
Abstract
Background
Iron deficiency anemia (IDA) is a common health problem worldwide. The objective of this study was to noninvasively and quantitatively evaluate early changes in left ventricular systolic function in patients with IDA using the left ventricular press–strain loop (LV-PSL).
Methods
Sixty-two patients with IDA were selected and divided into two groups based on hemoglobin (Hb) concentration: Group B with Hb > 9 g/dL and group C with 6 g/dL < Hb < 9 g/dL. Thirty-three healthy individuals were used as the control (Group A). The global longitudinal strain (GLS), global work index (GWI), global constructive work (GCW), global waste work (GWW), global work efficiency (GWE) were derived using LV-PSL analysis. Receiver operating characteristic (ROC) curves were constructed for MW parameters to detect abnormal left ventricular systolic function in IDA patients.
Results
Compared to group A, GWI and GCW were reduced in group B (both P < 0.01). Compared with groups B and A, GLS, GWI, GCW and GWE, and E/A were all diminished, and GWW, LVEDV, LVESV, and E/mean e’ were all increased in group C (all P < 0.01). GLS was positively correlated with GWI, GCW, and GWE (r = 0.679, 0.681, and 0.447, all P < 0.01), and negatively associated with GWW (r = − 0.411, all P < 0.01). For GWI, area under the ROC curve (AUROC) was 0.783. The optimal GWI threshold for detecting abnormal LV systolic function in IDA was1763 mmHg%, with sensitivity of 0.71 and specificity of 0.78.
Conclusions
LV-PSL allows noninvasive quantitative assessment of early impaired LV systolic function in IDA patients with preserved LV ejection fraction, and GWI has high sensitivity and specificity compared with other parameters.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Anemia is a condition in which the volume of red blood cells in the human peripheral blood is reduced below the lower limit of the normal range, resulting in a lower level of hemoglobin (Hb). The WHO estimates that about 1/4 of the global population, mainly preschool children and females, suffer from anemia, making it still a major public health problem worldwide [1, 2]. Among these, iron deficiency is the underlying cause of most anemias, which currently affects about 1.6 billion people worldwide, or 24.8% of the global population [3]. Therefore, Iron deficiency anemia (IDA) is one of the most predominant types of anemia worldwide [4].
Iron deficiency anemia is very common in daily clinical practice, with symptoms such as weakness, fatigue, dizziness, headache, tinnitus, palpitations and shortness of breath. These symptoms are mild at first, so patients often do not notice them. As the degree of iron deficiency and anemia worsens, these symptoms will also gradually worsen. Several observational studies have shown that iron deficiency and anemia are considered independent risk factors for cardiovascular disease (CVD) in the general population, leading to higher morbidity and mortality [5, 6]. Long-term anemia can cause abnormal changes in cardiac structure and function [7]. Early IDA treatment can improve the prognosis of CVD, repair the myocardium, promote myocardial effective work, and restore the patient's activity endurance [8, 9]. Therefore, early assessment of cardiac trends in IDA patients can help guide medical therapy and prevent cardiovascular events.
The left ventricular pressure–strain loops (LV-PSL) technique is a new noninvasive method for assessing myocardial function based on the principle of two-dimensional speckle tracking. Compared to the traditional left ventricular ejection fraction (LVEF) and global longitudinal strain (GLS) obtained by two dimensional speckle tracking, LV-PSL accounts for afterload effects on LV myocardial contraction. This improves the accuracy of assessing myocardial function [10]. The reliability of LV-PSL has been demonstrated in healthy and cardiovascular disease groups, but it has not been studied in IDA [11,12,13]. The aim of this study was to investigate the application of the noninvasive LV-PSL technique for quantitatively assessing early changes in left ventricular systolic function in patients across a spectrum of IDA severities.
Results
Study population and clinical characteristics
Demographic characteristics of the three groups are presented in Table 1. There were no statistically significant differences in gender, age, heart rate, systolic blood pressure, diastolic blood pressure, BMI, and duration of IDA between the groups with different degrees of IDA and the control group (all P > 0.05).
Traditional echocardiographic parameters
Traditional echocardiographic characteristics of IDA patients and healthy controls are compared in Table 2. LVEDV, LVESV, and E/mean e’ were all increased in Group C compared with Groups A and B, and E/A was reduced, with a statistically significant difference (all P < 0.01). These conventional echocardiographic parameters were not statistically different between Groups A and B (all P > 0.05). Left ventricular ejection fraction (LVEF) was similar across all three groups (all P > 0.05).
Myocardial work parameters and correlation analysis
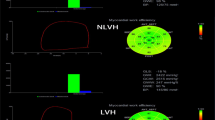
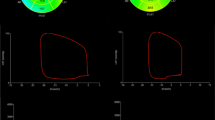
Myocardial work parameters for the 3 groups are shown in Table 3. Compared to Groups A and B, Group C exhibited significantly decreased GLS, GWI, GCW, and GWE and a significant increase in GWW (all P < 0.01). Group B showed reduced GWI and GCW compared with Group A (both P < 0.01).The LV PSL curves for the three groups are shown in Figs. 1, 2, 3. Correlation analysis showed that GLS was positively correlated with GWI, GCW, and GWE (r = 0.679, 0.681, and 0.447, all P < 0.01), and negatively correlated with GWW (r = − 0.411, P < 0.01).

A LV-PSL analysis of the control group (GWI 1940 mmHg%, GCW 2221 mmHg%, GWW 81 mmHg%, GWE 96%)

B LV-PSL analysis graph for mild anemia group (GWI 1619 mmHg%, GCW 1939 mmHg%, GWW 159 mmHg%, GWE 92%)

C LV-PSL analysis graph for moderate anemia group (GWI 1306 mmHg%, GCW 1774 mmHg%, GWW 203 mmHg%, GWE 89%)
Intra- and inter-observer variability
Intra- and interobserver variabilities in the myocardial work parameters are shown in Table 4. The intra-observer correlation coefficients (ICC) between LV GLS and GWI, GCW, GWW, and GWE were 0.905, 0.913, 0.924, 0.943, and 0.896, respectively. Between different observers, ICCs were 0.843, 0.917, 0.911, 0.939, and 0.878, respectively. These results demonstrate good reproducibility of the noninvasive LV-PSL technique for evaluating left ventricular myocardial work indices in relation to GLS analyzed by 2D-speckle tracking echocardiography.
Receiver operating characteristic (ROC) curve analysis
Based on ROC curve analysis of main MW parameter, AUROC of GWI, GCW, GWW and GWE were 0.784, 0.741, 0.711 and 0.659, respectively. GWI was the best diagnostic index for identifying impaired LV myocardial function in IDA patients with preserved LV ejection fraction. The sensitivity and specificity were 71% and 78%, respectively. The optimal threshold of GWI was 1763 mmHg% (Fig. 4).

Area under the ROC curve of GLS and LV myocardial work parameters for the diagnosis of IDA: the AUC of the GWI was superior to the other parameters, with sensitivities, specificities, and optimal thresholds of 71%, 78%, and 1763 mmHg%, respectively
Discussion
Iron deficiency anemia is a commonly overlooked complication in patients with heart failure [15,16,17]. In this case, the body does not have enough iron to produce hemoglobin, resulting in the blood not being able to effectively carry oxygen to all parts of the body, which further burdens the heart [18]. Therefore, in order to better evaluate left ventricular function in patients with iron deficiency anemia, many echocardiographic methods have been proposed. In recent years, two-dimensional and three-dimensional speckle tracking LV-GLS has become a routine measurement method to evaluate LV function in patients with iron deficiency anemia, which can indicate the early changes of left ventricular myocardial function before LVEF changes. The results of this study showed that the GLS of the moderate anemia group was lower than that of the control group and the mild anemia group, which was consistent with the results of ZHOU et al. [7], indicating that the myocardial contractility of patients with moderate IDA was impaired even if LVEF was within the normal range. Abnormal GLS is associated with the development of HF, mortality and LV remodeling [19]. Decreased strain rate is a marker of decreased contractility. The underlying reason may be that GLS is mainly dominated by endocardial longitudinal myocardial fibers supplied by small vessels at the end of coronary arteries and is more susceptible to ischemia and hypoxia. Results in decreased systolic and diastolic function of the left ventricle. In addition, IDA causes the heart to be in a state of high cardiac output for a long time, which increases the pre- and post-load of the left ventricle, leading to a gradual decline in myocardial systolic function and GLS.
However, due to the load-dependent nature of GLS, it is difficult to distinguish whether it is the actual myocardial damage or the changes in cardiac function caused by the change in load [20]. Therefore, new and more comprehensive ultrasound detection techniques are needed. Russell et al. combined speckle-tracking strain analysis with noninvasive left ventricular pressure curves to form a left ventricular pressure–strain loop (LV-PSL), in which strain represents distance and wall pressure represents force, to derive continuous changes in myocardial work throughout the cardiac cycle independent of afterload [21]. Previous studies have shown a good correlation between noninvasively measured left ventricular pressure (cuff pressure) and invasively measured left ventricular pressure [22]. In this study, GWI and GCW in group B were reduced compared with group A, while GLS did not change, indicating that GWI and CCW are more sensitive than GLS and LVEF in evaluating myocardial systolic function. With the aggravation of anemia, GWI and GCW in group C were lower than those in group A and B, and GWW was higher than that in group A and B. GWE was the ratio of GCW to the sum of GCW and GWW, which was also significantly reduced. It indicated that the myocardial systolic function of patients with moderate anemia was further reduced, suggesting that LV dysfunction may occur in the early stage of myocardial damage in patients with anemia even if LVEF was preserved. The possible reason is that iron deficiency can lead to the decrease of collagen synthesis in myocardial cells, resulting in the change of pressure–volume relationship and the decrease of myocardial elasticity [23]. Elcioğlu et al. [24] also found that young women with low ferritin levels, regardless of anemia, showed reduced left ventricular systolic function in the early stage. In addition, IDA can lead to myocardial ischemia and hypoxia symptoms, impaired energy metabolism and mitochondrial biosynthesis, accumulation of anaerobic fermentation products such as lactic acid, and disorder of intracellular ion homeostasis, resulting in cell edema, fine structure changes, loss of normal contract-relaxation ability, and eventually lead to the decrease of GWI, GCW, GWE and the increase of GWW [25]. The decrease of Hb can lead to the activation of the sympathetic nervous system, and the heart is in a state of overload for a long time, thus aggravating myocardial hypoxia. At the same time, the activation of renin–angiotensin–aldosterone system leads to the increase of peripheral circulatory resistance, which causes vasoconstriction and sodium retention, and then increases the volume load and pressure load of the left ventricle, and eventually leads to the decline of global cardiac function. Hiemstra et al. showed that the rhythm of myocardial contraction mainly affected GWW [26]. There was no significant difference in GWW and GWE between group B and group A, which may be due to the fact that although there was a certain degree of systolic dysfunction in mild IDA patients, the cardiac systolic function was still in the compensatory period, and the myocardial contraction rhythm was still synchronous, showing no significant difference in the overall futility of the left ventricle. Although the GCW decreased, the proportion of GWW in GWE was small, and there was no significant change in GWW.
In this study, GLS was positively correlated with GWI, GCW, and GWE, and negatively correlated with GWW, indicating that myocardial work parameters and GLS have a high agreement in evaluating LV systolic function. In addition, the results of this study also showed that the ICC of the global left ventricular myocardial work parameters GWI, GCW, GWW and GWE were all within and between observers. 0.75, indicating good reproducibility.
In our study, ROC curve analysis showed that GWI had the best diagnostic performance of each MW parameter for mild and moderate IDA, and the AUC of GWI was 0.783, indicating that GWI could accurately evaluate left ventricular systolic function in IDA patients. The best cut-off value of GWI for the diagnosis of left ventricular systolic dysfunction in IDA patients was 1763 mmHg %, with a sensitivity of 0.71 and a specificity of 0.78. In conclusion, LV-PSL can provide reference value for early detection of left ventricular systolic dysfunction in IDA patients with preserved left ventricular ejection fraction.
Limitations There are some limitations in this study: (1) the sample size is relatively small. Further studies with larger sample sizes are needed; (2) IDA patients were mostly young women. Therefore, the results may not generalize to other age groups and males; and (3) LV-PSL parameters are based on 2D measurements, whereas myocardial motion involves 3D multidirectional fibers, introducing spatial constraints.
Conclusion
Prolonged anemia induces LV remodeling and systolic dysfunction. Noninvasive LV-PSL allows early detection of altered myocardial mechanics in IDA patients with preserved LVEF. ROC analysis showed GWI has high AUC, sensitivity and specificity, outperforming other parameters for detecting LV systolic changes. This reproducible technique provides a new comprehensive imaging approach for early diagnosis and treatment efficacy assessment in IDA.
Methods
Study population
This prospective study enrolled consecutive IDA patients diagnosed at Heping Hospital Affiliated to Changzhi Medical College from March 2022 to June 2023. Inclusion criteria included: (1) Microcytic hypochromic anemia: adult males with Hb < 13 g/dl and adult females with Hb < 12 g/dl; erythrocyte morphology showing hypochromic manifestations: mean corpuscular volume (MCV) < 80fL; mean corpuscular Hb (MCH) level < 27 pg; and MHC concentration (MCHC) < 32%. (2) Clear iron deficiency etiology and clinical manifestations of iron deficiency anemia such as pallor, fatigue, fatigue, lethargy, dizziness, and tinnitus. (3) LVEF > 50%. (4).No regular anemia treatment. Exclusion criteria were: (1) history of hypertension, coronary atherosclerosis, myocardial infarction, congenital heart disease, significant heart valve disease, valvular stenosis or greater than mild valvular regurgitation affecting left ventricular systolic function, (2) cardiac injury due to hyperlipidemia, diabetes, hyperthyroidism, and cirrhosis, (3) severe arrhythmia or heart rate > 100 beats/min, (4) pregnant patients, and (5) incomplete clinical data or poor echocardiographic image quality. According to the diagnostic guidelines for iron deficiency anemia, all patients with iron deficiency anemia were diagnosed by the hematologist’s doctor, obstetrician and gynecologist, and gastroenterologist. There were 41 patients with gynecological diseases, such as uterine fibroids, endometriosis, and increased menstrual bleeding, 15 patients with digestive system diseases such as gastroduodenal ulcer, gastric polyps, and subtotal gastrectomy, and 6 patients with IDA of malnutrition. Finally, 62 IDA patients were included (male to female ratio 1∶4.2; mean age, 38.76 ± 8.59 years. disease duration, 1–20 years). In addition, 33 healthy controls undergoing physical examination were enrolled (male to female ratio 1:2.3; mean age, 43.9 ± 15.2 years) after confirming no abnormalities on history, examination, electrocardiography, echocardiography, and laboratory tests.
The 62 IDA patients were further divided into two groups by Hb level: Group B (n = 30, adult males 9 g/dL < Hb < 13 g/dL, adult females 9 g/dL < Hb < 12 g/dL; mean age, 44.4 ± 9.1 years; disease duration, 1 year to 20 years), Group C (n = 32, 6 g/dL ≤ Hb ≤ 9 g/dL; mean age, 44.8 ± 8.1 years; disease duration, 1 year to 15 years).
The study was approved by the Ethics Committee of Heping Hospital Affiliated to Changzhi Medical College (CMZC-2022-03-07-S15), and all subjects provided informed consent before participation.
Transthoracic echocardiogram
All echocardiographic images were acquired using a GE Vivid E95 color Doppler diagnostic ultrasound machine equipped with an M5S probe, and the images were acquired and analyzed by two sonographers with more than 5 years of experience. First, all subjects were placed in the left lateral position in a stationary resting state. At the same time, the electrocardiogram was connected to measure the brachial artery blood pressure of the bilateral upper limbs by the cuff method, and the bilateral mean value was calculated. All sections were acquired with reference to the recommendations of the American Society of Echocardiography Dynamic acquisition was performed after the images were stabilized for display, and apical four-chamber, three-chamber, and two-chamber images were stored for at least three or more consecutive cardiac cycles, with the frame rate and depth of the acquisition to be consistent [14]. Left ventricular end-diastolic diameter (LVDd), left ventricular end-systolic diameters (LVDs), interventricular septal end-diastolic thickness (IVSD), and left ventricular posterior wall end-diastolic thickness (LVPWD) were measured on parasternal left ventricular long-axis views, and peak early diastolic mitral inflow velocities (E) and peak late diastolic mitral inflow velocities (A) were measured on apical four-chamber cardiac views using Doppler ultrasound, along with the velocity of early diastolic tissue motion in the left ventricular septum and the lateral mitral annulus velocities, and E/A and E/mean e' were calculated. Left ventricular end-diastolic volume (LVEDV), left ventricular end-systolic volume (LVESV) and left ventricular ejection fraction (LVEF) were measured in the standard apical four-chamber and two-chamber views using the modified biplanar Simpson method.
Image analysis for ventricular global longitudinal strain and myocardial work
The acquired dynamic images were imported into Echopac version 203 for image analysis, and the apical three-sectional images were sequentially selected to enter the automatic functional imaging (AFI) analysis mode. The endocardial boundaries were traced according to the prompts to create the region of interest, and the software displayed the results of the automatic tracking. Where the tracing is unsatisfactory, the tracing points can be slightly adjusted manually, and the system can automatically provide the global longitudinal strain (GLS) of the left ventricle, which is the average of the peak strains of the 17 segments, and the GLS cannot be estimated if two or more segments are excluded. The myocardial work (MW) mode is then entered, and after inputting the brachial cuff pressure the timing of valvular events is determined on the apical three-chamber cardiac section: aortic valve closure time (AVC), aortic valve opening time (AVO), mitral valve opening time (MVO), and mitral valve closure time (MVC). The software automatically constructed LV-PSL curves and global myocardial work index (GWI), global constructive work (GCW), global wasted work (GWW), and global work efficiency (GWE).
Intra- and inter-observer variability
To assess intra- and inter-observer variability, 25 subjects were randomly selected from the three groups. Two experienced attending physicians independently performed repeated measurements of all myocardial work parameters to determine inter-observer variability. The same physicians repeated the measurements after a 7-day interval to determine intra-observer variability. Intra- and inter-observer variability were expressed as intraclass correlation coefficients (ICCs).
Statistical analysis
Statistical analysis was performed using SPSS Statistics version 26 (IBM SPSS Inc., Chicago, USA). Normally distributed continuous data were expressed as mean ± standard deviation. Differences among the three groups were analyzed by one-way ANOVA, and Post-hoc analysis between groups was conducted using either the LSD-t test when the variances were equal or, the Dunnett's t test when the variances were unequal. Non-normally distributed data were expressed as median and interquartile range and compared among groups using the Kruskal–Wallis H test. Post-hoc pairwise comparisons were adjusted using the Bonferroni method. Correlation between variables was assessed using Pearson’s or Spearman’s coefficients as appropriate. Receiver operating characteristic (ROC) curves were constructed to determine optimal sensitivity and specificity of myocardial work parameters. Optimal thresholds were estimated using Youden’s index. P < 0.05 was considered statistically significant.
Availability of data and materials
No data sets were generated or analysed during the current study.
References
Safiri S, Kolahi AA, Noori M, et al. Burden of anemia and its underlying causes in 204 countries and territories, 1990–2019: results from the global burden of disease study 2019. J Hematol Oncol. 2021;14(1):185.
Kumar SB, Arnipalli SR, Mehta P, et al. Iron deficiency anemia: efficacy and limitations of nutritional and comprehensive mitigation strategies. Nutrients. 2022;14(14):2976.
McLean E, Cogswell M, Egli I, et al. Worldwide prevalence of anaemia, WHO vitamin and mineral nutrition information system, 1993–2005. Publ Health Nutr. 2009;12(4):444–54.
Myles PS, Richards T, Klein A, et al. Rationale and design of the intravenous iron for treatment of anemia before cardiac surgery trial. Am Heart J. 2021;239:64–72.
Moliner P, Enjuanes C, Tajes M, et al. Association between norepi-nephrine levels and abnormal iron status in patients with chronicheart failure: is iron deficiency more than a comorbidity? J Am Heart Assoc. 2019;8(4): e010887.
Savarese G, Jonsson A, Hallberg AC, et al. Prevalence of, associalions with, and prognostic role of anemia in heart failure across the ejection fraction spectrum. Int J Cardiol. 2020;298:59–65.
Zhou Q, Shen J, Liu Y, et al. Assessment of left ventricular systolic function in patients with iron deficiency anemia by three-dimensional speckle-tracking echocardiography. Anatol J Cardiol. 2017;18(3):194–9.
Suryani LD, Raharjo SB, Sagita R, et al. Oral ferrous sulphate improves functional capacity on heart failure patients with iron deficiency anemia. Glob Heart. 2022;17(1):81.
Mei Z, Chen J, Luo S, et al. Comparative efficacy of intravenous and oral iron supplements for the treatment of iron deficiency in patients with heart failure: a network meta-analysis of randomized controlled trials[J]. Pharmacol Res. 2022;182: 106345.
Cui C, Li Y, Liu Y, et al. Association between echocardiographic non-invasive myocardial work indices and myocardial fibrosis in patients with dilated cardiomyopathy. Front Cardiovasc Med. 2021;8: 704251.
Li Y, Zheng Q, Cui C, et al. Application value of myocardial work technology by non-invasive echocardiography in evaluating left ventricular function in patients with chronic heart failure. Quant Imag Med Surg. 2022;12(1):244–56.
Luo X, Ge Q, Su J, et al. Normal ranges of non-invasive left ventricular myocardial work indices in healthy young people. Front Pediatr. 2022. https://doi.org/10.3389/fped.2022.1000556.
Lin J, Wu W, Gao L, et al. Global myocardial work combined with treadmill exercise stress to detect significant coronary artery disease. J Am Soc Echocardiogr. 2022;35(3):247–57.
Mitchell C, Rahko PS, Blauwet LA, et al. Guidelines for performing a comprehensive transthoracic echocardiographic examination in adults: recommendations from the American society of echocardiography. J Am Soc Echocardiogr. 2019;32(1):1–64.
Paolillo S, Scardovi AB, Campodonico J, et al. Role of comorbidities in heart failure prognosis part I: anaemia, iron deficiency, diabetes, atrial fibrillation. Eur J Prev Cardiol. 2020;27:27–34.
Siddiqui SW, Ashok T, Patni N, et al. Anemia and heart failure: a narrative review. Cureus. 2022;14(7): e27167.
Manceau H, Ausseil J, Masson D, et al. Neglected comorbidity of chronic heart failure: iron deficiency. Nutrients. 2022;14(15):3214.
Parcha V, Patel N, Kalra R, et al. Clinical, demographic, and imaging correlates of anemia in heart failure with preserved ejection fraction (from the RELAX trial). Am J Cardiol. 2020;125(12):1870–8.
Ernande L, Bergerot C, Girerd N, et al. Longitudinal myocardial strain alteration is associated with left ventricular remodeling in asymptomatic patients with type 2 diabetes mellitus. J Am Soc Echocardiogr. 2014;27(5):479–88.
Roemer S, Jaglan A, santos D, et al. The utility of myocardial work in clinical practice. J Am Soc Echocardiogr. 2021;34(8):807–18.
Russell K, Eriksen M, Aaberge L, et al. Assessment of wasted myocardial work: a novel method to quantify energy loss due to uncoordinated left ventricular contractions. Am J Physiol Heart Circ Physiol. 2013;305(7):H996–1003.
Hubert A, Le Rolle V, Leclercq C, et al. Estimation of myocardial work from pressure-strain loops analysis: an experimental evaluation. Eur Heart J Cardiovasc Imag. 2018;19(12):1372–9.
Chvapil M, Hurych J, Ehrlichova E, et al. The effect of iron deficiency on the synthesis of collagenous and non-collagenous proteins in wound granulation tissue and in the heart of rats. Exp Med Surg. 1968;26(1–2):52–60.
Elçioğlu BC, Baydar O, Kilic A, et al. Effects of iron deficiency on left ventricular functions in young women regardless of anemia: A speckle tracking echocardiography study. Turk J Med Sci. 2022;52(3):754–61.
Altman M, Bergerot C, Aussoleil A, et al. Assessment of left ventricular systolic function by deformation imaging derived from speckle tracking: a comparison between 2D and 3D echo modalities. Eur Heart J Cardiovasc Imag. 2014;15(3):316–23.
Hiemstra YL, van der Bijl P, El Mahdiui M, et al. Myocardial work in nonobstructive hypertrophic cardiomyopathy: implications for outcome. J Am Soc Echocardiog. 2020;33(10):1201–8.
Acknowledgements
Not applicable.
Funding
Four “Batches” Innovation Project of Invigorating Medical through Science and Technology of Shanxi Province (2022XM19).
Author information
Authors and Affiliations
Contributions
Performed the literature review: XXC and MJ; carried out echocardiography measurements: XXC, MJ, LYR, XNH, and QFS; selected participants and collected the clinical data: XXC, MJ, LYR, and XNH; checked the validity of data: XXC, MJ, LYR, and XNH; data analysis: XXC, MJ, and XNH; wrote the manuscript: XXC and MJ; prepared the manuscript: XXC, MJ, and XYW; supported the experiments financially: QFS and XYW; checked the paper: KFL and XYW. All authors have checked and confirmed the paper. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by Heping Hospital Affiliated to Changzhi Medical College.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cui, X., Jing, M., Ren, L. et al. Evaluation of left ventricular systolic function in patients with iron deficiency anemia based on non-invasive left ventricular pressure–strain loops. BioMed Eng OnLine 23, 82 (2024). https://doi.org/10.1186/s12938-024-01276-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12938-024-01276-2