
Abstract
Background
Polyparasitism is a common condition in humans but its impact on the host immune system and clinical diseases is still poorly understood. There are few studies of the prevalence and the effect of malaria-intestinal parasite co-infections in the immune response to malaria vaccine candidates. The present study determines whether the presence of malaria and intestinal parasites co-infection is associated with impaired IgG responses to Plasmodium vivax AMA-1 and MSP-119 in a rural population of the Brazilian Amazon.
Methods
A cross-sectional survey was performed in a rural area of Rondonia State and 279 individuals were included in the present study. At recruitment, whole blood was collected and Plasmodium and intestinal parasites were detected by microscopy and molecular tests. Blood cell count and haemoglobin were also tested and antibody response specific to P. vivax AMA-1 and MSP-119 was measured in plasma by ELISA. The participants were grouped according to their infection status: singly infected with Plasmodium (M); co-infected with Plasmodium and intestinal parasites (CI); singly infected with intestinal parasites (IP) and negative (N) for both malaria and intestinal parasites.
Results
The prevalence of intestinal parasites was significantly higher in individuals with malaria and protozoan infections were more prevalent. IgG antibodies to PvAMA-1 and/or PvMSP-119 were detected in 74 % of the population. The prevalence of specific IgG was similar for both proteins in all four groups and among the groups the lowest prevalence was in IP group. The cytophilic sub-classes IgG1 and IgG3 were predominant in all groups for PvAMA-1 and IgG1, IgG3 and IgG4 for PvMSP-119. In the case of non-cytophilic antibodies to PvAMA-1, IgG2 was significantly higher in IP and N group when compared to M and CI while IgG4 was higher in IP group.
Conclusions
The presence of intestinal parasites, mainly protozoans, in malaria co-infected individuals does not seem to alter the antibody immune responses to P. vivax AMA-1 and MSP-119. However, IgG response to both AMA1 and MSP1 were lower in individuals with intestinal parasites.
Similar content being viewed by others


Background
It is well known that polyparasitism is a common condition in humans, however, little is known about the interaction between parasites and its impact on the host immune system and clinical diseases [1]. Malaria and intestinal parasitic infections are distributed throughout the world and are highly prevalent in humid and warm environments in the tropics. The World Health Organization estimates that 3.3 billion people, almost half the world’s population, are at risk of contracting malaria and approximately 3.5 billion people are affected by intestinal protozoa and/or helminths [2]. Thus, protozoa of the genus Plasmodium, etiological agents of malaria, and many species of intestinal parasites (protozoa and helminths) share the same geographic distribution area and both types of parasites can infect the same population of hosts.
The implication of concomitant infection in humans has been evaluated mainly regarding the effects of intestinal helminth infections on falciparum malaria, obtaining conflicting results. While Ascaris lumbricoides infection may protect against cerebral malaria [3, 4] and Schistosoma haematobium has a protective effect on the density of the Plasmodium falciparum infection, [5, 6] children carrying intestinal helminth infections including Ascaris lumbricoides were more susceptive to either P. falciparum infection or acute malaria attacks [7–9]. In other studies, co-infections can make no difference [10–13]. In rodent models of co-infection, schistosome and plasmodia infections are affected at the immunological level [14–17]. In humans, studies demonstrating an effect of helminths on vaccine-induced immune responses against influenza, cholera and tetanus have been described [18, 19]. So far, little information is available about whether and how co-infections of helminths and malaria parasites can affect specific immune response to malaria parasites and vaccine candidates [20–26]. In some epidemiological studies schistosomiasis co-infection favors anti-malarial protective antibody responses [21, 25] while in others no significant association between schistosome-specific and Plasmodium-specific antibody responses was observed [22, 23]. Similarly, systemic cytokine levels rose with age as well as with infection and exposure to schistosome or had no effect [22, 26].
The effects of helminths on falciparum malaria in humans remain uncertain and few data are available about the interaction between intestinal parasites and Plasmodium vivax [27]. In Brazil, P. vivax is the most prevalent malaria species corresponding to 83.7 % of the 134,907 cases registered in 2014 and it is concentrated in the Amazon region where intestinal parasites infections are prevalent [28, 29].
AMA-1 is expressed on merozoites and sporozoites as a type I integral membrane protein and MSP-1 is expressed abundantly on the merozoite surface and synthesized as a 195-kDa protein and sequentially processed into a cysteine-rich 19-kDa fragment (MSP-119) [30, 31]. The proteins MSP-1 and AMA-1 are promising vaccine candidates for both P. falciparum and P. vivax and they are involved in erythrocyte invasion [32, 33].
Therefore, the aim of the study was to determine the prevalence of co-infection of malaria and intestinal parasites and whether the presence of co-infection was associated with impaired IgG responses against P. vivax proteins, apical membrane antigen-1 (AMA-1) and merozoite surface protein (MSP-119) in individuals co-infected with Plasmodium and intestinal parasites and in individuals with single infections.
Methods
Study population
The individuals who took part in this study were part of a previous study investigating the effect of intestinal parasites on the circulating levels of cytokines and inflammatory markers [20]. The study area and population were also described in detail in this study. Briefly, a cross-sectional survey was conducted in a rural settlement community of Porto Velho, municipality of Rondonia State, and Brazilian Amazon. Only individuals that lived in the area and provided a blood sample and stool samples were included in the study (279 participants).
Ethical consideration
Ethical approval was given by the Fundação Oswaldo Cruz Ethical Committee (CEP/FIOCRUZ, 492/08). Informed and written consents were obtained from all participants. For all eligible participants a clinical examination was performed. Donors positive for P. vivax and/or P. falciparum at the time of blood collection were subsequently treated using the chemotherapeutic regimen recommended by the Brazilian Ministry of Health. Participants positive for intestinal parasites were also treated.
Sample collection and diagnosis
After written informed consent and an epidemiological survey from all adult donors or from parents of donors in the case of minors, blood samples were collected by venipuncture for serological assay and a thick and thin blood smear was prepared for microscopic detection of Plasmodium. Parasitaemia was expressed as the number of parasites/µL of blood in the thick blood smear. To confirm the parasitological diagnoses, molecular analyses of all samples using primers specific for genus (Plasmodium sp.) and species (P. falciparum and P. vivax) were done. PCR amplification and detection and the PCR primers used have been previously described [34]. Subjects positive in the thick blood smear and/or PCR were considered positive for malaria infection. Blood cell counts, including haematologic indices, were done using an automatic haematology analyzer (Pentra, Horiba Medical, Montpellier, France). The individuals were considered anaemic when their haemoglobin levels were ≤13 g/dL blood in males and ≤12 g/dL blood in females.
Collection and examination of stool samples
For parasitological examinations, participants were requested to provide a morning faecal sample and a labelled screw-capped plastic container was provided. A single stool sample was collected from each subject on the following day and samples were screened for intestinal parasites and examined at the same day by direct wet mount microscopic and concentration techniques by a technician with expertise in intestinal parasites identification.
Specific antibody for Plasmodium vivax antigen-specific IgG antibody and sub-classes in plasma samples
Specific IgG antibodies to PvMSP-119 and PvAMA-1 in plasma were determined by enzyme-linked immunosorbent assays (ELISA). The expression and purification of the recombinant proteins were performed as previously described [35, 36]. The recombinant proteins were diluted in phosphate-buffered saline (PBS) pH 7.2 to a concentration of 2 μg/ml. High-binding ELISA plates (Nunc/Maxicorp) were coated with 100 μL of recombinant proteins and incubated overnight at 4 °C. Plates were washed four times with washing buffer, PBS-0.05 % Tween 20 (PBS-T) and were then blocked with blocking buffer (PBS-T containing 5 % low-fat milk) for 2 h at 37 °C. Individual plasma sample were diluted 1:100 in blocking buffer, 100 µl were added in duplicate to the respective wells and incubated for 1 h at 37 °C. After four washes with PBS-T, bound antibodies were detected with peroxidase-conjugated goat antihuman IgG (Sigma, St Louis, MO, USA) followed by o-phenylenediamine and hydrogen peroxide. The absorbance was read at 492 nm using an ELISA reader (Spectramax 250, Molecular Devices, Sunnyvale, CA, USA). The results for total IgG were expressed as reactivity indices (RI), which were calculated by dividing the mean optical density (OD) values of tested samples by the mean OD values plus three standard deviations (SD) of 24 non-exposed control individuals living in non-endemic areas of malaria (cut-off: PvAMA-1 = 0.1881, PvMSP-119 = 0.1915). As positive controls, five plasma samples from exposed native individuals with high antibodies OD levels for both proteins were used. Subjects were considered as positive to the corresponding antigen if the RI was higher than 1. An ELISA to detect the IgG sub-classes was also performed for positive responders. Plates were coated with antigen, blocked and incubated with plasma diluted 1:100 as in the ELISA for total IgG. After washing, plates were incubated for 1 h at 22 °C with mouse mAbs to human IgG sub-classes diluted in blocking buffer according to the manufacturer’s specifications. The mAbs were from clones HP-6001 for IgG1, HP-6002 for IgG2, HP-6050 for IgG3, and HP-6023 for IgG4 (Sigma) and have been used previously to characterize IgG subclass reactivity. After incubation, plates were washed and incubated for 1 h at 22 °C with peroxidase-labelled goat anti-mouse antibody (KPL) diluted 1:1,000 in blocking buffer.
Plates were washed, incubated with ABTS (2,2′-Azinobis [3-ethylbenzothiazoline-6-sulfonic acid]-diammonium salt) substrate solution, and the (OD) measured as described above. Sub-class-specific prevalence for each antigen was determined from OD values using three standard deviation (SD) above the appropriate mean OD of 24 non-exposed controls as the cut-off for positivity. The corresponding cut-offs for PvAMA-1 were: IgG1 = 0.1910, IgG2 = 0.2401, IgG3 = 0.1558, IgG4 = 0.1828, and for PvMSP-119 were: IgG1 = 0.1885, IgG2 = 0.2718, IgG3 = 0.1579, IgG4 = 0.1462.
Statistical analysis
Epidemiological and experimental data were stored in Epi- Info 3.5.1 (CDC, Atlanta, GA, USA). Statistical analysis were performed using the R statistical environment and all p values were adjusted with false discovery rate method [37]. The risk of malaria associated with intestinal parasites was estimated using odds ratios (OR) and confidence interval of 95 % (CI). Chi-squared (χ2) with Yates correction was used to calculate differences in seroprevalence between groups. Wilcoxon-Mann–Whitney rank sum test was used for comparison between M and CI groups. Differences of reactivity index values were calculated with a pairwise test for multiple comparisons of mean rank sums (Nemenyi-Tests) [38]. P values of <0.05 were considered as significant.
Results
Prevalence of malaria and intestinal parasites
Combining the results across all tests (Table 1), 279 individuals were grouped according to their infection status: individuals infected with Plasmodium only (n = 16, M); individuals co-infected with Plasmodium and intestinal parasites (48, CI); individuals infected with intestinal parasites only (98, IP) and individuals negative (117, N). The group N was defined as subjects with no symptoms, negative for Plasmodium by thick blood smear and PCR and negative for intestinal parasites by direct wet mount microscopic and concentration techniques. CI and IP groups were composed of individuals positive for intestinal parasite infection: helminths only (H), protozoa only (P), and both helminths and protozoa (P+H).
In both M and CI groups, P. vivax was the most prevalent species (81.2 and 75.0 %, respectively). The prevalence of intestinal parasites was significantly higher in individuals infected with malaria (75 %) than with those who were not infected (45 %). Of note, all study participants with malaria presented clinical symptoms, such as history of fever and headache, and no difference was observed in the parasitaemia levels between malaria and co-infected groups. Among the 146 individuals infected with intestinal parasites, ten different parasite species were detected (Fig. 1), four intestinal protozoa (Giardia intestinalis, Entamoeba coli, Entamoeba histolytica, Iodamoeba butschlii) and six helminths (Ancylostoma duodenale, Strongyloides stercoralis, Ascaris lumbricoides, Trichuris trichiura, Hymenolepis nana, Hymenolepis diminuta). Giardia intestinalis and Entamoeba coli were the most prevalent protozoa, found in single infections or associated with other species of protozoa and helminths (Ancylostoma duodenale, Strongyloides stercoralis). The prevalence of protozoan in CI group (81.25 %) was not statistically different from IP (70.4 %). In both, CI and IP groups, Giardia intestinalis and Entamoeba coli were the most prevalent protozoan and Ancylostoma duodenale, Ascaris lumbrocoides the most prevalent helminths.

Prevalence of intestinal parasites among individuals co-infected with Plasmodium and intestinal parasites (CI) and individuals infected with intestinal parasites only (IP) in the studied population. Black bars indicate the frequency of intestinal parasite species in CI group and grey bars indicate the frequency of intestinal parasites in the IP group. Y axis illustrates the species corresponding to infections with Protozoa, Helminths and Protozoa + Helminths. Numbers on top of bars indicate number of individuals infected with each species of protozoa and helminths
Characteristics of the studied groups
Table 2 summarizes the characteristics of the studied groups. Male were overrepresented in the M and CI groups and no differences were observed in the median age between all groups. Comparing M and CI groups, there were no differences in age, time since last malaria episode (LME) and eosinophils count. Anaemia was more prevalent in individuals from malaria and co-infected groups than in IP and N. Additionally, IP and N groups were similar and differed from M and CI in LME, and both groups presented higher eosinophils counts.
Specific IgG antibody responses to Plasmodium vivax AMA-1 and MSP-119
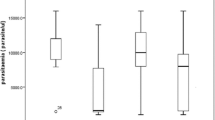
The percentage of individuals containing naturally acquired IgG antibodies against PvAMA-1 and PvMSP-119 is presented in Fig. 2. IgG antibodies to PvAMA-1 and/or PvMSP-119 were detected in 74 % of the population. The prevalence of individuals that recognize both proteins (55 %) was higher than those that recognize a single protein (8 % PvAMA-1 and 11 % PvMSP-119). To determine whether the presence of co-infection was associated with impaired IgG responses, the prevalence of specific IgG directed to PvAMA-1 and PvMSP-119 between groups were compared (Fig. 3). The prevalence of specific IgG was similar for both proteins in all four groups and among the groups, the lowest prevalence was in IP. The M group presented the highest frequency of IgG responders as compared to uninfected, and no appreciable differences were observed between M and CI groups (Fig. 3a, c). When plasma levels from individual serum samples were compared, the RI values obtained for the recombinant protein PvAMA-1 were not significantly higher than the values obtained for PvMSP-119 (Fig. 3b, d). However, the RIs were lower in IP group for both proteins.

Frequency of specific antibody response to PvMSP-119 and PvAMA-1 of individuals from a malaria-endemic area, determined by ELISA. Individuals were grouped in responders and non-responders for the recombinant proteins. The Y axis represents the frequency (%) of individuals responding to PvAMA1+PvMSP-119, PvAMA-1 or PvMSP-119 only, and individuals non-responders to PvAMA-1 and/or PvMSP-119

Prevalence and reactivity index of IgG antibodies to P. vivax AMA1 and MSP-119 recombinant antigens. M individuals infected with Plasmodium only, CI individuals co-infected with Plasmodium and intestinal parasites, IP individuals infected with intestinal parasites only and N negative for both malaria and intestinal parasites. a Prevalence of PvAMA-1 IgG in M, CI, IP and N groups. b IgG Reactivity Index for PvAMA-1 among M, CI, IP and N groups. c Prevalence of PvMSP-119 IgG in M, CI, IP and N groups. d IgG Reactivity Index for PvMSP-119 among M, CI, IP and N groups. In b and d panels, the horizontal bolded-bar in the Box and whisker plot represents the median value and all individual data points are shown as dots. Whiskers extend ×1.5 of the interquartile range or to the minimum/maximum value, when these fall within ×1.5 of the interquartile range. Differences of reactivity index values were calculated from pairwise test for multiple comparisons of mean rank sums (Nemenyi-Tests) and all differences of prevalence between groups were calculated using X2 with Yates correction. Significant statistical differences are represented in the bars and the level of significance expressed as *P < 0.05, **P < 0.001, ***P < 0.0001
Results in Fig. 4 show the prevalence and reactivity index of IgG response specific to PvAMA-1 and PvMSP-1 in the groups CI and IP among individuals infected with helminths (H), protozoa (P) and both protozoa and helminths (PH). There was no significant changes in the prevalence and RI of antibody to PvAMA-1 (Fig. 4a) and PvMSP-1 (Fig. 4b) in CI and IP groups when individuals infected with H, P and PH were compared in each group. However, IgG response to both PvAMA-1 and PvMSP-1 were lower in individuals with protozoa in the Intestinal parasites group when compared to Co-infected group. Similar results were also observed when the reactivity index were compared between the same groups. Although in some groups the sample size were small after stratification in H, P and HP, the group of individuals with P in both CI and IP groups seemed to be comparable. In the group Intestinal parasites, individuals infected with protozoa (P) also presented lower antibodies prevalence and RI to PvAMA-1 and PvMSP-1 than the group Malaria (p < 0.001 for PvAMA-1 and Pv-MSP-1) and negative (p < 0.01 for PvAMA-1 and PvMSP-1). In contrast, no differences were observed in prevalence and RI of antibodies to PvAMA-1 and PvMSP-1 between co-infected group infected with P and Malaria or Negative groups.

Prevalence and reactivity index of IgG antibodies to PvAMA-1 and PvMSP-119 in the group of individuals co-infected with malaria and intestinal parasites (CI) and infected with intestinal parasites only (IP) according to intestinal parasite infection. H individuals infected with helminths, P individuals infected with protozoa, PH individuals infected with protozoa + helminths. a Prevalence of PvAMA-1 IgG in CI and IP groups among H, P and PH infected individuals; b IgG reactivity index for PvAMA-1 in CI and IP groups among H, P and PH infected individuals; c Prevalence of PvMSP-119 IgG in CI and IP groups among H, P and PH infected individuals; d IgG Reactivity Index for PvMSP-119 in CI and IP groups among H, P and PH infected individuals. In b and d panels, the horizontal bolded-bar in the Box and whisker plot represents the median value and all individual data points are shown as dots. Whiskers extend ×1.5 of the interquartile range or to the minimum/maximum value, when these fall within ×1.5 of the interquartile range. Differences of reactivity index values were calculated from pairwise test for multiple comparisons of mean rank sums (Nemenyi-Tests) and all differences of prevalence between groups were calculated using X2 with Yates correction. Significant statistical differences are represented in the bars and the level of significance expressed as *P < 0.05, **P < 0.001, ***P < 0.0001
Comparison of IgG subclasses to Plasmodium vivax PvAMA-1 and PvMSP-119
Since the IgG subclass produced in response to a given antigen may determine the function of the antibody, plasma samples positive for total anti-PvAMA-1 and anti-PvMSP-1 IgG were evaluated for IgG sub-class responses. Among the IgG responders, the cytophilic sub-class IgG1 and IgG3 were predominant in all groups for PvAMA-1 and IgG1, IgG3 and IgG4 for PvMSP-119. In the case of non-cytophilic antibodies to PvAMA-1, IgG2 was significantly higher in IP and N group when compared to M and CI, while IgG4 was higher in IP group (Fig. 5a, c). No differences were observed in the prevalence of non-cytophilic antibodies specific to PvMSP-119 among the groups. RIs of specific IgG sub-classes were also measured and increased IgG1 followed by IgG3 were detected for both proteins in all groups (Fig. 5b, d). In contrast, although IgG2 and IgG4 were frequent in the groups, their RI was low or similar for both proteins in all groups. However, RI of IgG2 to AMA-1 was significantly higher in IP when compared to CI group while IgG4 was higher in IP when compared to N and CI groups. Moreover, IgG1 RI to MSP-1 was significantly lower in IP group than in N group.

Prevalence and reactivity index of IgG subclasses to PvAMA-1 and PvMSP-119. M individuals infected with Plasmodium only, CI individuals co-infected with Plasmodium and intestinal parasites, IP individuals infected with intestinal parasites only and N negative for both malaria and intestinal parasites. a Prevalence of IgG subclasses to PvAMA-119 among groups; b IgG subclasses reactivity index for PvAMA-1 among; c prevalence of PvMSP-119 IgG subclasses in M, CI, PI and N groups; d IgG subclasses reactivity index directed for PvMSP-119 among M, CI, IP and N groups. X2 with Yates correction was used to evaluate subclasses differences into the groups. In b and d panels, the horizontal bolded-bar in the Box and whisker plot represents the median value and all individual data points are shown as dots. Whiskers extend ×1.5 of the interquartile range or to the minimum/maximum value, when these fall within ×1.5 of the interquartile range. Differences of reactivity index values were calculated from pairwise test for multiple comparisons of mean rank sums (Nemenyi-Tests) and all differences of prevalence between groups were calculated using X2 with Yates correction. Significant statistical differences are represented in the bars and the level of significance expressed as *P < 0.05, **P < 0.001, ***P < 0.0001
Discussion
Although some studies have explored the influence of helminth co-infections on antibody production directed to P. falciparum antigens [21, 25, 39, 40], this is the first study to evaluate the influence of intestinal parasites on the acquired specific humoral immune responses to P. vivax malaria antigens [21, 24, 25, 39]. The present results show that in malaria-endemic area of Rondonia State, the prevalence of individuals singly infected with intestinal parasites (52.3 %) and co-infected with malaria and intestinal parasites (17.2 %) was higher than that singly infected with malaria (5.7 %). Some epidemiological studies have demonstrated an increased risk of infection by P. falciparum in those individuals co-infected with helminths but the results were conflicting [3, 6, 27, 40]. However, in the present study helminth infection was not predominant, the protozoan Giardia intestinalis alone or associated with other parasites was the most prevalent parasite in IP and CI groups, and P. vivax was the predominant Plasmodium species. Studies reporting the prevalence of co-infection in malaria-endemic areas of Brazil are scarce but a high prevalence of intestinal parasites has been reported in several areas of the Brazilian Amazon [27–29]. Although the prevalence of intestinal parasites was significantly higher in individuals infected with malaria, parasitaemia did not differ between co-infected and malaria-infected individuals. On the other hand, anaemia was frequent in both groups and increased numbers of eosinophils were observed in individuals with intestinal parasites and in the uninfected group. It seems that the haematological alteration observed in both malaria and co-infected groups is due to the effect of malaria, rather than intestinal parasites or co-infection. Indeed, anaemia is a common feature of acute malaria while increased number of eosinophils is common in helminths infections [41].
The study of antibody responses to Plasmodium antigens is a key process to the discovery and development of malaria vaccines. Several studies report high antibody response to P. vivax antigens in individuals exposed to malaria infection [42–44]. In malaria-endemic areas of Brazil, high prevalences of antibodies specific to P. vivax circumsporozoite protein [45], PvMSP-1 [46], MSP-9 [47], and PvAMA-1 [44] have been reported. In the present study, 73.8 % of individuals presented antibodies for at least one of the two studied proteins, indicating that both proteins are immunogenic. These values are comparable to other studies in the Amazon region [44, 46, 48, 49]. Higher prevalences and RI of specific antibodies were observed in the groups of individuals with patent P. vivax infection (groups M and CI) reaching almost 100 % in the group of individuals singly infected with malaria (M group). This confirms that PvAMA-1 and PvMSP-119 are immunogenic molecules during natural malaria infections and that the presence of intestinal parasites does not interfere in the antibody response to both antigens. However, it cannot be ignored the reduced IgG prevalence and RI to both proteins in the group of individuals singly infected with intestinal parasites (IP), even when compared with the Negative Group. These results cannot be compared to those that reported reduced levels of IgG directed to P. falciparum antigens in helminths and P. falciparum co-infection, since helminth infections counted for only 19.7 % of the intestinal parasites detected in IP and 29.6 % in CI groups [21, 24]. On the other hand, Protozoa were the most prevalent intestinal parasites in the IP (70 %) and CI (80 %) and reduced antibodies prevalence and reactivity index in the IP group could be due to the presence of intestinal protozoa. However, in the group CI, the IgG prevalence and reactivity indexed were not reduced and were similar to the group infected with malaria only (M). In the CI group, the effect of intestinal protozoa might not be relevant when compared to the effect of Plasmodium in the immune response. It seems that Plasmodium have some effect on intestinal protozoa and not the contrary since lower antibodies response is only observed in IP group. Chronic protozoan infections have previously been suggested to be associated with type 1-regulatory immune response and combined with the induced pro-inflammatory response induced by the Plasmodium could balance the anti-inflammatory effect of the response [50]. Studies on malaria and protozoan co-infections are rare and the effect of intestinal protozoa on malaria infections or the contrary it is unknown.
Analysis of IgG isotypes response to PvAMA-1 and PvMSP-119 antigens is important for evaluating protective activity as IgG subclasses differ in their immune effector functions and having such knowledge is important for understanding the immunity to vaccine development. The results of the present study confirmed studies that showed IgG1 and IgG3 isotypes, previously identified as protective to malaria, were the predominant subclasses in response to both antigens in all groups [44, 46, 51]. Therefore, the presence of intestinal parasites in malaria-infected individuals does not seem to alter the cytophilic and non-cytophilic response to PvAMA-1 and PvMSP-119 in malaria and intestinal parasites co-infected individuals. However, in the IP group IgG1 reactivity index to MSP-1 were lower when compared to individuals from N. These results suggest that the presence of intestinal parasites can induce non-cytophilic antibodies that could counterbalance the production of cytophilic antibodies in IP group. The increased prevalence observed for non-cytophilic IgG2 response to PvAMA-1 in IP group does not seem to be due to intestinal parasites since N group also presented increased IgG2. In this group IgG4 RI to AMA-1 were also increased when compared to CI and N groups. Studies that investigate malaria and helminths co-infection reported a decrease of cytophilic IgG1 and IgG3 responses to MSP-1 and an increase in non-cytophilic IgG4 response to MSP-3 in individuals infected by Ascaris lumbricoides, Strongyloides stercolaris, Trichuris trichiura and Hymenolepis nana [52]. Similarly, a generalized decrease in cytophilic IgG directed to both GLURP, MSP-3, AMA-1, MSP-1, and MSP-2 and a significant negative association between Schistosoma infection and IgG1 and IgG3 directed to anti-malarial total extract was reported in individuals infected with Schistosoma haematobium and malaria [24]. In contrast, an increased IgG1 to MSP-1 response as well as IgG1 and IgG3 to total extract in malaria and Schistosoma haematobium co-infection was also reported [21]. Although protozoa infection was predominant in the present study, it is generally believed that in helminth infection the type 2 T helper (Th2) response induced by helminths could alter the natural immune response of the host to Plasmodium, due to the anti-inflammatory effect of cytokines induced by helminths. However, the cytokine profile of this population have been published and for malaria-infected individuals (M and CI groups) the profile showed high levels of IL-1, IL-6, TNF, IL-10, and CRP and decreased levels of IL-17A while for malaria-negative individuals (IP and N) the profile was high levels of IL-17A, NO and decreased levels of IL-10 and CRP [20]. Therefore, it seems that intestinal parasites co-infection (mainly protozoan) does not influence the plasmatic cytokine levels of acute malaria-infected individuals.
Conclusions
The presence of antibody responses to both P. vivax AMA-1 and MSP-1 proteins in all groups indicated that the participants had been exposed to malaria infection and the IgG subclass responses were largely in agreement with previously published results. Although in the present work there were changes in total IgG directed to PvAMA1 and PvMSP-119 in Intestinal parasites group, a decrease in IgG and in cytophilic responses associated to co-infections was not observed. These responses might perhaps relate to other factors such as antigen properties, number and time of exposure, host age and genetic determinants. Further studies should be conducted to determine the effect of intestinal protozoa in the immune response to malaria antigens.
References
Griffiths EC, Pedersen AB, Fenton A, Petchey OL. The nature and consequences of coinfection in humans. J Infect. 2011;63:200–6.
WHO. Control of tropical disease. Geneva: World Health Organization; 1998.
Nacher M, Gay F, Singhasivanon P, Krudsood S, Treeprasertsuk S, Mazier D, et al. Ascaris lumbricoides infection is associated with protection from cerebral malaria. Parasite Immunol. 2000;22:107–13.
Brutus L, Watier L, Hanitrasoamampionona V, Razanatsoarilala H, Cot M. Confirmation of the protective effect of Ascaris lumbricoides on Plasmodium falciparum infection: results of a randomized trial in Madagascar. Am J Trop Med Hyg. 2007;77:1091–5.
Lemaitre M, Watier L, Briand V, Garcia A, Le Hesran JY, Cot M. Coinfection with Plasmodium falciparum and Schistosoma haematobium: additional evidence of the protective effect of Schistosomiasis on malaria in Senegalese children. Am J Trop Med Hyg. 2014;90:329–34.
Lyke KE, Dicko A, Dabo A, Sangare L, Kone A, Coulibaly D, et al. Association of Schistosoma haematobium infection with protection against acute Plasmodium falciparum malaria in Malian children. Am J Trop Med Hyg. 2005;73:1124–30.
Nacher M, Singhasivanon P, Yimsamran S, Manibunyong W, Thanyavanich N, Wuthisen R, et al. Intestinal helminth infections are associated with increased incidence of Plasmodium falciparum malaria in Thailand. J Parasitol. 2002;88:55–8.
Sokhna C, Le Hesran JY, Mbaye PA, Akiana J, Camara P, Diop M, et al. Increase of malaria attacks among children presenting concomitant infection by Schistosoma mansoni in Senegal. Malar J. 2004;3:43.
Spiegel A, Tall A, Raphenon G, Trape JF, Druilhe P. Increased frequency of malaria attacks in subjects co-infected by intestinal worms and Plasmodium falciparum malaria. Trans R Soc Trop Med Hyg. 2003;97:198–9.
Shapiro AE, Tukahebwa EM, Kasten J, Clarke SE, Magnussen P, Olsen A, et al. Epidemiology of helminth infections and their relationship to clinical malaria in southwest Uganda. Trans R Soc Trop Med Hyg. 2005;99:18–24.
Ojurongbe O, Adegbayi AM, Bolaji OS, Akindele AA, Adefioye OA, Adeyeba OA. Asymptomatic falciparum malaria and intestinal helminths co-infection among school children in Osogbo, Nigeria. J Res Med Sci. 2011;16:680–6.
Abanyie FA, McCracken C, Kirwan P, Molloy SF, Asaolu SO, Holland CV, et al. Ascaris co-infection does not alter malaria-induced anaemia in a cohort of Nigerian preschool children. Malar J. 2013;12:1.
Florey LS, King CH, Van Dyke MK, Muchiri EM, Mungai PL, Zimmerman PA, et al. Partnering parasites: evidence of synergism between heavy Schistosoma haematobium and Plasmodium species infections in Kenyan children. PLoS Negl Trop Dis. 2012;6:e1723.
Wang ML, Cao YM, Luo EJ, Zhang Y, Guo YJ. Pre-existing Schistosoma japonicum infection alters the immune response to Plasmodium berghei infection in C57BL/6 mice. Malar J. 2013;12:322.
Laranjeiras RF, Brant LC, Lima AC, Coelho PM, Braga EM. Reduced protective effect of Plasmodium berghei immunization by concurrent Schistosoma mansoni infection. Mem Inst Oswaldo Cruz. 2008;103:674–7.
Helmby H, Kullberg M, Troye-Blomberg M. Altered immune responses in mice with concomitant Schistosoma mansoni and Plasmodium chabaudi infections. Infect Immun. 1998;66:5167–74.
Saric J, Li JV, Swann JR, Utzinger J, Calvert G, Nicholson JK, et al. Integrated cytokine and metabolic analysis of pathological responses to parasite exposure in rodents. J Proteome Res. 2010;9:2255–64.
Cooper PJ, Espinel I, Wieseman M, Paredes W, Espinel M, Guderian RH, et al. Human onchocerciasis and tetanus vaccination: impact on the postvaccination antitetanus antibody response. Infect Immun. 1999;67:5951–7.
Sabin EA, Araujo MI, Carvalho EM, Pearce EJ. Impairment of tetanus toxoid-specific Th1-like immune responses in humans infected with Schistosoma mansoni. J Infect Dis. 1996;173:269–72.
Sanchez-Arcila JC, Perce-da-Silva Dde S, Vasconcelos MP, Rodrigues-da-Silva RN, Pereira VA, Aprigio CJ, et al. Intestinal parasites coinfection does not alter plasma cytokines profile elicited in acute malaria in subjects from endemic area of Brazil. Mediators Inflamm. 2014;2014:857245.
Diallo TO, Remoue F, Gaayeb L, Schacht AM, Charrier N, De Clerck D, et al. Schistosomiasis coinfection in children influences acquired immune response against Plasmodium falciparum malaria antigens. PLoS One. 2010;5:e12764.
Imai N, Rujeni N, Nausch N, Bourke CD, Appleby LJ, Cowan G, et al. Exposure, infection, systemic cytokine levels and antibody responses in young children concurrently exposed to schistosomiasis and malaria. Parasitology. 2011;138:1519–33.
Sangweme DT, Midzi N, Zinyowera-Mutapuri S, Mduluza T, Diener-West M, Kumar N. Impact of schistosome infection on Plasmodium falciparum Malariometric indices and immune correlates in school age children in Burma Valley Zimbabwe. PLoS Negl Trop Dis. 2010;4:e882.
Courtin D, Djilali-Saiah A, Milet J, Soulard V, Gaye O, Migot-Nabias F, et al. Schistosoma haematobium infection affects Plasmodium falciparum-specific IgG responses associated with protection against malaria. Parasite Immunol. 2011;33:124–31.
Mutapi F, Roussilhon C, Mduluza T, Druilhe P. Anti-malaria humoral responses in children exposed to Plasmodium falciparum and Schistosoma haematobium. Mem Inst Oswaldo Cruz. 2007;102:405–9.
Mutapi F, Winborn G, Midzi N, Taylor M, Mduluza T, Maizels RM. Cytokine responses to Schistosoma haematobium in a Zimbabwean population: contrasting profiles for IFN-gamma, IL-4, IL-5 and IL-10 with age. BMC Infect Dis. 2007;7:139.
Melo GC, Reyes-Lecca RC, Vitor-Silva S, Monteiro WM, Martins M, Benzecry SG, et al. Concurrent helminthic infection protects schoolchildren with Plasmodium vivax from anemia. PLoS One. 2010;5:e11206.
de Souza EA, da Silva-Nunes M, Malafronte Rdos S, Muniz PT, Cardoso MA, Ferreira MU. Prevalence and spatial distribution of intestinal parasitic infections in a rural Amazonian settlement, Acre State, Brazil. Cad Saude Publica. 2007;23:427–34.
Araujo CF, Fernandez CL. Prevalence of intestinal parasitosis in the city of Eirunepe, Amazon. Rev Soc Bras Med Trop. 2005;38:69 (in Portuguese).
Blackman MJ, Heidrich HG, Donachie S, McBride JS, Holder AA. A single fragment of a malaria merozoite surface protein remains on the parasite during red cell invasion and is the target of invasion-inhibiting antibodies. J Exp Med. 1990;172:379–82.
Bannister LH, Hopkins JM, Dluzewski AR, Margos G, Williams IT, Blackman MJ, et al. Plasmodium falciparum apical membrane antigen 1 (PfAMA-1) is translocated within micronemes along subpellicular microtubules during merozoite development. J Cell Sci. 2003;116:3825–34.
Dutta S, Ware LA, Barbosa A, Ockenhouse CF, Lanar DE. Purification, characterization, and immunogenicity of a disulfide cross-linked Plasmodium vivax vaccine candidate antigen, merozoite surface protein 1, expressed in Escherichia coli. Infect Immun. 2001;69:5464–70.
Kocken CH, Dubbeld MA, Van Der Wel A, Pronk JT, Waters AP, Langermans JA, et al. High-level expression of Plasmodium vivax apical membrane antigen 1 (AMA-1) in Pichia pastoris: strong immunogenicity in Macaca mulatta immunized with P. vivax AMA-1 and adjuvant SBAS2. Infect Immun. 1999;67:43–9.
Snounou G, Viriyakosol S, Zhu XP, Jarra W, Pinheiro L, do Rosario VE, et al. High sensitivity of detection of human malaria parasites by the use of nested polymerase chain reaction. Mol Biochem Parasitol. 1993; 61:315–20.
Cunha MG, Rodrigues MM, Soares IS. Comparison of the immunogenic properties of recombinant proteins representing the Plasmodium vivax vaccine candidate MSP1(19) expressed in distinct bacterial vectors. Vaccine. 2001;20:385–96.
Vicentin EC, Francoso KS, Rocha MV, Iourtov D, Dos Santos FL, Kubrusly FS, et al. Invasion-inhibitory antibodies elicited by immunization with Plasmodium vivax apical membrane antigen-1 expressed in Pichia pastoris yeast. Infect Immun. 2014;82:1296–307.
Team RC. R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing; 2013.
Pohlert T. The pairwise multiple comparison of mean ranks package (PMCMR). 2014.
Hartgers FC, Obeng BB, Boakye D, Yazdanbakhsh M. Immune responses during helminth-malaria co-infection: a pilot study in Ghanaian school children. Parasitology. 2008;135:855–60.
Nacher M. Severe malaria attack is associated with high prevalence of Ascaris lumbricoides infection among children in rural Senegal. Trans R Soc Trop Med Hyg. 2005;99:161–3.
Meeusen EN, Balic A. Do eosinophils have a role in the killing of helminth parasites? Parasitol Today. 2000;16:95–101.
Ladeia-Andrade S, Ferreira MU, Scopel KK, Braga EM, Bastos Mda S, Wunderlich G, et al. Naturally acquired antibodies to merozoite surface protein (MSP)-1(19) and cumulative exposure to Plasmodium falciparum and Plasmodium vivax in remote populations of the Amazon Basin of Brazil. Mem Inst Oswaldo Cruz. 2007;102:943–51.
Lima-Junior JC, Jiang J, Rodrigues-da-Silva RN, Banic DM, Tran TM, Ribeiro RY, et al. B cell epitope mapping and characterization of naturally acquired antibodies to the Plasmodium vivax merozoite surface protein-3alpha (PvMSP-3alpha) in malaria exposed individuals from Brazilian Amazon. Vaccine. 2011;29:1801–11.
Morais CG, Soares IS, Carvalho LH, Fontes CJ, Krettli AU, Braga EM. Antibodies to Plasmodium vivax apical membrane antigen 1: persistence and correlation with malaria transmission intensity. Am J Trop Med Hyg. 2006;75:582–7.
Arruda ME, Zimmerman RH, Souza RM, Oliveira-Ferreira J. Prevalence and level of antibodies to the circumsporozoite protein of human malaria parasites in five states of the Amazon region of Brazil. Mem Inst Oswaldo Cruz. 2007;102:367–71.
Soares IS, da Cunha MG, Silva MN, Souza JM, Del Portillo HA, Rodrigues MM. Longevity of naturally acquired antibody responses to the N- and C-terminal regions of Plasmodium vivax merozoite surface protein 1. Am J Trop Med Hyg. 1999;60:357–63.
Lima-Junior JC, Rodrigues-da-Silva RN, Banic DM, Jiang J, Singh B, Fabricio-Silva GM, et al. Influence of HLA-DRB1 and HLA-DQB1 alleles on IgG antibody response to the P. vivax MSP-1, MSP-3alpha and MSP-9 in individuals from Brazilian endemic area. PLoS One. 2012;7:e36419.
Barbedo MB, Ricci R, Jimenez MC, Cunha MG, Yazdani SS, Chitnis CE, et al. Comparative recognition by human IgG antibodies of recombinant proteins representing three asexual erythrocytic stage vaccine candidates of Plasmodium vivax. Mem Inst Oswaldo Cruz. 2007;102:335–9.
Rodrigues MH, Rodrigues KM, Oliveira TR, Comodo AN, Rodrigues MM, Kocken CH, et al. Antibody response of naturally infected individuals to recombinant Plasmodium vivax apical membrane antigen-1. Int J Parasitol. 2005;35:185–92.
Diaz A, Allen JE. Mapping immune response profiles: the emerging scenario from helminth immunology. Eur J Immunol. 2007;37:3319–26.
Fernandez-Becerra C, Sanz S, Brucet M, Stanisic DI, Alves FP, Camargo EP, et al. Naturally-acquired humoral immune responses against the N- and C-termini of the Plasmodium vivax MSP1 protein in endemic regions of Brazil and Papua New Guinea using a multiplex assay. Malar J. 2010;9:29.
Roussilhon C, Brasseur P, Agnamey P, Perignon JL, Druilhe P. Understanding human-Plasmodium falciparum immune interactions uncovers the immunological role of worms. PLoS One. 2010;5:e9309.
Authors’ contributions
JOF conceived and supervised the study. JOF and DMB designed the study. Fieldwork and sample collection was performed by JOF, JCSA, JCLJ, DSPS, MPAV JRN, CJLA, and DMB; JCSA, MMF, VAP, and JCSA carried out the experiments. MMR and ISS produced the recombinant proteins. Data were collected and analysed by JCSA and MMF with support from JOF. The first draft of this manuscript was written by JCSA and MMF; JOF critically read and advised on the manuscript. All authors read and approved the final version and agreed to the submission. All authors read and approved the final manuscript.
Acknowledgements
The authors are in debt to the individuals who participated in this study, the Secretary of Health and Laboratory Central (LACEN) of Rondonia, the local malaria control team in Joana D´Arc settlement for their logistic support and the Institute Oswaldo Cruz (Fiocruz) for overall support. This work was supported by PRONEX Malaria network funded by the Brazilian Ministry of Science and Technology (MCT), Conselho Nacional de Desenvolvimento Cientifico e Tecnologico (CNPq, Brazil) and Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ, Brazil). PROEP, Instituto Oswaldo Cruz (FIOCRUZ, Brazil). JOF is recipient of a Research Productivity Fellowship from CNPq, JCSA is recipient of a fellowship from Instituto Oswaldo Cruz and VAR, MM from CNPq.
Competing interests
The authors have declared that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Sánchez-Arcila, J.C., de França, M.M., Pereira, V.A. et al. The influence of intestinal parasites on Plasmodium vivax-specific antibody responses to MSP-119 and AMA-1 in rural populations of the Brazilian Amazon. Malar J 14, 442 (2015). https://doi.org/10.1186/s12936-015-0978-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-015-0978-7