
Abstract
Background
Epidemiological studies of long-term exposure to outdoor air pollution have consistently documented associations with morbidity and mortality. Air pollution exposure in these epidemiological studies is generally assessed at the residential address, because individual time-activity patterns are seldom known in large epidemiological studies. Ignoring time-activity patterns may result in bias in epidemiological studies. The aims of this paper are to assess the agreement between exposure assessed at the residential address and exposures estimated with time-activity integrated and the potential bias in epidemiological studies when exposure is estimated at the residential address.
Main body
We reviewed exposure studies that have compared residential and time-activity integrated exposures, with a focus on the correlation. We further discuss epidemiological studies that have compared health effect estimates between the residential and time-activity integrated exposure and studies that have indirectly estimated the potential bias in health effect estimates in epidemiological studies related to ignoring time-activity patterns.
A large number of studies compared residential and time-activity integrated exposure, especially in Europe and North America, mostly focusing on differences in level. Eleven of these studies reported correlations, showing that the correlation between residential address-based and time-activity integrated long-term air pollution exposure was generally high to very high (R > 0.8). For individual subjects large differences were found between residential and time-activity integrated exposures. Consistent with the high correlation, five of six identified epidemiological studies found nearly identical health effects using residential and time-activity integrated exposure. Six additional studies in Europe and North America showed only small to moderate potential bias (9 to 30% potential underestimation) in estimated exposure response functions using residence-based exposures. Differences of average exposure level were generally small and in both directions. Exposure contrasts were smaller for time-activity integrated exposures in nearly all studies. The difference in exposure was not equally distributed across the population including between different socio-economic groups.
Conclusions
Overall, the bias in epidemiological studies related to assessing long-term exposure at the residential address only is likely small in populations comparable to those evaluated in the comparison studies. Further improvements in exposure assessment especially for large populations remain useful.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Air pollution has been associated with a range of adverse health effects [59]. Outdoor air pollution is the most important environmental exposure in the Global Burden of Disease assessments [8]. The evidence for these burden of disease assessments derives primarily from epidemiological studies, especially on long-term air pollution exposure that is particularly important in terms of health. A Panel appointed by the Health Effects Institute (HEI) has recently reviewed epidemiological studies of traffic-related air pollution, addressing exposure assessment issues in detail [4, 18]. The Panel primarily assessed how well specific methods assessed the outdoor concentration and how well outdoor exposure was assigned to the residential address, e.g. by assessing the spatial resolution of the exposure surfaces and addresses. Virtually all studies assigned outdoor concentrations to the residential address only [18], a few studies in children incorporated exposures at the school address. Even fewer studies in adults have incorporated work address in the exposure assessment.
Environmental health researchers have understood for decades that the true personal exposure to air pollution is experienced in multiple so-called micro-environments [15, 41]. Personal exposure can be assessed by direct personal exposure monitoring or indirectly by assessing concentrations in key micro-environments and obtaining time-activity data [15]. There is a large exposure science literature on both approaches. However, in large epidemiological studies neither direct nor indirect personal exposure have often been assessed. The main reason for this is that personal exposure monitoring is too costly to perform in a large number of subjects and that assessing long-term exposure requires a fair number of repeated samples per subject. Indirect exposure assessment is also not applied often, because most epidemiological studies do not have information on where people spend time other than the home location. Post-hoc time-activity diaries are also prohibitive in large cohort studies and not feasible in retrospective cohort studies. The lack of time-activity data beyond the residential address is related to the fact that very few cohort studies, which have been used in air pollution epidemiology, have been primarily designed to investigate health effects of air pollution. In the recent large studies based on administrative databases, information on residential address is also typically the only location data available [13, 55]. The few studies that were designed to investigate outdoor air pollution and did obtain more detailed data on work or school address, include the SAPALDIA study in Switzerland and the PIAMA birth cohort study in the Netherlands [32, 61].
Epidemiological studies on air pollution and other environmental exposures have been criticized for not taking time-activity patterns into account [24, 42, 56]. Residence-based exposure assessment is generally criticized because of the fact that air pollution differs in space and people spend a sizable amount of time outside their home. This is occasionally documented with anecdotal figures of individual subject’s exposure data along specific tracks, showing large variability depending on location and time [58]. We note that this alone is insufficient to make strong statements about potential bias in epidemiological studies as the documented exposure contrasts are not the contrasts used in epidemiological studies: what is used is the contrast in long-term average (e.g., annual average) concentrations across individuals. Furthermore, major air pollutants including fine particles have been shown to infiltrate efficiently into homes [20]. While it is understandable that epidemiological studies have relied on the residential address, the questions remain as to how poorly exposure is assessed and how much bias is potentially introduced in health effect estimates by focusing on the residential address only.
The objective of this paper is to review studies that have evaluated how air pollution exposures assessed at the residence only compare with exposures that integrate time-activity patterns. Our second objective is to review studies that have evaluated the potential bias of using residential exposure assessment in epidemiological studies of long-term air pollution exposure.
Main text
Methods
Review methods
We built on a previous review discussing methods for long-term air pollution exposure assessment in which the issue of residential exposure assessment was addressed [19]. We added more recent studies by searching in the database Pubmed with the search terms “mobility”, “static exposure”, “dynamic exposure”, “personal exposure”, “residential exposure” AND “air pollution” OR “air pollutants”. We limited the search to studies in humans and in the English language. The search was conducted February 15, 2024. In addition, we reviewed the reference lists of identified papers. We treat the following exposure-related terms used by researchers in the identified papers as synonymous: a) dynamic, mobility enhanced, integrated, time-activity integrated and personal exposure, and b) static, home-based and residential exposure.
Methods to assess time-activity patterns and dynamic exposures
We can compare residential exposure with directly measured personal exposure or indirectly assessed personal exposure based on validation studies. The literature using directly measured personal exposure as a validation metric is small and difficult to interpret [35, 38]. In these studies, statistically significant but weak associations between long-term outdoor and personal exposure were found. The main problem for the interpretation is the difficulty in obtaining a sufficiently large number of measurements per person for a large group of subjects to credibly assess long-term personal exposure. A second reason is that measured personal exposure of e.g., PM2.5 and NO2 includes both outdoor and indoor sources, which are difficult to separate. This is in sharp contrast to personal exposure validation studies of short-term air pollution, which have convincingly documented that the temporal variation at a single outdoor site correlates well with temporal variations in personal exposure [5]. The spatial comparison is much more complicated, see the IARC monograph on outdoor air pollution for a discussion [20]. In the remainder of this review, we focus on studies comparing residential exposure with indirectly assessed personal exposure.
Obtaining information on time-activity patterns of individuals to calculate personal exposure as a weighted sum of time spent in different micro-environments, and the concentration in that micro-environment, is also challenging. Key micro-environments for air pollution exposure are the residence, work or school location and commuting route [10]. We identified three approaches to assess time-activity patterns that have been applied in the framework of exposure assessment and epidemiological studies. First, agent-based modelling has been applied to simulate individual time-activity, typically based upon existing survey data [29, 37]. In most applications, the actual individual work or school address is not known. This approach can be applied to large populations. Second, tracking studies have been performed in which volunteers carried a GPS tracker or smartphone App to empirically determine time-activity patterns [30, 31, 60]. Tracking studies are typically studies in small population groups (several hundred at most) and cover a limited amount of time, often one to two weeks because of the demand on the participants’ time. Third, a few epidemiological studies, designed to assess environmental exposures such as air pollution and noise, have collected information on the school or work address, including a large Canadian cohort using census data [7] and a study in Southern-Californian children [33]. While these studies did not formally obtain full time-activity patterns, notably not capturing mobility between these locations and leisure time activities, we included these studies as school and work cover major micro-environments for children and working-age adults.
Studies have compared residence-based exposure and indirectly assessed personal exposure in different ways. Some studies compared the level and contrast of exposure [29, 31]. One of the first empirical tracking studies compared the contribution of the residential environment to the time-integrated exposure with that of other micro-environments [10]. As the primary focus of our review is application in epidemiological studies, an important comparison metric is the correlation between residence-based exposure and indirectly assessed personal exposure. The correlation is a very important metric because in epidemiological studies we compare the health status of individuals with high and low exposures, typically on a continuous scale. If the correlation is low, we may anticipate different associations with health depending on whether exposure is assessed at the residence only or with time-activity integrated. In the case of classical exposure measurement error, we typically expect a downward bias of effect estimates in epidemiological studies [49]. We included studies if they reported correlations or directly assessed the possible bias in epidemiological studies. We additionally evaluated the difference in contrasts and absolute levels between residence-based and indirect personal exposure. In the case of a high correlation between the two exposure estimates, higher health effect estimates may be obtained when using an exposure metric with a smaller contrast. Finally, we evaluated the epidemiological studies that directly compared health effect estimates using residential and time-activity integrated exposures.
Time-activity surveys
Time-activity surveys have shown that people spend about 60–70% of their time in their own home environment, with differences between population groups and individuals [20, 26]. In two large North American surveys (Canada and USA), people (including adults and children) spent 65–66% in the home, 10% at work/school and 6% outdoors [26]. Children spent about 6–8% more time at home in both cohorts [26]. In a large German survey of children, children spent 15.5 h per day at home, 4.75 in other indoor locations and 3.6 h outdoors [9]. In a large survey of 100,000 people in Los Angeles county, USA, the population spent 66% of their time in their home (workers 60% and non-workers 72%) [28].
Results
Figure 1 shows the selection of studies. The search resulted in 2139 abstracts to be screened, of which the full text of 107 were assessed for eligibility. In total, 29 studies were included in the review for quantitative comparisons. Exclusions were related to No comparison of residence-based and dynamic exposure (n = 45), Papers addressing residential moving in typically birth cohort studies (n = 14) and papers on short-term personal exposure (n = 19). Of the 45 excluded studies, some were used in the supporting text.

Flowchart of selection of studies for quantitative comparison of residence-based and dynamic air pollution exposure
Comparison between residential and time-activity integrated exposure level and contrast
Table 1 shows the identified studies that analyzed the relationship between residential address-based exposure and time-activity integrated exposure assessment. Studies were primarily conducted in North America and Europe, with three studies from China.
Exposure levels were generally only modestly different between residential and dynamic exposure assessment methods on a population average level, with residential exposure being higher in some studies and lower in other studies (Table 1). Exposure was on average higher in Canada when the work address was incorporated in the exposure assessment compared to the residential address alone, as work addresses were within locations that on average had higher PM2.5 concentrations [7]. A study in the New York City region, USA, showed significantly different population weighted PM2.5 exposures in 71 districts between active and home scenarios, although differences were small in absolute terms (-0.26 to 0.73 μg/m3), [39]. In studies in Boston, USA and the Netherlands, mean levels were similar for static and dynamic exposures [36, 40]. In a study in Montreal, Canada, almost 90% of the population had a higher integrated NO2 exposure compared to the residential exposure [52]. In another study in Montreal, NO2 and UFP exposures were lower for dynamic exposures of UFP and NO2 and nearly identical for PM2.5 [16]. Substantially larger mobility-integrated exposures compared to residential exposures were found for UFP and BC in Toronto, Canada related to commuting exposures [53]. Residential exposures of 106 participants in a study in Beijing were higher compared to mobility-based exposures, both on low and high pollution days [30]. All subjects lived in a highly polluted neighborhood and therefore mobility resulted in lower mobility-integrated exposures [30]. A study in Hong-Kong found lower dynamic exposures for PM2.5 and BC and higher dynamic exposures for NO2 [58]. A study in the UK found a small increase in population weighted NO2 and PM2.5 exposures when including exposure at the work address (2 and 0.3% respectively) [46].
Almost none of the studies incorporated differences between indoor and outdoor concentrations, related to infiltration into homes, schools or offices. A study in Hong-Kong found that if infiltration indoors was taken into account, dynamic exposures were on average about 20% lower than residential exposures because infiltration of outdoor air pollution was more efficient in residences than in commercial buildings [58]. A study in London found that dynamic exposure accounting for infiltration and commuting was lower than residential outdoor concentrations [54]. The mean dynamic exposure to outdoor sources was estimated to be 37% lower for PM2.5 and 63% lower for NO2 than at the residential address. These decreased estimates reflect the effects of reduced exposure indoors (with mean infiltration assumed to be 0.31 for NO2 and 0.56 for PM2.5), the large amount of time spent indoors (95–98%) and the mode and duration of travel in London [54]. A study in schoolchildren in five European cities, found that after taking into account time-activity patterns, exposures at school and in traffic and infiltration, residential outdoor PM2.5 concentrations were on average 26% higher than the integrated exposure [23]. In the models, infiltration factors were 0.66 and 0.82 for residences and schools in the four South-European cities and 0.55 for residences for the Finish city. Children spent 87% and 91% indoors in the South-European cities and Kuopio, Finland respectively [23]. A study in Beijing, reported an annual mean outdoor PM2.5 concentration of 87.6 μg/m3 versus a 47.5 μg/m3 average personal exposure, calculated based on an assumed mean infiltration factor of 0.47 (Shi, 2017). Studies furthermore did not take indoor sources into account, which is reasonable if the interest is in outdoor-generated pollution.
Overall, differences between studies are related to differences in locations where people live and work. Commuting exposures are, in general, especially higher for traffic-related pollutants such as NO2 and UFP, but most people spend only a small amount of time in traffic. A study in Israel found that the contribution of high NO2 concentration during commute to the overall, integrated exposure, was small [51].
Variability in dynamic exposure levels was lower compared to residential based exposure in almost all studies (Table 1). In most studies the difference in exposure contrast was small to moderate. The explanation for the smaller dynamic exposure contrast is probably related to the phenomenon that subjects living at the highest exposed locations likely work at less exposed locations and vice versa. Kim and Park (2021) argued that this pattern is common and use the term neighborhood effect averaging, distinguishing upward and downward averaging [22]. Subjects living in the suburbs or towns near the city are more likely to work in higher polluted urban centers. The reverse pattern is less likely, however subjects living in local hotspots such as major roads may work in more urban background conditions. In the Montreal study, plots of the difference between the dynamic and residential exposure show that dynamic exposure was higher for those with low residential exposure levels and lower for those with high residential concentrations [16]. In the NYC study, boxplots comparing residential and integrated exposures by district reveal that the majority of districts have a lower integrated exposure compared to residential exposure, except for one district with a very low residential exposure and the highest integrated exposure [39].
Several studies have investigated determinants of the difference between dynamic and residential exposures. In a study in Paris, France, the difference between dynamic and static exposure was larger for deprived neighborhoods [3]. The locations where people work likely differ by socio-economic group, e.g., because offices and industrial facilities are located in different places. Exposure contrasts between urban and rural areas were different for residential exposure and time-weighted average exposure including the work address [7]. The exposure contrast between major streets and urban background in the city of Utrecht was smaller for dynamic exposure than for residential exposure [29]. In a detailed analysis of residential and mobility-enhanced exposures of UFP, NO2 and PM2.5 in Montreal, Canada, various built-environment characteristics (e.g. income, unemployment rate, major road length, walkability) at the neighborhood level and smaller predicted differences for individuals, though with only small differences in the overall average between residential and mobility exposures [16]. In a study in Los Angeles, USA, the overall average static and dynamic PM2.5 exposure was identical, but for individual subjects larger differences occurred e.g. for those living in a low pollution neighborhood and working in a high pollution area and vice versa, related to socio-economic factors [28]. The difference was larger for those travelling more than 20 miles between home and work, if these two locations differed in exposure [28]. In a large study in US workers, disparities between different population groups by race, income, age and urbanicity were larger when the work address was taken into account [11].
Several studies have found differences in population exposure distributions across neighborhoods or districts depending on using residential or dynamic exposures, related to where people predominantly work and live [39]. In studies in Belgium and the UK, researchers found that NO2 exposure differed when considering the working-hour and night-time population distribution [2, 14, 46]. In the UK study, population-weighted NO2, PM2.5 and O3 exposures were on average 2%, 0.3% and -0.3% higher when the workday-population distribution was taken into account [46]. Population exposures differed between daytime and nighttime, partly because many areas are predominantly residential or areas where a large number of people work.
These observations may be very useful for overall population exposure assessment and subsequent risk or health impact assessment. However, in epidemiological studies we need to know the exposure of individuals, and especially the correlation between the residential and more refined exposure estimates incorporating time-activity patterns.
Correlation between residential and time-activity integrated exposures
Eleven studies reported on the correlation between residential and time-activity integrated exposure. The correlation between residential address-based and dynamic long-term air pollution exposure was generally high to very high (Table 1). This holds both for studies that simulated the time spent in locations other than the home based on agent-based modelling and for studies that had access to the actual individual time-activity patterns. Studies have been performed in adults and children and in different settings (Netherlands, France, Canada, Switzerland, USA, United Kingdom and China). While the overall correlation is high for the full population, large differences may occur for individual subjects as illustrated in the Montreal study [16]. The agreement between residential and mobility-enhanced exposure was less for UFP than for NO2 and PM2.5 in the Montreal study (correlation coefficient not reported). In a study in Israel, the correlation was high for working-age adults (R2 = 0.64) and very high for school children (R2 = 0.89) [50]. In the Israel study, the correlation was lower for commuters than for non-commuters: R2 = 0.56 vs R2 = 0.68 for the adults and R2 = 0.86 vs R2 = 0.94 for the children [50].
In London, correlations differed between commuting mode, despite the small percentage of time spent in travel (1–4%) and the large percentage of time indoors (95–98% across populations) [54]. Across the population, high correlations were found between dynamic exposure including infiltration into homes and offices and residential exposure for non-commuters and those using active travel (R = 0.91 and 0.77 for NO2), while only moderate correlations were reported for those using inactive travel (R = 0.57 for NO2, affected by the high concentrations assumed in the London underground) [54].
The generally high correlations between residence-based exposure and time-activity integrated exposure is probably due to the relatively large time fraction spent at home and the correlation between exposure at home and other micro-environments.
One of the first empirical tracking studies compared the contribution of the residential, work and commuting environment to overall exposure [10]. In 36 subjects in Barcelona, Spain the tracking-based study documented that subjects spent about 70% of their time in their residence, and the residence contributed 54% to the personal exposure to NO2. In a large study in Southern California, USA, people spent 66% of their time in their own home, which contributed 61% of the overall PM2.5 exposure [28].
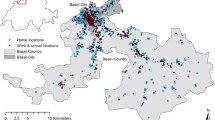
Several studies reported that the exposure at the residence correlated with the exposure at school or work, the two other major micro-environments where people spend time [36, 45]. In the Swiss study including 680 adults and children in the cantons of Basel-Stadt (i.e. “Basel city”) and Baselland (i.e. “Basel country” with towns, villages and rural areas), the correlation between residential and work and commuting exposure were 0.48 and 0.69 respectively. In the Dutch study of school-age children, correlations for NO2 between residential and estimated school and travelling exposures were 0.92 and 0.92 (0.90 and 0.88 for PM2.5) [36]. The correlation between residential and actual school exposures was nearly identical (0.89). Therefore, the residential exposure estimate also contains some information on the exposure in other locations, because children tend to go to a school near their home. Adults also on average tend to work relatively close to their home. Given the moderate correlation, the residential exposure clearly does not perfectly predict exposure elsewhere, but it does add information in addition to the time actually spent at home.
In the PIAMA cohort study, information about the actual school address was available. The estimated and actual exposure at school were highly correlated (R = 0.93) [36], providing support for the estimation methods. The 24-h integrated exposure incorporating the actual and the integrated exposure using the assumed school was very highly correlated (R = 0.995).
Comparison of health effect estimates in epidemiological studies
Table 2 shows epidemiological studies comparing health effect estimates of residential and time- activity integrated exposures. Consistent with the high correlation between residential and time-activity integrated exposures, health effects estimated from both approaches were nearly identical in five of the six studies. The sixth study used a difficult to interpret exposure metric (exposure in a 1600 m buffer) to represent residential exposure.
In a large Canadian administrative cohort with over ten million person-years of follow-up, significant associations of long-term PM2.5 exposure with natural mortality were found with both residential and time-weighted average exposure of residential and work address [7]. The actual work address was reported in the census questionnaire. Hazard ratios (HRs) were almost the same for the two exposure metrics, both in the full cohort and the cohort of people reporting that they commuted to work. Furthermore, no association with mortality was found when only the exposure at the work address was used. This observation agreed with a study in the Health Professionals cohort in the USA, in which no association with mortality was found for work address PM2.5 [44]. The lack of association with air pollution at the work address in two studies could be related to a combination of the reduced time spent at work or less infiltration of ambient particles into the occupational environment. A study in Hong-Kong indeed reported lower infiltration ratios for commercial buildings than for residences and schools [58]. For PM2.5, infiltration ratios were 0.82, 0.40 and 0.92 for residences, commercial buildings and schools, respectively. For NO2 differences in infiltration were much smaller [58]. More work is needed to assess how general this finding is.
In a study in 700 Dutch primary school children aged 8 years, associations between long-term exposure to PM2.5, NO2 and PM2.5 absorbance with lung function were similar for residential and time-activity integrated exposure, based on agent-based modelling [36]. Health effect estimates were nearly identical when the estimated and the actual school location were used in the exposure assessment.
In a study of 500 adults in San Diego, USA, PM2.5 and NO2 were associated with some cardio-metabolic markers for dynamic exposures only [27]. For the residential exposure, no associations were found. However, exposure was characterized as the average exposure in a 1600 m buffer around the address, thus neglecting fine-spatial resolution variations in outdoor concentrations. As the actual exposure to outdoor generated air pollution largely occurs indoors, the focus on characterizing residential outdoor air pollution in the immediate vicinity to the home, instead of a large buffer around it, in virtually all epidemiological studies seems more appropriate.
In a study in 140 adults living near a major interstate in the Greater Boston area (USA) or in a control neighborhood farther away from the interstate, associations of long-term exposure to UFP with the inflammation markers C-Reactive Protein and Interleukin-6 were weak with both home-based and mobility-integrated exposures derived from a detailed (15-min resolution) time-activity diary [25].
In a cohort study of 2,497 kindergarten and first-grade children of the Southern California Children’s Health Study (USA), incident asthma was associated with both home and school exposure to traffic-related air pollution obtained from a line source dispersion model [33]. A time-weighted average exposure at home and school gave almost identical relative risks compared to the residential exposure.
In a tracking study of 392 Dutch adults (18–65 years), sampled from a large representative survey by Statistics Netherlands, depressive symptoms from a standard questionnaire were not significantly associated with PM2.5 exposure estimated at the residential address and with mobility integrated [47]. The authors did find a significant negative association with green space, both for residential and mobility-integrated exposure [47].
Two further studies combined school and residential exposure, but did not report a comparison with residential only exposure [17, 34]. Both studies did not find an association with asthma.
Bias in epidemiological studies calculated from exposure validation studies
Table 3 shows the six studies that estimated the potential bias related to assessing exposure at the residential address only. Consistent with the high correlation and the small differences in effect estimates found in epidemiological studies, these six studies generally showed small to moderate bias in estimated exposure response functions, assuming classical error [11, 28, 40, 49] (Ragettli, 2015; Yu, 2020). The specific formula used in these studies was:
where
The bias factor expresses the degree to which a health effect is underestimated, e.g., a bias factor of 0.7 implies that the theoretical true risk is underestimated by 30%.
The Setton [49] study evaluated potential bias by comparing residential address only NO2 exposure and an indirect personal exposure integrating work and commuting exposures using simulations in Vancouver based on a Canadian time-activity survey and actual individual-level time-activity data in a Southern California time survey of 25,000 adults [49]. In the Vancouver analysis, 10,000 random draws of single locations from each of 382 census tracts were performed. In both settings, subjects who did not travel, or travelled within the same census tract, were not included in the analysis. This implies that the estimated bias overestimates the actual bias in a mixed population of commuters and non-commuters. Overall, the bias in Vancouver was moderate. However, the bias factor was larger when a more spatially varying surface was included in the analysis (0.70 for LUR compared to 0.84 for interpolated surface). The bias factor in Southern California was small (mean 0.93) but increased for those travelling longer distances from home to work and working more hours (Table 3). For those working 6–8 h and more than 40 km away from home, the bias factor was 0.70 and higher.
The study in Basel-Stadt and Baselland extracted information on commute routes, home, work and school locations from geo-coded 24-h time-activity diaries from the 2010 Swiss Mobility and Transport Microcensus [45]. This national telephone-based survey includes coordinates of origin and destination locations and geo-coded travel, including travel modes, duration and hour of the day. In the sample population, 76% of time was spent at home and 22% at work/school. The mean commute duration and distance of the study participants was 49 min and 14 km per day. The bias factor for assessing exposure at the residential address only was 0.87 when compared with the integrated home, work and commuting exposures. The largest contribution was from the work address exposure, as the bias factor was 0.88 when commuting was excluded.
A study in the greater Boston area, estimated work and home address location from mobile phone data for over 400,000 individuals [40]. A comparison of home-based and home-work time weighted exposures of PM2.5, linked from a fine resolution spatio-temporal LUR model, showed nearly identical mean exposures with moderately lower contrast in home-work exposure. The bias factor calculated assuming classical error was 0.91.
A study in Los Angeles County used agent-based modelling combined with PM2.5 concentrations estimated at 500 × 500 m resolution for a group of about 100,000 individuals [28]. A modest bias factor of 0.87 was found [28]. The bias factor indicated more bias for commuters (0.78) than for non-working people (0.95).
A study in Shenzhen using cell-phone data combined with exposure modelled at 3*3 km resolution, found that bias factor for NO2 and PM2.5 varied between 0.70 and 1 dependent on mobility across grids [62]. Bias factors below 0.8 were calculated for less than 5% of the population.
The six studies document small to moderate potential bias in epidemiological studies. We note that the impact of measurement error on effect estimates in reality is more complex and depends, for example, on the contribution of classical and Berkson error to the total error [48]. We thus view these calculations as an illustration of the potential bias. For the interpretation of these findings, the following observations are important.
First, the modelling and epidemiological studies that have integrated work or school address and commuting in the assessment of personal exposure have not considered all activity patterns, e.g. leisure time activities. These activities are more difficult to model. However, work and school are likely to be the key micro-environments beyond the home for a large part of the population (children and non-retired adults), based on time survey data. A study in Israel documented the largest discrepancy between residential and time-activity integrated exposure related to exposure during work time [51]. Furthermore, the studies based upon actual tracking and agent-based modelling including leisure time have found similar high correlations and effect estimates.
Second, in the current assessment, we have devoted little attention to indoor exposures. If the findings in the Hong Kong study of less infiltration of outdoor particles in the indoor environment of workplaces are more widely applicable [58], the residential environment would be even more important than the work environment for most (indoor) occupations.
Third, the potential bias may be outcome or age-group dependent, for example on whether we study childhood disease or adult morbidity or mortality. For the large body of literature on mortality effects of air pollution, the agreement for the elderly needs to be assessed. Residential exposure may be more closely related to personal exposure for this age group, though we lack the data to support this hypothesis.
Implications, generalizability and future work
The main implication of the high correlation between residence-based and estimated personal exposure is that epidemiological studies on long-term outdoor air pollution exposure are unlikely to have substantial bias related to exposure assessment. In particular, studies are unlikely to miss true associations. Consistently, six studies showed only moderate bias in effect estimates related to assumed classical exposure measurement error (Table 3). More directly, in five epidemiological studies the differences in effect estimates were small between residential and time-activity integrated personal exposure [7, 25, 33, 36, 47].
Effect estimates may differ if there is a sizable difference in exposure contrast between residential and dynamic exposure assessments, even if the correlation between the two metrics is high. However, most studies showed only a moderately smaller contrast in exposure for time-activity integrated exposure compared to residential exposure.
Because of the observation that differences between residential and personal exposure may differ between subgroups of the population, it is possible that subgroup analysis in epidemiological studies may be more affected than the overall effect estimate. No studies have empirically evaluated this. The same applies to health impact assessment based upon epidemiological evidence.
High correlations between residential and dynamic exposure have been found in a diversity of populations, in children and adults and in different countries. However, as illustrated for a Californian and Canadian population, the potential bias depends on specific characteristics of the population studied, including time spent out of the home, distance between home and work and the spatial variability of outdoor air pollution [49]. In the large Canadian cohort study, a distinction was made between commuting and non-commuting subjects (Christidis, 2019). Bias may be larger in settings with longer times spent out of the home and larger distances between home and work than in the studies evaluated in this review. For example, in specific populations such as truck drivers or aircraft personnel, the bias may be more substantial. For children with a long commute in previously polluting diesel-powered school busses, bias may also be more substantial than has been reported for the Dutch studies of children visiting schools in their own neighborhood. Hence, in cohort studies it is worthwhile to collect information on work / school address, commuting times and mode of transport. Tracking studies in smaller populations also remain useful for validation. It remains difficult to imagine the application of dynamic exposure assessment in the mega-cohorts based on administrative data [13, 55].
Despite the consistency across different study designs (exposure, epidemiology), further work on the comparison of health effect estimates in epidemiological studies is useful, particularly in different populations than those studied to date. In the studies calculating bias based on exposure comparisons, more sophisticated analyses, accounting for both classical and Berkson error would be useful.
The observed usefulness of the residential exposure furthermore does not imply that we should not address air pollution exposures elsewhere. Several studies in children have reported health effects related to outdoor air pollution exposure at school, including studies in the Netherlands [6, 21], Barcelona [1, 43, 57] and California [33]. These studies specifically measured air pollution exposures at and in the schools. In one study in children [43], inflammation markers and blood pressure were associated both with home and school-based exposure in the week prior to the health evaluation.
In population exposure assessment, it is likely useful to account for more than just the residential address. Studies showed that differences in exposure between different socio-economic groups were more pronounced for personal compared to residential exposure [3]. Hence in evaluating environmental injustice there is benefit in a broader exposure assessment approach. The level of exposure also generally differs between residential and personal exposure. It is not obvious that this in itself is of great interest as the judgement of health risks can only be based on residential outdoor levels, as this is the method used in the epidemiological studies forming the evidence base to assess health risks. When comparing different populations, time-integrated exposure may show a different pattern if people predominantly work in differently exposed locations e.g. people living in suburbs / rural towns working either in a major city center versus more rural places. Finally, in studies on the impact of interventions on commuting exposures will be less reflected at the residential address.
Conclusions
We found that the correlation between residential address-based and dynamic time-activity integrated long-term air pollution exposure was generally high to very high in diverse populations. Consistent with the high correlation, epidemiological studies found generally similar health effects using residential and dynamic exposure. Six additional studies showed only small to moderate bias in estimated exposure response functions using residence-based exposures, assuming classical error. Overall, the bias in epidemiological studies related to assessing long-term exposure at the residential address only is likely small in populations comparable to those evaluated in the reviewed studies.
Exposure studies did show generally modest differences in exposure level and exposure contrast, potentially affecting the magnitude of estimated health effects. The difference in exposure, however, is not equally distributed across the population including between different socio-economic groups, urban and rural populations and different neighborhoods. Further improvements in exposure assessment for epidemiological and health impact assessment studies, especially for large populations, remain highly useful. A limitation of the studies is that few considered indoor – outdoor relationships. Incorporation of infiltration of outdoor air pollutants may further improve exposure assessment.
Availability of data and materials
No datasets were generated or analysed during the current study.
Abbreviations
- GPS:
-
Geographical positioning system
- HR:
-
Hazard ratio
- NO2 :
-
Nitrogen dioxide
- PM2.5 :
-
Fine particles, particles smaller than 2.5 µm
- R:
-
Correlation coefficient
- UFP:
-
Ultrafine particles, particles smaller than 100 nm
References
Alvarez-Pedrerol M, Rivas I, López-Vicente M, Suades-González E, Donaire-Gonzalez D, Cirach M, de Castro M, Esnaola M, Basagaña X, Dadvand P, Nieuwenhuijsen M, Sunyer J. Impact of commuting exposure to traffic-related air pollution on cognitive development in children walking to school. Environ Pollut. 2017;231:837–44. https://doi.org/10.1016/j.envpol.2017.08.075.
Beckx C, Int Panis L, Arentze TA, Janssens D, Torfs R, Broekx S, Wets G. A dynamic activity-based population modelling approach to evaluate exposure to air pollution: methods and application to Dutch urban area. Environmental Impact assessment review 2009;179–185. https://doi.org/10.1016/j.eiar.2008.10.001.
Blanchard O, Deguen S, Kihal-Talantikite W, François R, Zmirou-Navier D. Does residential mobility during pregnancy induce exposure misclassification for air pollution? Environ Health. 2018;17:72. https://doi.org/10.1186/s12940-018-0416-8.
Boogaard H, Samoli E, Patton AP, Atkinson RW, Brook JR, Chang HH, Hoffmann B, Kutlar Joss M, Sagiv SK, Smargiassi A, Szpiro AA, Vienneau D, Weuve J, Lurmann FW, Forastiere F, Hoek G. Long-term exposure to traffic-related air pollution and non-accidental mortality: a systematic review and meta-analysis. Environ Int. 2023;176:107916.
Brauer M. How much, how long, what, and where: air pollution exposure assessment for epidemiologic studies of respiratory disease. Proc Am Thorac Soc. 2010;7:111–5. https://doi.org/10.1513/pats.200908-093RM.
Brunekreef B, Janssen NAH, de Hartog J, Harssema H, Knape M, van Vliet P. Air pollution from truck traffic and lung function in children living near motorways. Epidemiology. 1997;8:298–303.
Christidis T, Pinault LL, Crouse DL, Tjepkema M. The influence of outdoor PM(2.5) concentration at workplace on nonaccidental mortality estimates in a Canadian census-based cohort. Environ Epidemiol. 2021;5:e180. https://doi.org/10.1097/ee9.
Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K, Balakrishnan K, Brunekreef B, Dandona L, Dandona R, Feigin V, Freedman G, Hubbell B, Jobling A, Kan H, Knibbs L, Liu Y, Martin R, Morawska L, Pope CA 3rd, Shin H, Straif K, Shaddick G, Thomas M, van Dingenen R, van Donkelaar A, Vos T, Murray CJL, Forouzanfar MH. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. Lancet. 2017;389(10082):1907–18. https://doi.org/10.1016/S0140-6736(17)30505-6.
Conrad A, Seiwert M, Hünken A, Quarcoo D, Schlaud M, Groneberg D. The German Environmental Survey for Children (GerES IV): reference values and distributions for time-location patterns of German children. Int J Hyg Environ Health. 2013;216(1):25–34. https://doi.org/10.1016/j.ijheh.2012.02.004.
de Nazelle A, Seto E, Donaire-Gonzalez D, et al. Improving estimates of air pollution exposure through ubiquitous sensing technologies. Environ Pollut. 2013;176:92–9. https://doi.org/10.1016/j.envpol.2012.12.032.
de Souza P, Anenberg S, Makarewicz C, Shirgaokar M, Duarte F, Ratti C, Durant JL, Kinney PL, Niemeier D. Quantifying disparities in air pollution exposures across the United States using home and work addresses. Environ Sci Technol. 2024;58(1):280–90. https://doi.org/10.1021/acs.est.3c07926.
Dewulf B, Neutens T, Lefebvre W, Seynaeve G, Vanpoucke C, Beckx C, Van de Weghe N. Dynamic assessment of exposure to air pollution using mobile phone data. Int J Health Geogr. 2016;15:14. https://doi.org/10.1186/s12942-016-0042-z.
Di Q, Dominici F, Schwartz JD. Air Pollution and Mortality in the Medicare Population. N Engl J Med. 2017;377(15):1498–9. https://doi.org/10.1056/NEJMc1709849.
Dons E, Van Poppel M, Kochan B, Wets G, Int PL. Implementation and validation of a modeling framework to assess personal exposure to black carbon. Environ Int. 2014;62:64–71. https://doi.org/10.1016/j.envint.2013.10.003.
Duan N. Models for human exposure to air pollution. Environ Int. 1982;8(1):305–9. https://doi.org/10.1016/0160-4120(82)90041-1.
Fallah-Shorshani M, Hatzopoulou M, Ross NA, Patterson Z, Weichenthal S. Evaluating the impact of neighborhood characteristics on differences between residential and mobility-based exposures to outdoor air pollution. Environ Sci Technol. 2018;52(18):10777–86. https://doi.org/10.1021/acs.est.8b02260.
Hasunuma H, Sato T, Iwata T, Kohno Y, Nitta H, Odajima H, Ohara T, Omori T, Ono M, Yamazaki S, Shima M.’ Association between trafficrelated air pollution and asthma in preschool children in a national Japanese nested case-control study. BMJ Open. 2016;25:e010410. https://doi.org/10.1136/bmjopen-2015-010410.
HEI Panel on the Health Effects of Long-Term Exposure to Traffic-Related Air Pollution. Systematic Review and Meta-analysis of Selected Health Effects of Long-Term Exposure to Traffic-Related Air Pollution. Special Report 23. Boston: Health Effects Institute; 2022.
Hoek G. Methods for assessing long-term exposures to outdoor air pollutants. Curr Environ Health Rep. 2017;4(4):450–62.
IARC. Outdoor Air Pollution. Monographs on the Evaluation of Carcinogenic Risks to Humans Volume 109. Lyon: International Agency for Research on Cancer; 2015.
Janssen NA, Brunekreef B, van Vliet P, Aarts F, Meliefste K, Harssema H, Fischer P. The relationship between air pollution from heavy traffic and allergic sensitization, bronchial hyperresponsiveness, and respiratory symptoms in Dutch schoolchildren. Environ Health Perspect. 2003;111(12):1512–8. https://doi.org/10.1289/ehp.6243.
Kim J, Kwan MP. Assessment of sociodemographic disparities in environmental exposure might be erroneous due to neighborhood effect averaging: Implications for environmental inequality research. Environ Res. 2021;195:110519. https://doi.org/10.1016/j.envres.2020.110519.
Korhonen A, Relvas H, Miranda AI, Ferreira J, Lopes D, Rafael S, Almeida SM, Faria T, Martins V, Canha N, Diapouli E, Eleftheriadis K, Chalvatzaki E, Lazaridis M, Lehtomäki H, Rumrich I, Hänninen O. Analysis of spatial factors, time-activity and infiltration on outdoor generated PM2.5 exposures of school children in five European cities. Sci Total Environ. 2021;785:147111. https://doi.org/10.1016/j.scitotenv.2021.147111.
Kwan M-P. From place-based to people-based exposure measures. Soc Sci Med. 2009;69(9):1311–3.
Lane KJ, Levy JI, Scammell MK, Patton AP, Durant JL, Mwamburi M, Zamore W, Brugge D. Effect of time-activity adjustment on exposure assessment for traffic-related ultrafine particles. J Expo Sci Environ Epidemiol. 2015;25(5):506–16. https://doi.org/10.1038/jes.2015.11.
Leech JA, Nelson WC, Burnett RT, Aaron S, Raizenne ME. It’s about time: a comparison of Canadian and American time-activity patterns. J Expo Anal Environ Epidemiol. 2002;12(6):427–32. https://doi.org/10.1038/sj.jea.7500244.
Letellier N, Zamora S, Spoon C, Yang JA, Mortamais M, Escobar GC, Sears DD, Jankowska MM, Benmarhnia T. Air pollution and metabolic disorders: Dynamic versus static measures of exposure among Hispanics/Latinos and non-Hispanics. Environ Res. 2022;209:112846. https://doi.org/10.1016/j.envres.2022.112846.
Lu Y. Beyond air pollution at home: Assessment of personal exposure to PM(2.5) using activity-based travel demand model and low-cost air sensor network data. Environ Res. 2021;201:111549. https://doi.org/10.1016/j.envres.2021.111549.
Lu M, Schmitz O, Vaartjes I, Karssenberg D. Activity-based air pollution exposure assessment: differences between homemakers and cycling commuters. Health Place. 2019;60:102233. https://doi.org/10.1016/j.healthplace.2019.102233.
Ma X, Li X, Kwan MP, Chai Y. Who could not avoid exposure to high levels of residence-based pollution by daily mobility? Evidence of Air Pollution Exposure from the Perspective of the Neighborhood Effect Averaging Problem (NEAP). Int J Environ Res Public Health. 2020;17(4):1223. https://doi.org/10.3390/ijerph17041223.
Marquet O, Tello-Barsocchini J, Couto-Trigo D, Gómez-Varo I, Maciejewska M. Comparison of static and dynamic exposures to air pollution, noise, and greenness among seniors living in compact-city environments. Int J Health Geogr. 2023;22(1):3. https://doi.org/10.1186/s12942-023-00325-8.
Martin B, Ackermann-Liebrich U, Leuenberger P, et al. SAPALDIA: methods and participation in the cross-sectional part of the swiss study on Air pollution and lung diseases in adults. Soz Praventivmed. 1997;42. https://doi.org/10.1007/bf01318136.
McConnell R, Islam T, Shankardass K, Jerrett M, Lurmann F, Gilliland F, et al. Childhood incident asthma and traffic-related air pollution at home and school. Environ Health Perspect. 2010;118:1021–6. https://doi.org/10.1289/ehp.0901232.
Mölter A, Agius R, de Vocht F, Lindley S, Gerrard W, Custovic A, et al. Effects of long-term exposure to PM10 and NO2 on asthma and wheeze in a prospective birth cohort. J epidemiol Commun Health. 2014;68(1):21–8. https://doi.org/10.1136/jech-2013-202681.
Montagne D, Hoek G, Nieuwenhuijsen M, Lanki T, Pennanen A, Portella M, Meliefste K, Eeftens M, Yli-Tuomi T, Cirach M, Brunekreef B. Agreement of land use regression models with personal exposure measurements of particulate matter and nitrogen oxides air pollution. Environ Sci Technol. 2013;47(15):8523–31.
Ntarladima AM, Karssenberg D, Vaartjes I, Grobbee DE, Schmitz O, Lu M, Boer J, Koppelman G, Vonk J, Vermeulen R, Hoek G, Gehring U. A comparison of associations with childhood lung function between air pollution exposure assessment methods with and without accounting for time-activity patterns. Environ Res. 2021;202:111710. https://doi.org/10.1016/j.envres.2021.111710.
Ntarladima AM, Vaartjes I, Grobbee DE, Dijst M, Schmitz O, Uiterwaal C, Dalmeijer G, van der Ent C, Hoek G, Karssenberg D. Relations between air pollution and vascular development in 5-year-old children: a cross-sectional study in the Netherlands. Environ Health. 2019;18(1):50. https://doi.org/10.1186/s12940-019-0487-1.
van Nunen E, Vermeulen R, Tsai MY, Probst-Hensch N, Ineichen A, Imboden M, Naccarati A, Tarallo S, Raffaele D, Ranzi A, Nieuwenhuijsen M, Jarvis D, Amaral AFS, Vlaanderen J, Meliefste K, Brunekreef B, Vineis Pl, Gulliver J, Hoek G. Associations between modeled residential outdoor and measured personal exposure to ultrafine particles in four European study areas. Atmos Environ. 2020;194:110579.
Nyhan M, Grauwin S, Britter R, Misstear B, McNabola A, Laden F, Barrett SR, Ratti C. “Exposure track”-the impact of mobile-device-based mobility patterns on quantifying population exposure to air pollution. Environ Sci Technol. 2016;50(17):9671–81. https://doi.org/10.1021/acs.est.6b02385.
Nyhan MM, Kloog I, Britter R, Ratti C, Koutrakis P. Quantifying population exposure to air pollution using individual mobility patterns inferred from mobile phone data. J Expo Sci Environ Epidemiol. 2019;29(2):238–47. https://doi.org/10.1038/s41370-018-0038-9.
Ott W, Wallace L, Mage D, et al. The environmental protection agency’s research program on total human exposure. Environ Int. 1986;12(1):475–94. https://doi.org/10.1016/0160-4120(86)90064-4.
Park YM, Kwan MP. Individual exposure estimates may be erroneous when spatiotemporal variability of air pollution and human mobility are ignored. Health Place. 2017;43:85–94. https://doi.org/10.1016/j.healthplace.2016.
de Prado-Bert P, Warembourg C, Dedele A, Heude B, Borràs E, Sabidó E, Aasvang GM, Lepeule J, Wright J, Urquiza J, Gützkow KB, Maitre L, Chatzi L, Casas M, Vafeiadi M, Nieuwenhuijsen MJ, de Castro M, Grazuleviciene R, McEachan RRC, Basagaña X, Vrijheid M, Sunyer J, Bustamante M. Short- and medium-term air pollution exposure, plasmatic protein levels and blood pressure in children. Environ Res. 2022;211:113109. https://doi.org/10.1016/j.envres.2022.113109.
Puett RC, Hart JE, Suh H, Mittleman M, Laden F. Particulate matter exposures, mortality, and cardiovascular disease in the health professionals follow-up study. Environ Health Perspect. 2011;119:1130–5.
Ragettli MS, Phuleria HC, Tsai M-Y, et al. The relevance of commuter and work/school exposure in an epidemiological study on traffic-related air pollution. J Eposure Sci Environ Epidemiol. 2014;25:474. https://doi.org/10.1038/jes.2014.83.
Reis S, Liška T, Vieno M, Carnell EJ, Beck R, Clemens T, Dragosits U, Tomlinson SJ, Leaver D, Heal MR. The influence of residential and workday population mobility on exposure to air pollution in the UK. Environ Int. 2018;121:803–13. https://doi.org/10.1016/j.envint.2018.10.005.
Roberts H, Helbich M. Multiple environmental exposures along daily mobility paths and depressive symptoms: a smartphone-based tracking study. Environ Int. 2021;156:106635. https://doi.org/10.1016/j.envint.2021.106635.
Samoli E, Butland BK. Incorporating measurement error from modeled air pollution exposures into epidemiological analyses. Curr Environ Health Rep. 2017;4(4):472–80. https://doi.org/10.1007/s40572-017-0160-1.
Setton E, Marshall JD, Brauer M, et al. The impact of daily mobility on exposure to traffic-related air pollution and health effect estimates. J Eposure Sci Environ Epidemiol. 2011;21(1):42–8. https://doi.org/10.1038/jes.2010.14.
Shafran-Nathan R, Yuval, Levy I, Broday DM. Exposure estimation errors to nitrogen oxides on a population scale due to daytime activity away from home. Sci Total Environ. 2017 ;580:1401–1409. https://doi.org/10.1016/j.scitotenv.2016.12.105.
Shafran-Nathan R, Yuval, Broday DM. Impacts of personal mobility and diurnal concentration variability on exposure misclassification to ambient pollutants. Environ Sci Technol. 2018; 52:3520–3526. https://doi.org/10.1021/acs.est.7b05656.
Shekarrizfard M, Faghih-Imani A, Hatzopoulou M. An examination of population exposure to traffic related air pollution: comparing spatially and temporally resolved estimates against long-term average exposures at the home location. Environ Res. 2016;147:435–44. https://doi.org/10.1016/j.envres.2016.02.039.
Shekarrizfard M, Minet L, Miller E, Yusuf B, Weichenthal S, Hatzopoulou M. Influence of travel behaviour and daily mobility on exposure to traffic-related air pollution. Environ Res. 2020;184:109326. https://doi.org/10.1016/j.envres.2020.109326.
Smith JD, Mitsakou C, Kitwiroon N, Barratt BM, Walton HA, Taylor JG, Anderson HR, Kelly FJ, Beevers SD. London hybrid exposure model: improving human exposure estimates to NO(2) and PM(2.5) in an urban setting. Environ Sci Technol. 2016;50(21):11760–8. https://doi.org/10.1021/acs.est.6b01817.
Stafoggia M, Oftedal B, Chen J, Rodopoulou S, Renzi M, Atkinson RW, Bauwelinck M, Klompmaker JO, Mehta A, Vienneau D, Andersen ZJ, Bellander T, Brandt J, Cesaroni G, de Hoogh K, Fecht D, Gulliver J, Hertel O, Hoffmann B, Hvidtfeldt UA, Jöckel KH, Jørgensen JT, Katsouyanni K, Ketzel M, Kristoffersen DT, Lager A, Leander K, Liu S, Ljungman PLS, Nagel G, Pershagen G, Peters A, Raaschou-Nielsen O, Rizzuto D, Schramm S, Schwarze PE, Severi G, Sigsgaard T, Strak M, van der Schouw YT, Verschuren M, Weinmayr G, Wolf K, Zitt E, Samoli E, Forastiere F, Brunekreef B, Hoek G, Janssen NAH. Long-term exposure to low ambient air pollution concentrations and mortality among 28 million people: results from seven large European cohorts within the ELAPSE project. Lancet Planet Health. 2022;6(1):e9–18.
Steinle S, Reis S, Sabel CE. Quantifying human exposure to air pollution—moving from static monitoring to spatio-temporally resolved personal exposure assessment. Sci Total Environ. 2013;443:184–93. https://doi.org/10.1016/j.scitotenv.2012.10.098.
Sunyer J, Esnaola M, Alvarez-Pedrerol M, Forns J, Rivas I, López-Vicente M, Suades-González E, Foraster M, Garcia-Esteban R, Basagaña X, Viana M, Cirach M, Moreno T, Alastuey A, Sebastian-Galles N, Nieuwenhuijsen M, Querol X. Association between traffic-related air pollution in schools and cognitive development in primary school children: a prospective cohort study. PLoS Med. 2015;12(3):e1001792. https://doi.org/10.1371/journal.pmed.1001792.
Tang R, Tian L, Thach TQ, Tsui TH, Brauer M, Lee M, Allen R, Yuchi W, Lai PC, Wong P, Barratt B. Integrating travel behavior with land use regression to estimate dynamic air pollution exposure in Hong Kong. Environ Int. 2018;113:100–8. https://doi.org/10.1016/j.envint.2018.01.009.
Thurston GD, Kipen H, Annesi-Maesano I, Balmes J, Brook RD, Cromar K, De Matteis S, Forastiere F, Forsberg B, Frampton MW, Grigg J, Heederik D, Kelly FJ, Kuenzli N, Laumbach R, Peters A, Rajagopalan ST, Rich D, Ritz B, Samet JM, Sandstrom T, Sigsgaard T, Sunyer J, Brunekreef B. A joint ERS/ATS policy statement: what constitutes an adverse health effect of air pollution? An analytical framework. Eur Respir J. 2017;49(1):1600419. https://doi.org/10.1183/13993003.00419-2016.
Wei L, Kwan M-P, Vermeulen R, Helbich M. Measuring environmental exposures in people’s activity space: The need to account for travel modes and exposure decay. J Exposure Sci Environ Epidemiol. 2023. https://doi.org/10.1038/s41370-023-00527-z.
Wijga AH, Kerkhof M, Gehring U, de Jongste JC, Postma DS, Aalberse RC, Wolse AP, Koppelman GH, van Rossem L, Oldenwening M, Brunekreef B, Smit HA. Cohort profile: the prevention and incidence of asthma and mite allergy (PIAMA) birth cohort. Int J Epidemiol. 2014;43(2):527–35. https://doi.org/10.1093/ije/dys231.
Yu H, Russell A, Mulholland J, Huang Z. Using cell phone location to assess misclassification errors in air pollution exposure estimation. Environ Pollut. 2018;233:261–6. https://doi.org/10.1016/j.envpol.2017.10.077.
Funding
This work was performed in the framework of the MOBI-AIR study, funded by the Health Effects Institute, grant agreement # 4972-RFA19-1/20–6.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conceptualization of the study. GH and KH performed the search for studies and prepared the tables. All authors critically read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Hoek, G., Vienneau, D. & de Hoogh, K. Does residential address-based exposure assessment for outdoor air pollution lead to bias in epidemiological studies?. Environ Health 23, 75 (2024). https://doi.org/10.1186/s12940-024-01111-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12940-024-01111-0