and CVD risk, and managing obesity is crucial for improving MASLD outcomes and reducing CVD risk.
MASLD and atherogenic dyslipidemia
Dyslipidemia, a common metabolic disorder, is defined by abnormalities in blood lipid concentrations and compositions. MASLD extends beyond liver fat accumulation and is closely tied to atherogenic dyslipidemia, a lipid disorder typically characterized by elevated TG levels, diminished high-density lipoprotein cholesterol (HDL-C) levels, and an increase in sdLDL particles [82]. In MASLD, metabolic dysregulation exacerbates lipid metabolism, impacting cardiovascular health. High levels of cholesterol, which is essential for cell membrane function and the synthesis of hormones and bile acids, are a concern. This may indicate an increase in atherogenic lipoproteins, which can be deposited in the arterial walls. In MASLD, the altered metabolic state of the liver can lead to increased production and decreased clearance of lipoproteins, resulting in elevated total cholesterol levels [51]. LDL cholesterol, often referred to as “bad” cholesterol, is a significant contributor to atherosclerosis due to its role in plaque formation. MASLD patients may experience increased secretion of VLDL, which is converted to LDL after TG removal. This can lead to arterial wall thickening and hardening, heightening the risk of coronary heart disease and other cardiovascular events [50]. TG serves as the body’s primary energy reserve and is converted from excess caloric intake to TG and is stored in adipose tissue or the liver. Elevated TG levels are associated with an increased risk of CVD, as they can directly and indirectly contribute to atherosclerosis by forming sdLDL particles that are particularly atherogenic [83]. HDL-C, known for its protective role against atherosclerosis through reverse cholesterol transport, is often reduced in MASLD patients. This decrease can be attributed to increased clearance of HDL particles from circulation and alterations in enzymes and transfer proteins that modify HDL, such as lecithin cholesterol acyltransferase (LCAT) and cholesterol ester transfer protein (CETP) [84]. In short, the convergence of high TGs, low HDL-C, and the presence of small, dense LDL particles creates a lipid profile that significantly promotes atherosclerosis. Coupled with the proinflammatory state and IR characteristic of MASLD, the risk of cardiovascular events is substantially increased.
MASLD and hypertension
MASLD and hypertension share a reciprocal relationship, with each exacerbating the other’s development and progression [85]. IR is a hallmark of MASLD and can elevate sympathetic nervous system activity, resulting in increased blood pressure. Additionally, IR may lead to renal salt and water retention, contributing to hypertension through increased blood volume [86]. Chronic low-grade inflammation associated with MASLD can also impact the vasculature, promoting vasoconstriction and elevating blood pressure [87]. Evidence from genetically modified mice implicates angiotensinogen from adipose tissue in blood pressure regulation [88]. In humans, a gain-of-function variant in the angiotensin receptor type 1 gene (AGTR1), specifically rs5186 A1166C, is linked to hypertension in individuals with MASLD [89]. This finding suggested that MASLD could intensify the renin-angiotensin-aldosterone system (RAAS), leading to vasoconstriction and increased blood volume, both of which further increase blood pressure. Given this interplay, a concurrent management approach for MASLD and hypertension is warranted to address their mutual reinforcement.
MASLD and T2DM
There is a significant interconnection between MASLD and T2DM, with more than 70% of T2DM patients presenting MASLD [90]. Recent studies have indicated that MASLD patients with T2DM, including nondiabetic MASLD patients who are overweight/obese or have other metabolic risk factors, experience more adverse clinical outcomes than those without T2DM [91]. The relationship between these conditions is bidirectional, with MASLD increasing the risk of developing T2DM, in turn exacerbating the progression of MASLD [92]. The advancement of MASLD to liver fibrosis and hepatocellular carcinoma is closely tied to T2DM, and the presence of MASLD heightens the risk of all-cause mortality and CVD in individuals with T2DM [93, 94]. Hence, early recognition and management of CVD risk are imperative for individuals with MASLD, especially those with comorbid T2DM.
MASLD and correlated CVD risk factors
MASLD is closely associated with various types of CVD, as it is associated with numerous CVD risk factors. A systematic review and meta-analysis suggested that NAFLD is associated with an increased risk of CAC progression over time [95]. A cross-sectional and longitudinal study comparing NAFLD and MASLD with CAC also suggested that both NAFLD and MASLD may increase the incidence of CAC, with the association being stronger for MASLD [96]. These findings imply a propensity for MASLD patients to develop coronary artery disease (CAD). In addition to CAC, the association between MASLD and the risk of MI or stroke was investigated in a large prospective cohort study. These findings showed that MASLD and its subtypes are associated with the occurrence of major adverse cardiovascular events (MACEs) [97]. Another study focused on the effects of MASLD on left ventricular diastolic function and cardiac morphology and revealed a significantly greater prevalence of left ventricular diastolic dysfunction (LVDD) and cardiac remodeling in MASLD patients, particularly in the MASLD subgroups with overweight and diabetes [98], indicating a potential association with heart failure. A large Chinese cohort study with a follow-up of 14.01 years reported a greater incidence of heart failure in MASLD patients, with worsening fatty liver disease associated with an increased risk of heart failure [99]. This association was particularly pronounced in individuals under 45 years of age, emphasizing the significant increase in risk between MASLD and heart failure in younger populations [100]. In addition, another large cohort study revealed a significant association between MASLD and a greater risk of prevalent and incident atrial fibrillation (AF), emphasizing the link between MASLD and the risk of cardiac arrhythmias [101]. These findings highlight the importance of recognizing MASLD as a critical component in CV risk assessment screening, as it is closely associated with various forms of CVD.
MASLD and its multifaceted CVD complications
MASLD is closely linked to a spectrum of CVD complications due to its association with metabolic dysfunction (Fig. 3). In MASLD, cardiovascular complications such as coronary heart disease, angina, and MI stem predominantly from accelerated atherosclerosis, characterized by lipid deposition in arterial walls. Research evidence suggests that patients with MI who also have MASLD face a significantly higher mortality risk compared to those with MI alone, underscoring the potential of MASLD as an independent risk factor for coronary heart disease [102]. Furthermore, MI has been observed to disrupt systemic homeostasis and enhance the expression of profibrotic mediators, which may initiate inter-disease signaling pathways and exacerbate the progression of hepatic fibrosis in MASLD [103]. These findings bolster the established correlation between MASLD and ASCVD. The condition also raises the incidence of ischemic stroke due to atherosclerotic changes in cerebral arteries [97]. Additionally, MASLD may be exacerbated by the comorbidity of heart failure. A substantial cohort study in China, encompassing 98,685 individuals, indicated a positive correlation between MASLD and an elevated risk of heart failure. The study findings also highlighted that the severity of fatty liver disease is significantly associated with the heightened susceptibility to heart failure [99]. A meta-analysis investigating the correlation between MASLD and AF has indicated a marked elevation in the risk of AF among middle-aged and elderly individuals afflicted with MASLD, with a particularly pronounced risk among diabetic patients [104]. This finding is complemented by subsequent research, which posits that the presence of fatty liver disease per se may not be linked to the prevalence or incidence of AF. In contrast, it is the increased liver stiffness, a marker of liver fibrosis, that exhibits a significant correlation with AF risk, notably in patients without evidence of fatty degeneration [105]. These insights underscore the intricate relationship between hepatic function, fibrosis, and arrhythmias. Looking ahead, the scientific community anticipates an escalation in research endeavors focusing on the cardiovascular complications associated with MASLD, with a particular emphasis on diverse cardiovascular conditions. These studies aim to robustly substantiate the correlation between MASLD and CVD, providing a more comprehensive understanding of this complex clinical interplay.

MASLD and its multifaceted CVD complications (Created with BioRender.com). MASLD: metabolic dysfunction-associated steatotic liver disease, CVD: cardiovascular disease
Noninvasive imaging techniques and biomarkers for the assessment of CVD risk in patients with MASLD
CVD risk assessment in patients with MASLD is crucial for the prevention and management of potential cardiovascular events. Noninvasive imaging techniques and biomarkers play important roles in risk assessment (Table 2).
Transient elastography and acoustic radiation force impulse imaging
Transient elastography (TE) is a noninvasive technique for assessing liver fibrosis by measuring tissue stiffness, which indicates the degree of fibrosis. This method offers a quick, easy and patient-friendly alternative to invasive liver biopsy and is valuable for monitoring disease progression and treatment efficacy in chronic liver disease patients, including patients with MASLD, where fibrosis is an important indicator of disease progression and a risk factor for CVD [106]. TE is accurate for the diagnosis of severe fibrosis or cirrhosis but less accurate for mild to moderate stages. Measurements can be affected by obesity, inflammation or other liver diseases and are less effective for the assessment of hepatic steatosis [107]. Despite these limitations, TE is recommended in international hepatology guidelines as the preferred method for fibrosis assessment because it is noninvasive. TE also helps to stratify CVD risk in MASLD patients to enable targeted treatment [108]. A recent scholarly article has emphasized that an elevated liver stiffness measurement (LSM) serves as a sophisticated alternative for evaluating liver fibrosis and is correlated with an increased risk of cardiovascular events in individuals with MASLD [109].This technique is an active area of research with growing potential and provides a valuable tool for the management of liver fibrosis and CVD risk in MASLD patients.
Acoustic radiation force impulse imaging (ARFI) is an ultrasound-based technology that assesses the extent of liver fibrosis by measuring the elasticity of liver tissue. ARFI imaging uses short-lived mechanical pressure waves generated by acoustic radiation to push the tissue and then calculates the displacement of the tissue based on changes in the echo signal, providing elastic information about the tissue [110]. Compared to TE, ARFI does not require special cooperation from the patient to breathe, which facilitates the operation and is particularly suitable for patients who have difficulty breathing or who are unable to cooperate. The ARFI provides a quantitative method for measuring liver elasticity that can be used to create an elastogram to visually depict the degree of fibrosis in different areas of the liver. Studies have shown that ARFI is highly accurate in diagnosing liver fibrosis, particularly in identifying significant liver fibrosis and cirrhosis [111, 112]. Similar to TE, the accuracy of ARFI measurement can be affected by factors such as obesity and liver inflammation. The higher the shear wave velocity, the stiffer the tissue. The application of this technology in the carotid artery can predict ASCVD risk. As ARFI is based on existing ultrasound equipment, it may have advantages in terms of cost-effectiveness.
Both TE and ARFI are mounted on devices by which is also possible to determine fat quantification and their employment in this scenario is improving a lot [113, 114]. Probably if we consider that ARFI is mounted on an ultrasound scanner by which is possible with the same machine to evaluate the fat in the liver, but also the fat in the belt, together with the presence of atherosclerosis in carotid arteries, abdominal aorta and in the arteries of the lower limb, it could be considered the most complete device to determine the CVD risks of these patients. Future research could focus on further optimizing ARFI technology, using it in combination with other biomarkers and evaluating its diagnostic performance in different liver diseases and CVD risk.
Magnetic resonance elastography and spectroscopy
Magnetic resonance elastography (MRE) is an advanced, noninvasive imaging technology that quantifies the extent of liver fibrosis and fatty liver by assessing the elasticity of liver tissue. MRE uses magnetic resonance imaging (MRI) to excite tiny vibrations in liver tissue with special pulses, and then the elasticity of the tissue is calculated by analyzing the propagation of these vibrations [115]. MRE is currently under investigation for its utility in cardiac diagnostics. This technique holds promise for the early identification and surveillance of cardiovascular conditions through the quantification of myocardial and vascular stiffness, as well as the detection of minute alterations in tissue elasticity [116].MRE has shown greater sensitivity and greater accuracy than TE in diagnosing significant liver fibrosis and cirrhosis [117]. Unlike computed tomography (CT) scans, MREs do not use radiation, making them safer options for repeat examinations. However, MREs are associated with higher costs and more specific equipment requirements, which may limit their availability in some areas.
Magnetic resonance spectroscopy (MRS) is another magnetic resonance technique that focuses on measuring fat content in the liver. MRS utilizes chemical shifts to distinguish hydrogen atoms in different molecular environments (e.g., hydrogen atoms in water and lipids) to quantify the intrahepatic fat concentration. MRS can accurately measure the amount of fat in the liver and is very useful in the assessment of fatty liver disease [118]. MRS can also identifies metabolic derangements, such as increased TG and lactate levels, which are suggestive of myocardial stress and ischemia. Additionally, MRS can accurately delineate lipid-rich atherosclerotic plaques in the arterial vasculature, a critical risk factor for CAD and cerebrovascular events [119]. When combined with MRS, MRE can simultaneously assess liver fibrosis and fatty liver, providing a more comprehensive picture of liver health and making it an important tool in the investigation of MASLD and CVD risk.
Biomarkers and noninvasive scoring systems
Biomarkers and noninvasive scoring systems play important roles in the assessment of MASLD and CVD risk. These tools can help physicians assess patients’ disease status and risk without the need for liver biopsies or invasive cardiac testing [120]. The AST to plate ratio index (APRI) and the fibrosis-4 (FIB-4) index are two widely validated hematologic indices that are widely used due to their ease of collection and rapid availability of clinical data. The APRI is a simple model that was originally developed to predict significant fibrosis and cirrhosis in hepatitis C virus (HCV)-infected patients. However, the APRI has shown lower diagnostic accuracy in predicting advanced fibrosis in patients with other causes of chronic lung disease. Similarly, the APRI has lower prognostic accuracy for fibrosis in patients with MASLD [108]. The FIB-4 index is a well-studied, simple algorithm that was first validated in HCV-infected patients. Elevated FIB-4 scores are indicative of advanced liver fibrosis, which is associated with systemic inflammation and an increased prothrombotic state. It has been identified as an independent predictor of MACEs in patients with MASLD [121]. These events include MI, hospitalization due to unstable angina or heart failure, and coronary revascularization. A study analyzing data from 81,108 patients showed that a FIB-4 score of ≥ 2.67 was a significant predictor of MACEs, even after adjusting for established CV risk factors [122]. A recent study has identified a link between the FIB-4 index and aortic valve sclerosis (AVS), a degenerative condition marked by valve leaflet thickening and calcification. Given the high prevalence of AVS in older adults and its correlation with elevated cardiovascular morbidity and mortality, the FIB-4 index may emerge as a valuable predictor for AVS, reinforcing its utility in CV risk profiling [123].The NAFLD fibrosis score (NFS) is an alternative non-invasive method for assessing the degree of hepatic fibrosis in patients with MASLD. Research indicates that higher NFS values are associated with an increased risk of MACEs. Specifically, the risk of MACEs escalates with higher NFS values, with a hazard ratio (HR) of 1.938 for the intermediate NFS group compared to the low NFS group, and an HR of 3.492 for the high NFS group [124]. Although the APRI, NFS, and FIB-4 score have been extensively studied, FIB-4 is the most effective and has the highest prognostic accuracy [125]. However, another study demonstrated that liver fibrosis biomarkers, particularly the Forns index and Hepamet fibrosis score (HFS), are highly effective in ruling out advanced liver fibrosis and are positively correlated with CV risk, providing valuable insights for clinical risk stratification in patients with chronic liver disease [126].
The pericoronary fat attenuation index (FAI) is a new method for assessing the risk of cardiac death and reflects pericoronary inflammation [127]. One study revealed that the FAI on coronary computed tomography angiography (CCTA) is greater in patients with MASLD and that MASLD patients with a greater FAI have worse cardiovascular outcomes [128]. In light of these findings, high vascular inflammation may play a role in the progression of CVD in patients with MASLD. In short, MASLD patients should be screened using the FIB-4 index, HFS and LSM to determine the extent of liver fibrosis. If the score is high, CVD screening should be performed proactively, especially CCTA screening in patients with CVD symptoms such as chest pain.
These noninvasive imaging techniques and biomarkers provide an effective means of assessing CVD risk in patients with MASLD and facilitate early diagnosis, risk stratification and treatment decisions. However, their application requires further validation and optimization in clinical practice.
Implications for clinical management and prevention strategies for CVD risk in MASLD patients
The presence of MASLD significantly increases the risk of CVD in affected individuals. Therefore, it is critical for clinicians to apply appropriate clinical management and prevention strategies to reduce CVD risk in patients with MASLD (Fig. 4).

Potential preventive and therapeutic strategies for CVD risk in MASLD (Created with BioRender.com). MASLD: metabolic dysfunction-associated steatotic liver disease, CVD: cardiovascular disease, DM: diabetes mellitus, GLP-1: glucagon-like Peptide 1, SGLT-2: sodium glucose-linked transporter 2, ACEI: angiotensin-converting enzyme inhibitor, ARB: angiotensin receptor blocker, MASH: metabolic dysfunction-associated steatohepatitis, TZDs: thiazolidinediones
Lifestyle modifications
Encouraging patients with MASLD to adopt a healthy lifestyle is essential both for the treatment of MASLD and for reducing CVD risk. This includes encouraging regular physical activity, eating a balanced diet with plenty of fruit, vegetables, whole grains and lean protein, and maintaining a healthy weight. Recently, a study reported that eating between meals and eating quickly is a risk factor for the onset of MASLD in both men and women, while walking quickly is a protective factor against the onset of MASLD in women [129]. This means that changing these lifestyle factors may help prevent the onset of MASLD. In addition, weight loss, particularly through a combination of diet and exercise, can help improve liver health and reduce CVD risk factors such as high cholesterol and high blood pressure.
Monitoring and treatment of risk factors
Regular monitoring and treatment of CVD risk factors such as obesity, hypertension, dyslipidemia, and diabetes are essential in patients with MASLD. In overweight and obese patients with MASLD, weight loss of 7–10% is necessary to reduce hepatic steatosis and vascular and metabolic complications [130].
Recommendations for the treatment of MASLD and prevention of CVD include a low-carbohydrate, ketogenic, low-fat, high-protein Mediterranean diet, which can reduce dyslipidemia, fatty liver disease and associated comorbidities [131]. On the other hand, there is relevant evidence that smoking promotes the development of MASLD through direct and indirect mechanisms [132]. Since smoking is an established CV risk factor and smoking cessation is crucial for the prevention of cardiovascular events, smoking cessation is also advised in patients with MASLD. A nonnegligible fact is that bariatric surgery can induce weight loss and mitigate the harmful effects of MS and T2DM. Recent data suggest that bariatric surgery has significant effects on glucagon-like peptide-1 (GLP-1) and other gut hormones and produces important beneficial changes in lipid, metabolic, and inflammatory abnormalities in MASLD patients [133]. Therefore, bariatric surgery may reverse some pathological changes in the liver and reduce cardiovascular outcomes in patients with MASLD and MASH.
Pharmacological interventions
Pharmacological interventions may be necessary to treat MASLD and reduce CVD risk. These medications may target various aspects of the pathophysiology of MASLD and associated metabolic abnormalities to improve liver health and reduce the risk of cardiovascular complications [134] (Table 3).
Medication intervention for hepatic steatosis
MASLD is a hepatic manifestation of MS, characterized by the accumulation of lipids within hepatocytes, leading to a spectrum of liver diseases ranging from simple steatosis to MASH and cirrhosis. The management of MASLD, particularly its steatotic component, is crucial due to its strong association with CVD. In this context, pharmacological interventions have emerged as pivotal strategies to mitigate liver fat accumulation and reduce the attendant CV risks.
Thiazolidinediones (TZDs), a class of peroxisome proliferator-activated receptor gamma (PPARγ) agonists, have been instrumental in the management of T2DM and have shown promise in the treatment of liver steatosis in MASLD, at the same time, it has been shown to have potential beneficial effects on CV risk factors [135]. By activating PPARγ, TZDs enhance insulin sensitivity, thereby reducing hepatic fat accumulation and improving overall metabolic health. A recent study suggested that the novel dual PPARα/γ agonist (G4/G5) can prevent hepatic fatty degeneration by upregulating PPARα and improve systemic insulin sensitivity by increasing PPARγ. It can also inhibit the adverse effects of obesity such as weight gain, adipocyte hypertrophy and fluid retention, and is safer than TZDs [136]. On the other side, one research demonstrates that semaglutide, as a novel GLP-1 receptor agonist modulates the gut microbiota, improves lipid levels and glucose metabolism, leading to a significant improvement in MASLD, thus validating its potential as a therapeutic intervention for hepatic steatosis [137]. In addition,,a randomized controlled trial (RCT) evaluated the efficacy of the sodium-glucose transporter 2(SGLT-2) inhibitor empagliflozin in non-diabetic patients with MASLD. The study demonstrated significant reductions in liver fat content, with median levels dropping from approximately 10% at baseline to notably lower levels after 52 weeks of treatment [138]. These pharmacological agents are shown to diminish hepatic steatosis, thereby mitigating the progression of liver fat accumulation and subsequently lowering the incidence of CV risk factors.
Medication intervention for liver fibrosis
In the context of MASLD, pharmacological interventions for liver fibrosis encompass a spectrum of therapies. Vitamin E is one of the most promising drugs for the treatment of MASH. A retrospective analysis of patients with MASH confirmed by liver biopsy suggested that treatment for 2 years or longer may improve MASH fibrosis [139]. The FLINT trial evaluated the efficacy and safety of obeticholic acid (OCA), a farnesoid X nuclear receptor agonist, in adults with non-cirrhotic, MASH. The study found that OAC significantly improved liver histology, including steatosis, inflammation, hepatocyte ballooning, and fibrosis, compared to placebo, but also resulted in higher rates of pruritus and changes in serum cholesterol levels [140]. Recently, SYNERGY-NASH trial investigated the efficacy and safety of tirzepatide, a novel dual glucose- dependent insulinotropic polypeptide (GIP) and GLP-1 receptor agonist, in patients with MASH and moderate or severe fibrosis, demonstrating significantly higher resolution of MASH without fibrosis worsening compared to placebo. The trial suggests that 52 weeks of tirzepatide treatment is more effective than placebo for MASH resolution without exacerbating fibrosis [141]. Resmetirom, a liver-targeting agent that targets the thyroid hormone beta receptor, has been shown to be effective in reducing liver fat content, improving liver histology ((MASH) dissolution and improving fibrosis) and improving biomarkers of liver damage without significantly affecting body weight or glucose metabolism [142]. The phase 2b ENLIVEN trial has shown that pegozafermin, a fibroblast growth factor 21 (FGF21) analogue, leads to significant amelioration of liver fibrosis without worsening MASH in patients with biopsy-confirmed MASH. These findings indicate a potential therapeutic advantage for pegozafermin in MASH resolution and support its advancement to phase 3 clinical trials, highlighting its potential as a novel treatment for MASH and associated liver fibrosis [143]. Meanwhile, a phase 2 randomized trial has demonstrated that survodutide, a dual agonist of the glucagon receptor and GLP-1 receptor, significantly ameliorates MASH without exacerbating liver fibrosis in patients with this condition. These findings underscore the promise of survodutide as a therapeutic candidate, warranting its advancement into phase 3 clinical trials for the treatment of MASH and associated liver fibrosis [144]. Notably, these drugs can improve metabolic status and reduce CV risk, which holds good therapeutic promise.
Pharmacological interventions evaluating inflammation in MASLD
In the realm of MASLD, the pharmacological management of inflammation represents a pivotal therapeutic strategy. Agents that target inflammatory pathways have demonstrated potential to attenuate hepatic inflammation, a key component of MASLD pathogenesis. Current pharmacological strategi-es to curb inflammation in MASLD include the utilization of nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroids, and potentially novel agents such as statins and pentoxifylline, which have demonstrated anti-inflammatory properties. These interventions aim to reduce the hepatic inflammatory response, a key driver of disease progression.
Acetylsalicylic acid remains the cornerstone of antiplatelet therapy for ASCVD [145]. One study suggest that daily aspirin use may reduce the risk of fibrosis progression in patients with MASLD [146]. Additionally, previous evidence has established that MASLD is an independent risk factor for AF. Consequently, it is anticipated that an increasing cohort of patients with advanced fatty liver disease, including those progressed to MASH, will be considered for antithrombotic therapy in the forthcoming years. Moreover, given the association between inflammation, coagulation system activation, and hepatic fibrosis progression. Intriguingly, antithrombotic treatment may exert salutary effects on liver fibrosis as well [147].
Therefore, patients with MASLD should be treated with ASA/ oral anticoagulants according to the recommendations for the prevention of cardiovascular events.
Dyslipidemia plays an important role in the progression of MASLD and CVD. Among lipid-lowering drugs, statins are the most commonly prescribed, most effective and best documented. These agents can reduce CV risk, although statins can increase transaminase levels. Patients with mildly elevated transaminase levels but MASLD should not stop taking statins for primary and secondary prevention of cardiovascular events because statins have anti-inflammatory, antioxidant, antifibrotic, and plaque-stabilizing effects that can improve MASLD patients. They improve vascular and liver function and reduce CV risk, and their safety has been confirmed in MASLD patients [148, 149].
There is growing evidence that MASLD, an underrecognized metabolic abnormality, is closely associated with an increased risk of prehypertension and hypertension [87]. The development of hypertension is more likely in patients with advanced MASLD than in those with normal or mild MASLD, suggesting that MASLD is an independent risk factor for hypertension [150]. In addition, prevalent MASLD may lead to the development of hypertension early in life even in the absence of other metabolic risk factors. Controlling blood pressure in nonobese hypertensive patients may help to prevent or limit MASLD [151]. Although beta-blockers can suppress the stress response to hypoglycemia in MASLD patients treated concomitantly with T2DM, angiotensin receptor blockers (ARB), on the other hand, have anti-inflammatory and antifibrotic effects, and the RAAS is involved in the development of MASLD and CVD; therefore, angiotensin converting enzyme inhibitors (ACEI) /ARB have become potential drugs for the treatment of MASLD. However, studies have confirmed that caution should be exercised when expanding the use of ACEIs/ARBs for the sole purpose of controlling fibrosis in patients with MASLD [152].
Conclusion
MASLD is strongly associated with an increased risk of CVD, and this association is mediated by several metabolic disorders, including obesity, T2DM, hypertension, and dyslipidemia. The global prevalence of MASLD is increasing, and MASLD is associated with unhealthy lifestyle factors, which include increased liver fat content and the presence of metabolic abnormalities. Pathological mechanisms include IR, chronic inflammation, OS, endothelial dysfunction, abnormal lipid metabolism, genetic susceptibility, etc. All these factors favor the development of atherosclerosis and multiple-CVD. Patients with MASLD have a significantly increased risk of cardiovascular events. Therefore, early assessment of CV risk, noninvasive screening and management of these patients are crucial. Treatment of MASLD focuses on lifestyle improvement and, if necessary, medication. Future research directions may focus on discovering new biomarkers and exploring therapeutic targets, as well as evaluating the efficacy of various interventions to reduce CVD risk in patients with MASLD.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- ACEI:
-
Angiotensin converting enzyme inhibitors
- ADMA:
-
Asymmetric dimethylarginine
- AF:
-
Atrial fibrillation
- AGTR1:
-
Angiotensin receptor type 1 gene
- APRI:
-
AST to plate ratio index
- ARB:
-
Angiotensin receptor blockers
- ARFI:
-
Acoustic radiation force impulse imaging
- ASCVD:
-
Atherosclerotic cardiovascular disease
- AVS:
-
Aortic valve sclerosis
- CAC:
-
Coronary artery calcification
- CAD:
-
Coronary artery disease
- CAP:
-
Controlled attenuation parameter
- CCTA:
-
Coronary computed tomography angiography
- CETP:
-
Cholesterol ester transfer protein
- CRP:
-
C-reactive protein
- CT:
-
Computed tomography
- CV risk:
-
Cardiovascular risk
- CVD:
-
Cardiovascular disease
- ET-1:
-
Endothelin-1
- eNOS:
-
Endothelial NO synthase
- FAI:
-
Fat attenuation index
- FFAs:
-
Free fatty acids
- FGF21:
-
Fibroblast growth factor 21
- FIB-4:
-
Fibrosis-4
- FXR:
-
Faresoid X Receptor
- GIP:
-
Glucose- dependent insulinotropic polypeptide
- GLP-1:
-
Glucagon-like peptide-1
- GGT:
-
Gamma-glutamyltransferase
- HCV:
-
Hepatitis C virus
- HDL-C:
-
High-density lipoprotein cholesterol
- HFS:
-
Hepamet fibrosis score
- HOMA-IR:
-
Homeostatic model assessment for insulin resistance
- HR:
-
Hazard ratio
- IL-6:
-
Interleukin-6
- IR:
-
Insulin resistance
- I148M:
-
Isoleucine to methionine at position 148
- LCAT:
-
Lecithin cholesterol acyltransferase
- LSM:
-
Liver stiffness measurement
- LVDD:
-
Left ventricular diastolic dysfunction
- MACEs:
-
Major adverse cardiovascular events
- MAFLD:
-
Metabolic -associated fatty liver disease
- MASH:
-
Metabolic dysfunction-associated steatohepatitis
- MASLD:
-
Metabolic dysfunction-associated steatotic liver disease
- MBOAT7:
-
Membrane-bound O-acyltransferase domain 7
- MetALD:
-
Metabolic and alcohol related/associated liver disease
- MI:
-
Myocardial infarction
- MRI:
-
Magnetic resonance imaging
- MRE:
-
Magnetic resonance elastography
- MRS:
-
Magnetic resonance spectroscopy
- MS:
-
Metabolic syndrome
- NAFLD:
-
Nonalcoholic fatty liver disease
- NFS:
-
NAFLD fibrosis score
- NF-κB:
-
Nuclear factor kappa-B
- NO:
-
Nitric oxide
- NSAIDs:
-
Nonsteroidal anti-inflammatory drugs
- OCA:
-
Obeticholic acid
- OS:
-
Oxidative stress
- ox-LDL:
-
Oxidized low-density lipoprotein
- PAFV:
-
Periaortic fat volume
- PAI-1:
-
Plasminogen activator inhibitor-1
- PNPLA3:
-
Phospholipase domain-containing protein 3
- PPARγ:
-
Peroxisome proliferator-activated receptor gamma
- RAAS:
-
Renin-angiotensin-aldosterone system
- RCT:
-
Randomized controlled trial
- ROS:
-
Reactive oxygen species
- SAA:
-
Serum amyloid A
- SCFAs:
-
Short-chain fatty acids
- sdLDL:
-
Small dense low-density lipoprotein
- SGLT-2:
-
Sodium-glucose transporter 2
- SNP:
-
Single nucleotide polymorphism
- SREBP-1:
-
Sterol regulatory element-binding protein 1
- TE:
-
Transient elastography
- TG:
-
Triglyceride
- TMA:
-
Trimethylamine
- TMAO:
-
Trimethylamine N-oxide
- TM6SF2:
-
Transmembrane 6 superfamily member 2
- TNF-α:
-
Tumor necrosis factor-alpha
- TZDs:
-
Thiazolidinediones
- T2DM:
-
Type 2 diabetes mellitus
- VAT:
-
Visceral adipose tissue
- VCTE:
-
Vibration-controlled transient elastography
- VLDL:
-
Very low-density lipoprotein
References
Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84.
Targher G, Byrne CD, Tilg H. MASLD: a systemic metabolic disorder with cardiovascular and malignant complications. Gut. 2024;73(4):691–702.
Eslam M, Newsome PN, Sarin SK, Anstee QM, Targher G, Romero-Gomez M, Zelber-Sagi S, Wai-Sun Wong V, Dufour JF, Schattenberg JM, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73(1):202–9.
Gofton C, Upendran Y, Zheng MH, George J. MAFLD: how is it different from NAFLD? Clin Mol Hepatol. 2023;29(Suppl):S17–31.
Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, Kanwal F, Romero D, Abdelmalek MF, Anstee QM, Arab JP, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;79(6):1542–56.
Diehl AM, Day C. Cause, Pathogenesis, and treatment of Nonalcoholic Steatohepatitis. N Engl J Med. 2017;377(21):2063–72.
Kaya E, Yilmaz Y. Metabolic-associated fatty liver Disease (MAFLD): a multi-systemic disease beyond the liver. J Clin Transl Hepatol. 2022;10(2):329–38.
Tsutsumi T, Nakano D, Hashida R, Sano T, Kawaguchi M, Amano K, Kawaguchi T. The Inter-organ Crosstalk reveals an inevitable link between MAFLD and Extrahepatic diseases. Nutrients 2023, 15(5).
Adams LA, Anstee QM, Tilg H, Targher G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut. 2017;66(6):1138–53.
Li AA, Ahmed A, Kim D. Extrahepatic manifestations of nonalcoholic fatty liver disease. Gut Liver. 2020;14(2):168–78.
Lee HH, Lee HA, Kim EJ, Kim HY, Kim HC, Ahn SH, Lee H, Kim SU. Metabolic dysfunction-associated steatotic liver disease and risk of cardiovascular disease. Gut. 2024;73(3):533–40.
Targher G, Byrne CD, Lonardo A, Zoppini G, Barbui C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: a meta-analysis. J Hepatol. 2016;65(3):589–600.
Janssen A, Grobbee DE, Dendale P. Non-alcoholic fatty liver disease, a new and growing risk indicator for cardiovascular disease. Eur J Prev Cardiol. 2020;27(10):1059–63.
Francque SM, van der Graaff D, Kwanten WJ. Non-alcoholic fatty liver disease and cardiovascular risk: pathophysiological mechanisms and implications. J Hepatol. 2016;65(2):425–43.
Stahl EP, Dhindsa DS, Lee SK, Sandesara PB, Chalasani NP, Sperling LS. Nonalcoholic fatty liver disease and the heart: JACC state-of-the-art review. J Am Coll Cardiol. 2019;73(8):948–63.
Choudhary NS, Duseja A. Screening of cardiovascular disease in nonalcoholic fatty liver disease: whom and how? J Clin Exp Hepatol. 2019;9(4):506–14.
Kasper P, Martin A, Lang S, Kutting F, Goeser T, Demir M, Steffen HM. NAFLD and cardiovascular diseases: a clinical review. Clin Res Cardiol. 2021;110(7):921–37.
Pan Z, Shiha G, Esmat G, Mendez-Sanchez N, Eslam M. MAFLD predicts cardiovascular disease risk better than MASLD. Liver Int 2024.
Ciardullo S. The MAFLD-MASLD debate: does cardiovascular risk prediction define the winner? Liver Int. 2024;44(7):1564–6.
Ramirez-Mejia MM, Jimenez-Gutierrez C, Eslam M, George J, Mendez-Sanchez N. Breaking new ground: MASLD vs. MAFLD-which holds the key for risk stratification? Hepatol Int. 2024;18(1):168–78.
Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, Charlton M, Sanyal AJ. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Association for the study of liver diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology. 2012;55(6):2005–23.
Cheng YM, Wang CC, Kao JH. Metabolic associated fatty liver disease better identifying patients at risk of liver and cardiovascular complications. Hepatol Int. 2023;17(2):350–6.
Xu X, Zhou X, Tian T, Ding Y, Yu C, Zhao W, Wang X, Lu J, Guo W, Jiang L, et al. Comparison of clinical characteristics and outcomes of MAFLD and NAFLD in Chinese Health examination populations. J Clin Transl Hepatol. 2023;11(4):777–86.
Hagstrom H, Vessby J, Ekstedt M, Shang Y. 99% of patients with NAFLD meet MASLD criteria and natural history is therefore identical. J Hepatol. 2024;80(2):e76–7.
Kang MK, Song J, Loomba R, Park S, Tak W, Kweon Y, Lee Y, Park JG. Comparative associations of MASLD and MAFLD with the presence and severity of coronary artery calcification. 2024.
Ciardullo S, Mantovani A, Morieri ML, Muraca E, Invernizzi P, Perseghin G. Impact of MASLD and MetALD on clinical outcomes: a meta-analysis of preliminary evidence. Liver Int. 2024;44(8):1762–7.
Choe HJ, Moon JH, Kim W, Koo BK, Cho NH. Steatotic liver disease predicts cardiovascular disease and advanced liver fibrosis: a community-dwelling cohort study with 20-year follow-up. Metabolism. 2024;153:155800.
Aedh AI, Alshahrani MS, Huneif MA, Pryme IF, Oruch R. A glimpse into milestones of insulin resistance and an updated review of its management. Nutrients 2023, 15(4).
Pal SC, Mendez-Sanchez N. Insulin resistance and adipose tissue interactions as the cornerstone of metabolic (dysfunction)-associated fatty liver disease pathogenesis. World J Gastroenterol. 2023;29(25):3999–4008.
Zhao J, Wu Y, Rong X, Zheng C, Guo J. Anti-lipolysis Induced by insulin in diverse pathophysiologic conditions of adipose tissue. Diabetes Metab Syndr Obes. 2020;13:1575–85.
Kosmas CE, Bousvarou MD, Kostara CE, Papakonstantinou EJ, Salamou E, Guzman E. Insulin resistance and cardiovascular disease. J Int Med Res. 2023;51(3):3000605231164548.
Yang K, Song M. New Insights into the pathogenesis of metabolic-associated fatty liver disease (MAFLD): gut-liver-heart crosstalk. Nutrients 2023, 15(18).
Zhao J, Liu L, Cao YY, Gao X, Targher G, Byrne CD, Sun DQ, Zheng MH. MAFLD as part of systemic metabolic dysregulation. Hepatol Int 2024.
Burger K, Jung F, Baumann A, Brandt A, Staltner R, Sanchez V, Bergheim I. TNFalpha is a key trigger of inflammation in diet-induced non-obese MASLD in mice. Redox Biol. 2023;66:102870.
Zhu M, Lei L, Zhu Z, Li Q, Guo D, Xu J, Chen J, Sha H, Zhang X, Yang X, et al. Excess TNF-alpha in the blood activates monocytes with the potential to directly form cholesteryl ester-laden cells. Acta Biochim Biophys Sin (Shanghai). 2015;47(11):899–907.
Rafaqat S, Gluscevic S, Mercantepe F, Rafaqat S, Klisic A. Interleukins: pathogenesis in non-alcoholic fatty liver disease. Metabolites 2024, 14(3).
Duan Y, Pan X, Luo J, Xiao X, Li J, Bestman PL, Luo M. Association of inflammatory cytokines with non-alcoholic fatty liver disease. Front Immunol. 2022;13:880298.
Ngwa DN, Pathak A, Agrawal A. IL-6 regulates induction of C-reactive protein gene expression by activating STAT3 isoforms. Mol Immunol. 2022;146:50–6.
Medina-Leyte DJ, Zepeda-Garcia O, Dominguez-Perez M, Gonzalez-Garrido A, Villarreal-Molina T, Jacobo-Albavera L. Endothelial dysfunction, inflammation and coronary artery disease: potential biomarkers and promising therapeutical approaches. Int J Mol Sci. 2021;22(8).
Castillo-Nunez Y, Almeda-Valdes P, Gonzalez-Galvez G, Arechavaleta-Granell MDR. Metabolic dysfunction-associated steatotic liver disease and atherosclerosis. Curr Diab Rep. 2024;24(7):158–66.
Ma Y, Lee G, Heo SY, Roh YS. Oxidative stress is a key modulator in the development of nonalcoholic fatty liver disease. Antioxid (Basel) 2021, 11(1).
Batty M, Bennett MR, Yu E. The role of oxidative stress in atherosclerosis. Cells 2022, 11(23).
Munzel T, Camici GG, Maack C, Bonetti NR, Fuster V, Kovacic JC. Impact of oxidative stress on the heart and vasculature: part 2 of a 3-Part series. J Am Coll Cardiol. 2017;70(2):212–29.
Colak E, Pap D. The role of oxidative stress in the development of obesity and obesity-related metabolic disorders. J Med Biochem. 2021;40(1):1–9.
Kruger-Genge A, Blocki A, Franke RP, Jung F. Vascular endothelial cell Biology: an update. Int J Mol Sci 2019, 20(18).
Nasiri-Ansari N, Androutsakos T, Flessa CM, Kyrou I, Siasos G, Randeva HS, Kassi E, Papavassiliou AG. Endothelial Cell Dysfunction and Nonalcoholic Fatty Liver Disease (NAFLD): A Concise Review. Cells 2022, 11(16).
Andrabi SM, Sharma NS, Karan A, Shahriar SMS, Cordon B, Ma B, Xie J. Nitric oxide: physiological functions, delivery, and biomedical applications. Adv Sci (Weinh). 2023;10(30):e2303259.
Vairappan B. Endothelial dysfunction in cirrhosis: role of inflammation and oxidative stress. World J Hepatol. 2015;7(3):443–59.
Gunawardena T, Merinopoulos I, Wickramarachchi U, Vassiliou V, Eccleshall S. Endothelial dysfunction and coronary vasoreactivity - A review of the history, physiology, diagnostic techniques, and clinical relevance. Curr Cardiol Rev. 2021;17(1):85–100.
Shimabukuro M. MAFLD and small dense LDL cholesterol: a mechanistic link. J Atheroscler Thromb. 2024;31(1):17–8.
Heeren J, Scheja L. Metabolic-associated fatty liver disease and lipoprotein metabolism. Mol Metab. 2021;50:101238.
Virovic-Jukic L, Stojsavljevic-Shapeski S, Forgac J, Kukla M, Mikolasevic I. Non-alcoholic fatty liver disease - a procoagulant condition? Croat Med J. 2021;62(1):25–33.
Ogresta D, Mrzljak A, Cigrovski Berkovic M, Bilic-Curcic I, Stojsavljevic-Shapeski S, Virovic-Jukic L. Coagulation and endothelial dysfunction Associated with NAFLD: current status and therapeutic implications. J Clin Transl Hepatol. 2022;10(2):339–55.
Gallo G, Savoia C. New insights into endothelial dysfunction in cardiometabolic diseases: potential mechanisms and clinical implications. Int J Mol Sci 2024, 25(5).
Shabalala SC, Dludla PV, Mabasa L, Kappo AP, Basson AK, Pheiffer C, Johnson R. The effect of adiponectin in the pathogenesis of non-alcoholic fatty liver disease (NAFLD) and the potential role of polyphenols in the modulation of adiponectin signaling. Biomed Pharmacother. 2020;131:110785.
Martinez-Una M, Lopez-Mancheno Y, Dieguez C, Fernandez-Rojo MA, Novelle MG. Unraveling the role of leptin in liver function and its relationship with Liver diseases. Int J Mol Sci 2020, 21(24).
Vilarino-Garcia T, Polonio-Gonzalez ML, Perez-Perez A, Ribalta J, Arrieta F, Aguilar M, Obaya JC, Gimeno-Orna JA, Iglesias P, Navarro J et al. Role of leptin in obesity, Cardiovascular Disease, and type 2 diabetes. Int J Mol Sci 2024, 25(4).
Kirichenko TV, Markina YV, Bogatyreva AI, Tolstik TV, Varaeva YR, Starodubova AV. The role of Adipokines in inflammatory mechanisms of obesity. Int J Mol Sci 2022, 23(23).
Lim S, Meigs JB. Links between ectopic fat and vascular disease in humans. Arterioscler Thromb Vasc Biol. 2014;34(9):1820–6.
Kozawa J, Shimomura I. Ectopic fat accumulation in pancreas and heart. J Clin Med 2021, 10(6).
Sakurai Y, Kubota N, Yamauchi T, Kadowaki T. Role of insulin resistance in MAFLD. Int J Mol Sci 2021, 22(8).
Berardo C, Di Pasqua LG, Cagna M, Richelmi P, Vairetti M, Ferrigno A. Nonalcoholic fatty liver disease and non-alcoholic steatohepatitis: current issues and future perspectives in preclinical and clinical research. Int J Mol Sci 2020, 21(24).
D’Oria R, Genchi VA, Caccioppoli C, Calderoni I, Marrano N, Biondi G, Borrelli A, Di Gioia L, Giorgino F, Laviola L. Impact of dysfunctional adipose tissue depots on the cardiovascular system. Int J Mol Sci 2022, 23(22).
Kenchaiah S, Ding J, Carr JJ, Allison MA, Budoff MJ, Tracy RP, Burke GL, McClelland RL, Arai AE, Bluemke DA. Pericardial Fat and the risk of heart failure. J Am Coll Cardiol. 2021;77(21):2638–52.
Zhu J, Yang Z, Li X, Chen X, Pi J, Zhuang T, Liu J, Li G, Peng S, Zhang L, et al. Association of periaortic fat and abdominal visceral fat with coronary artery atherosclerosis in Chinese middle aged and elderly patients undergoing computed tomography coronary angiography. Glob Heart. 2021;16(1):74.
Cherubini A, Casirati E, Tomasi M, Valenti L. PNPLA3 as a therapeutic target for fatty liver disease: the evidence to date. Expert Opin Ther Targets. 2021;25(12):1033–43.
Shen JH, Li YL, Li D, Wang NN, Jing L, Huang YH. The rs738409 (I148M) variant of the PNPLA3 gene and cirrhosis: a meta-analysis. J Lipid Res. 2015;56(1):167–75.
Luukkonen PK, Qadri S, Lehtimaki TE, Juuti A, Sammalkorpi H, Penttila AK, Hakkarainen A, Orho-Melander M, Arola J, Yki-Jarvinen H. The PNPLA3-I148M variant confers an antiatherogenic lipid profile in insulin-resistant patients. J Clin Endocrinol Metab. 2021;106(1):e300–15.
Huang G, Wallace DF, Powell EE, Rahman T, Clark PJ, Subramaniam VN. Gene variants implicated in steatotic liver disease: opportunities for diagnostics and therapeutics. Biomedicines 2023, 11(10).
Dongiovanni P, Petta S, Maglio C, Fracanzani AL, Pipitone R, Mozzi E, Motta BM, Kaminska D, Rametta R, Grimaudo S, et al. Transmembrane 6 superfamily member 2 gene variant disentangles nonalcoholic steatohepatitis from cardiovascular disease. Hepatology. 2015;61(2):506–14.
Jonas W, Schurmann A. Genetic and epigenetic factors determining NAFLD risk. Mol Metab. 2021;50:101111.
Song Q, Zhang X. The role of gut-liver axis in gut microbiome dysbiosis associated NAFLD and NAFLD-HCC. Biomedicines 2022, 10(3).
Han H, Jiang Y, Wang M, Melaku M, Liu L, Zhao Y, Everaert N, Yi B, Zhang H. Intestinal dysbiosis in nonalcoholic fatty liver disease (NAFLD): focusing on the gut-liver axis. Crit Rev Food Sci Nutr. 2023;63(12):1689–706.
Zhen J, Zhou Z, He M, Han HX, Lv EH, Wen PB, Liu X, Wang YT, Cai XC, Tian JQ, et al. The gut microbial metabolite trimethylamine N-oxide and cardiovascular diseases. Front Endocrinol (Lausanne). 2023;14:1085041.
Querio G, Antoniotti S, Geddo F, Levi R, Gallo MP. Modulation of endothelial function by TMAO, a gut microbiota-derived metabolite. Int J Mol Sci. 2023;24(6).
Nesci A, Carnuccio C, Ruggieri V, D’Alessandro A, Di Giorgio A, Santoro L, Gasbarrini A, Santoliquido A, Ponziani FR. Gut microbiota and cardiovascular disease: evidence on the metabolic and inflammatory background of a complex relationship. Int J Mol Sci 2023, 24(10).
Al Khodor S, Reichert B, Shatat IF. The Microbiome and Blood pressure: can microbes regulate our blood pressure? Front Pediatr. 2017;5:138.
Wei J, Zhang Y, Dalbeth N, Terkeltaub R, Yang T, Wang Y, Yang Z, Li J, Wu Z, Zeng C, et al. Association between gut microbiota and elevated serum urate in two independent cohorts. Arthritis Rheumatol. 2022;74(4):682–91.
Zhao D, Cui H, Shao Z, Cao L. Abdominal obesity, chronic inflammation and the risk of non-alcoholic fatty liver disease. Ann Hepatol. 2023;28(4):100726.
Gutierrez-Cuevas J, Santos A, Armendariz-Borunda J. Pathophysiological molecular mechanisms of obesity: a link between MAFLD and NASH with cardiovascular diseases. Int J Mol Sci 2021, 22(21).
Dao AD, Nguyen VH, Ito T, Cheung R, Nguyen MH. Prevalence, characteristics, and mortality outcomes of obese and nonobese MAFLD in the United States. Hepatol Int. 2023;17(1):225–36.
Pipitone RM, Ciccioli C, Infantino G, La Mantia C, Parisi S, Tulone A, Pennisi G, Grimaudo S, Petta S. MAFLD: a multisystem disease. Ther Adv Endocrinol Metab. 2023;14:20420188221145549.
Finney AC, Das S, Kumar D, McKinney MP, Cai B, Yurdagul A Jr., Rom O. The interplay between nonalcoholic fatty liver disease and atherosclerotic cardiovascular disease. Front Cardiovasc Med. 2023;10:1116861.
McCullough A, Previs SF, Dasarathy J, Lee K, Osme A, Kim C, Ilchenko S, Lorkowski SW, Smith JD, Dasarathy S, et al. HDL flux is higher in patients with nonalcoholic fatty liver disease. Am J Physiol Endocrinol Metab. 2019;317(5):E852–62.
Golubeva JA, Sheptulina AF, Elkina AY, Liusina EO, Kiselev AR, Drapkina OM. Which comes first, nonalcoholic fatty liver disease or arterial hypertension? Biomedicines 2023, 11(9).
Sata Y, Head GA, Denton K, May CN, Schlaich MP. Role of the sympathetic nervous system and its modulation in renal hypertension. Front Med. 2018;5:82.
Zhao YC, Zhao GJ, Chen Z, She ZG, Cai J, Li H. Nonalcoholic fatty liver disease: an emerging driver of hypertension. Hypertension. 2020;75(2):275–84.
Yiannikouris F, Gupte M, Putnam K, Thatcher S, Charnigo R, Rateri DL, Daugherty A, Cassis LA. Adipocyte deficiency of angiotensinogen prevents obesity-induced hypertension in male mice. Hypertension. 2012;60(6):1524–30.
Musso G, Saba F, Cassader M, Paschetta E, De Michieli F, Pinach S, Framarin L, Berrutti M, Leone N, Parente R, et al. Angiotensin II type 1 receptor rs5186 gene variant predicts Incident NAFLD and Associated hypertension: role of dietary fat-induced pro-inflammatory cell activation. Am J Gastroenterol. 2019;114(4):607–19.
Cho IJ, Oh DH, Yoo J, Hwang YC, Ahn KJ, Chung HY, Jeong SW, Moon JY, Lee SH, Lim SJ, et al. Allopurinol ameliorates high fructose diet induced hepatic steatosis in diabetic rats through modulation of lipid metabolism, inflammation, and ER stress pathway. Sci Rep. 2021;11(1):9894.
Zhou XD, Cai J, Targher G, Byrne CD, Shapiro MD, Sung KC, Somers VK, Chahal CAA, George J, Chen LL, et al. Metabolic dysfunction-associated fatty liver disease and implications for cardiovascular risk and disease prevention. Cardiovasc Diabetol. 2022;21(1):270.
Koutentakis M, Kucinski J, Swieczkowski D, Surma S, Filipiak KJ, Gasecka A. The ketogenic effect of SGLT-2 inhibitors-beneficial or harmful? J Cardiovasc Dev Dis 2023, 10(11).
Stepanova M, Rafiq N, Younossi ZM. Components of metabolic syndrome are independent predictors of mortality in patients with chronic liver disease: a population-based study. Gut. 2010;59(10):1410–5.
Koehler EM, Plompen EP, Schouten JN, Hansen BE, Darwish Murad S, Taimr P, Leebeek FW, Hofman A, Stricker BH, Castera L, et al. Presence of diabetes mellitus and steatosis is associated with liver stiffness in a general population: the Rotterdam study. Hepatology. 2016;63(1):138–47.
Koulaouzidis G, Charisopoulou D, Kukla M, Marlicz W, Rydzewska G, Koulaouzidis A, Skonieczna-Zydecka K. Association of non-alcoholic fatty liver disease with coronary artery calcification progression: a systematic review and meta-analysis. Prz Gastroenterol. 2021;16(3):196–206.
Sung KC, Yoo TK, Lee MY, Byrne CD, Zheng MH, Targher G. Comparative associations of nonalcoholic fatty liver disease and metabolic dysfunction-associated fatty liver disease with coronary artery calcification: a cross-sectional and longitudinal cohort study. Arterioscler Thromb Vasc Biol. 2023;43(3):482–91.
Chen S, Xue H, Huang R, Chen K, Zhang H, Chen X. Associations of MAFLD and MAFLD subtypes with the risk of the incident myocardial infarction and stroke. Diabetes Metab. 2023;49(5):101468.
Peng D, Yu Z, Wang M, Shi J, Sun L, Zhang Y, Zhao W, Chen C, Tang J, Wang C, et al. Association of metabolic dysfunction-associated fatty liver disease with left ventricular diastolic function and cardiac morphology. Front Endocrinol. 2022;13:935390.
Wei Z, Huang Z, Song Z, Zhao W, Zhao D, Tan Y, Chen S, Yang P, Li Y, Wu S. Metabolic dysfunction-associated fatty liver disease and incident heart failure risk: the Kailuan cohort study. Diabetol Metab Syndr. 2023;15(1):137.
Wu S, Li Y, Zhang Y, Su X, Zuo Y, Chen G, Xu G, Chen S, He Y, Wang A. Sex and age differences in the Association between Metabolic Dysfunction-Associated fatty liver disease and heart failure: a prospective cohort study. Circ Heart Fail. 2024;17(2):e010841.
Lei F, Qin JJ, Song X, Liu YM, Chen MM, Sun T, Huang X, Deng KQ, Zuo X, Yao D, et al. The prevalence of MAFLD and its association with atrial fibrillation in a nationwide health check-up population in China. Front Endocrinol (Lausanne). 2022;13:1007171.
Keskin M, Hayiroglu MI, Uzun AO, Guvenc TS, Sahin S, Kozan O. Effect of nonalcoholic fatty liver disease on in-hospital and long-term outcomes in patients with ST-segment elevation myocardial infarction. Am J Cardiol. 2017;120(10):1720–6.
Xie W, Gan J, Zhou X, Tian H, Pan X, Liu W, Li X, Du J, Xu A, Zheng M, et al. Myocardial infarction accelerates the progression of MASH by triggering immunoinflammatory response and induction of periosti. Cell Metab. 2024;36(6):1269–e12861269.
Mantovani A, Dauriz M, Sandri D, Bonapace S, Zoppini G, Tilg H, Byrne CD, Targher G. Association between non-alcoholic fatty liver disease and risk of atrial fibrillation in adult individuals: an updated meta-analysis. Liver Int. 2019;39(4):758–69.
van Kleef LA, Lu Z, Ikram MA, de Groot NMS, Kavousi M, de Knegt RJ. Liver stiffness not fatty liver disease is associated with atrial fibrillation: the Rotterdam study. J Hepatol. 2022;77(4):931–8.
Castera L, Forns X, Alberti A. Non-invasive evaluation of liver fibrosis using transient elastography. J Hepatol. 2008;48(5):835–47.
Myers RP, Elkashab M, Ma M, Crotty P, Pomier-Layrargues G. Transient elastography for the noninvasive assessment of liver fibrosis: a multicentre Canadian study. Can J Gastroenterol. 2010;24(11):661–70.
Liver, EAftSot. Hígado ALpeEd: EASL-ALEH clinical practice guidelines: non-invasive tests for evalution of liver disease severity and prognosis. J Hepatol. 2015;63:237–64.
Boeckmans J, Sandrin L, Knackstedt C, Schattenberg JM. Liver stiffness as a cornerstone in heart disease risk assessment. Liver Int. 2024;44(2):344–56.
Nightingale K. Acoustic radiation force impulse (ARFI) imaging: a review. Curr Med Imaging Rev. 2011;7(4):328–39.
Alem SA, Abdellatif Z, Mabrouk M, Zayed N, Elsharkawy A, Khairy M, Musa S, Anwar I, Yosry A. Diagnostic accuracy of acoustic radiation force impulse elastography (ARFI) in comparison to other non-invasive modalities in staging of liver fibrosis in chronic HCV patients: single-center experience. Abdom Radiol (NY). 2019;44(8):2751–8.
Vidili G, Arru M, Meloni P, Solinas G, Atzori S, Maida I. Comparison of 2D Shear Wave Elastography and transient elastography in non-invasive evaluation of liver fibrosis in Hepatitis C Virus-Related Chronic Liver Disease. J Clin Med 2024, 13(14).
Erre GL, Cadoni ML, Meloni P, Castagna F, Mangoni AA, Piga M, Passiu G, Carru C, Zinellu A, Vidili G. Methotrexate therapy is not associated with increased liver stiffness and significant liver fibrosis in rheumatoid arthritis patients: a cross-sectional controlled study with real-time two-dimensional shear wave elastography. Eur J Intern Med. 2019;69:57–63.
Erre GL, Castagna F, Sauchella A, Meloni P, Mangoni AA, Farina G, Woodman R, Dore MP, Vidili G. Prevalence and risk factors of moderate to severe hepatic steatosis in patients with rheumatoid arthritis: an ultrasonography cross-sectional case-control study. Ther Adv Musculoskelet Dis. 2021;13:1759720X211042739.
Dulai PS, Sirlin CB, Loomba R. MRI and MRE for non-invasive quantitative assessment of hepatic steatosis and fibrosis in NAFLD and NASH: clinical trials to clinical practice. J Hepatol. 2016;65(5):1006–16.
Thomas Elgeti MB, Hamm B. Ju¨rgen Braun, and Ingolf Sack: <2010 Cardiac magnetic resonance Elastography toward the diagnosis of abnormal myocardial Relaxation.pdf>. Invest Radiol. 2010;45(12):782–7.
Park CC, Nguyen P, Hernandez C, Bettencourt R, Ramirez K, Fortney L, Hooker J, Sy E, Savides MT, Alquiraish MH, et al. Magnetic resonance elastography vs transient elastography in detection of fibrosis and noninvasive measurement of steatosis in patients with biopsy-proven nonalcoholic fatty liver disease. Gastroenterology. 2017;152(3):598–e607592.
AlShaalan R, Aljiffry M, Al-Busafi S, Metrakos P, Hassanain M. Nonalcoholic fatty liver disease: noninvasive methods of diagnosing hepatic steatosis. Saudi J Gastroenterol. 2015;21(2):64–70.
van Ewijk PA, Schrauwen-Hinderling VB, Bekkers SC, Glatz JF, Wildberger JE, Kooi ME. MRS: a noninvasive window into cardiac metabolism. NMR Biomed. 2015;28(7):747–66.
Iqra Nadeem Kazi M, Lily Kuo M, Eugenia Tsai M. Noninvasive methods for assessing liver fibrosis and Steatosis. Gastroenterol Hepatol 2024, 20(1).
Ciardullo S, Cannistraci R, Muraca E, Zerbini F, Perseghin G. Liver fibrosis, NT-ProBNP and mortality in patients with MASLD: a population-based cohort study. Nutr Metab Cardiovasc Dis. 2024;34(4):963–71.
Vieira Barbosa J, Milligan S, Frick A, Broestl J, Younossi Z, Afdhal N, Lai M. Fibrosis-4 Index can independently predict major adverse Cardiovascular events in nonalcoholic fatty liver disease. Am J Gastroenterol. 2022;117(3):453–61.
Durak H, Çetin M, Emlek N, Ergül E, Özyıldız AG, Öztürk M, Duman H, Yılmaz AS, Şatıroğlu Ö. FIB-4 liver fibrosis index correlates with aortic valve sclerosis in non-alcoholic population. 2024, 41(1):e15732.
Shibata N, Ito T, Toyoda H, Tanaka A, Morita Y, Kanzaki Y, Watanabe N, Yoshioka N, Morishima I. Predictability of noninvasive liver fibrosis score for cardiac events in patients with nonalcoholic fatty liver disease. Eur Heart J 2023, 44(Supplement_2).
Lee J, Vali Y, Boursier J, Spijker R, Anstee QM, Bossuyt PM, Zafarmand MH. Prognostic accuracy of FIB-4, NAFLD fibrosis score and APRI for NAFLD-related events: a systematic review. Liver Int. 2021;41(2):261–70.
Ballestri S, Mantovani A, Baldelli E, Lugari S, Maurantonio M, Nascimbeni F, Marrazzo A, Romagnoli D, Targher G, Lonardo A. Liver Fibrosis Biomarkers Accurately Exclude Advanced Fibrosis and Are Associated with Higher Cardiovascular Risk Scores in Patients with NAFLD or Viral Chronic Liver Disease. Diagnostics (Basel) 2021, 11(1).
van der Bijl P, Kuneman JH, Bax JJ. Pericoronary adipose tissue attenuation: diagnostic and prognostic implications. Eur Heart J Cardiovasc Imaging. 2022;23(12):e537–8.
Yuvaraj J, Lin A, Nerlekar N, Munnur RK, Cameron JD, Dey D, Nicholls SJ, Wong DTL. Pericoronary Adipose tissue attenuation is Associated with High-Risk Plaque and subsequent Acute Coronary Syndrome in patients with stable coronary artery disease. Cells 2021, 10(5).
Takahata Y, Takahashi A, Anzai Y, Abe N, Sugaya T, Fujita M, Hayashi M, Abe K, Ohira H. Lifestyle factors affecting new-onset nonalcoholic fatty liver disease. Prev Med Rep. 2024;37:102577.
Promrat K, Kleiner DE, Niemeier HM, Jackvony E, Kearns M, Wands JR, Fava JL, Wing RR. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology. 2010;51(1):121–9.
Niederseer D, Wernly B, Aigner E, Stickel F, Datz C. NAFLD and cardiovascular diseases: epidemiological, mechanistic and therapeutic considerations. J Clin Med. 2021;10(3).
Akhavan Rezayat A, Dadgar Moghadam M, Ghasemi Nour M, Shirazinia M, Ghodsi H, Rouhbakhsh Zahmatkesh MR, Tavakolizadeh Noghabi M, Hoseini B, Akhavan Rezayat K. Association between smoking and non-alcoholic fatty liver disease: a systematic review and meta-analysis. SAGE Open Med. 2018;6:2050312117745223.
Laursen TL, Hagemann CA, Wei C, Kazankov K, Thomsen KL, Knop FK, Gronbaek H. Bariatric surgery in patients with non-alcoholic fatty liver disease - from pathophysiology to clinical effects. World J Hepatol. 2019;11(2):138–49.
Stefan N, Haring HU, Cusi K. Non-alcoholic fatty liver disease: causes, diagnosis, cardiometabolic consequences, and treatment strategies. Lancet Diabetes Endocrinol. 2019;7(4):313–24.
Quinn CE, Hamilton PK, Lockhart CJ, McVeigh GE. Thiazolidinediones: effects on insulin resistance and the cardiovascular system. Br J Pharmacol. 2008;153(4):636–45.
Guru B, Tamrakar AK, Manjula SN, Prashantha Kumar BR. Novel dual PPARalpha/gamma agonists protect against liver steatosis and improve insulin sensitivity while avoiding side effects. Eur J Pharmacol. 2022;935:175322.
Mao T, Zhang C, Yang S, Bi Y, Li M, Yu J. Semaglutide alters gut microbiota and improves NAFLD in db/db mice. Biochem Biophys Res Commun. 2024;710:149882.
Cheung KS, Ng HY, Hui RWH, Lam LK, Mak LY, Ho YC, Tan JT, Chan EW, Seto WK, Yuen MF et al. Effects of empagliflozin on liver fat in patients with metabolic dysfunction-associated steatotic liver disease without diabetes mellitus: a randomized, double-blind, placebo-controlled trial. Hepatology 2024.
Sumida Y, Naito Y, Tanaka S, Sakai K, Inada Y, Taketani H, Kanemasa K, Yasui K, Itoh Y, Okanoue T, et al. Long-term (> = 2 year) efficacy of vitamin E for non-alcoholic steatohepatitis. Hepatogastroenterology. 2013;60(126):1445–50.
Neuschwander-Tetri BA, Loomba R, Sanyal AJ, Lavine JE, Van Natta ML, Abdelmalek MF, Chalasani N, Dasarathy S, Diehl AM, Hameed B, et al. Farnesoid X nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): a multicentre, randomised, placebo-controlled trial. Lancet. 2015;385(9972):956–65.
Loomba R, Hartman ML, Lawitz EJ, Vuppalanchi R, Boursier J, Bugianesi E, Yoneda M, Behling C, Cummings OW, Tang Y, et al. Tirzepatide for metabolic dysfunction-associated steatohepatitis with liver fibrosis. N Engl J Med. 2024;391(4):299–310.
Petta S, Targher G, Romeo S, Pajvani UB, Zheng MH, Aghemo A, Valenti LVC. The first MASH drug therapy on the horizon: current perspectives of resmetirom. Liver Int 2024.
Loomba R, Sanyal AJ, Kowdley KV, Bhatt DL, Alkhouri N, Frias JP, Bedossa P, Harrison SA, Lazas D, Barish R, et al. Randomized, controlled trial of the FGF21 analogue pegozafermin in NASH. N Engl J Med. 2023;389(11):998–1008.
Sanyal AJ, Bedossa P, Fraessdorf M, Neff GW, Lawitz E, Bugianesi E, Anstee QM, Hussain SA, Newsome PN, Ratziu V, et al. A phase 2 randomized trial of survodutide in MASH and fibrosis. N Engl J Med. 2024;391(4):311–9.
Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey RF, Deaton C, Cuisset T, et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407–77.
Simon TG, Henson J, Osganian S, Masia R, Chan AT, Chung RT, Corey KE. Daily aspirin use associated with reduced risk for fibrosis progression in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. 2019;17(13):2776-e27842774.
Ballestri S, Capitelli M, Fontana MC, Arioli D, Romagnoli E, Graziosi C, Lonardo A, Marietta M, Dentali F, Cioni G. Direct oral anticoagulants in patients with liver disease in the era of non-alcoholic fatty liver disease global epidemic: a narrative review. Adv Ther. 2020;37(5):1910–32.
Pastori D, Polimeni L, Baratta F, Pani A, Del Ben M, Angelico F. The efficacy and safety of statins for the treatment of non-alcoholic fatty liver disease. Dig Liver Dis. 2015;47(1):4–11.
Pastori D, Pani A, Di Rocco A, Menichelli D, Gazzaniga G, Farcomeni A, D’Erasmo L, Angelico F, Del Ben M, Baratta F. Statin liver safety in non-alcoholic fatty liver disease: a systematic review and metanalysis. Br J Clin Pharmacol. 2022;88(2):441–51.
Ryoo JH, Suh YJ, Shin HC, Cho YK, Choi JM, Park SK. Clinical association between non-alcoholic fatty liver disease and the development of hypertension. J Gastroenterol Hepatol. 2014;29(11):1926–31.
Aneni EC, Oni ET, Martin SS, Blaha MJ, Agatston AS, Feldman T, Veledar E, Conceicao RD, Carvalho JA, Santos RD, et al. Blood pressure is associated with the presence and severity of nonalcoholic fatty liver disease across the spectrum of cardiometabolic risk. J Hypertens. 2015;33(6):1207–14.
Li Y, Xu H, Wu W, Ye J, Fang D, Shi D, Li L. Clinical application of angiotensin receptor blockers in patients with non-alcoholic fatty liver disease: a systematic review and meta-analysis. Oncotarget. 2018;9(35):24155–67.
Acknowledgements
We thank the above authors and their affiliated institutions for their contribution and support in the preparation of this chapter, and we thank BioRender for graphic support.
Funding
This work was supported by grants from Fondazione di Sardegna (FDS2017VIDILI).
Author information
Authors and Affiliations
Contributions
The study was designed by GV and HXZ was responsible for drafting the manuscript. GV, GC, EPN and LAS reviewed the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable for this review.
Consent for publication
All authors gave their consent to the publication of the article.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zheng, H., Sechi, L.A., Navarese, E.P. et al. Metabolic dysfunction-associated steatotic liver disease and cardiovascular risk: a comprehensive review. Cardiovasc Diabetol 23, 346 (2024). https://doi.org/10.1186/s12933-024-02434-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-024-02434-5