
Abstract
Background
It remains unclear whether the association between dyslipidemia status and triglyceride-glucose (TyG) index with myocardial damage varies in the context of type 2 diabetes mellitus (T2DM). This study aimed to determine the differential effects of dyslipidemia status and TyG index on left ventricular (LV) global function and myocardial microcirculation in patients with T2DM using cardiac magnetic resonance (CMR) imaging.
Methods
A total of 226 T2DM patients and 72 controls who underwent CMR examination were included. The T2DM group was further categorized into subgroups based on the presence or absence of dyslipidemia (referred to as T2DM (DysL+) and T2DM (DysL-)) or whether the TyG index exceeded 9.06. CMR-derived LV perfusion parameters, remodeling index, and global function index (GFI) were assessed and compared among groups. A multivariable linear regression model was employed to evaluate the effects of various variables on LV myocardial microcirculation, remodeling index, and GFI.
Results
The LV GFI sequentially decreased in controls, T2DM (DysL-), and T2DM (DysL+) groups (p < 0.001), and was lower (p = 0.003) in T2DM with higher TyG index group than in lower TyG index group. The LV remodeling index was higher in higher TyG index group than in lower TyG index group (p = 0.002), but there was no significant difference in whether the subgroup was accompanied by dyslipidemia. Multivariable analysis revealed that the TyG index, but not dyslipidemia status, was independently associated with LV remodeling index (β coefficient[95% confidence interval], 0.152[0.025, 0.268], p = 0.007) and LV GFI (− 0.159[− 0.281, − 0.032], p = 0.014). For LV myocardial microcirculation, perfusion index, upslope, and max signal intensity sequentially decreased in controls, T2DM (DysL-), and T2DM (DysL+) groups (all p < 0.001). Dyslipidemia status independently correlated with perfusion index (− 0.147[− 0.272, − 0.024], p = 0.02) and upslope (− 0.200[− 0.320, 0.083], p = 0.001), while TyG index was independently correlated with time to maximum signal intensity (0.141[0.019, 0.257], p = 0.023).
Conclusions
Both dyslipidemia status and higher TyG index were associated with further deterioration of LV global function and myocardial microvascular function in the context of T2DM. The effects of dyslipidemia and a higher TyG index appear to be differential, which indicates that not only the amount of blood lipids and glucose but also the quality of blood lipids are therapeutic targets for preventing further myocardial damage.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Diabetes mellitus, particularly type 2 diabetes mellitus (T2DM), is a growing global health concern and a well-established cardiovascular risk factor [1, 2]. In individuals with T2DM, dyslipidemia commonly coexists due to the interconnection of glucose and lipid metabolism, and is considered to be a significant risk factor and major contributor to the heightened cardiovascular risk [3,4,5]. Numerous studies have explored the pathogenic effect of diabetic dyslipidemia in macro- and microvascular damage [6,7,8], however, there is still insufficient evidence regarding its impact on myocardial microcirculation [9, 10], and the additive effects of dyslipidemia on T2DM have been rarely investigated.
Furthermore, the triglyceride-glucose index (TyG index), calculated as the product of fasting triglycerides and fasting glucose, serves as a novel and reliable surrogate marker of insulin resistance and been proposed as a potential predictor of adverse cardiovascular events [11, 12]. Thus far, it remains unclear whether the association between dyslipidemia status and TyG index with myocardial damage is differential and in what pattern varies in the context of T2DM. Research into the differential effects of dyslipidemia and the TyG index can improve our understanding of how changes in the quantity and quality of blood lipids impact myocardial injury in T2DM, potentially leading to more personalized treatment strategies.
Given the importance of myocardial microcirculation, cardiac remodeling, and function in cardiovascular risk, understanding the effects of injury is essential for guiding early therapeutic interventions aimed at preventing the development and progression of complications in diabetic dyslipidemia patients [13]. Cardiac magnetic resonance (CMR) imaging, characterized by high spatial and temporal resolution, absence of harmful ionizing radiation, and automatic quantitative/semi-quantitative assessment of global and regional cardiac function, has emerged as a credible tool for the non-invasive evaluation of cardiac geometry and myocardial microvascular function [14, 15]. Therefore, in this study, left ventricular (LV) structure, function, and myocardial perfusion microvascular function were analyzed to determine the differential effects of dyslipidemia status and TyG index on LV global function and myocardial microcirculation in patients with T2DM.
Methods
The Biomedical Research Ethics Committee of our hospital approved this study (No. 2019-878), with the requirement for written informed consent being waived due to the retrospective nature of this study.
Study population
For this retrospective study, we consecutively enrolled patients with T2DM who underwent CMR examinations at our hospital from January 2014 to June 2022. The inclusion criteria comprised clinically confirmed subjects with T2DM according to the current guidelines [2, 16], who completed the CMR examination. Exclusion criteria, detailed in Fig. 1, encompassed primary cardiomyopathy, congenital heart disease, coronary heart disease, valvular heart disease, severe arrhythmia, cancer therapy, severe renal failure (estimated creatinine clearance < 30 mL/min/1.73 m2), heart failure (symptoms or LV ejection fraction [LVEF] < 50%), and invalid or missing CMR images. Ultimately, 226 patients meeting these criteria were included in this study and categorized into two groups based on the presence or absence of dyslipidemia: T2DM with dyslipidemia [T2DM(DysL+)] and T2DM without dyslipidemia [T2DM(DysL-)]. Dyslipidemia was defined as the use of lipid-lowering treatment or a range of lipid abnormalities, involving increased total cholesterol (TC) ≥ 6.20 mmol/L, low-density lipoprotein cholesterol (LDL-C) > 4.13 mmol/L, triglyceride (TG) levels > 2.25 mmol/L, or decreased high-density lipoprotein cholesterol (HDL-C) < 1.03 mmol/L [17, 18]. Additionally, to assess the influence of the TyG index on LV myocardial microvascular perfusion, based on the distribution of TyG index (Additional file: Fig. S1), T2DM patients were divided into two groups according to the median TyG index (Calculated as Ln[fasting triglycerides (mg/dl) × fasting glucose (mg/dl)/2]) [19, 20]: TyG index < 9.06 (n = 112) and TyG index ≥ 9.06 groups (n = 114). Meanwhile, 72 age- and sex-matched controls (age: 55.8 ± 8.8 years; 33 females, 45.8%) were screened and enrolled from the hospital database. Controls were excluded if they had been diagnosed with chronic diseases (diabetes, hypertension, dyslipidemia, etc.), arrhythmia, cardiovascular disease-related symptoms (chest pain, palpitation, etc.), cardiovascular diseases, CMR-detected abnormalities, or had a medication history (Fig. 1).

Study flowchart shows patient selection process
CMR protocol
CMR imaging for all subjects was conducted using the whole-body 3.0T Siemens MAGNETOM (Trio Tim or Skyra scanner, Siemens Healthcare, Inc.) with subjects in the supine position. Standard electrocardiogram (ECG)-triggering equipment and the breath-hold technique were employed to monitor and record each subject’s dynamic ECG changes and breathing. Images were acquired during end-inhalation breath-holding under ECG gating. Standard short-axis (covering the entire ventricles), long-axis two- and four-chamber cine images were obtained using a retrospectively segmented ECG-gated balanced steady-state free precession sequence (repetition time [TR], 3.4 ms or 2.8 ms; echo time [TE], 1.3 ms or 1.2 ms; flip angle, 50° or 35°; slice thickness, 8 mm; inter-slice spacing, 0 mm; field of view, 340 × 285 mm2; matrix size, 256 × 166), and reconstructed at 25 frames per breath-hold acquisition.
CMR first-pass contrast-enhanced perfusion images were acquired by injecting gadobenate dimeglumine (MultiHance; 0.5 mmol/mL; Bracco, Milan, Italy) at a dose of 0.2 mL/kg body weight at a flow rate of 2.5–3.0 mL/s, followed by 20 mL of 0.9% saline at 3.0 mL/s. First-pass perfusion was acquired concurrently with intravenous contrast agents in three standard short-axis slices (basal, mid-ventricular, and apical slices) and one four-chamber slice. This was performed by an inversion recovery prepared echoplanar sequence (TR, 149 ms or 163 ms; TE, 1.1 ms or 1.0 ms; flip angle, 10°; matrix, 154 × 192 pixels, and field of view, 258 × 322 mm2).
CMR analyses
All CMR images were analyzed using a commercial software (cvi42; Circle Cardiovascular Imaging Inc.) by two radiologists with a minimum of 5 years of CMR experience. For image post-processing, offline cine or perfusion images were loaded into corresponding functional modules. LV endocardial borders, epicardial borders, and blood pool (only in the post-processing of perfusion) were automatically delineated by the software and adjusted manually. When delineating the endocardial borders, papillary muscles and trabecular tissue were excluded from myocardial mass assessment but included in volume analyses [21].
LV geometric and functional parameters, including myocardial mass, end-diastolic volume (EDV), end-systolic volume (ESV), and stroke volume (SV), were measured based on cine images following current guidelines [21], and were indexed to body surface area. The LV remodeling index (calculated as LV mass/EDV), LVEF, and LV global function index (LV GFI, calculated as {LV SV/ [(LV EDV + LV ESV)/2 + (LV mass/1.05)]} × 100) were generated based on different formulas [21, 22].
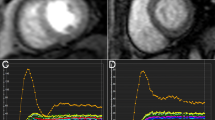
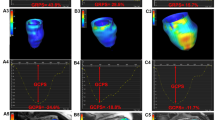
LV myocardial perfusion parameters, including upslope, time to maximum signal intensity (TTM), max signal intensity (MaxSI), and perfusion index (calculated as Upslope [myocardium]/Upslope [LV blood pool]), were derived from myocardial time–signal intensity and obtained in 16 myocardial segments (Bull’s eye plot) of the LV and the blood pool, respectively. LV global myocardial perfusion parameters were calculated by averaging values of the 16 myocardial segments (Fig. 2).

Representative cases show the TyG index, LV myocardial microvascular parameters and function in diabetic individuals with or without dyslipidemia. A0 and A1 shows the mid-ventricular slice of left ventricular end-diastolic in cine images; B0 and B1 shows the first-pass perfusion signal intensity-time curves in mid-ventricular slice of left ventricular; C0 and C1 shows the map of perfusion index based on Bull’s eye plot. The abbreviations are listed in Tables 1 and 2
Analyses of CMR parameters reproducibility
To assess intra-observer variability, a primary radiologist measured and analyzed perfusion images for myocardial perfusion parameters in 100 randomly selected subjects (70 patients with T2DM and 30 control subjects) at two distinct time points, separated by a 30-day interval. Inter-observer variability was evaluated by having a second radiologist independently measure and analyze images from the same sample without knowledge of the patient’s clinical data or the first radiologist’s findings.
Statistical analysis
Statistical analyses were conducted using SPSS (version 24.0; IBM SPSS, Inc., Chicago, IL, USA) and GraphPad Prism (version 8.0, GraphPad Software Inc., San Diego, CA, USA). The normal distribution of continuous variables was assessed using the Shapiro–Wilk test. Continuous variables conforming to a normal distribution are shown as mean ± standard deviation, while non-normally distributed data are shown as median (25–75% interquartile range). Categorical variables are shown as numbers (percentages) and were analyzed using chi-squared tests or Fisher’s exact test, as appropriate. Clinical variables and CMR parameters among controls, T2DM(DysL+), and T2DM(DysL-) were compared using one-way analysis of variance followed by Bonferroni’s post-hoc test or Kruskal–Wallis rank test. LV remodeling index, GFI and perfusion parameters between TyG index < 9.06 and TyG index ≥ 9.06 were compared using student’s t-test. Spearman’s/Pearson’s correlation coefficient and univariable analysis were performed to examine the association of LV perfusion parameters with clinical variables and LV geometric and functional parameters. Variables without collinearity and with P < 0.1 in univariable analysis were included in multivariable backward linear regression models to evaluate the effects of variables on LV remodeling, LV GFI, and myocardial microcirculation in patients with T2DM. Intraclass correlation coefficient (ICC) was used to measure the variability. A two-tailed P < 0.05 was considered significant.
Results
General characteristics of the study cohort
In total, 226 T2DM patients and 72 controls were included in this study. Among the T2DM patients, 109 (48.2%) had coexisting dyslipidemia. The general characteristics of the study cohort are summarized in Table 1 and Table S1 (Additional file). No significant differences were observed between the control, T2DM(DysL-), and T2DM(DysL+) groups regarding age, gender, smoking history, and resting heart rate (all P > 0.05). Compared with controls, T2DM patients presented higher systolic blood pressure, higher glycated hemoglobin (HbA1c), higher TyG index, and lower estimated glomerular filtration rate (all P < 0.05). For T2DM subgroup, the T2DM(DysL+) group showed higher TG, higher TC, and lower LDL-C compared to the T2DM(DysL-) group (all P < 0.05), while no significant difference was observed in HbA1c, TyG index, and HDL-C.
Comparison of CMR results among T2DM with or without dyslipidemia
The CMR results among controls, T2DM(DysL+), and T2DM(DysL-) are summarized in Table 2. For LV geometric and functional parameters, the LV GFI sequentially decreased in controls, T2DM(DysL-), and T2DM(DysL+) groups (controls vs. T2DM(DysL-) vs. T2DM(DysL+); 50.05 ± 6.20 vs. 47.06 ± 8.69 vs. 44.01 ± 8.31, p < 0.001). T2DM patients presented higher LV remodeling index when compared with controls, but there was no significant difference between the T2DM(DysL-) and T2DM(DysL+) groups (0.61 ± 0.16 g/mL vs. 0.70 ± 0.22 g/mL vs. 0.76 ± 0.21 g/mL, p < 0.001). For LV myocardial perfusion parameters, the perfusion index, upslope, and MaxSI sequentially decreased in controls, T2DM(DysL-), and T2DM(DysL+) groups (Perfusion index, 13.38% ± 3.33% vs. 11.91% ± 2.50% vs. 10.86% ± 2.75%, p < 0.001; Upslope, 2.68 ± 0.74 SI/sec vs. 2.29 ± 0.98 SI/sec vs. 1.73 ± 0.89 SI/sec, p < 0.001; MaxSI, 23.94 ± 4.91SI vs. 21.36 ± 7.82 SI vs. 18.50 ± 7.40 SI, p < 0.001).
Comparison of CMR results among T2D with different TyG index
The CMR results between the TyG index < 9.06 group and TyG index ≥ 9.06 group in patients with T2DM are summarized in Fig. 3. When compared with the lower TyG index group, the higher TyG index group presented a higher LV remodeling index (0.77 ± 0.22 g/mL vs. 0.68 ± 0.20 g/mL, p = 0.002), lower LV GFI (43.83 ± 8.67 vs. 47.22 ± 8.34, p = 0.003), lower Upslope (1.79 ± 0.70 SI/sec vs. 2.23 ± 1.14 SI/sec, p = 0.001), and longer TTM (34.40 ± 13.30 s vs. 31.17 ± 13.81 s, p = 0.017), but the perfusion index and MaxSI were not significantly different between the two groups (both p > 0.05).

Comparison of cardiac magnetic resonance results among Type 2 diabetes mellitus with different TyG index. LV, left ventricular; GFI, global function index; MaxSI, maximal signal intensity; TTM, time to maximum signal intensity
Association of LV myocardial microvascular perfusion function with clinical variables, LV remodeling index, and LV GFI
As shown in Table 3, gender, fasting blood glucose, HbA1c, TyG index, and LV GFI were significantly correlated with LV myocardial perfusion function (perfusion index, Upslope, MaxSI, and TTM) (all p < 0.05). However, among the lipid-related indicators, only TG and HDL were slightly correlated with Upslope (TG, r = − 0.137, p = 0.039; HDL, r = 0.154, p = 0.026), and TG was slightly correlated with TTM (r = 0.149, p = 0.025).
The effect of clinical variables on LV remodeling and LV GFI
To determine the effect of clinical variables on LV remodeling and LV GFI, age, gender, BMI, heart rate, HbA1c, TyG, hypertension, and dyslipidemia were included in univariable and multivariable linear regression analysis. Detailed results are shown in Table 4. The multivariable analysis indicated that female and TyG index were independently associated with LV remodeling index (β coefficient [95% confidence interval]; Female, − 0.237[− 0.354, − 0.107], p < 0.001; TyG index, 0.152[0.025, 0.268], p = 0.007) and LV GFI (Female, 0.323[0.196, 0.447], p < 0.001; TyG index, − 0.159(− 0.281, − 0.032), p = 0.014). Hypertension remained an independent determinant of LV remodeling index (0.197[0.071, 0.312], p = 0.002) rather than LV GFI.
The effect of clinical variables and LV remodeling on LV myocardial microvascular perfusion function
As shown in Table 5, multivariable linear regression analysis revealed independent correlations: gender (female) with all LV myocardial perfusion parameters (Perfusion index, β = 0.337, p < 0.001; Upslope, β = 0.314, p < 0.001; MaxSI, β = 0.196, p = 0.004; TTM, β = −0.337, p < 0.001), HbA1c with all LV myocardial perfusion parameters except TTM (Perfusion index, β = −0.127, p = 0.028; Upslope, β = −0.189, p = 0.012; Max [SI], β = −0.159, p = 0.013). Dyslipidemia status independently correlated with perfusion index (-0.147[-0.272, -0.024], p = 0.02) and upslope (-0.200[-0.320, 0.083], p = 0.001). And TyG index was independently correlated with TTM (0.141[0.019, 0.257], p = 0.023), but not with perfusion index, Upslope, and MaxSI.
Intra- and inter‐observer variability
The intra- and inter‐observer agreements of LV remodeling index, GFI, and myocardial perfusion parameters are summarized in Additional file 1: Table S2 and were considered excellent (ICC = 0.948–0.989 for intra‐observer variability and 0.921–0.957 for inter‐observer variability).
Discussion
This study used CMR-based measurements of LV myocardial perfusion, geometric structure and function to investigate the differential effects of dyslipidemia and TyG index on LV global function and myocardial microvascular function in diabetic individuals, yielding the following findings: 1) In patients with T2DM, higher TyG index had an additive deleterious effect on higher LV remodeling index, lower LV GFI, and impaired microvascular perfusion function; and the coexistence of dyslipidemia further deteriorated LV GFI and microvascular perfusion function, but not LV remodeling index; 2) In the context of diabetes, the damage effects of dyslipidemia and TyG index on myocardial damage were differential, that is, dyslipidemia status was an independent determinant of reduced perfusion index and upslope, while higher TyG index was an independent determinant of LV remodeling, decreased LV GFI, and heightened TTM.
Diabetic dyslipidemia on cardiac injury
Accumulating data confirm that diabetic dyslipidemia involves quantitative, qualitative, and kinetic changes in major circulating lipids, leading to a shift in the lipid profile toward a more atherogenic and inflammatory response [7, 8]. This, in turn, is considered a significant factor in vascular damage, intensifying the detrimental effects on the heart and contributing to increased cardiovascular risk in T2DM patients [7, 8]. Although the full pathophysiological mechanism of diabetic dyslipidemia remains unclear, previous studies have suggested that insulin resistance and relative insulin deficiency observed in patients with T2DM may contribute to these lipid changes [7, 23]. In real-world practice, the use of lipid-lowering medications makes the blood lipid of most patients with dyslipidemia be controlled. Nevertheless, previous studies have reported that residual risk persists even after intensive lipid reduction [24], and it remains unclear whether the association between dyslipidemia status and TyG index (an insulin resistance marker) and LV injury is differential in the context of T2DM. Herein, the effects of dyslipidemia status and the TyG index in the context of T2DM were simultaneously analyzed, providing a more comprehensive understanding of the impact of diabetic dyslipidemia on cardiac injury.
Effect of dyslipidemia status on myocardial microcirculation in T2DM patients
Previous studies have separately demonstrated the detrimental effects of diabetes or dyslipidemia on microvascular function [10, 25, 26]. However, when diseases coexist, previous studies have found that TG is significantly associated with myocardial damage in the context of T2DM or obesity [27, 28]. When diabetes and dyslipidemia coexist, Song and Bourgonje et al. found a significant association between dyslipidemia and the progression of diabetic retinopathy and diabetic nephropathy, highlighting the additive impact of dyslipidemia on microvascular damage in diabetic patients [29, 30]. In alignment with these effects on eye and kidney damage [29, 30], our study observed that diabetic patients with dyslipidemia exhibited more severe coronary microvascular dysfunction compared to those without dyslipidemia. Dyslipidemia status independently predicted reduced myocardial perfusion index and upslope in T2DM patients.
Despite this, biomarkers of dyslipidemia (TG, TC, HDL, and LDL) showed weakly associated with microvascular function in our study. It is speculated that lipid-lowering drugs may have reversed elevated biomarkers and weakened or interfered with the correlation between biomarkers and microvascular function. However, in the diabetes context, patients with dyslipidemia often experience qualitative and kinetic changes in lipid particles (lipoprotein size, glycation of apoproteins, increased susceptibility to oxidation, etc.), exacerbating microvascular damage through significantly amplified oxidative stress and inflammation [31]. Additionally, the protective effect of HDL on the development of microvascular complications is thought to be diminished in established T2DM [30, 32]. These findings underscore the importance of addressing not only quantitative changes in circulating lipids but also qualitative and kinetic changes.
Effect of TyG index on myocardial microcirculation in T2DM patients
Certainly, insulin resistance is a well-recognized contributor to impaired cardiac function and the initiation and progression of cardiovascular events [33,34,35]. Recently, several studies have highlighted the TyG index as a convenient and reliable surrogate marker for insulin resistance, considering the complexity and cost associated with the homeostasis model index [20, 36]. Zhang et al. demonstrated a significant association between the TyG index and the risk of coronary microvascular dysfunction in patients with chronic coronary syndrome, establishing it as an independent predictor of major adverse cardiac events [10]. Similarly, Kassab et al. identified a significant association between a higher TyG index and diabetic retinopathy, diabetic nephropathy, and diabetic peripheral neuropathy [37]. In line with these findings [11, 37], our study revealed a significant correlation between the TyG index and myocardial microvascular dysfunction. The TyG index independently predicted an increase in TTM, rather than impacting perfusion index, upslope, and MaxSI, suggesting that the TyG index primarily induces coronary microvascular dysfunction by reducing coronary slow flow. In addition, compared to previous study [38], the median of TyG index in our study was higher. We speculated that the reason for this difference was that our study was conducted in the diabetic cohort, which had a higher proportion of dyslipidemia, and therefore presented a higher TyG index.
LV remodeling and global function in diabetic dyslipidemia patients
Herein, for patients with T2DM, LV volume and EF were not significantly reduced, while LV mass and remodeling index were increased, which is consistent with previous studies and believe to be related to myocardial hypertrophy caused by modified intracellular signaling and metabolic disturbances in diabetic patients [39, 40]. However, the coexistence of dyslipidemia did not exacerbate LV remodeling. While patients with dyslipidemia exhibited a higher LV mass, further investigation is needed to confirm whether dyslipidemia fails to additionally increase LV remodeling in the context of diabetes. Conversely, a higher TyG index was associated with worsened LV remodeling, aligning with previous studies suggesting that insulin resistance can contribute to LV remodeling [41, 42].
Regarding LV GFI, it integrates LV volumetric and functional parameters, reflecting cardiac remodeling and correlating with prognosis in multiple study cohorts [22, 43, 44]. In our cohorts, even when LV EF falls within the normal range and does not differ statistically from the controls, LV GFI in diabetes patients is significantly reduced. The coexistence of dyslipidemia further amplifies their detrimental effect on LV GFI, and a higher TyG index is also associated with decreased LV GFI. These findings emphasize the additive effect of dyslipidemia and insulin resistance on LV injury in the context of T2DM. Moreover, they suggest that LV GFI is more effective in the early detection of LV dysfunction compared to LV remodeling index and LV EF.
Limitation
This study has several limitations. First, being a single-center retrospective observational study, it is inherently limited. Additional multicenter and prospective analyses are essential to validate the results and establish cause-effect relationships. Second, the small sample size and the exclusion of patients with Type 1 diabetes mellitus, as these factors could impact the generalizability of our findings. Third, our present study did not evaluate other advanced CMR techniques, such as T1 mapping and T2 mapping, which are important tools for further characterization of myocardial tissue and are valuable for assessing the differential effect between dyslipidemia status and TyG index. Relevant studies will be investigated in future studies. Finally, considering compensations caused by heart failure may eliminate early damage and relationships, and therefore exclude patients with heart failure. However, this exclusion allows us to focus on early research and corresponding treatments.
Conclusions
Both dyslipidemia status and higher TyG index were associated with further deterioration of LV global function and myocardial microvascular function in T2DM. Nevertheless, their detrimental effects on myocardial damage were differential: a higher TyG index independently determined LV remodeling, decreased LV GFI, and heightened TTM, and dyslipidemia status independently determined reduced perfusion index and upslope. Our findings indicate that not only the amount of blood lipids and glucose but also the quality of blood lipids are therapeutic targets for preventing further myocardial microvascular dysfunction and LV global functional damage in the context of T2DM.
Data availability
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CMR:
-
Cardiac magnetic resonance
- EDVi:
-
End-diastolic volume index
- EF:
-
Ejection fraction
- ESVi:
-
End-systolic volume index
- GFI:
-
Global function index
- HDL-C:
-
High density lipoprotein cholesterol
- LDL-C:
-
Low density lipoprotein cholesterol
- MaxSI:
-
Maximal signal intensity
- LV:
-
Left ventricular
- TTM:
-
Time to maximum signal intensity
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- TyG index:
-
Triglyceride-glucose index
- T2DM:
-
Type 2 diabetes mellitus
References
American Diabetes Association Professional Practice Committee. 10. Cardiovascular disease and risk management: standards of care in diabetes-2024. Diabetes Care. 2024;47(Suppl 1):S179–218.
Marx N, Federici M, Schütt K, Müller-Wieland D, Ajjan RA, Antunes MJ, et al. 2023 ESC guidelines for the management of cardiovascular disease in patients with diabetes. Eur Heart J. 2023;44(39):4043–140.
Ide S, Maezawa Y, Yokote K. Updates on dyslipidemia in patients with diabetes. J Diabetes Investig. 2023;14(9):1041–4.
Dake AW, Sora ND. Diabetic dyslipidemia review: an update on current concepts and management guidelines of diabetic dyslipidemia. Am J Med Sci. 2016;351(4):361–5.
Adiels M, Olofsson SO, Taskinen MR, Borén J. Diabetic dyslipidaemia. Curr Opin Lipidol. 2006;17(3):238–46.
Savelieff MG, Callaghan BC, Feldman EL. The emerging role of dyslipidemia in diabetic microvascular complications. Curr Opin Endocrinol Diabetes Obes. 2020;27(2):115–23.
Vergès B. Pathophysiology of diabetic dyslipidaemia: where are we? Diabetologia. 2015;58(5):886–99.
Filippatos T, Tsimihodimos V, Pappa E, Elisaf M. Pathophysiology of diabetic dyslipidaemia. Curr Vasc Pharmacol. 2017;15(6):566–75.
Souza ACDAH, Rosenthal MH, Moura FA, Divakaran S, Osborne MT, Hainer J et al. Body composition, coronary microvascular dysfunction, and future risk of cardiovascular events including heart failure. JACC Cardiovasc Imaging 202:S1936-878X(23)00383-2.
Camici PG, d’Amati G, Rimoldi O. Coronary microvascular dysfunction: mechanisms and functional assessment. Nat Rev Cardiol. 2015;12(1):48–62.
Zhang W, Liu L, Chen H, Li S, Wan M, Mohammed AQ, et al. Association between the triglyceride-glucose index and the presence and prognosis of coronary microvascular dysfunction in patients with chronic coronary syndrome. Cardiovasc Diabetol. 2023;22(1):113.
Wang W, Yang J, Wang K, et al. Association between the triglyceride-glucose index and in-hospital major adverse cardiovascular events in patients with acute coronary syndrome: results from the improving care for Cardiovascular Disease in China (CCC)-Acute Coronary Syndrome project. Cardiovasc Diabetol. 2024;23(1):170.
Marcovecchio ML. Importance of identifying novel biomarkers of microvascular damage in type 1 diabetes. Mol Diagn Ther. 2020;24(5):507–15.
Ordovas KG, Baldassarre LA, Bucciarelli-Ducci C, Carr J, Fernandes JL, Ferreira VM, et al. Cardiovascular magnetic resonance in women with cardiovascular disease: position statement from the Society for Cardiovascular Magnetic Resonance (SCMR). J Cardiovasc Magn Reson. 2021;23(1):52.
Nagel E, Greenwood JP, McCann GP, Bettencourt N, Shah AM, Hussain ST, et al. Magnetic resonance perfusion or fractional flow reserve in coronary disease. N Engl J Med. 2019;380(25):2418–28.
American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S13–28.
Kopin L, Lowenstein C, Dyslipidemia. Ann Intern Med. 2017;167(11):ITC81–96.
Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–88.
Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, Martínez-Abundis E, Ramos-Zavala MG, Hernández-González SO, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95(7):3347–51.
Lopez-Jaramillo P, Gomez-Arbelaez D, Martinez-Bello D, et al. Association of the triglyceride glucose index as a measure of insulin resistance with mortality and cardiovascular disease in populations from five continents (PURE study): a prospective cohort study. Lancet Healthy Longev. 2023;4(1):e23–33.
Schulz-Menger J, Bluemke DA, Bremerich J, Flamm SD, Fogel MA, Friedrich MG, et al. Standardized image interpretation and post-processing in cardiovascular magnetic resonance– 2020 update: society for cardiovascular magnetic resonance (SCMR): Board of Trustees Task Force on standardized post-processing. J Cardiovasc Magn Reson. 2020;22(1):19.
Zhang TY, An DA, Fang Y, Zhou H, Yan H, Chen B, et al. Assessment of the prognostic value of MRI left ventricular global function index (LVGFI) in patients with end-stage renal disease under maintenance dialysis. J Magn Reson Imaging. 2023;5. https://doi.org/10.1002/jmri.28979.
Takei Y, Tomiyama H, Tanaka N, Yamashina A, Chikamori T. Association between Insulin Resistance, oxidative stress, sympathetic activity and coronary microvascular function in patients with early stage impaired glucose metabolism. Circ J. 2022;86(5):866–73.
Sirimarco G, Labreuche J, Bruckert E, et al. Atherogenic dyslipidemia and residual cardiovascular risk in statin-treated patients. Stroke. 2014;45(5):1429–36.
El-Seweidy MM, Sarhan Amin R, Husseini Atteia H, El-Zeiky RR, Al-Gabri NA. Dyslipidemia induced inflammatory status, platelet activation and endothelial dysfunction in rabbits: protective role of 10-Dehydrogingerdione. Biomed Pharmacother. 2019;110:456–64.
Yu Y, Yang W, Dai X, Yu L, Lan Z, Ding X, et al. Microvascular myocardial ischemia in patients with diabetes without obstructive coronary stenosis and its Association with Angina. Korean J Radiol. 2023;24(11):1081–92.
Hussein AA, Abdel-Aziz A, Gabr M, Hemmaid KZ. Myocardial and metabolic dysfunction in type 2 diabetic rats: impact of ghrelin. Can J Physiol Pharmacol. 2012;90(1):99–111.
Widya RL, de Mutsert R, den Heijer M, le Cessie S, Rosendaal FR, Jukema JW, et al. Association between hepatic triglyceride content and left ventricular diastolic function in a population-based cohort: the Netherlands epidemiology of obesity study. Radiology. 2016;279(2):443–50.
Song KH, Jeong JS, Kim MK, Kwon HS, Baek KH, Ko SH, et al. Discordance in risk factors for the progression of diabetic retinopathy and diabetic nephropathy in patients with type 2 diabetes mellitus. J Diabetes Investig. 2019;10(3):745–52.
Bourgonje AR, Connelly MA, van Goor H, van Dijk PR, Dullaart RPF. Both LDL and HDL particle concentrations associate positively with an increased risk of developing microvascular complications in patients with type 2 diabetes: lost protection by HDL (Zodiac-63). Cardiovasc Diabetol. 2023;22(1):169.
Toma L, Stancu CS, Sima AV. Endothelial dysfunction in diabetes is aggravated by glycated lipoproteins; novel molecular therapies. Biomedicines. 2020;9(1):18.
Higashi Y. Endothelial function in Dyslipidemia: roles of LDL-Cholesterol, HDL-cholesterol and triglycerides. Cells. 2023;12(9):1293.
Zhao S, Yu S, Chi C, Fan X, Tang J, Ji H, et al. Association between macro- and microvascular damage and the triglyceride glucose index in community-dwelling elderly individuals: the Northern Shanghai Study. Cardiovasc Diabetol. 2019;18(1):95.
Bonora E, Formentini G, Calcaterra F, Lombardi S, Marini F, Zenari L, et al. HOMA-estimated insulin resistance is an independent predictor of cardiovascular disease in type 2 diabetic subjects: prospective data from the Verona Diabetes complications Study. Diabetes Care. 2002;25(7):1135–41.
Wang T, Li M, Zeng T, Hu R, Xu Y, Xu M, et al. Association between insulin resistance and cardiovascular disease risk varies according to glucose tolerance status: a nationwide prospective cohort study. Diabetes Care. 2022;45(8):1863–72.
Zhou Y, Wang C, Che H, Cheng L, Zhu D, Rao C, et al. Association between the triglyceride-glucose index and the risk of mortality among patients with chronic heart failure: results from a retrospective cohort study in China. Cardiovasc Diabetol. 2023;22(1):171.
Kassab HS, Osman NA, Elrahmany SM. Assessment of triglyceride-glucose index and ratio in patients with type 2 diabetes and their relation to microvascular complications. Endocr Res. 2023;48(4):94–100.
Lu YW, Chang CC, Chou RH, Tsai YL, Liu LK, Chen LK, et al. Gender difference in the association between TyG index and subclinical atherosclerosis: results from the I-lan longitudinal aging study. Cardiovasc Diabetol. 2021;20(1):206.
Jiang L, Wang J, Liu X, et al. The combined effects of cardiac geometry, microcirculation, and tissue characteristics on cardiac systolic and diastolic function in subclinical diabetes mellitus-related cardiomyopathy. Int J Cardiol. 2020;320:112–8.
Bugger H, Abel ED. Molecular mechanisms of diabetic cardiomyopathy. Diabetologia. 2014;57(4):660–71.
Samuelsson AM, Bollano E, Mobini R, Larsson BM, Omerovic E, Fu M, et al. Hyperinsulinemia: effect on cardiac mass/function, angiotensin II receptor expression, and insulin signaling pathways. Am J Physiol Heart Circ Physiol. 2006;291(2):H787–96.
Li X, Chan JSK, Guan B, Peng S, Wu X, Lu X, et al. Triglyceride-glucose index and the risk of heart failure: evidence from two large cohorts and a mendelian randomization analysis. Cardiovasc Diabetol. 2022;21(1):229.
Larina VN, Lunev VI. Prognostic role of the left ventricular global function index companion in patients with chronic heart failure. Eur J Intern Med. 2023;117:134–6.
Ta HT, Critser PJ, Schäfer M, Ollberding NJ, Taylor MD, Di Maria MV, et al. Ventricular global function index is associated with clinical outcomes in pediatric pulmonary hypertension. J Cardiovasc Magn Reson. 2023;25(1):39.
Acknowledgements
Not applicable.
Funding
This work was financially supported by the National Natural Science Foundation of China (No. 82202115, 82120108015, 82371925 and 81771887); Science and Technology Support Program of Sichuan Province (2023NSFSC1725 and 2023ZYD0100); 1·3·5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYGD23019).
Author information
Authors and Affiliations
Contributions
L.J. and Z.G.Y. designed the study. L.J. wrote the manuscript. K.S., H.F., Y.W.F., Y.K.G. and H.Y.X. analyzed the data and gave advice on data presentation. L.J., K.S., H.F. and Y.W.F. collected the data. L.J., H.Y.X, Y.L. and Z.G.Y. revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Biomedical Research Ethics Committee of our hospital approved this study (No. 2019 − 878), with the requirement for written informed consent being waived due to the retrospective nature of this study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jiang, L., Xu, H., Li, Y. et al. The differential effects of dyslipidemia status and triglyceride-glucose index on left ventricular global function and myocardial microcirculation in diabetic individuals: a cardiac magnetic resonance study. Cardiovasc Diabetol 23, 345 (2024). https://doi.org/10.1186/s12933-024-02435-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-024-02435-4