
Abstract
Background
Gestational diabetes mellitus (GDM) is a common complication of pregnancy, with significant short-term and long-term implications for both mothers and their offspring. Previous studies have indicated the potential benefits of vitamin D in reducing the risk of GDM, yet little is known about this association in twin pregnancies. This study aimed to investigate maternal vitamin D status in the second trimester and examine its association with the risk of GDM in twin pregnancies.
Methods
We conducted a prospective cohort study based on data from the Chongqing Longitudinal Twin Study (LoTiS). Peripheral blood serum was collected from the mothers in the second trimester to measure 25(OH)D concentrations. GDM was diagnosed at 23–26 weeks of gestation using a 75-g 2-h oral glucose tolerance test. We used multivariable logistic regression analyses to examine the correlations between vitamin D status and the risk of GDM.
Results
Of the total participants, 93 (29.9%) women were diagnosed with GDM. The mean serum 25(OH)D concentration in the second trimester was 31.1 ± 11.2 ng/mL, and the rate of vitamin D insufficiency and deficiency were 23.5% and 18.7%, respectively. Compared to women with a 25(OH)D concentration < 30 ng/mL, those with a 25(OH)D concentration ≥ 30 ng/mL had a significantly lower risk of GDM (RR 0.61; 95% CI: 0.43, 0.86), especially those who were overweight before pregnancy (RR 0.32; 95% CI: 0.16, 0.64). The restricted cubic splines model showed an inverted J-shaped relationship between vitamin D concentrations and GDM risk.
Conclusions
The risk of GDM was significantly reduced in twin pregnant women with vitamin D concentrations ≥ 30 ng/mL in the second trimester.
Trial registration
ChiCTR-OOC-16,008,203. Retrospectively registered on 1 April 2016.
Similar content being viewed by others
Background
Gestational diabetes mellitus (GDM) is defined as diabetes diagnosed in the second or third trimester of pregnancy in women who did not have clearly overt diabetes prior to gestation according to the American Diabetes Association (ADA) [1]. GDM is one of the most common pregnancy complications and exhibits varying prevalence rates ranging from 7.1% to 27.6% worldwide according to country, ethnicity and diagnostic thresholds [2]. The prevalence of GDM among the Chinese population ranges from 17.5% to 18.9% [3], while in Europe and North America, the prevalence is lower, at 7.1-7.8% [2]. GDM has been found to have short- and long-term adverse effects on both mothers and their offspring, including an increased risk of hypertensive diseases of pregnancy, cesarean deliveries and macrosomia at birth during the perinatal period, as well as a higher risk of type 2 diabetes in mothers and metabolic complications in offspring later in life [4].
Given the potential negative effects of GDM, it is crucial to identify the risk factors associated with its development. Accumulative studies have reported an association between vitamin D status and GDM prevalence [5, 6], with vitamin D deficiency being linked to an increased risk of developing GDM [7,8,9]. Nevertheless, it is noteworthy that all the aforementioned studies have focused primarily on singleton pregnancies, and there is a lack of comprehensive exploration of vitamin D concentrations and status in twin pregnancies and their association with the development of GDM.
With the development of assisted reproductive technology and delayed childbearing, the rate of twin births has exceeded 3% [10]. When the same diagnostic criteria are used to diagnose GDM, twin pregnancies are found to have a higher prevalence of GDM than singleton pregnancies in the same geographical region [11,12,13]. This may be attributed to older age, larger placental areas and greater gestational weight gain in twin pregnant women [14]. However, studies on the impact of GDM on perinatal outcomes in twin pregnancies have reported conflicting results. Studies conducted in North America revealed that GDM is associated with an increased risk of cesarean section, preterm delivery and large-for-gestational age (LGA) neonates in twin pregnancies [15,16,17,18]. However, Lin et al. reported that the perinatal outcomes of women with twin pregnancies with GDM are comparable to those without GDM in a Chinese population [19]. In our previous prospective investigation, we found that twin pregnancies with GDM are related to an elevated risk of gestational hypertension, childhood overweight at 6 months [20] and preterm delivery [21]. This suggests that GDM may affect the health of both twin pregnant women and their offspring. Therefore, it is worth exploring whether there is a correlation between vitamin D status and the occurrence of GDM in twin pregnancies.
The aim of the present study was to investigate the vitamin D concentrations and status in the second trimester and to examine their associations with the development of GDM in twin pregnancies. To achieve this goal, we utilized a longitudinal birth cohort of twin pregnancies from Southwest China.
Methods
Study design and participants
This study was conducted as part of the Chongqing Longitudinal Twin Study (LoTiS), which is an ongoing prospective study conducted at the First Affiliated Hospital of Chongqing Medical University and Chongqing Health Center for Women and Children in China [22]. Chongqing is located in southwestern China at a latitude of 29.35° N and has a humid subtropical monsoon climate with insufficient sunshine (1000–1400 h per year). The LoTiS study recruited twin pregnant women aged 20–40 years who began receiving prenatal care at 11–16 weeks of gestation in the study centers. The twin birth cohort was launched in January 2016; by February 2019, a total of 439 women were recruited at the first visit, and 333 women had completed all the required visits during the pregnancy period. The study was approved by the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University (No. 201530). All the methods and procedures carried out in this study were in accordance with the principles of the Declaration of Helsinki as revised in 2008. Written informed consent was obtained from each participant at recruitment.
In the current study, women were eligible for inclusion if they had peripheral blood samples collected in the second trimester, underwent a 75-g oral glucose-tolerance test (OGTT) between 23 and 26 weeks of gestation, and had complete pregnancy records. Women with any of the following conditions were excluded from the study: preexisting chronic metabolic diseases, such as hypertension or type 2 diabetes; fetal complicated with severe malformation and complications, such as twin-to-twin transfusion syndrome and intrauterine death of one or both fetuses.
Vitamin D measurement
Peripheral blood samples were collected from mothers in the second trimester (23–26 weeks of gestation) by using a coagulation-promoting blood collection tube. Serum samples were centrifuged for 10 min at 4℃ and 3000 rpm, and transferred to -80 ℃ freezers within 3 h for long-term storage. Serum 25(OH)D3 and 25(OH)D2 concentrations were measured by high-performance liquid chromatography- electrospray tandem mass spectrometry (HPLC-MS/MS, Waters, USA), which is the gold standard measurement method. The intra-assay and inter-assay coefficients of variation were < 15%, indicating good repeatability.
The concentration of 25(OH)D was calculated by summing the concentrations of 25(OH)D3 and 25(OH)D2. The women were categorized into three 25(OH)D status groups according to the Endocrine Society guidelines: 25(OH)D concentrations below 20 ng/mL were classified as deficient, concentrations ranging from 20 to 30 ng/mL were considered insufficient, and concentrations above 30 ng/mL were considered sufficient [23].
Diagnosis of GDM
GDM was diagnosed after the 75 g 2-h OGTT if ≥ 1 of the following plasma glucose values was met or exceeded according to the International Association of Diabetes and Pregnancy Study Group (IADPSG): a fasting plasma glucose (FPG) level ≥ 5.1 mmol/L, a 1-h plasma glucose (PG-1 h) level ≥ 10.0 mmol/L, or a 2-h plasma glucose (PG-2 h) level ≥ 8.5 mmol/L [24].
Data collection
We collected data on maternal age (< 35 y, ≥ 35 y), height, prepregnancy weight, weight at 12 weeks, weight at 24 weeks, education level (≤ 12 y, > 12 y), employment status (employed, unemployed), smoking status before pregnancy, chorionicity (monochorionic, dichorionic), mode of conception (naturally conceived, conceived by assisted reproductive technology), parity (0, ≥ 1), family history of diabetes, gestational age and season of blood sample collection (summer/autumn, winter/spring). Prepregnancy BMI (kg/m2) was calculated as the ratio of weight (kg) to squared height (m2) (< 24 and ≥ 24 kg/m2), which was derived from self-reported prepregnancy weight and measured height at the first visit.
Statistical analysis
Continuous variables are expressed as the means and standard deviations and were analyzed using Student’s t test or one-way analysis of variance. Categorical variables are expressed as count and percentage and were analyzed using the chi-squared test or Fisher’s exact test. Multivariate logistic regression models were utilized to estimate the relative ratio (RR) and 95% confidence interval (CI) for GDM risk related to vitamin D status. Adjusted confounders included maternal age, prepregnancy BMI, education level, employment status, parity, mode of conception and family history of diabetes. Additionally, we employed a restricted cubic spline (RCS) regression model to further examine the nonlinear association between vitamin D concentrations and GDM risk.
All the statistical analyses were conducted in Stata 15.0 (StataCorp, College Station, TX, USA).
Results
Characteristics of the participants according to GDM status
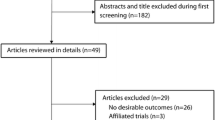
After exclusions of twin pregnancies due to the death of one or both twins, complicated with severe fetal malformation and complications, preexisting hypertension/type 2 diabetes, lost to follow-up and missing peripheral blood samples, a total of 311 twin pregnant women were included in the current study (Fig. 1). Among them, 93 (29.9%) were diagnosed with GDM (Fig. 1).

Flowchart showing selection of participants included in this analysis from LoTiS study
Table 1 presents the participant characteristics according to GDM status. Overall, compared to women uncomplicated with GDM, women complicated with GDM tended to be older (30.0 ± 3.9 vs. 29.0 ± 3.9, p = 0.031) and were more likely to have a BMI higher than 24.0 kg/m2 before pregnancy (26.9% vs. 17.0%, p = 0.045). There were no significant differences between the GDM and non-GDM groups in terms of education level, employment status, primipara, mode of conception, chorionicity, smoking status before pregnancy, family history of diabetes and season of sampling. Importantly, women complicated with GDM had significantly lower concentrations of 25(OH)D and a lower proportion of vitamin D sufficiency than women uncomplicated with GDM (27.8 ± 9.9 vs. 32.5 ± 11.4, p < 0.001; 44.1% vs. 63.8%, p = 0.002). The distribution of serum 25(OH)D concentrations between the two groups is presented in Fig. 2.

Comparison of vitamin D concentrations between women complicated with GDM and without GDM. (***) represents p < 0.001
Comparisons of vitamin D concentrations in the second trimester according to the maternal characteristics
As shown in Table 2, the average concentration of 25(OH)D in the second trimester was 31.1 ± 11.2 ng/mL, with vitamin D sufficiency present in 57.9% of mothers, vitamin D insufficiency in 23.5% and vitamin D deficiency in 18.7%. A significant difference in the mean 25(OH)D concentration was observed among twin pregnant women with different modes of conception. Women who conceived with the aid of assisted reproductive technology had a lower mean 25(OH)D concentration (29.3 ± 10.9 vs. 32.2 ± 11.3, p = 0.030). There were no significant differences in the mean 25(OH)D concentration between the other maternal characteristics and the season of sampling.
Association between vitamin D status and the risk of GDM
The multivariate regression analyses performed to determine the association between vitamin D status in the second trimester and the risk of GDM are summarized in Table 3. Compared to women with vitamin D sufficiency, women with vitamin D insufficiency had a higher risk of developing GDM (RR 1.98; 95% CI: 1.37, 2.87; p < 0.001). After adjusting for maternal age, prepregnancy BMI, education level, employment status, parity, mode of conception and family history of diabetes, the association between vitamin D insufficiency and GDM risk remained significant (RR 1.85; 95% CI: 1.28, 2.67; p = 0.001). Women with vitamin D deficiency did not have an increased risk of GDM according to either the unadjusted or the adjusted model.
In the subgroup analysis, a significant increase in GDM risk was observed in both the vitamin D insufficiency group (RR 3.55; 95% CI: 1.75, 7.20; p = 0.001) and vitamin D deficiency group (RR 2.38; 95% CI: 1.03, 5.53; p = 0.043) among overweight women compared to the vitamin D sufficiency group after adjustments were made for confounding factors (Table 3). Age did not modify the association between vitamin D insufficiency and GDM risk, as increased GDM risks were observed in both the vitamin D insufficiency group among both twin pregnant women aged ≥ 35 years (RR 2.88; 95% CI: 1.25, 6.61; p = 0.013) and those aged < 35 years (RR 1.67; 95% CI: 1.09, 2.56; p = 0.018) after adjusting for confounding factors (Table 3).
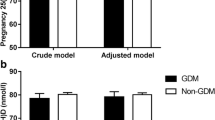
Furthermore, we examined the association of vitamin D sufficiency with the incidence of GDM (Fig. 3). Women with vitamin D concentrations ≥ 30 ng/mL had a reduced risk of developing GDM compared to those with vitamin D concentrations < 30 ng/mL (RR 0.61; 95% CI: 0.43, 0.86; p = 0.005) after adjusting for potential confounding factors. The effect modification by prepregnancy BMI remained significant, as overweight women with sufficient vitamin D had a reduced risk of GDM (RR 0.32; 95% CI: 0.16, 0.64; p = 0.001).

Associations between vitamin D levels and the risk of GDM, and stratified by pre-pregnancy body mass index levels (< 24.0 vs. ≥ 24.0) and age (< 35 vs. ≥ 354.0). Adjusted for maternal age, prepregnancy BMI, education level, occupation, parity, mode of conception and family history of diabetes. (●) represents vitamin D concentrations < 30 ng/mL; (■) representsvitamin D concentrations ≥ 30 ng/mL
Associations between vitamin D concentrations and the risk of GDM
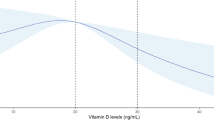
The RCS model showed an inverted J-shaped association between vitamin D concentrations and the risk of GDM. This association was observed after adjusting for maternal age, prepregnancy BMI, education level, employment status, parity, mode of conception and family history of diabetes (Fig. 4). Break-point analysis showed that the knot of the steep downward trend was 30 ng/mL. There was no significant association between vitamin D concentration and GDM when the 25(OH)D concentration was < 30 ng/mL, while the risk of GDM decreased when the 25(OH)D concentration was ≥ 30 ng/mL.

Nonlinear association between vitamin D levels in the second trimester and GDM risk by restricted cubic spline curve, maternal age, prepregnancy BMI, education level, occupation, parity, mode of conception and family history of diabetes were adjusted. A vitamin D concentration of 20 ng/mL was selected as the reference level. The area between dashed lines represents 95% CIs. Knots were located at the 5th, 35th, 65th and 95th percentiles
Discussion
In the current cohort study, the results demonstrated that the average concentration of 25(OH)D in the second trimester among twin pregnant women was 31.1 ± 11.2 ng/mL, and 57.9%, 23.5% and 18.7% of women had sufficient, insufficient and deficient vitamin D levels, respectively. A nonlinear association between vitamin D concentrations and the incidence of GDM was observed. A vitamin D concentration above 30 ng/mL in the second trimester was found to be a protective factor against the development of GDM. This protective effect was more pronounced in twin pregnant women who were overweight prior to pregnancy.
Vitamin D deficiency is a prevalent public health issue, particularly among pregnant women. In our study, the average concentration of vitamin D in twin pregnant women in the second trimester was 31.1 ng/mL, which was higher than that observed in singleton pregnant women in China during the same trimester [25,26,27]. This difference may be attributed to the fact that twin pregnancies are widely recognized as high-risk pregnancies in clinical practice, leading to better compliance among twin pregnant women with prenatal health management recommendations, such as more frequent ultrasound examinations and nutritional supplementation. However, we observed that twin pregnant women who conceived with the assistance of assisted reproductive technology had lower vitamin D concentrations compare to women who conceived naturally. This may be due to the health issues commonly associated with women undergoing assisted reproductive technology, such as infertility or hormonal imbalances, traumatic procedures like embryo transfer, and the use of additional medications. These factors may impact the absorption and metabolism of vitamin D. Individual variations in vitamin D supplementation may also contribute to the observed differences.
Extensive research has been conducted on the association between vitamin D levels and the occurrence of GDM in singleton pregnancies. There are conflicting reports exist regarding the association between vitamin D levels during early pregnancy and the development of GDM. Some studies have figured out that vitamin D deficiency during early pregnancy is associated with an increased risk of GDM [7, 8, 28,29,30], while other studies have not supported this association [31,32,33]. A systematic review and meta‑analysis consisting of 37,838 pregnant women concluded that lower levels of vitamin D in early pregnancy were associated with a higher risk of developing GDM. However, in some of the included studies, vitamin D concentrations were measured in the second trimester, which limits the applicability of the findings [5]. In terms of the correlation between second trimester vitamin D levels and the occurrence of GDM, eighteen studies utilized a prospective cohort or nested case-control study design to measure vitamin D levels at 24–28 weeks of gestation. Among these studies, eleven studies reported a positive association between vitamin D deficiency and GDM risk [5, 6]. These varying results may be attributed to several factors, such as the study design, sample size, methods used to determine vitamin D levels, region and latitude. For instance, most nested case-control investigations concluded a positive association between vitamin D deficiency and higher risk of GDM. Four studies conducted on Chinese women have consistently reported an association between vitamin D levels in the second trimester and GDM risk [25,26,27, 34]. Hence, we assessed the vitamin D concentration in twin pregnant women in the second trimester and investigated its association with GDM.
In the current study, we discovered that vitamin D insufficiency in the second trimester was associated with an elevated risk of GDM. This association was more pronounced among overweight women, which aligns with the findings of a previous study that reported a stronger association between vitamin D and GDM risk among overweight/obese women [26]. However, we did not observe a connection between vitamin D deficiency in the second trimester and a higher risk of GDM. Therefore, we speculated that there might be a nonlinear relationship between vitamin D concentrations and GDM risk. Previous studies have shown that GDM risk was significantly reduced among pregnant women with vitamin D concentrations ≥ 20 ng/mL [25, 28], or decreased among those with vitamin D concentrations > 35 ng/mL [35], or decreased among those with vitamin D concentrations 25–40 ng/mL [32] in singleton pregnancies, suggesting the existence of a threshold concentration for vitamin D that determines the significance of its association with GDM risk. In our study, nonlinear association analysis revealed an inverted J-shaped relationship between vitamin D concentrations and the risk of GDM. A vitamin D level of 30 ng/mL was identified as the threshold that significantly reduced the risk of GDM in twin pregnant women. The variations in the identified thresholds of vitamin D, which affect GDM risk, across different studies may be ascribed to inconsistent population characteristics, diagnostic criteria for GDM and timing of vitamin D measurement.
Several biological mechanisms have been proposed to elucidate the role of vitamin D in regulating glucose metabolism. First, vitamin D may enhance the peripheral/hepatic uptake of glucose, which can help decrease glucose levels [36]. Second, vitamin D deficiency may impair pancreatic β-cell functions, thereby compromising the secretion of insulin [37]. Third, vitamin D plays a role in immune system regulation. It has been suggested that dysregulation of the immune system during pregnancy may contribute to the development of GDM, and vitamin D may help modulate immune responses and promote a balanced immune system, potentially reducing the risk of GDM. Finally, vitamin D deficiency can exacerbate inflammation and oxidative stress in the pancreas and other organs, leading to insulin resistance [37]. Compared to singleton pregnant women with GDM, twin pregnant women with GDM are more likely to have abnormal postprandial blood glucose levels, which is more likely attribute to insulin resistance than impaired pancreatic islet β cell function [21, 38,39,40]. Thus, higher vitamin D concentrations are significant for alleviating insulin resistance and reducing the risk of GDM in twin pregnant women. This also explains why the threshold of vitamin D, which can affect the incidence of GDM, is higher in twin pregnancies than in singleton pregnancies in the Chinese population under the same diagnostic criteria for GDM [25].
The strength of our study lies in the specific study population. To our knowledge, this was the first study to investigate the association between vitamin D status and the risk of GDM in a population of women with twin pregnancies. However, there are several limitations that should be considered in this study. One limitation was the single-center study design of this study, which limits the generalizability of the findings. Another limitation was the lack of accurate data on vitamin D supplementation during the second trimester. The questionnaire used to assess vitamin D supplementation frequency had only two options: “daily” and “sometimes or less frequently”. Further detailed investigations are needed to understand the associations among vitamin D supplementation, vitamin D absorption, and the causal mechanism underlying the relationship between vitamin D supplementation and GDM. Finally, the lack of certain biological indicators related to GDM, such as glycosylated hemoglobin and insulin, limits our ability to fully explain the effect of vitamin D on GDM.
Conclusions
In twin pregnant women with vitamin D concentrations < 30 ng/mL in the second trimester, the risk of GDM was significantly reduced in those with vitamin D levels ≥ 30 ng/mL in the second trimester. There was a nonlinear association between vitamin D concentrations and the incidence of GDM, with 30 ng/mL considered as the cutoff for the vitamin D concentration that could significantly reduce the risk of GDM in twin pregnancies. Further multicenter research is needed to provide more evidence elucidating the relationship between vitamin D and GDM in twin pregnancies.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon request.
Abbreviations
- ADA:
-
America Diabetes Association
- ART:
-
assistant reproductive technology
- BMI:
-
body mass index
- CI:
-
confidence interval
- GDM:
-
gestational diabetes mellitus
- IADPSG:
-
International Association of Diabetes and Pregnancy Study Groups
- LGA:
-
large-for-gestational age
- LoTiS:
-
Longitudinal Twin Study
- OGTT:
-
oral glucose tolerance test
- RCS:
-
restricted cubic spline
- RR:
-
relative ratio
References
American Diabetes A. 2. Classification and diagnosis of diabetes: standards of Medical Care in Diabetes-2021. Diabetes Care. 2021;44:S15–33.
Wang H, Li N, Chivese T, Werfalli M, Sun H, Yuen L, Hoegfeldt CA, Elise Powe C, Immanuel J, Karuranga S, et al. IDF Diabetes Atlas: estimation of Global and Regional Gestational Diabetes Mellitus Prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group’s Criteria. Diabetes Res Clin Pract. 2022;183:109050.
Zhu WW, Fan L, Yang HX, Kong LY, Su SP, Wang ZL, Hu YL, Zhang MH, Sun LZ, Mi Y, et al. Fasting plasma glucose at 24–28 weeks to screen for gestational diabetes mellitus: new evidence from China. Diabetes Care. 2013;36:2038–40.
Coustan DR, Lowe LP, Metzger BE, Dyer AR. International Association of D, pregnancy study G: the hyperglycemia and adverse pregnancy outcome (HAPO) study: paving the way for new diagnostic criteria for gestational diabetes mellitus. Am J Obstet Gynecol. 2010;202:e654651–656.
Fatima K, Asif M, Nihal K, Hussain HU, Hasan AW, Zahid M, Burney MH, Asad F, Fatima S, Saleem MB, Khalid MA. Association between vitamin D levels in early pregnancy and gestational diabetes mellitus: a systematic review and meta-analysis. J Family Med Prim Care. 2022;11:5569–80.
Milajerdi A, Abbasi F, Mousavi SM, Esmaillzadeh A. Maternal vitamin D status and risk of gestational diabetes mellitus: a systematic review and meta-analysis of prospective cohort studies. Clin Nutr. 2021;40:2576–86.
Shang M, Zhao N. Early pregnancy vitamin D insufficiency and gestational diabetes mellitus. J Obstet Gynaecol Res. 2022;48:2353–62.
Aslan Cin NN, Yalcin M, Yardimci H. Vitamin D Deficiency during the first trimester of pregnancy and the risk of developing gestational diabetes Mellitus. J Obstet Gynecol Neonatal Nurs. 2022;51:526–35.
Xia J, Song Y, Rawal S, Wu J, Hinkle SN, Tsai MY, Zhang C. Vitamin D status during pregnancy and the risk of gestational diabetes mellitus: a longitudinal study in a multiracial cohort. Diabetes Obes Metab. 2019;21:1895–905.
Chen P, Li M, Mu Y, Wang Y, Liu Z, Li Q, Li X, Dai L, Xie Y, Liang J, Zhu J. Temporal trends and adverse perinatal outcomes of twin pregnancies at differing gestational ages: an observational study from China between 2012–2020. BMC Pregnancy Childbirth. 2022;22:467.
Ashwal E, Berger H, Hiersch L, Yoon EW, Zaltz A, Shah B, Halperin I, Barrett J, Melamed N. Gestational diabetes and fetal growth in twin compared with singleton pregnancies. Am J Obstet Gynecol. 2021;225:420. e421-420 e413.
Lai FY, Johnson JA, Dover D, Kaul P. Outcomes of singleton and twin pregnancies complicated by pre-existing diabetes and gestational diabetes: a population-based study in Alberta, Canada, 2005-11. J Diabetes. 2016;8:45–55.
Luo ZC, Simonet F, Wei SQ, Xu H, Rey E, Fraser WD. Diabetes in pregnancy may differentially affect neonatal outcomes for twins and singletons. Diabet Med. 2011;28:1068–73.
Simoes T, Queiros A, Correia L, Rocha T, Dias E, Blickstein I. Gestational diabetes mellitus complicating twin pregnancies. J Perinat Med. 2011;39:437–40.
Hiersch L, Berger H, Okby R, Ray JG, Geary M, McDonald SD, Murray-Davis B, Riddell C, Halperin I, Hasan H, et al. Gestational diabetes mellitus is associated with adverse outcomes in twin pregnancies. Am J Obstet Gynecol. 2019;220:102. e101-102 e108.
Dave ED, Bodnar LM, Vani K, Himes KP. Perinatal outcomes in twin pregnancies complicated by gestational diabetes. Am J Obstet Gynecol MFM. 2021;3:100396.
Alkaabi J, Almazrouei R, Zoubeidi T, Alkaabi FM, Alkendi FR, Almiri AE, Sharma C, Souid AK, Ali N, Ahmed LA. Burden, associated risk factors and adverse outcomes of gestational diabetes mellitus in twin pregnancies in Al Ain, UAE. BMC Pregnancy Childbirth. 2020;20:612.
Tward C, Barrett J, Berger H, Kibel M, Pittini A, Halperin I, Cohen H, Melamed N. Does gestational diabetes affect fetal growth and pregnancy outcome in twin pregnancies? Am J Obstet Gynecol. 2016;214:e653651–658.
Lin D, Fan D, Li P, Chen G, Rao J, Zhou Z, Zhang H, Luo X, Ma H, Feng J, et al. Perinatal outcomes among twin pregnancies with gestational diabetes mellitus: a nine-year retrospective cohort study. Front Public Health. 2022;10:946186.
Mei Y, Yu J, Wen L, Fan X, Zhao Y, Li J, Qiao J, Fu H, Leong P, Saffery R, et al. Perinatal outcomes and offspring growth profiles in twin pregnancies complicated by gestational diabetes mellitus: a longitudinal cohort study. Diabetes Res Clin Pract. 2021;171:108623.
Wen L, Chen Y, Liu T, Wang Y, Baker PN, Qi H, Wang L. Different subtypes of gestational diabetes mellitus are associated with distinct perinatal outcomes in twin pregnancies. Diabetes Res Clin Pract. 2023;204:110920.
Tong C, Wen L, Wang L, Fan X, Zhao Y, Liu Y, Wang X, Huang S, Li J, Li J et al. Cohort Profile: the Chongqing Longitudinal Twin Study (LoTiS). Int J Epidemiol 2022.
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, Murad MH, Weaver CM, Endocrine S. Evaluation, treatment, and prevention of vitamin D deficiency: an endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911–30.
International Association of D, Pregnancy Study Groups, Consensus P, Metzger BE, Gabbe SG, Persson B, Buchanan TA, Catalano PA, Damm P, Dyer AR, Leiva A, et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33:676–82.
Yin WJ, Tao RX, Hu HL, Zhang Y, Jiang XM, Zhang MX, Jin D, Yao MN, Tao FB, Zhu P. The association of vitamin D status and supplementation during pregnancy with gestational diabetes mellitus: a Chinese prospective birth cohort study. Am J Clin Nutr. 2020;111:122–30.
Shao B, Mo M, Xin X, Jiang W, Wu J, Huang M, Wang S, Muyiduli X, Si S, Shen Y, et al. The interaction between prepregnancy BMI and gestational vitamin D deficiency on the risk of gestational diabetes mellitus subtypes with elevated fasting blood glucose. Clin Nutr. 2020;39:2265–73.
Wang L, Yu T, Jiao R, Fan X, Wang Y, Liu W, Wang S, Xie J, Zhao C. The association between vitamin D levels in the second trimester of pregnancy and gestational diabetes mellitus. J Obstet Gynaecol Res. 2022;48:2748–55.
Cheng Y, Chen J, Li T, Pei J, Fan Y, He M, Liu S, Liu J, Zhang Q, Cheng H. Maternal vitamin D status in early pregnancy and its association with gestational diabetes mellitus in Shanghai: a retrospective cohort study. BMC Pregnancy Childbirth. 2022;22:819.
Chen GD, Pang TT, Li PS, Zhou ZX, Lin DX, Fan DZ, Guo XL, Liu ZP. Early pregnancy vitamin D and the risk of adverse maternal and infant outcomes: a retrospective cohort study. BMC Pregnancy Childbirth. 2020;20:465.
Wilson RL, Leviton AJ, Leemaqz SY, Anderson PH, Grieger JA, Grzeskowiak LE, Verburg PE, McCowan L, Dekker GA, Bianco-Miotto T, Roberts CT. Vitamin D levels in an Australian and New Zealand cohort and the association with pregnancy outcome. BMC Pregnancy Childbirth. 2018;18:251.
Luo C, Li Z, Lu Y, Wei F, Suo D, Lan S, Ren Z, Jiang R, Huang F, Chen A, et al. Association of serum vitamin D status with gestational diabetes mellitus and other laboratory parameters in early pregnant women. BMC Pregnancy Childbirth. 2022;22:400.
Salakos E, Rabeony T, Courbebaisse M, Taieb J, Tsatsaris V, Guibourdenche J, Senat MV, Haidar H, Jani JC, Barglazan D, et al. Relationship between vitamin D status in the first trimester of pregnancy and gestational diabetes mellitus - A nested case-control study. Clin Nutr. 2021;40:79–86.
Magnusdottir KS, Tryggvadottir EA, Magnusdottir OK, Hrolfsdottir L, Halldorsson TI, Birgisdottir BE, Hreidarsdottir IT, Hardardottir H, Gunnarsdottir I. Vitamin D status and association with gestational diabetes mellitus in a pregnant cohort in Iceland. Food Nutr Res 2021, 65.
Wen J, Hong Q, Zhu L, Xu P, Fu Z, Cui X, You L, Wang X, Wu T, Ding H, et al. Association of maternal serum 25-hydroxyvitamin D concentrations in second and third trimester with risk of gestational diabetes and other pregnancy outcomes. Int J Obes (Lond). 2017;41:489–96.
Pham TTM, Huang YL, Chao JC, Chang JS, Chen YC, Wang FF, Bai CH. Plasma 25(OH)D concentrations and gestational diabetes Mellitus among pregnant women in Taiwan. Nutrients 2021, 13.
Yaribeygi H, Maleki M, Sathyapalan T, Iranpanah H, Orafai HM, Jamialahmadi T, Sahebkar A. The molecular mechanisms by which vitamin D improve glucose homeostasis: a mechanistic review. Life Sci. 2020;244:117305.
Mohd Ghozali N, Giribabu N, Salleh N. Mechanisms Linking Vitamin D Deficiency to Impaired Metabolism: An Overview. Int J Endocrinol 2022, 2022:6453882.
Retnakaran R, Shah BR. Impact of Twin Gestation and fetal sex on maternal risk of diabetes during and after pregnancy. Diabetes Care. 2016;39:e110–111.
Rauh-Hain JA, Rana S, Tamez H, Wang A, Cohen B, Cohen A, Brown F, Ecker JL, Karumanchi SA, Thadhani R. Risk for developing gestational diabetes in women with twin pregnancies. J Matern Fetal Neonatal Med. 2009;22:293–9.
Papachatzopoulou E, Chatzakis C, Lambrinoudaki I, Panoulis K, Dinas K, Vlahos N, Sotiriadis A, Eleftheriades M. Abnormal fasting, post-load or combined glucose values on oral glucose tolerance test and pregnancy outcomes in women with gestational diabetes mellitus. Diabetes Res Clin Pract. 2020;161:108048.
Acknowledgements
The authors would like to thank all the families, health professionals and researchers who contributed to this cohort study.
Funding
This work was supported by the National Key Research and Development Program of China (2023YFC2705900) and Chongqing Science and Technology Foundation (CSTB2023NSCQ-MSX0384).
Author information
Authors and Affiliations
Contributions
D.L., L.Wang., L.Wen. and H.Q. designed the research protocol; D.L., L.Wang., L.Wen., L.L., S.Z., J.T. and T.L. conducted the study; L.Wen., C.T. and Q.L. analysed the data; D.L. and L.Wang. drafted the manuscript; L.Wen. and H.Q. critically revised the manuscript; L.Wen. and H.Q. were responsible for the final contents. All authors reviewed and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University. Written informed consent were obtained from all participants.
Consent for publication
Participants were provided a study overview and verbal consent was attained.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, Dy., Wang, L., Li, L. et al. Maternal vitamin D status and risk of gestational diabetes mellitus in twin pregnancies: a longitudinal twin pregnancies birth cohort study. Nutr J 23, 41 (2024). https://doi.org/10.1186/s12937-024-00944-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12937-024-00944-2