
Abstract
Background
For the results of clinical trials to have external validity, the patients included in the study must be representative of the population presenting in the general clinical settings. A scoping literature review was performed to evaluate how the eligibility criteria used in anti-malarial efficacy and safety trials translate into patient selection.
Methods
A search of the WorldWide Antimalarial Resistance Network (WWARN) Clinical Trials Publication Library, MEDLINE, The Cochrane Library, and clinicaltrials.gov was conducted to identify trials investigating anti-malarial efficacy and safety, published between 14th April 2001 and 31st December 2017. An updated search using the WWARN Clinical Trial Publication Library was undertaken to identify eligible publications from 1st January 2018 to 31st July 2021. The review included studies in patients of any age with uncomplicated malaria and any pharmaceutical therapeutic intervention administered. The proportion of trials with malaria-positive patients excluded was calculated and linked to the reported reason for exclusion. A subgroup analysis on eligibility criteria and trial baseline demographics was conducted to assess whether criteria are complied with when recruiting patients.
Results
Out of 847 studies, 176 (21%) trials were included in the final synthesis, screening a total of 157,516 malaria-positive patients, of whom 56,293 (36%) were enrolled and treated. Across the 176 studies included, 84 different inclusion and exclusion criteria were identified. The reason for exclusion of patients who tested positive for malaria was reported in 144 (82%) studies. Three criteria account for about 70% of malaria-positive patients excluded: mixed-species malaria infections or other specific Plasmodium species, parasite counts outside the set study ranges, and refusal of consent.
Conclusions
Nearly two-thirds of the malaria-positive subjects who present to health facilities are systematically excluded from anti-malarial treatment trials. Reasons for exclusions are largely under-reported. Anti-malarial treatment in the general population is informed by studies on a narrow selection of patients who do not fully represent the totality of those seeking antimalarial treatment in routine practice. While entry criteria ensure consistency across trials, pragmatic trials are also necessary to supplement the information currently available and improve the external validity of the findings of malaria clinical trials.
Similar content being viewed by others
Background
Despite significant successes in malaria control, over 200 million malaria cases still occur globally every year, requiring treatment [1]. Guidelines for the management of clinical malaria are largely based on empirical evidence from clinical efficacy trials [2].
Standardizing trial methodologies is important for comparability across sites and over time [3], especially when monitoring efficacy for possible parasite resistance, and facilitates aggregating and meta-analysing findings [3,4,5]. Eligibility criteria tend to be stricter during the clinical development of a new medicine (phase II-III clinical trials) but are expected to become more inclusive as knowledge of the treatment increases, in post-registration (phase IV) studies. However, if clinical trials are systematically selective in their eligibility criteria, this may result in a proportional under-representation of certain segments of the patient population seen in clinical practice and limit the generalizability of the findings in the general population [5]. When determining the programmatic effectiveness of a treatment, trial methodology, notably eligibility criteria, should be adapted to reflect the full range of the malaria patients seen in clinical practice.
The World Health Organization (WHO) guidelines for the assessment of anti-malarial drug efficacy in falciparum malaria (see Box 1) are geared towards ensuring that treatments are consistently tested to measure efficacy and monitor parasite resistance [6]. A different question is whether these trials also provide a comprehensive picture of the efficacy and safety of treatments across the range of malaria patients routinely seen in the clinics.
This scoping review was conducted to assess the representativeness of the study participants enrolled in malaria clinical trials vis-à-vis the general population by identifying the reasons for excluding patients who had tested malaria-positive from the published literature and calculating the proportion of patients excluded.
Methods
The Preferred Reporting Items for Systematic reviews and Meta-Analyses extension (PRISMA) methodology was used [8].
Literature search
Data for this review were identified through searches of MEDLINE, the WorldWide Antimalarial Research Network (WWARN) Clinical Trials Publication Library [9], The Cochrane Library, clinicaltrials.gov, and manually examined bibliographic references from relevant articles using the search terms “malaria” AND “therapy” OR “treatment” OR “therapy” OR “therapeutics”. Literature search strategies were developed using the medical subject headings (MeSH) terms and text words related to uncomplicated malaria pharmaceutical therapy. Search terms and conditions are provided as supplementary information (see Additional file 3). The initial search was limited to trials published between 14th April 2001 and 31st December 2017. The starting date was selected as it correlated with the publication of the first Consolidated Standards of Reporting Trials (CONSORT) statement [10]. Articles were limited to those published in English, Portuguese, Spanish, or French and reviewed for their adherence to the CONSORT statement and reporting of malaria clinical trial eligibility criteria.
An update search using the WWARN Clinical Trial Publication Library, a living systematic review of all malaria clinical efficacy trials [11], was conducted to identify eligible studies published from 1st January 2018 to the latest update available, 31st July 2021.
Study selection
Studies identified from the search were screened for eligibility using the following criteria. A study was included if it met all the criteria.
-
a non-comparative or comparative design (randomized controlled trial (RCT), cluster RCT, or controlled (non-randomized) clinical trial);
-
uncomplicated symptomatic malaria, caused by parasitologically-confirmed Plasmodium falciparum, Plasmodium vivax, Plasmodium malariae, Plasmodium ovale, or Plasmodium knowlesi;
-
a CONSORT flow diagram [12], or similar adaptation, available with the total number of patients screened, the total number of malaria-positive patients and the total number of malaria-positive patients excluded;
There were no restrictions on study settings or age of the patients enrolled. Studies were excluded if they met one of the following criteria: phase 1 (healthy volunteers), studies on severe malaria, cross-sectional studies, case-series and case-reports, meta-analyses, observational studies, studies on prevention, prophylaxis, or animal studies.
Data extraction and management
Data extraction from the initial search was conducted by one researcher (MZ), using a detailed predefined variable dictionary and partially checked by two other researchers (CH, PLO). Extraction of data from eligible studies identified in the update search was completed by one researcher (LA) and validated by another researcher (VC) using the same predefined variable dictionary. To ensure consistency across the totality of extracted data, two researchers (LA, VC) reviewed and validated the information extracted from the initial search. Information on study inclusion and exclusion criteria, number of patients excluded for each criterion were extracted from the text and the CONSORT flow diagram, and data on population demographics were extracted from tables and text. Information was recorded on a standardized REDCap database [13, 14] and analysed with R studio and Excel. Source data used for the analysis, and the associated dictionary are available as Additional files 1 and 2.
Further information on the recording of the data items, baseline demographics, and the subsequent subgroup narrative analysis can be found in Additional files 2 and 7.
Results
Search results, number of eligible articles
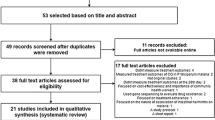
Of the 1493 articles screened by title and abstract (Fig. 1), 646 were excluded. Of these excluded, 532 were published prior to the CONSORT 2001 cut-off date (14th April 2001); 79 full texts were not accessible, 11 focused on severe malaria, 20 focused on prevention, and 4 contained ineligible study designs. The remaining 847 full-text articles were accessed and assessed for eligibility. Of these, 291 (34%) were excluded for not providing sufficient information on eligibility and exclusions (such as absence of the CONSORT Flow Diagram or similar adaptation in the manuscript), and/or not meeting other inclusion criteria. From the remaining 556 records, a further 132 publications were excluded from the analysis as they did not provide the total number of subjects screened, and another 248 for not reporting the total number of malaria-positive screened as well as the total number of malaria-positive and excluded screened patients from the clinical trial. A total of 176 records were retained in the final synthesis (see Additional file 9), accounting for 157,516 malaria-positive patients diagnosed of whom 56,293 were enrolled and treated. These 176 papers represent 21% of the 847 identified on the treatment of uncomplicated malaria published after the CONSORT 2001 statement. The species and geographical distribution of studies are summarized in Table 2.

PRISMA flow chart representing the number of items identified in the search and subsequently screened and assessed for eligibility. The search strategy and eligibility criteria are summarized in the Methods section and further details are given in the supplementary information
Study eligibility criteria
Across the 176 eligible publications, 48 (27%) referenced either WHO guidelines [3, 15,16,17] for the assessment of anti-malarial drug efficacy in falciparum malaria (90%) or other protocols [18,19,20] for the definition of the eligibility criteria (see Box 1). The definitions of the study inclusion and exclusion criteria extracted from each study are described in Additional file 2.
Eighty-four (84) eligibility criteria were identified, 17 inclusions and 77 exclusions, with ten criteria reported in either inclusion or exclusion eligibility sections, five of which (parasitaemia, history of fever or current fever, temperature, pregnancy, haemoglobin level) are described in Fig. 2 and the remaining in Additional file 4. Twenty eligibility criteria were commonly reported across 25% of the publications with a large proportion of the trials requiring consent (n = 174, 99%) of the patient or guardian to be enrolled in the trial. Two of the eligible trials did not explicitly report having requested consent to enrol patients in the study. As inclusion criteria, out of the 176 studies, 151 of the eligible studies (86%) required specific age ranges for inclusion, 121 (69%) had history of fever or current fever, or in 118 (67%) documentation of body temperature above a predefined cut-off. Ability to comply with the study follow-up, ability to consume oral medication and specific weight ranges, and proximity to the study centre, were reported in 61 (35%), 52 (30%), 52 (30%), respectively. As exclusion criteria, 150 studies (85%) excluded patients with signs and symptoms of severe malaria (123, 82%), 15 (10%), 11 (7%) and 1 (0.7%) studies for P. falciparum, mixed, P. vivax and P. knowlesi trials, respectively. Patients with mixed infections or other specific Plasmodium species (143/176, 81%), recent use of an anti-malarial (113, 64%), allergy to medication (112, 64%) or pregnancy (78, 44%) were commonly excluded. Accepted parasitaemia ranges were reported as either inclusion in 137 (78%) studies or as exclusion criteria (i.e. values outside which a patient is not eligible) in 9 (5%) studies (Fig. 2).

Frequencies of inclusion and exclusion criteria reported in at least 25% of the 176 studies included in the final analysis. Criteria could be reported as inclusion (green) as well as exclusion (red), according to the publication. For example, accepted parasitaemia ranges could be reported either as range within which patients are eligible for inclusion or as cut-off values below or above which patients are excluded
Parasitaemia
All 176 studies specified the diagnostic method to confirm malaria; microscopy alone was the most common (104, 59% of studies); combinations of microscopy and Polymerase Chain Reaction (PCR) or Rapid Diagnostic Test (RDT) were used in 37 (21%) and 29 (16%) studies, respectively. A combination of microscopy, PCR and RDT were reported in 4 (2%) studies. RDT or PCR alone was reported in 1 study each (0.6%).
Parasitaemia inclusion ranges were described in 110/134 (82%), 15/23 (65%), 1/1 (100%) of the pure P. falciparum, P. vivax and P. knowlesi studies, respectively. Of the 110 P. falciparum studies, 50 (45%) had an upper limit of 200,000 asexual parasites/µl, and 22 (20%) had a range of 2000–200,000. Of the 15 P. vivax studies, 14 (93%) required having ≥ 250 asexual parasites/µl while 10/14 (71%) of mixed-infection studies included different parasitaemia ranges for the different Plasmodium species. Less frequently used criteria involve the presence of gametocytes (8/176 studies, 5.0%), and second malaria episode or symptomatic malaria (1/176, 0.6%).
Demographics
(i) One hundred thirty-three (76%) of the eligible studies were conducted in children ≥ 6 months old and above and/or adults; (ii) 17/% (30/176) enrolled only children between 0 and 5 years old; (iii) 21/176 (12%) enrolled only 6–59 month-old; (iv) 63/176 (36%) enrolled subjects ≥ 6 months with no upper age limit. A broad range of other ages was used with various frequencies in the reminding studies (Additional file 9).
Forty-nine (28%) trials included participants who weighed more than 5 kg, 46 of which with no upper weight limit. Two (1%) studies restricted the inclusion only to male participants.
Fever
Documentation of body temperature above a predefined cut-off temperature, typically 37.5 °C or 38 °C (Additional file 10), was reported in 113/176 (64%) of studies; 97/176 (55%) required both history of fever or current fever temperature above a predefined cut-off; 23/176 required history of fever or current fever alone.
Pregnancy
Twelve (7%) studies included pregnant women with a minimum gestational age of 12 weeks. None included women in the first trimester of pregnancy. Other reasons for exclusion associated with pregnancy were: lactation (48/176,) multiple pregnancies (4/176), women of reproductive age (3/176), previous history of complicated pregnancy (2/176) or abortion (2/176), planning pregnancy (1/176), missed menstrual cycle (1/176) or currently menstruating (1/176).
Concomitant illness
Patients with unspecified concomitant illness, severe malnutrition, or chronic underlying diseases were excluded in 71 (40%), 70 (40%), and 55 (31%) publications, respectively. 50/176 of the trials that excluded subjects with severe malnutrition were located in the WHO African region, and 14 (20%) were in the WHO South-East Asia Region, while 6 were located in the America, Eastern Mediterranean, or globally. 14/50 studies included the definition used for severe malnutrition: 6/14 defined a patient as severely malnourished when the weight for height falls below three standard deviations from the median of the WHO reference values, 6/14 as weight for height less than 70% of the median of WHO reference values, 1/14 reported both definitions, 1/14 defined patient malnourished when the weight for age < 60% and bilateral oedema was present. Thirty-four (49%) studies excluding severe malnutrition were in children < 15 years, 7/70 studies reported included patients aged above 15 years old, 24/70 did not include an upper age limit for enrolment, 5/70 did not define age limits for study inclusion. Other concomitant reasons for exclusion were: febrile illness other than malaria (55, 31%), heart impairment (30, 17%), current medication likely to interfere with therapy (21, 12%), history of convulsions (20, 11%), HIV infection (16, 9%), ECG abnormalities (9, 5%), previous history of splenectomy (9, 5%), recent blood transfusion (5, 3%), hepatitis (4, 2%), and sickle cell disease (4, 2%). One study specifically included patients who were only HIV positive. Further details on concomitant criteria are reported in Additional file 4.
Clinical reasons
Patients experiencing severe vomiting or diarrhoea (39, 22%), impaired consciousness (12, 7%), and inability to stand up or eat (9, 5%) were excluded in 39/176, 12/176 and 9/176 trials, respectively. Seven out of 176 studies mentioned G6PD minimum level as criteria for inclusion, three of which were on P. falciparum and four on P. vivax. Three (2%) studies excluded patients with G6PD minimum level, one (0.6%) on P. falciparum and two (1%) on P. vivax. Other unspecified clinical reasons, respiratory distress, and haemoglobinuria were also reported in 5/176, 2/176, and 1/176 trial(s), respectively.
Laboratory values and cut-off levels—Haematology
Minimum cut-off levels were reported for haemoglobin, packed cell volume (PCV), or haematocrit in 65 (37%), five (3%), and five (3%) of the studies, respectively. The haemoglobin cut-off level was used as a criterion for 51/134 (38%) of P. falciparum, and 7/23 (30%) P. vivax trials. The cut-off levels were: for haemoglobin < 5 g/dL in 23/55 (42%) trials, < 6 g/dL in 3/55 (6%), < 7 g/dL in 15/55 (27%), < 8 g/dL in 12/55 (22%) studies and < 10 g/dL and < 11 g/dL in one publication (2%) each. Ten studies did not report a cut-off for exclusion. For PCV < 20% in 4 studies, and < 25% in one study; for haematocrit < 25% in four and < 18% in one trial. Low platelets patients were excluded in one (0.6%) study, no cut-off for exclusion was defined in the publication.
Laboratory values and cut-off levels—Biochemistry
Thirty-six (20%) trials excluded subjects with hepatic impairment: 29 for P. falciparum, five for P. vivax, one for mixed infection, and one for P. knowlesi. 3/36 publications included a definition for hepatic impairment: either as alanine aminotransferase (ALT) concentration 2.5-fold above the upper limit of normal (1/3 studies) or more than twice the upper limit of normal (2/3). Thirty-six (20%) trials excluded subjects with renal impairment: 31 on P. falciparum, three on P. vivax, one on mixed infection, and one on P. knowlesi. Only one study defined renal impairment as creatinine level above 1.5 times the upper limit of normal. Abnormal creatine phosphokinase, glucose level and electrolyte imbalance were exclusion criteria in one (0.6%) study per criteria.
Operational reasons
Eleven percent (19/176) of the trials excluded patients participating in another research study. 14 (8%) studies excluded patients for operational reasons without reporting a more specific motive. Patients that were lost during the screening process, who had recently travelled beyond their hometown, or withdrawn were excluded in four (2%), one (0.6%), and one (0.6%) of the trials, respectively. Problems with mosquito husbandry (one, 0.6%) were also reported as exclusion criteria.
Other criteria
Non-descriptive criteria like ‘not specified’ were reported as the criteria in patients in 42 (24%) studies.
Reported reasons for exclusions of malaria-positive subjects
The 176 studies, which collectively screened 553,300 suspected malaria cases, identified as malaria-positive 157,516 (28%), of whom 56,293 (36%) were enrolled into the trial and treated, while 101,223 (64%) were excluded.
The reason for excluding those who tested positive for malaria was reported for 72,226/101,223 (71%). Three criteria account for 69.5% of exclusions: mixed-species malaria infections or other specific Plasmodium species (35.5%); parasite counts outside the set study ranges (20.5%); and refusal of consent (13.5%) (Table 3). The remaining studies did not specify reasons for exclusion, corresponding to 28,921 (29%) unaccounted exclusions.
Comparison of the baseline characteristics and planned eligibility criteria
Baseline demographics of the 176 studies were extracted from the study baseline demographics table, or the text when available. When presented in the paper, the baseline demographics were then compared with the study eligibility criteria range (Table 4).
Age
Of the 151 studies reporting age as an inclusion criterion, 60 (40%) reported both the eligible age and the actual baseline age range. Of those studies that reported both eligible and baseline age, 26 (43%) reported only a minimum age limit for inclusion in the study (no upper limit). One of those 60 studies enrolled one or more patient(s) aged below the defined cut-off. Four of the 60 studies included participants aged above the pre-defined ranges.
Parasitaemia
For this analysis, we separated the parasite counts by species as P. falciparum and P. vivax. Forty-five percent of studies (61/136) that reported parasitaemia inclusion ranges also reported actual baseline ranges: 52 (85%) of these were for P. falciparum (and mixed species including P. falciparum), 10 were for P. vivax and one for P. knowlesi. Of the 52 P. falciparum studies, 18 did not have an upper limit for inclusion. Of the 34 studies with an eligible parasite count range, 14 (41%) had a baseline parasitaemia range that fell outside the study eligible range, with eight of them enrolling patients with counts exceeding the maximum value allowed for inclusion in the study. Seven of the P. vivax studies which reported baseline parasitaemia ranges did not report an upper limit for study parasite count inclusion criteria. One of the P. vivax studies had a baseline parasitaemia range that fell outside the study inclusion criteria ranges.
Haemoglobin level
The range of haemoglobin cut-off minimum level for exclusion reported in the studies was from ≤ 11 g/dL to < 5 g/dL. In 10/176 (5%) of studies both a haemoglobin minimum cut-off level for exclusion and baseline haemoglobin range were reported, of which eight studies were for P. falciparum and two were on P. vivax. Four of those 10 studies enrolled one or more patient(s) with a haemoglobin level below the defined cut-off.
Other baseline characteristics collected are reported in Table 4.
Discussion
This is the first review to address the question of the representativeness of the patients enrolled in malaria treatment trials with respect to the spectrum of patients seen in clinical practice. This effort identified 176 studies conducted over the last two decades, screening over 150,000 patients from which both the eligibility criteria adopted and how these translated into patient selection could be extracted. About two-thirds of the malaria-positive subjects screened for enrolment are systematically excluded from anti-malarial treatment trials, and the reason for almost one-third of them was not reported.
This analysis points also to an even larger body of information which is currently not available, largely because basic reporting rules are not adhered to, leading to a substantial erosion of the mass of information potentially available. These 176 studies represent about one-fifth of the articles on the treatment of uncomplicated malaria which could have contributed to this analysis; however, it is unclear whether the desired information in the remaining approximately four-fifths of studies was not collected, not recorded, or simply not reported by the authors. Although this analysis was restricted to studies published after the CONSORT 2001 [12] statement, only just over half of the malaria clinical trials conducted between 2001 and 2021 (556/847) present the CONSORT flow diagram or an adaptation thereof, or produce similar information.
The study population from these trials consists of parasitological and non-parasitological confirmed uncomplicated malaria, either symptomatic or asymptomatic, across Plasmodium species of either mono- or mixed-infection. Severe malaria patients are generally excluded, either explicitly or by excluding parasite count levels defining more complicated malaria cases. This is also due to the eligibility criteria defined in the review which did not include studies investigating severe malaria patients. Studies also covered a broad age range, with more than one-fifth of the enrolled subjects being under five years of age.
The WHO guidelines [3], which aim to standardize the assessment of treatment efficacy primarily to monitor resistance in the most reproducible and consistent manner possible, require stringent eligibility criteria when measuring an outcome of interest, especially drug efficacy in terms of parasite and fever clearance in subjects with no or little immunity to help clear the parasites [21]. The current analysis identified 84 main criteria (17 inclusions, 75 exclusions, 8 reported in both sections) from the 176 studies assessed which generally complied with the guidelines, though to various degrees.
In the studies reporting the number of subjects excluded due to a specific reason, three criteria account for about 70% of exclusion of malaria-positive patients in studies, although some patients could have been excluded for not meeting more than one criterion. One set of reasons (more than half of exclusions) relates to parasitological diagnosis requiring microscopy—mixed or other infections and parasitaemia outside the established range.
As currently designed, anti-malarial efficacy trials do not provide information on how patients with higher parasitaemia and no obvious sign of severe malaria would respond to oral treatment, as well as participants with other concomitant diseases or other clinical reasons. Conversely, trials seem to cover adequately subjects with all degrees of anaemia except severe anaemia defined as haemoglobin < 5 g/dl. More detailed information on patients with high parasitaemia and/or severely anaemic would be desirable.
Some inconsistencies also emerged between the study criteria ranges or cut-off levels for eligibility and the related baseline characteristics of the recruited patients. Among the criteria analysed, temperature, parasitaemia and age ranges are poorly reported across the studies, although this inconsistency could be due to the timing at which the value is measured, with a variation in the value according to whether the measurement occurred at the screening or the baseline.
Limitations
The criteria were extracted and grouped according to how they were reported in the publications. As also demonstrated by the poor definition of some criteria (e.g., hepatic and renal impairment) or the difference in definitions detected (e.g., severe malnutrition), there is no standardized definition for each criteria reported, which will likely make the profile of the study populations heterogenous. The search strategy of this review did not include the grey literature and 12% of the peer-reviewed articles were excluded as they could not be accessed. Nonetheless, the sizable number of studies identified and number of participants give confidence in the evidence of knowledge gaps on the generalizability of malaria clinical trials. It is possible that some studies were missed, also considering that the update search was performed using only the WWARN Publication library [11], as the iterative approach used might have created some discrepancy in the search methods used. While it was not possible to report separately on phase II, III or IV studies as this information was not provided systematically, it is reasonable to assume that they were mostly “phase IV-type” studies as they tested therapies in routine use; phase II or III aimed at supporting drug registrations were clearly identified and limited in numbers.
Accurate reporting is essential. The CONSORT [10] statement offers a useful framework for improving the transparency of clinical trials, including adequate reporting of the eligibility criteria and patient attrition. Papers should report details on the reasons for excluding subjects against the pre-established eligibility criteria; trial screening logs could be an important source of information. Recording and sharing this information would allow a better profiling of the patients seen in routine practice and a better understanding of the representativeness of the body of evidence from clinical trials. A number of tools have been made available to the research community and should be further disseminated to improve the quality of anti-malarial efficacy trials and their reporting [22, 23].
Conclusion
Research findings are summarized in Box 5. The studies identified generally adhere to the WHO standards, which are important for assessing drug efficacy in a consistent way [3]. At the same time, pragmatic (effectiveness) trials are clearly lacking, and these too are important, as they would provide critical, generalizable information on patient groups who are systematically excluded from efficacy trials but are routinely seen and treated. The purpose of such evaluation is different, and the selection criteria established for monitoring resistance applied may limit the external validity of results for the general population and the conditions in which treatments are delivered in practice.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its Additional files.
Abbreviations
- WWARN:
-
WorldWide antimalarial resistance network
- WHO:
-
World Health Organization
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses extension
- MESH:
-
Medical subject headings
- CONSORT:
-
Consolidated standards of reporting trials
- RCT:
-
Randomized controlled trial
- PCR:
-
Polymerase chain reaction
- RDT:
-
Rapid diagnostic test
- G6PD:
-
Glucose-6-Phosphate dehydrogenase
- PCV:
-
Packed cell volume
References
WHO. World malaria report 2021. Geneva: World Health Organization; 2021.
WHO. Guidelines for malaria. Geneva: World Health Organization; 2021.
Van Spall HG, Toren A, Kiss A, Fowler RA. Eligibility criteria of randomized controlled trials published in high-impact general medical journals: a systematic sampling review. JAMA. 2007;297:1233–40.
Dekkers OM, von Elm E, Algra A, Romijn JA, Vandenbroucke JP. How to assess the external validity of therapeutic trials: a conceptual approach. Int J Epidemiol. 2010;39:89–94.
Nsanzabana C, Djalle D, Guérin PJ, Ménard D, González IJ. Tools for surveillance of anti-malarial drug resistance: an assessment of the current landscape. Malar J. 2018;17:75.
WHO. Method for surveillance of antimalarial drug efficacy. Geneva: World Health Organization; 2009.
Bassat Q, González R, Machevo S, Nahum A, Lyimo J, Maiga H, et al. Similar efficacy and safety of artemether-lumefantrine (Coartem®) in African infants and children with uncomplicated falciparum malaria across different body weight ranges. Malar J. 2011;10:369.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009. https://doi.org/10.1136/bmj.b2535.
Worldwide Antimalarial Resistance Network. WWARN Clinical Trials Publication Library. 2021. https://www.wwarn.org/tools-resources/literature-reviews/wwarn-clinical-trials-publication-library. Accessed 28 Mar 2021
Schulz KF, Altman DG, Moher D, CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomized trials. Ann Intern Med. 2010;152:726–32.
Takata J, Sondo P, Humphreys GS, Burrow R, Maguire B, Hossain MS, et al. The worldwide antimalarial resistance network clinical trials publication library: a live, open-access database of plasmodium treatment efficacy trials. Am J Trop Med Hyg. 2020;103:359–68.
Moher D, Schulz KF, Altman DG. The CONSORT statement: revised recommendations for improving the quality of reports of parallel group randomized trials. BMC Med Res Methodol. 2001;1:2.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2010;42:377–81.
Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, Neal LO, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208.
WHO. Assessment of therapeutic efficacy. Geneva: World Health Organization; 1996.
WHO. Monitoring antimalarial drug resistance. Geneva: World Health Organization; 2002.
WHO. Assessment and monitoring of antimalarial drug efficacy for the treatment of uncomplicated Falciparum Malaria. Geneva: World Health Organization; 2003.
Sutherland CJ, Drakeley CJ, Obisike U, Coleman R, Jawara M, Targett GAT, et al. The addition of artesunate to chloroquine for treatment of Plasmodium falciparum malaria in Gambian children delays, but does not prevent treatment failure. Am J Trop Med Hyg. 2003;69:19–25.
Valecha N, Phyo AP, Mayxay M, Newton PN, Krudsood S, Keomany S, et al. An open-label, randomised study of dihydroartemisinin-piperaquine versus artesunate-mefloquine for falciparum malaria in Asia. PLoS ONE. 2010. https://doi.org/10.1371/journal.pone.0011880.
Secretaria de Salud de Honduras. Norma de Malaria en Honduras. Secretaria de Salud SdRP, Direccion General de Promocion de la Salud, Programa Nacional de la Prevencion y Control de la Malaria. Tegucigalpa, Honduras: Secretaria de Salud de Honduras, 2010.
Allen EN, Chandler CIR, Mandimika N, Pace C, Mehta U, Barnes KI. Evaluating harm associated with anti-malarial drugs: a survey of methods used by clinical researchers to elicit, assess and record participant-reported adverse events and related data. Malar J. 2013;12:325.
Worldwide Antimalarial Resistance Network. Malaria Clinical Trials Toolkit. https://www.wwarn.org/tools-resources/malaria-clinical-trials-toolkit. Accessed 28 Mar 2022
Global Health Trial Network. Global Drug Trials. https://globaldrugdevelopment.tghn.org/ Accessed 28 Mar 2022
Acknowledgements
We would like to thank our colleagues at the Special Programme for Research and Training in Tropical Diseases (TDR) at the World Health Organization Dr John Reeder, Dr Annette Kuesel, and Dr Corinne Merle for their informative discussions on the evidence. We would like to thank our colleagues from the University of Oxford, Dr Prabin Dahal and Dr Eric Ohuma for their support with the descriptive summary statistics. Ms Ekua Johnson for her support during the research.
Funding
This investigation received financial support from the Special Programme for Research and Training in Tropical Disease (TDR) World Health Organization (WHO), Geneva, Switzerland, and the MSc in International Health and Tropical Medicine, Centre for Tropical Medicine and Global Health, University of Oxford, UK.
Author information
Authors and Affiliations
Contributions
Conceptualization: Piero L. Olliaro, Data curation: Mazvita Zanamwe, Christine M. Halleux, Piero L. Olliaro, Lorenzo Arena, Verena Carrara, Formal analysis: Mazvita Zanamwe, Christine M. Halleux, Piero L. Olliaro, Lorenzo Arena, Kasia Stepniewska, Methodology: Piero L. Olliaro, Mazvita Zanamwe, Christine M. Halleux, Lorenzo Arena, Kasia Stepniewska, Supervision: Piero L. Olliaro, Brian J. Angus, Christine M. Halleux, Philippe J. Guérin, Writing of original draft: Piero L. Olliaro, Mazvita Zanamwe, Christine M. Halleux, Lorenzo Arena, Verena Carrara, Caitlin Richmond, Kasia Stepniewska, Philippe J. Guérin, Editing: Piero L. Olliaro, Mazvita Zanamwe, Christine M. Halleux, Brian J. Angus, Proochista Ariana, Georgina S. Humphreys, Philippe J. Guérin. All authors read and approved the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
We have read the journal’s policy and the authors of this manuscript have the following competing interests: Christine M. Halleux is a staff member of the World Health Organization (WHO) and Piero L. Olliaro was also a staff member of WHO during part of this work; the authors alone are responsible for the views expressed in this publication and they do not necessarily represent the decisions, policy or views of the WHO. The designations used and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area, or of its authorities, nor concerning the delimitation of its frontiers or boundaries.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 5.
Reasons for exclusion summary analysis.
Additional file 6.
Details of 176 articles included in the final assessment.
Additional file 7.
Data items, baseline demographics, and subgroup narrative analysis details.
Additional file 8.
Yearly and cumulative number of studies by Plasmodium species between 2001-2021 for 176 studies.
Additional file 9.
Age ranges distributions across the studies reporting Age as inclusion criteria.
Additional file 10.
Temperature (°C) minimum requirement for enrolment across the studies reporting Temperature as inclusion criteria.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Arena, L., Zanamwe, M., Halleux, C.M. et al. Malaria patient spectrum representation in therapeutic clinical trials of uncomplicated malaria: a scoping review of the literature. Malar J 22, 50 (2023). https://doi.org/10.1186/s12936-023-04441-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-023-04441-5