
Abstract
Objectives
This study aimed to evaluate the association between different levels of physical activity and risk of developing type 2 diabetes (T2D) mellitus among adults with prediabetes in Chinese population.
Methods
This prospective population-based cohort study included 12,424 participants (mean [SD] age, 52.8 [16.8] years; 82.2% men) with prediabetes at 2014 survey of the Kailuan study. Physical activity information was collected through the International Physical Activity Questionnaire-Short Form and categorized by metabolic equivalent (MET) of task as low, moderate, and high. Cox regression models were built to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for associations between physical activity levels and incident T2D.
Results
During a median follow-up of 3.6 years, 2,207 (17.8%) participants developed T2D. The incident rate of T2D were 55.83/1000, 35.14/1000, and 39.61/1000 person-years in the low, moderate, and high physical activity level group, respectively. Both moderate (HR 0.57, 95% CI 0.49 to 0.67) and high (HR 0.76, 95% CI 0.66 to 0.89) physical activity levels were associated with lower risks of developing T2D compared to low physical activity level (P for trend < 0.001). The association between high physical activity level and T2D was primarily observed in participants without metabolic syndrome (P for interaction < 0.001). Moreover, participants with moderate or high levels of physical activity had significantly decreased fasting blood glucose levels during follow-up when compared to those with low level (P group*time < 0.001).
Conclusion
This study suggested that individuals with prediabetes might benefit from moderate and high levels of physical activity.
Similar content being viewed by others

Introduction
Prediabetes, a stage before diabetes, is characterized by moderately elevated blood glucose levels and, without intervention, approximately 70% of individuals at this state will progress to T2D [1,2,3]. The number of adults aged 20–79 years with prediabetes currently stands at approximately 762 million globally, and an estimated 1 billion people will be affected by 2045 [4, 5]. Prediabetes is also linked with a higher risk of developing cardiovascular diseases and all causes mortality [4, 6]. Fortunately, the prediabetic stage is manageable, and lifestyle modification including physical activity can effectively slow the progression from prediabetes to T2D [7].
Regular physical activity has been showed to improve blood glucose level and overall well-being in population with diabetes [8,9,10,11]. A review included 28 prospective studies on leisure-time physical activity or total physical activity and risk of T2D had indicated physical activity to be the primary approach for preventing and controlling T2D [12]. A meta-analysis of 6 studies found that better diet and physical activity were associated with a 53% higher possibility of returning to normal glucose levels in prediabetes participants [13]. Intervention studies like the Da Qing study, Finnish diabetes study, the American Diabetes Prevention Program, and the India Diabetes Prevention Program also indicated that moderate to vigorous physical activity could reduce the risk of developing T2D in high-risk individuals [14,15,16,17,18,19]. Korean Genome and Epidemiology study and Taiwan MJ cohort study found that prediabetes participants with higher physical activity were more likely to achieve normoglycemia and had lower risks of T2D progression and death compared to those with lower activity levels [20, 21]. However, it’s worth noting that most of those studies incorporated interventions combined physical activity with diet, making it challengeable to explore the distinct impact of physical activity alone. Furthermore, there is limited evidence regarding the association between different levels or intensities of physical activity and the risk of T2D, especially among individuals at the prediabetes stage. Hence, we aimed to investigate the association between different levels of physical activity and the risk of developing T2D in a cohort of approximately 12,400 adults with prediabetes.
Methods
Study design and participants
In this analysis, participants were derived from the ongoing Kailuan Study, which was a population-based prospective cohort study conducted in the Kailuan community of Tangshan, China. The study design has been described in previous publications [22,23,24]. In brief, the study enrolled 101,510 adult participants (81,110 men and 20,400 women) during 2006 to 2007. Furthermore, between 2008 and 2009, an additional 24,540 adult participants (19,356 men and 5,184 women) were enrolled. Participants completed questionnaires, and underwent physical measurements, clinical evaluations, and lab tests were performed in a single measurement at baseline. Subsequently, same assessments were conducted biennially. The study obtained approval from the ethics committees of Kailuan General Hospital, and all participants provided written informed consent.
This study investigated the relationship between physical activity levels and risk of T2D in the prediabetes population. Physical activity and other covariates of participants were collected from the 2014 survey (as baseline of this study) of the Kailuan Study. Participants included in present analyses were followed until December 31 2018, the average follow up time was 3.6 years. The fasting blood glucose (FBG) values were collected twice, at 2014 survey and end of the follow up period. In 2014, out of 101,588 participants, 1,718 lacked fasting plasma glucose data, 31,567 had no physical activity data, 52,626 did not meet the prediabetes criteria for FBG levels, 2,649 were lost to follow-up, and 604 deaths were excluded (Supplementary Fig. 1). Finally, a total of 12,424 participants were eligible for analysis.
Assessment of physical activity
Physical activity information of participants was collected once during 2006–2009 by using the International Physical Activity Questionnaire-Short Form [25]. Participants were asked how many days per week they did exercise; what kind of physical activity they performed; and how long each exercise session lasted (< 30 min; 30–60 min; ≥60 min). We categorize MET intensity into three levels: high (8 METs), moderate (4 METs), and low (3.3 METs). The formula is: weekly exercise days × daily exercise duration (minutes) × MET intensity = weekly total MET minutes. Add up all weekly MET minutes to get the total MET value. After collecting frequency and intensity of the weekly physical activity, participants were categorized into three groups based on their weekly MET value: low (< 600 MET-minutes per week), moderate (600–3000 MET-minutes per week), and high (≥ 3000 MET-minutes per week). These categories represented different levels of physical activity engagement, as detailed elsewhere [26, 27].
Assessment of prediabetics, T2D, changes of FBG, and metabolic syndrome
The primary outcome of our study is the incidence of T2D among prediabetic participants during the follow-up period. Prediabetes is defined as FBG level range between 5.6 and 6.9 mmol/L according to the guidelines of American Diabetes Association [28]. T2D is defined as meeting any of the following criteria: FBG ≥ 7.0 mmol/L, a self-reported physician diagnosis, or self-reported use of anti-diabetic medication. The secondary outcome is the change in FBG levels between the baseline (2014 resurvey) and final FBG tests (2016 or 2018 resurvey) among participants from different physical activity groups. Metabolic syndrome was diagnosed by three or more of the following criteria: TG ≥ 150 mg/dl (1.7 mmol/L), HDL-C < 40 mg/dl (1.03 mmol/L) in men and < 50 mg/dl (1.29 mmol/L) in women, fasting glucose ≥ 100 mg/dl (5.6 mmol/L) or previously diagnosed with type 2 diabetes, blood pressure ≥ 130/85 mmHg or on antihypertensive medication, and central obesity (defined as waist circumference ≥ 90 cm in men and ≥ 80 cm in women, according to the ethnic criteria for Asians) [29, 30].
Data collection and definition
Demographic information (e.g., age, sex), socioeconomic status (e.g., income), family history of diabetes, and lifestyle factors (e.g., smoking status, alcohol consumption, sleep duration, physical activity, and dietary intake) were collected through a structured questionnaire. Education level was categorized as middle school and below, high school, or college and above. Average monthly income of each family member was classified as < 1,000 Yuan, 1,000–3,000 Yuan and ≥ 3,000 Yuan. Smoking status was defined as either a current smoker or never having smoked. Alcohol consumption was defined as either a current drinker or never having drunk.
Height and weight measurements were taken by trained nurses under standardized conditions, with participants wearing light clothes and being barefoot. Heights were measured to the nearest 0.1 cm, and weights were measured to the nearest 0.1 kg. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Waist circumference was also measured at standing position. Blood pressure was measured in the seated position and the average of three readings was recorded as systolic blood pressure (SBP) and diastolic blood pressure (DBP). Hypertension was defined as SBP ≥ 140 mm Hg or DBP ≥ 90 mm Hg, the use of antihypertensive medication, or a self-reported history of hypertension. Blood samples were collected after an 8 to 12-hours fasting period. FBG levels were measured using the Hexokinase/Glucose-6-phosphate dehydrogenase method (Mind Bioengineering Co., Ltd., Shanghai, China), with an upper detection limit of 30.07 mmol/L. Triglyceride (TG), total cholesterol (TC), low-density lipoprotein-cholesterol (LDL-C), and high-density lipoprotein-cholesterol (HDL-C) levels were measured by automatic analyzer (Hitachi 747, Hitachi, Tokyo, Japan).
Statistical analysis
Continuous, normally distributed data were summarized as mean and standard deviations; while categorical data were summarized as the numbers and percentages. For 12,424 prediabetes participants included in the analysis, their demographic information (sex, age, education, income, marital status), behavioral status (smoking status, sleep duration, TV hours), and biochemical characteristics (FBG, DBP, and SBP) were described according to three levels of physical activity. For each individual, the person-time of follow-up was calculated from the 2014 survey date until the occurrence of T2D, being lost to follow-up, death or end of follow-up (December 31, 2018), whichever happened first. Supplementary Table 1 shows baseline characteristics for all participants and participants with prediabetes in the 2014 resurvey.
Cox proportional hazard models were utilized to determine hazard ratios (HR) and 95% confidence intervals (CIs) for the incidence of T2D in the three physical activity groups (low, moderate, and high), using the low physical activity group as reference. According to Schoenfeld residuals, our models satisfied the proportional assumption criteria. In Model 1, age and sex (men, women) were adjusted as covariates. Model 2 was further adjusted for smoking status (current or never), alcohol consumption (current drinker or never drink), sleep hours (< 5, 5–7, or ≥ 7 h/day), TV time (< 2, 2–3, or ≥ 4 h/day), central obesity (yes or no), family history of diabetes (yes or no), education level (middle school and below, high school, or college and above), average monthly income of each family member (< 1000, 1000–3000, or ≥ 3000 Yuan), marital status (married or single), dietary approaches to stop hypertension (DASH) diet score (≤ 25, 26–30, or ≥ 31 points), and BMI categories (< 24, 24 ≤ BMI < 28, or ≥ 28 kg/m2). In model 3, systolic blood pressure, LDL-C, and TG were further adjusted for as the full model. Supplementary Table 2 indicated how DASH score was classified. Sensitivity analyses were conducted after excluding participants with conditions such as cancer, cerebral hemorrhage, cerebral infraction, subarachnoid rainbow, ankylosing spondylitis, rheumatoid joint disease, gout, and Parkinson’s disease to test the consistency and stability of the results. Stratified analyses were performed based on sex, age, BMI, smoking status, alcohol consumption, nighttime sleeping hours, metabolic syndrome, hypertension, and DASH diet score. A likelihood ratio test was applied to examine the significance of interactions.
For FBG changes, mixed-effects liner models were used to analyze the effect of group (physical activity levels), time, and group by time interaction with adjusting for age, sex, and baseline FBG. In the analysis, individual participant was treated as random effects, while the group, times, and their interaction were considered as fixed effects. Statistical analysis was performed using R software (version 4.2.2) and SAS version 9.4 (SAS Institute, Cary, NC, USA). The level of significance was taken as two-sided P < 0.05.
Results
Characteristics of the study participants
The characteristics of the study population at the 2014 resurvey, grouped according to different levels of physical activity, were presented in Table 1. Among the 12,424 participants enrolled in this study, 66% were categorized as having a low level of physical activity, 17.3% as having a moderate level, and 16.7% as having a high level. The participants had an average age of 52.7 years with a standard deviation of 16.7 years, and 82.2% of them were men. Compared with participants in groups of moderate and high physical activity level, those in low physical activity level group tended to be older, had longer sleep duration, and higher levels of BMI, TC, and TG.
The association between physical activity levels and T2D
During an average follow-up period of 3.6 years [(IQR 2.4–4.4); total cumulative follow-up was 44,563 person years] among the 12,424 participants, 2,207 (17.8%) developed T2D. Concurrently, 5,638 (45.37%) remained prediabetic, while 4,579 (36.86%) returned to a normoglycemic state.
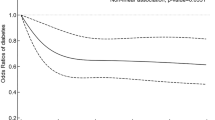
As shown in Table 2, both moderate and high physical activity levels were linked to a lower risk of developing T2D compared to low physical activity level. In the full model, the moderate and high physical activity groups had a 43% and 24% lower risk of T2D, respectively. Figure 1 presents the Kaplan-Meier curves, which reveals that the group with moderate activity levels exhibited the lowest risk for T2D, while the group engaged in low physical activity had the highest risk (P for log-rank test < 0.001).

Physical activity and risk of incident T2D. Kaplan-Meier estimation of association between physical activity and risk of incident T2D. Red, green, and blue lines represent for low (< 600 metablic equivalent-minutes per week), moderate (600–3000 metablic equivalent-minutes per week), and high (≥ 3000 metablic equivalent-minutes per week). Logrank P < 0.001 stands for observed differences between type 2 diabetes incidence between low, moderate and high physical activity groups were highly significant
Sensitivity analyses were conducted by excluding participants with cancer, cerebral hemorrhage, cerebral infraction, subarachnoid rainbow, ankylosing spondylitis, rheumatoid joint disease, gout, and Parkinson disease. Both groups of moderate and high physical activity levels remained significantly associated with lower risk of T2D (HR 0.56, 95% CI 0.48 to 0.68 and HR 0.75, 95% CI 0.66 to 0.88, respectively) compared with low physical activity group in fully adjusted model (Supplementary Table 3).
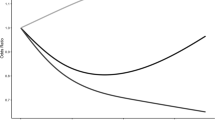
In the stratified analysis presented in Table 3, the relationship between different physical activity levels and the risk of T2D remained consistent across different strata, including sex, BMI, smoking status, alcohol consumption, nighttime sleeping hours, hypertension, and the DASH score (all P value for interaction ≥ 0.05). However, the association between high physical activity level and T2D was primarily observed in participants without metabolic syndrome (P value for interaction < 0.001). Figure 2 visually depicts a marked difference between participants with and without metabolic syndrome. A similar interaction was observed in the age-stratified group, indicating that the association between physical activity level and risk of T2D was stronger in young participants (Table 3, P value for interaction 0.02). A J-shaped relationship between physical activity and the risk of T2D was observed, which reached a nadir at 1100–1500 MET minutes/week (P for non-linear < 0.001, Supplementary Fig. 2).

Physical activity and risk of incident T2D stratified by metabolic syndrome status. Kaplan-Meier estimation of association between physical activity and risk of incident T2D stratified by metabolic syndrome status. A represents participants with metabolic syndrome and B represents individuals free of metabolic syndrome. Red, green, and blue lines represent for low (< 600 metablic equivalent-minutes per week), moderate (600–3000 metablic equivalent-minutes per week), and high (≥ 3000 metablic equivalent-minutes per week). Logrank P < 0.001 stands for observed differences between type 2 diabetes incidence between low, moderate and high physical activity groups were highly significant
Mixed-effects linear model
Supplementary Table 4 presents data on how different levels of physical activity were associated with FBG change in this cohort. All three physical activity groups had a similar average baseline FBG level. During the follow-up period, the low physical activity group experienced an average increase in FBG of 0.20 mmol/L (95% CI, 0.15 to 0.26) compared to their baseline level. Conversely, participants in both the moderate and high physical activity groups exhibited average reductions in their FBG values compared to baseline levels (-0.27 mmol/L, 95% CI, -0.38 to -0.16 in moderate group and − 0.18 mmol/L,95% CI, -0.30 to -0.07 in high level group, respectively). In the mixed-effects linear model, we observed a significant interaction of group × time (P group*time < 0.001) on FBG.
Discussion
In our prospective cohort study conducted in the Kailuan community, we investigated the association between three distinct levels of physical activity and the risk of developing T2D, specifically among individuals with prediabetes. Our findings suggest that moderate and high levels of physical activity were associated with lower risk of developing T2D, relative to low physical activity level. Moreover, the association between high physical activity level and incident T2D is primarily observed among participants without metabolic syndrome. During follow-up, a reduction of FBG value was observed in individuals with moderate and high physical activity levels, while an average increase of 0.2 mmol/L of FBG was found in the low physical activity level group. The results of our study provided further evidence to support the potential benefits of physical activity on risk of T2D particularly in participants with prediabetes, which contributes to our understanding of T2D prevention.
Majority studies to date have focused on the relationship of dietary habits, physical activity, and sedentary behavior with risk of T2D [31,32,33]. The investigation into how varying levels of physical activity is related to the risk of T2D is scare, particularly for population at the prediabetes stage. Researches had emphasized the influence of physical activity on life quality or change of glycemic markers rather than T2D risks. For instance, a cross-sectional study involving 232 Northern Alberta residents with prediabetes revealed that those with higher levels of physical activity had an enhanced quality of life in comparison to their inactive counterparts [34, 35]. In the cohort of 10,308 British civil servants (Whitehall II study), 957 participants with prediabetes were followed up for 5 years [35], and moderate-to-vigorous physical activity was associated with better insulin sensitivity and β-cell function. Moreover, a RCT tested the individual and combined effects of physical activities and metformin on insulin sensitivity in 32 participants with prediabetes, exhibiting improved insulin sensitivity in exercise training with or without adding metformin [36]. Our study was focused on the relationship between physical activity and risk of T2D in the prediabetes population, providing more evidence for the prevention strategies of this high-risk population.
Our study showed that participants with moderate and high physical activity had 43% and 24% lower T2D incidence than those with low activity levels. The findings are consistent with a previous cohort study, demonstrating that participating in physical activity was associated with lower risk of T2D [37]. However, the previous cohort study of 8,796 prediabetic Spanish workers has identified physical activity as one of the key factors influencing prediabetes persistence and progression to T2D, but didn’t compute MET values into different physical activity levels [38]. For general population, in a meta-analysis including 28 prospective cohort studies, physical activity level was converted into MET h/week or marginal MET (MMET) h/week for the analysis [12]. The results revealed that higher level of leisure-time physical activity, specifically exceeding 11.25 MET-hours per week, was linked to a 26% lower incidence of T2D. However, most cohorts in the meta-analysis were not designed to solely access physical activity level, making it challengeable to explore the specific impact of physical activity on risk of T2D. Our study has linked different levels of physical activity with risk of developing T2D among participants with prediabetes, supporting the recommendation of physical activity for this specific population.
Remarkably, we found that the association between high physical activity and the incidence of T2D was observed primarily in participants without metabolic syndrome (P value for interaction < 0.001). Metabolic syndrome refers to the pathological state related symptoms such as obesity, hypertension, dyslipidemia, and hyperglycemia, and significantly increases T2D risk [9]. The underlying mechanism was not fully understood but might be due to several reasons. First, the higher level of physical activity is often accompanied by increased blood flow and elevated blood pressure, which may pose a potential long-term risk for participants with unstable blood glucose [38]. Second, intense workouts can stimulate the release of stress hormones, including adrenaline, which can stimulate the liver to release glucose [39]. Third, the moderate physical activity may bring more benefits than high level physical activity. A recent systematic review and meta-analysis of 126 studies, including 8 focusing on prediabetics, identified a J-shaped relationship between physical activity and HbA1c levels [40]. For prediabetes, the optimal physical activity level was found to be 1,100 MET-minutes per week, achieving a reduction in HbA1c of -0.38% to -0.24%. This optimal physical activity level aligns with the moderate physical activity level defined in our study (600–3000 MET-minutes per week). These factors highlight potential concerns for individuals with unstable blood glucose during high level physical activity [39]. Although more evidence is needed for optimal physical activity level to improve glycemic control in prediabetics, American College of Sports Medicine often recommend a moderate level of physical activity for individuals with chronic diseases [41].
Our results indicated that the moderate physical activity group had lowest risk of T2D. After the physical activity level exceeded 4000 MET minutes/week, protective effects of physical activity against T2D diminished (Supplementary Fig. 2). Our finding suggests the existence of an “optimal range” where moderate levels of physical activity could benefit metabolic health without the potential stress or negative effects associated with very high levels of physical activity. A systematic review and meta-analysis of eight studies focusing on prediabetic individuals identified a J-shaped relationship between physical activity and HbA1c levels, which is consistent with our findings [42]. The underlying mechanisms, though not fully understand, might be multifaceted. Aerobic and resistance exercises, as major forms of moderate physical activity, have been shown to enhance insulin sensitivity in skeletal muscles and improve glucose transport, thereby demonstrating their effectiveness in controlling blood glucose levels [43]. However, prolonged high-intensity physical activity may increase the production of pro-inflammatory cytokines, leading to elevated muscle oxidative stress, which may create a vicious cycle that further escalates inflammation [44], thereafter increases the risk of T2D. In contrast, moderate intensity activities may be more sustainable for long-term adherence and less likely to cause hypoglycemia or other stress responses in the body [45]. Therefore, promoting and sustaining physical activity are essential priorities for managing blood glucose levels and improving overall health in individuals with prediabetes.
Limitations
Our study has several strengths such as its large sample size which allows for robust statistical analysis and capture of a relatively large number of T2D incident events. However, this study also has several limitations that should be acknowledged. First, physical activity was assessed once at baseline, which limits the possibility to analyze long-term patterns and changes in physical activity over time. Second, the physical activity data was acquired from questionnaires, and misclassification bias introduced by self-reported information were inevitable. Third, participants with prediabetes were defined by FBG measurement at baseline, which might be underestimated without including HbA1c and/or 2 h blood glucose after glucose tolerance test in the diagnostic criteria. Lastly, the mean follow-up duration of 3.6 years is relatively short; however, reverse causality bias is unlikely in our study since we excluded individuals with existing T2D or taking anti-diabetic medication at baseline and included only the first episode of T2D after baseline.
Conclusion
In summary, our study provides compelling evidence that engagement in physical activity holds a pivotal role in mitigating the occurrence of T2D among individuals classified as prediabetes based on FBG criteria. These results underscore the significance of integrating physical activity as a fundamental element in the management strategies for individuals with prediabetes.
Data availability
All data collected in the current study are available after permission of the Kailuan Institutional Review Board. Written proposals can be addressed to the corresponding authors for appropriateness of use.
Abbreviations
- BMI:
-
Body mass index
- DBP:
-
Diastolic blood pressure
- DASH:
-
dietary approaches to stop hypertension
- FBG:
-
Fasting blood glucose
- HDL-C:
-
high-density lipoprotein-cholesterol
- LDL-C:
-
low-density lipoprotein-cholesterol
- SBP:
-
Systolic blood pressure
- T2D:
-
Type 2 diabetes
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
References
Vendrame F, Gottlieb PA. Prediabetes: prediction and prevention trials. Endocrinol Metab Clin North Am. 2004;33:75–92. ix.
Tuomilehto J, Lindström J, Eriksson JG, Valle TT, Hämäläinen H, Ilanne-Parikka P, Keinänen-Kiukaanniemi S, Laakso M, Louheranta A, Rastas M, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001;344:1343–50.
Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, Nathan DM. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393–403.
Rooney MR, Fang M, Ogurtsova K, Ozkan B, Echouffo-Tcheugui JB, Boyko EJ, Magliano DJ, Selvin E. Global prevalence of Prediabetes. Diabetes Care. 2023;46:1388–94.
International Diabetes Federation. [https://diabetesatlas.org].
Shang Y, Marseglia A, Fratiglioni L, Welmer AK, Wang R, Wang HX, Xu W. Natural history of prediabetes in older adults from a population-based longitudinal study. J Intern Med. 2019;286:326–40.
Echouffo-Tcheugui JB, Perreault L, Ji L, Dagogo-Jack S. Diagnosis and management of prediabetes: a review. JAMA. 2023;329:1206–16.
Raghavan S, Jablonski K, Delahanty LM, Maruthur NM, Leong A, Franks PW, Knowler WC, Florez JC, Dabelea D. Interaction of Diabetes genetic risk and successful lifestyle modification in the Diabetes Prevention Programme. Diabetes Obes Metab. 2021;23:1030–40.
Kriska AM, Rockette-Wagner B, Edelstein SL, Bray GA, Delahanty LM, Hoskin MA, Horton ES, Venditti EM, Knowler WC, Group DPPR. The impact of physical activity on the Prevention of type 2 diabetes: evidence and lessons learned from the Diabetes Prevention Program, a long-standing clinical trial incorporating subjective and objective activity measures. Diabetes Care. 2021;44:43–9.
Kolb H, Martin S. Environmental/lifestyle factors in the pathogenesis and prevention of type 2 diabetes. BMC Med. 2017;15:131.
Colberg SR, Sigal RJ, Fernhall B, Regensteiner JG, Blissmer BJ, Rubin RR, Chasan-Taber L, Albright AL, Braun B. American College of Sports M, American Diabetes A: Exercise and type 2 diabetes: the American College of Sports Medicine and the American Diabetes Association: joint position statement executive summary. Diabetes Care. 2010;33:2692–6.
Smith AD, Crippa A, Woodcock J, Brage S. Physical activity and incident type 2 diabetes mellitus: a systematic review and dose-response meta-analysis of prospective cohort studies. Diabetologia. 2016;59:2527–45.
Balk EM, Earley A, Raman G, Avendano EA, Pittas AG, Remington PL. Combined Diet and Physical Activity Promotion Programs to prevent type 2 diabetes among persons at increased risk: a systematic review for the Community Preventive Services Task Force. Ann Intern Med. 2015;163:437–51.
Pan XR, Li GW, Hu YH, Wang JX, Yang WY, An ZX, Hu ZX, Lin J, Xiao JZ, Cao HB, et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care. 1997;20:537–44.
Laaksonen DE, Lindstrom J, Lakka TA, Eriksson JG, Niskanen L, Wikstrom K, Aunola S, Keinanen-Kiukaanniemi S, Laakso M, Valle TT, et al. Physical activity in the prevention of type 2 diabetes: the Finnish diabetes prevention study. Diabetes. 2005;54:158–65.
The Diabetes Prevention Program. Design and methods for a clinical trial in the prevention of type 2 diabetes. Diabetes Care. 1999;22:623–34.
Ramachandran A, Snehalatha C, Mary S, Mukesh B, Bhaskar AD, Vijay V. The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1). Diabetologia. 2006;49:289–97.
Ford CN, Do WL, Weber MB, Narayan KMV, Ranjani H, Anjana RM. Moderate-to-vigorous physical activity changes in a diabetes prevention intervention randomized trial among South asians with prediabetes - the D-CLIP trial. Diabetes Res Clin Pract. 2021;174:108727.
Bennett WC, Collins KA, Johnson JL, Slentz CA, Willis LH, Bales CW, Huffman KM, Kraus WE. Effects of exercise amount and intensity versus a combined exercise and lifestyle intervention on metabolic syndrome in adults with prediabetes: a STRRIDE-PD randomized trial. Front Physiol. 2023;14:1199763.
Nabila S, Kim J-E, Choi J, Park J, Shin A, Lee S-A, Lee J-k, Kang D, Choi J-Y. Associations between modifiable risk factors and changes in Glycemic Status among individuals with Prediabetes. Diabetes Care. 2023;46:535–43.
Cao Z, Li W, Wen CP, Li S, Chen C, Jia Q, Li W, Zhang W, Tu H, Wu X. Risk of death Associated with Reversion from prediabetes to Normoglycemia and the role of modifiable risk factors. JAMA Netw Open. 2023;6:e234989.
Wu S, Huang Z, Yang X, Zhou Y, Wang A, Chen L, Zhao H, Ruan C, Wu Y, Xin A, et al. Prevalence of ideal cardiovascular health and its relationship with the 4-year cardiovascular events in a northern Chinese industrial city. Circ Cardiovasc Qual Outcomes. 2012;5:487–93.
Wang A, Sun Y, Liu X, Su Z, Li J, Luo Y, Chen S, Wang J, Li X, Zhao Z, et al. Changes in proteinuria and the risk of myocardial infarction in people with diabetes or pre-diabetes: a prospective cohort study. Cardiovasc Diabetol. 2017;16:104.
Jin C, Chen S, Vaidya A, Wu Y, Wu Z, Hu FB, Kris-Etherton P, Wu S, Gao X. Longitudinal change in fasting blood glucose and myocardial infarction risk in a Population without Diabetes. Diabetes Care. 2017;40:1565–72.
International Physical Activity Questionnaire. - Short Form [https://youthrex.com/wp-content/uploads/2019/10/IPAQ-TM.pdf ].
Kim SY, Park JH, Lee MY, Oh KS, Shin DW, Shin YC. Physical activity and the prevention of depression: a cohort study. Gen Hosp Psychiatry. 2019;60:90–7.
Cleland C, Ferguson S, Ellis G, Hunter RF. Validity of the International Physical Activity Questionnaire (IPAQ) for assessing moderate-to-vigorous physical activity and sedentary behaviour of older adults in the United Kingdom. BMC Med Res Methodol. 2018;18:176.
Understanding Diabetes Diagnosis. https://diabetes.org/about-diabetes/diagnosis
Alberti G, Zimmet P, Shaw J, Grundy SM. The IDF consensus worldwide definition of the metabolic syndrome. Brussels: Int Diabetes Federation. 2006;23:469–80.
Liu J, Grundy SM, Wang W, Smith SC Jr., Vega GL, Wu Z, Zeng Z, Wang W, Zhao D. Ethnic-specific criteria for the metabolic syndrome: evidence from China. Diabetes Care. 2006;29:1414–6.
Zhu P, Lao G, Li H, Tan R, Gu J, Ran J. Replacing of sedentary behavior with physical activity and the risk of mortality in people with prediabetes and diabetes: a prospective cohort study. Int J Behav Nutr Phys Act. 2023;20:81.
Li Y, Schoufour J, Wang DD, Dhana K, Pan A, Liu X, Song M, Liu G, Shin HJ, Sun Q, et al. Healthy lifestyle and life expectancy free of cancer, cardiovascular disease, and type 2 diabetes: prospective cohort study. BMJ. 2020;368:l6669.
Jiang Z, Sun TY, He Y, Gou W, Zuo LS, Fu Y, Miao Z, Shuai M, Xu F, Xiao C, et al. Dietary fruit and vegetable intake, gut microbiota, and type 2 diabetes: results from two large human cohort studies. BMC Med. 2020;18:371.
Taylor LM, Spence JC, Raine K, Plotnikoff RC, Vallance JK, Sharma AM. Physical activity and health-related quality of life in individuals with prediabetes. Diabetes Res Clin Pract. 2010;90:15–21.
Faerch K, Witte DR, Brunner EJ, Kivimaki M, Tabak A, Jorgensen ME, Ekelund U, Vistisen D. Physical activity and improvement of Glycemia in Prediabetes by different diagnostic criteria. J Clin Endocrinol Metab. 2017;102:3712–21.
Malin SK, Gerber R, Chipkin SR, Braun B. Independent and combined effects of exercise training and metformin on insulin sensitivity in individuals with prediabetes. Diabetes Care. 2012;35:131–6.
Bennasar-Veny M, Fresneda S, Lopez-Gonzalez A, Busquets-Cortes C, Aguilo A, Yanez AM. Lifestyle and progression to type 2 diabetes in a cohort of workers with Prediabetes. Nutrients 2020, 12.
Kim D, Ha JW. Hypertensive response to exercise: mechanisms and clinical implication. Clin Hypertens. 2016;22:17.
Schweitzer GG, Ditzenberger GL, Hughey CC, Finck BN, Martino MR, Pacak CA, Byrne BJ, Cade WT. Elevated liver glycogenolysis mediates higher blood glucose during acute exercise in Barth syndrome. PLoS ONE. 2023;18:e0290832.
Gallardo-Gómez D, Salazar-Martínez E, Alfonso-Rosa RM, Ramos-Munell J, Del Pozo-Cruz J, Del Pozo Cruz B, Álvarez-Barbosa F. Optimal dose and type of physical activity to improve Glycemic Control in people diagnosed with type 2 diabetes: a systematic review and Meta-analysis. Diabetes Care. 2024;47:295–303.
Pescatello LS, Franklin BA, Fagard R, Farquhar WB, Kelley GA, Ray CA. American College of Sports M: American College of Sports Medicine position stand. Exercise and hypertension. Med Sci Sports Exerc. 2004;36:533–53.
Aune D, Norat T, Leitzmann M, Tonstad S, Vatten LJ. Physical activity and the risk of type 2 diabetes: a systematic review and dose-response meta-analysis. Eur J Epidemiol. 2015;30:529–42.
Evans PL, McMillin SL, Weyrauch LA, Witczak CA. Regulation of Skeletal Muscle Glucose Transport and glucose metabolism by Exercise Training. Nutrients 2019, 11.
Cheng AJ, Jude B, Lanner JT. Intramuscular mechanisms of overtraining. Redox Biol. 2020;35:101480.
Ryan BJ, Schleh MW, Ahn C, Ludzki AC, Gillen JB, Varshney P, Van Pelt DW, Pitchford LM, Chenevert TL, Gioscia-Ryan RA, et al. Moderate-intensity Exercise and high-intensity interval training affect insulin sensitivity similarly in obese adults. J Clin Endocrinol Metab. 2020;105:e2941–2959.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
WY, YW, SW, and LS conceived and designed this work. WY, YW, YC, SC, and XG researched data. WY analyzed the data. WY, YW, SW, and LS interpreted the results and drafted the manuscript. SW and LS supervised the study. All authors contributed to the review and revision of the manuscript and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was performed according to the guidelines of the Helsinki Declaration and was approved by the Ethics Committee of Kailuan General Hospital (Approval Number: 2006–05). All participants were agreed to take part in the study and provided informed written consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, W., Wu, Y., Chen, Y. et al. Different levels of physical activity and risk of developing type 2 diabetes among adults with prediabetes: a population-based cohort study. Nutr J 23, 107 (2024). https://doi.org/10.1186/s12937-024-01013-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12937-024-01013-4