
Abstract
Background
This study aimed to examine whether the neutrophil to high-density lipoprotein cholesterol ratio (NHR) can predict cardiovascular outcomes in normoglycemic individuals with elevated fasting glucose levels.
Methods
A total of 130,801 participants with normal blood glucose levels were enrolled in the Kailuan study. Participants were categorized according to NHR quartiles and further divided into normal glucose regulation (NGR) and pre-diabetes (pre-DM) subgroups. The follow-up endpoint was major adverse cardiovascular events (CVE), including stroke and myocardial infarction.
Results
Over a median of 12.53 (8.95–13.08) years of follow-up, subjects with NHR levels in the highest quartile experienced more CVE than those with NHR levels in the lowest quartile. Multivariate Cox analyses showed that continuous changes in NHR (hazard ratio, 1.21; 95% confidence interval [CI], 1.15–1.28) and the highest quartile of NHR (hazard ratio, 1.30; 95% CI, 1.21–1.39) were independent predictors of CVE (all P < 0.001). Furthermore, when participants were categorized by both NHR quartile and glucose metabolism status, the NHR level in the highest quartile plus pre-DM group was associated with a 1.60-fold (95% CI, 1.38–1.86; P < 0.001] higher risk of CVE than that in the lowest quartile plus normoglycemic group. Significantly, the addition of NHR only, presence of pre-DM only, or combination of NHR and pre-DM to the prediction algorithm, including traditional risk factors, improved the C-statistic by 0.19, 0.05, and 0.23 (all P < 0.001).
Conclusions
Elevated NHR or fasting blood glucose level were independently associated with a higher risk of CVE among normoglycemic individuals. Moreover, pre-DM participants with high NHR levels tended to have worse prognosis, suggesting that NHR could provide greater risk stratification value than traditional risk factors for subjects with pre-DM.
Similar content being viewed by others

Background
Cardiovascular diseases (CVD), including myocardial infarction and stroke, are the leading cause of death worldwide [1, 2]. The primary cause of vascular disease is the presence of atherosclerotic lesions in the arterial wall. Atherosclerosis is a dynamic development characterized by plaque formation and destabilization driven by multiple pathological factors [3]. Inflammation, lipid abnormalities, and glucose metabolism dysfunction play pivotal roles in this complex process [1].
Neutrophils potentiate cardiac injury through multiple mechanisms, including proinflammatory cell recruitment and cytokine release [4]. Elevated circulating neutrophils are significantly associated with greater arterial wall stiffness [5] and an increased risk of adverse cardiovascular outcomes, including stroke, rapidly progressing heart failure, and acute coronary syndrome [4,5,6]. Furthermore, high-density lipoprotein cholesterol (HDL-C) particles inhibit endothelial cells in response to inflammation and oxidative stress by suppressing neutrophil activation and low-density cholesterol (LDL-C) oxidation [7,8,9,10]. Moreover, activated neutrophils curb the crucial role of HDL-C in reverse cholesterol transport [11]. The neutrophil to HDL-C ratio (NHR) is an inflammatory and lipid metabolic marker that predicts adverse cardiovascular outcomes. A few observational studies have reported that NHR assisted in the risk profiling of adverse cardiovascular events (CVE) such as long-term mortality, recurrent myocardial infarction (MI), intravenous thrombolysis, and severe artery stenosis in ischemic stroke or MI populations [12,13,14]. However, the risk prediction value of NHR in low-risk populations has not yet been investigated.
Pre-diabetes mellitus (pre-DM), a glucose metabolic state over normal glucose regulation (NGR) but below the threshold of diabetes, includes impaired fasting glycemia and/or impaired glucose tolerance [15]. While increased fasting blood glucose (FBG) has long been recognized as a predictor of adverse CVE [16,17,18], accumulating evidence has revealed a significant association between elevated FBG levels in the normoglycemic range with subclinical inflammation [19], arterial stiffness [20], and a high incidence of CVD [21, 22]. Therefore, a healthy general population with pre-DM warrants further risk stratification for a better prognosis [23]. Moreover, glucose metabolism disorders and insulin resistance significantly accelerate the inflammatory response, endothelial dysfunction, and atherosclerosis progression [24, 25]. Thus, the NHR may identify a higher cardiovascular risk among individuals with pre-DM.
Thus, this follow-up study of a community-based Chinese population cohort sought to explore the prognostic value of NHR on cardiovascular outcomes in normoglycemic individuals with or without pre-DM.
Materials and methods
Study design and population
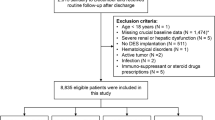
This Kailuan study (trial registration number, ChiCTR-TNC-1100148; trial registration site, http://www.chictr.org.cn/index.aspx) is a prospective cohort investigation conducted in communities in Tangshan City, Hebei Province, China [26]. The study was initiated from January 2006 to December 2012, and follow-up examinations were performed biennially, in which all participants underwent questionnaires, laboratory tests, and physical examinations. Meanwhile, cardiovascular, cerebrovascular, and related non-communicable diseases were monitored through provincial vital statistics data, the Tangshan medical insurance system, and the Kailuan Group Medical Insurance Information System. Overall, 157,926 individuals aged > 18 years participated in the Kailuan study. Of all recruited individuals, after the exclusion of 10,340 subjects for whom no neutrophil or HDL-C level information was available and 4,849 who had a medical history of malignant tumor, myocardial infarction (MI), or stroke, 142,737 individuals were enrolled. Furthermore, 11,936 individuals who received hypoglycemic therapy or insulin treatment or those with an FBG ≥ 7.0 mmol/L were excluded. Thus, a total of 130,801 individuals were included in the final analysis (Fig. 1).

Flowchart of the study population
This study was approved by the ethics committee of Kailuan Hospital and conformed to the Declaration of Helsinki. All participants signed an informed consent form.
Definition of diabetes and pre-diabetes
Blood samples from all participants were acquired within 24 h of fasting after hospital admission. According to American Diabetes Association criteria [27], pre-DM was defined as an FBG level of 5.60–6.99 mmol/L, while a normal NGR was defined as an FBG level of <5.60.
Outcomes
CVE was defined previously [28] as a composite of stroke and MI until December 31, 2019 [29]. The endpoints of this study were the first appearance of CVE, which was identified by medical staff from the provincial vital statistics data, Tangshan medical insurance system, and Kailuan Group Medical Insurance Information System during the semiannual interviews. An experienced panel of cardiologists gathered and examined the medical records. CVE were determined according to the International Classification of Diseases, Tenth Revision. MI was ascertained based on characteristic clinical symptoms, elevated myocardial enzyme activity, and changes in serial electrocardiography (I12) [30]. Stroke was defined based on characteristic clinical symptoms and signs, and brain imaging examinations (I61, I63) [31]. All-cause mortality was determined by cardiologists from vital statistical offices.
Laboratory tests
The concentrations of the lipid parameters were determined using an automatic biochemistry analyzer (Hitachi 747, Tokyo, Japan) [28]. White blood cell counts were measured using an XE-1200 automated hematology analyzer (Sysmex, Kobe, Japan). Plasma FBG levels were determined using a highly sensitive and specific commercial sandwich enzyme immunoassay (BI-20082H; Biomedica, Wien, Austria). Hyperlipidemia was determined by medical history review. Physical activity was defined as moderate-intensity exercise ≥3 times/week for ≥30 min [28].
Statistical analysis
The statistical analysis was conducted using SPSS version 22.0 and R language version 3.5.2. Multiple imputation methods were used to compensate for missing data [32]. The values are expressed as mean±SD, median (25th to 75th percentiles) for continuous variables and number (percentage) for categorical variables. The Kolmogorov–Smirnov test was performed to determine the distribution of the parameters. Intergroup comparisons of the continuous and categorical variables were examined using Student’s t-test and the chi-squared test, respectively. Cox proportional hazards models were used to examine the association between NHR or FBG level and the occurrence of CVE with the adjustment for traditional risk factors of CVD, including age, sex, smoking, drinking, education, physical status, obesity, hypertension, dyslipidemia, and C-reactive protein (CRP). In addition, a sensitivity analysis of the association of NHR or FBG with the prediction of CVE (with separate adjustment for each of the other variables in the multivariate model) was performed. The improved predictive efficiency of NHR and FBG over the clinical risk factors was evaluated using C-statistics and △ C-statistics. Kaplan-Meier curves for CVE were estimated, and differences among groups were compared using the log-rank test. Statistical significance was set at P < 0.05.
Results
Baseline characteristics
This study included 130,801 eligible participants. The baseline clinical data according to NHR quartile are presented in Table 1. The average NHR in Q1, Q2, Q3, and Q4 was 1.5±0.3, 2.2±0.2, 2.9±0.2, and 4.5±1.3, respectively (P <0.001). Participants in higher NHR quartiles were significantly younger, were more likely male and smokers, were inactive, had higher blood pressures, higher body mass index, FBG, triglyceride, LDL-C, CRP concentrations, and neutrophil counts and had lower HDL-C concentrations than those in the lowest NHR quartile (all P < 0.001). Furthermore, the percentages of individuals with higher education levels and those with hypertension or dyslipidemia also increased in the higher quartiles of the NHR group (all P < 0.001).
Association between NHR level and cardiovascular outcomes
Over a median of 12.53 (8.95–13.08) years of follow-up, 7,013 CVE occurred (1,552 MI, 5,602 strokes). The corresponding prevalence of CVE in Q2, Q3, and Q4 of the NHR level were 5.33%, 5.81%, and 5.86%, respectively (P < 0.001). According to univariate Cox proportional hazard regression analysis, per SD change in NHR (hazard ratio [HR], 1.12; 95% confidence interval [CI], 1.09-1.14; P < 0.001) and continuous change in NHR (HR, 1.29; 95% CI, 1.22–1.36; P < 0.001) were independently associated with increased CVE. Furthermore, Q2 of NHR (HR, 1.21; 95% CI, 1.13–1.29; P < 0.001), Q3 of NHR (HR, 1.35; 95% CI, 1.27–1.45; P < 0.001), and Q4 of NHR (HR, 1.41; 95% CI, 1.32–1.51; P < 0.001) were significantly associated with an increased risk of CVE compared with Q1 of NHR. The adjustment for potential confounding factors, including age, male sex, smoking, drinking, education, physical activity, obesity, hypertension, dyslipidemia, and CRP levels in models 1 and 2, did not change this relationship (Table 2). Moreover, NHR was also associated with all-cause mortality in uni- and multivariate Cox proportional hazard regression analyses (Supplementary Table 1).
Kaplan-Meier analysis with the log-rank test demonstrated that patients in higher NHR quartiles had a significantly higher risk of CVE. Individuals in the NHR Q4 had the highest cumulative incidence of CVE (P < 0.001; Fig. 2a).

Kaplan–Meier curves by neutrophil to high-density lipoprotein cholesterol ratio (NHR) (a); glucose metabolism status (b); and NHR combined with glucose metabolism status (c)
Pre-diabetes, NHR, and cardiovascular outcomes
During the follow-up period, the pre-DM group had a higher incidence of CVE (7.84%) than the NGR group (5.13%). The univariate Cox regression model showed that a per SD change in FBG and continuous change in FBG were associated with a 1.13-fold (95% CI, 1.10–1.16; P < 0.001) and 1.20-fold (95% CI, 1.16–1.24; P < 0.001) higher risk of CVE, respectively. Furthermore, patients with pre-DM were at increased risk of CVE (HR, 1.58; 95% CI, 1.47–1.69; P < 0.001). The data indicated that the association between MHR and CVE was not significantly altered after the adjustment for other confounders (Table 3). Pre-DM was also associated with a higher risk of all-cause mortality in the uni- and multivariate Cox regression models (Supplementary Table 2).
CVE risk was assessed according to both NHR quartile and the presence of pre-DM. Univariate Cox regression analysis showed that NHR was positively and significantly associated with CVE from NGR to pre-DM relative to NHR Q1 of the NHR and NGR groups (P for trend < 0.001; Table 4). Additionally, the risk of CVE in pre-DM with Q3 of NHR and pre-DM with Q4 of NHR was up to 2.13-fold (95% CI, 1.85–2.44; P < 0.001) and 2.30-fold (95% CI, 2.02–2.63; P < 0.001) higher, respectively. This association was not altered in multivariate-adjusted models 1 and 2 (Table 4). The same trend of NHR for all-cause mortality in patients with pre-DM was observed (Supplementary Table 3).
Kaplan-Meier curves indicated that individuals with pre-DM had lower cumulative event-free survival rates (Fig. 2b). Moreover, the risk of CVE was further stratified according to NHR quartile and the occurrence of pre-DM. Participants in the highest NHR quartile and pre-DM groups had the lowest cumulative incidence of CVE (P for trend < 0.01; Fig. 2c).
Incremental predictive value of NHR and pre-DM for cardiovascular outcomes
As shown in Table 5, the crude model of traditional risk factors had a C-statistic of 0.752 (95% CI, 0.747–0.757). The addition of NHR to the original model increased the C-statistic to 0.754 (95% CI, 0.749–0.759; ΔC-statistic, 0.19; P < 0.001). Similarly, adding pre-DM to the original model increased the C-statistic to 0.753 (95% CI, 0.748–0.758; ΔC-statistic, 0.05; P < 0.001). Furthermore, significant improvement in the model prediction for CVE was observed with the addition of NHR and pre-DM to the original model (C-statistic, 0.754; 95% CI, 0.749–0.759; ΔC-statistic, 0.23; P < 0.001).
Discussion
Main findings
This community-based cohort study of 130,801 normoglycemic individuals explored the effect of NHR on cardiovascular outcomes in subjects with or without pre-DM. Cox regression analysis showed that higher NHR or FBG levels were significantly associated with long-term adverse cardiovascular risk. Furthermore, pre-DM individuals with high NHR levels tended to have worse prognosis. Notably, the addition of NHR and pre-DM to the original model significantly improved the risk prediction beyond the original risk factor model. This study demonstrated that NHR, as a user-friendly factor, could assist in the risk stratification of individuals with pre-DM.
Predictive values of NHR for CVE
Discovering novel user-friendly laboratory indices could help stratify risk and identify therapeutic strategies [33]. Inflammation and dyslipidemia are two interactive pathological processes that drive the initiation and progression of atherosclerotic cardiovascular disease, while neutrophils drive its early inflammatory response [34, 35]. Neutrophil accumulation was identified at the site of atherosclerotic lesions and contributes to plaque instability [36]. The increased release of myeloperoxidase from neutrophils can aggravate atherosclerotic lesions [37, 38]. Dyslipidemia is causally associated with atherosclerosis progression. HDL-C displays an anti-atherogenic effect by transporting excess cholesterol from adipocytes or macrophages back to the liver [39]. Patients with lower HDL-C levels appear to be at higher risk of cardiovascular mortality and CVE in the general population [10, 40].
Additionally, HDL-C possesses the capacity to suppress the inflammatory response and oxidation [10, 41]. HDL-C can blunt neutrophil activation, adhesion, and migration [8]. Therefore, NHR was proposed as a novel index to evaluate the effects of inflammation and dyslipidemia on cardiovascular disease prognosis. Recent studies revealed that NHR is significantly elevated in multiple pathological states and contributes to the development of several diseases [12,13,14, 42]. NHR is significantly increased in patients with severe stroke and acts as an independent predictor of short-term outcomes [12].
A recent study of 404 patients who underwent coronary angiography demonstrated that NHR was associated with severe coronary stenosis [14]. Another study reported that NHR predicted long-term mortality and recurrent MI in elderly patients with acute MI [13]. Moreover, a cohort study of 983 peritoneal dialysis patients found that NHR had better prognostic value for all-cause mortality and new-onset CVE in patients with high cardiovascular risk [43]. However, whether NHR can predict long-term cardiovascular risk in a low-risk population has not been explored. Importantly, the present study showed that elevated NHR levels were significantly associated with a higher risk of CVE. Thus, NHR has important prognostic value in large community-based populations.
Individuals with pre-DM require precise cardiovascular risk stratification [23]. Thus, the identification of novel circulating biomarkers is crucial for this population. This study explored the predictive performance of NHR for cardiovascular risk in individuals with pre-DM. The present study demonstrated that, among normoglycemic individuals, pre-DM plus elevated NHR levels were associated with a 2.30-fold higher risk of adverse cardiovascular outcomes than NGR and low NHR levels. Moreover, combining NHR with pre-DM offers incremental predictive value over traditional risk factors in the general population, suggesting that subclinical inflammation influences the cardiovascular prognosis of patients with impaired fasting glucose.
The concrete mechanism of this phenomenon is as follows. Alterations in vascular homeostasis caused by endothelial dysfunction are the most apparent characteristics of diabetic angiopathy that facilitate an inflammatory response and finally lead to atherosclerosis [25]. Specifically, long-term exposure to impaired blood glucose coupled with dyslipidemia and subclinical inflammation contribute to the pathophysiological progression of hyperglycemia-related macrovascular disorders [44]. Abnormal glycemic concentrations induce oxidative stress and overload free radicals in endothelial cells, triggering multiple molecular mechanisms involving nuclear factor-kappa B (NF-κB)-mediated vascular inflammation and protein kinase C activation, which contributes to vasoconstriction and platelet adhesion [45]. In addition, NF-kB signaling activation upregulates multiple proinflammatory genes [44]. Therefore, NHR is a reliable and incremental prognostic biomarker that can aid the cardiovascular risk stratification in patients with pre-DM.
Comparisons with other studies and what does the current work add to the existing knowledge
Previous studies demonstrated that NHR is associated with adverse cardiovascular outcomes in high-risk patients with coronary disease or stroke[12,13,14]. However, whether it is associated with a higher cardiovascular risk in the low-risk general population remains unclear. The current study revealed that NHR could predict CVE in low-risk individuals. Moreover, pre-DM participants with high NHR levels appeared to have a higher cardiovascular risk.
Strength and study limitations
This study has several strengths. The present study revealed a novel cardiovascular risk prediction role for NHR in a low-risk population. In addition, this cohort study comprised a large population of over 130,000 Chinese adults and was followed up for a median 12.53 years, which confirms its credibility. However, this study also has several limitations. First, its observational and prospective design may have been influenced by potential biases from the non-random assignment of exposures. Second, its analyses were based on the baseline measurements of neutrophils and FBG without oral glucose tolerance testing and glycosylated hemoglobin A1c level examination; therefore, patients with new-onset diabetes during the follow-up period may have been missed. Third, although individuals with an acute infectious status were excluded during the physical examination, the present study had no data about infectious disease.
Conclusions
In the general population, higher FBG levels, even within the normal range, and elevated NHR are associated with a higher cardiovascular risk. Our findings suggest that NHR provides critical value for risk stratification and prognosis prediction for individuals with pre-DM.
Availability of data and materials
The datasets used and/or analyzed during the current study are available upon reasonable request from the corresponding author.
Abbreviations
- BMI:
-
Body mass index
- CABG:
-
Coronary artery bypass grafting
- CI:
-
Confidence interval
- CRP:
-
C-reactive protein
- CVE:
-
Cardiovascular events
- DM:
-
Diabetes mellitus
- FBG:
-
Fasting blood glucose
- HDL-C:
-
High-density lipoprotein cholesterol
- HR:
-
Hazard ratio
- LDL-C:
-
Low-density lipoprotein cholesterol
- MI:
-
Myocardial infarction
- NF-κB:
-
Nuclear factor-kappa B
- NGR:
-
Normal glucose regulation
- NHR:
-
Neutrophil to high-density lipoprotein cholesterol ratio
References
Libby P, Buring JE, Badimon L, Hansson GK, Deanfield J, Bittencourt MS, et al. Atherosclerosis. Nat Rev Dis Primers. 2019;5:56. https://doi.org/10.1038/s41572-019-0106-z.
Zhao D, Liu J, Wang M, Zhang X, Zhou M. Epidemiology of cardiovascular disease in China: current features and implications. Nat Rev Cardiol. 2019;16:203–12. https://doi.org/10.1038/s41569-018-0119-4.
Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41:407–77. https://doi.org/10.1093/eurheartj/ehz425.
Sreejit G, Abdel Latif A, Murphy AJ, Nagareddy PR. Emerging roles of neutrophil-borne S100A8/A9 in cardiovascular inflammation. Pharmacol Res. 2020;161:105212. https://doi.org/10.1016/j.phrs.2020.105212.
Angeli F, Angeli E, Ambrosio G, Mazzotta G, Cavallini C, Reboldi G, et al. Neutrophil count and ambulatory pulse pressure as predictors of cardiovascular adverse events in postmenopausal women with hypertension. Am J Hypertens. 2011;24:591–8. https://doi.org/10.1038/ajh.2011.18.
Zhu B, Pan Y, Jing J, Meng X, Zhao X, Liu L, et al. Neutrophil counts, neutrophil ratio, and new stroke in minor ischemic stroke or TIA. Neurology. 2018;90:e1870–8. https://doi.org/10.1212/wnl.0000000000005554.
Curcic S, Holzer M, Frei R, Pasterk L, Schicho R, Heinemann A, et al. Neutrophil effector responses are suppressed by secretory phospholipase A2 modified HDL. Biochim Biophys Acta. 2015;1851:184–93. https://doi.org/10.1016/j.bbalip.2014.11.010.
Murphy AJ, Woollard KJ, Suhartoyo A, Stirzaker RA, Shaw J, Sviridov D, et al. Neutrophil activation is attenuated by high-density lipoprotein and apolipoprotein A-I in in vitro and in vivo models of inflammation. Arterioscler Thromb Vasc Biol. 2011;31:1333–41. https://doi.org/10.1161/atvbaha.111.226258.
Pownall HJ, Rosales C, Gillard BK, Gotto AM Jr. High-density lipoproteins, reverse cholesterol transport and atherogenesis. Nat Rev Cardiol. 2021;18:712–23. https://doi.org/10.1038/s41569-021-00538-z.
Jia C, Anderson JLC, Gruppen EG, Lei Y, Bakker SJL, Dullaart RPF, et al. High-density lipoprotein anti-inflammatory capacity and incident cardiovascular events. Circulation. 2021;143:1935–45. https://doi.org/10.1161/circulationaha.120.050808.
Smith JD. Dysfunctional HDL as a diagnostic and therapeutic target. Arterioscler Thromb Vasc Biol. 2010;30:151–5. https://doi.org/10.1161/atvbaha.108.179226.
Chen G, Yang N, Ren J, He Y, Huang H, Hu X, et al. Neutrophil counts to high-density lipoprotein cholesterol ratio: a potential predictor of prognosis in acute ischemic stroke patients after intravenous thrombolysis. Neurotox Res. 2020;38:1001–9. https://doi.org/10.1007/s12640-020-00274-1.
Huang JB, Chen YS, Ji HY, Xie WM, Jiang J, Ran LS, et al. Neutrophil to high-density lipoprotein ratio has a superior prognostic value in elderly patients with acute myocardial infarction: a comparison study. Lipids Health Dis. 2020;19:59. https://doi.org/10.1186/s12944-020-01238-2.
Kou T, Luo H, Yin L. Relationship between neutrophils to HDL-C ratio and severity of coronary stenosis. BMC Cardiovasc Disord. 2021;21:127. https://doi.org/10.1186/s12872-020-01771-z.
Stehouwer CD, Henry RM, Ferreira I. Arterial stiffness in diabetes and the metabolic syndrome: a pathway to cardiovascular disease. Diabetologia. 2008;51:527–39. https://doi.org/10.1007/s00125-007-0918-3.
Ning F, Zhang L, Dekker JM, Onat A, Stehouwer CD, Yudkin JS, et al. Development of coronary heart disease and ischemic stroke in relation to fasting and 2-hour plasma glucose levels in the normal range. Cardiovasc Diabetol. 2012;11:76. https://doi.org/10.1186/1475-2840-11-76.
Kaneko H, Itoh H, Kiriyama H, Kamon T, Fujiu K, Morita K, et al. Fasting plasma glucose and subsequent cardiovascular disease among young adults: analysis of a nationwide epidemiological database. Atherosclerosis. 2021;319:35–41. https://doi.org/10.1016/j.atherosclerosis.2020.12.024.
Shi H, Ge Y, Wang H, Zhang Y, Teng W, Tian L. Fasting blood glucose and risk of Stroke: a Dose-Response meta-analysis. Clin Nutr. 2021;40:3296–304. https://doi.org/10.1016/j.clnu.2020.10.054.
Di Bonito P, Sanguigno E, Forziato C, Saitta F, Iardino MR, Capaldo B. Fasting plasma glucose and clustering of cardiometabolic risk factors in normoglycemic outpatient children and adolescents. Diabetes Care. 2011;34:1412–4. https://doi.org/10.2337/dc10-1783.
Shin JY, Lee HR, Lee DC. Increased arterial stiffness in healthy subjects with high-normal glucose levels and in subjects with pre-diabetes. Cardiovasc Diabetol. 2011;10:30. https://doi.org/10.1186/1475-2840-10-30.
Alexander CM, Landsman PB, Teutsch SM. Diabetes mellitus, impaired fasting glucose, atherosclerotic risk factors, and prevalence of coronary heart disease. Am J Cardiol. 2000;86:897–902. https://doi.org/10.1016/s0002-9149(00)01118-8.
Cai X, Zhang Y, Li M, Wu JH, Mai L, Li J, et al. Association between prediabetes and risk of all cause mortality and cardiovascular disease: updated meta-analysis. BMJ. 2020;370:m2297. https://doi.org/10.1136/bmj.m2297.
Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020;41:255–323. https://doi.org/10.1093/eurheartj/ehz486.
Ormazabal V, Nair S, Elfeky O, Aguayo C, Salomon C, Zuniga FA. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc Diabetol. 2018;17:122. https://doi.org/10.1186/s12933-018-0762-4.
Poznyak A, Grechko AV, Poggio P, Myasoedova VA, Alfieri V, Orekhov AN. The Diabetes Mellitus-Atherosclerosis Connection: The Role of Lipid and Glucose Metabolism and Chronic Inflammation. Int J Mol Sci. 2020;21.https://doi.org/10.3390/ijms21051835
Wang C, Yuan Y, Zheng M, Pan A, Wang M, Zhao M, et al. Association of age of onset of hypertension with cardiovascular diseases and mortality. J Am Coll Cardiol. 2020;75:2921–30. https://doi.org/10.1016/j.jacc.2020.04.038.
Diagnosis and classification of diabetes mellitus. Diabetes Care. 2011;34Suppl 1:S62-69. https://doi.org/10.2337/dc11-S062
Song QR, Liu SL, Bi YG, Chen SH, Wu SL, Cai J. Non-alcoholic fatty liver disease is associated with cardiovascular outcomes in subjects with prediabetes and diabetes: a prospective community-based cohort study. Front Cardiovasc Med. 2022;9:889597. https://doi.org/10.3389/fcvm.2022.889597.
Ferreira-Gonzalez I, Busse JW, Heels-Ansdell D, Montori VM, Akl EA, Bryant DM, et al. Problems with use of composite end points in cardiovascular trials: systematic review of randomised controlled trials. BMJ. 2007;334:786. https://doi.org/10.1136/bmj.39136.682083.AE.
Tunstall-Pedoe H, Kuulasmaa K, Amouyel P, Arveiler D, Rajakangas AM, Pajak A, Myocardial infarction and coronary deaths in the World Health Organization MONICA Project. Registration procedures, event rates, and case-fatality rates in 38 populations from 21 countries in four continents. Circulation. 1994;90:583–612. https://doi.org/10.1161/01.cir.90.1.583.
Stroke--198. Recommendations on stroke prevention, diagnosis, and therapy. Report of the WHO Task Force on Stroke and other Cerebrovascular Disorders. Stroke. 1989;20:1407–31. https://doi.org/10.1161/01.str.20.10.1407.
Chevret S, Seaman S, Resche-Rigon M. Multiple imputation: a mature approach to dealing with missing data. Intensive Care Med. 2015;41:348–50. https://doi.org/10.1007/s00134-014-3624-x.
Leonardi S, Gragnano F, Carrara G, Gargiulo G, Frigoli E, Vranckx P, et al. Prognostic Implications of Declining Hemoglobin Content in Patients Hospitalized With Acute Coronary Syndromes. J Am Coll Cardiol. 2021;77:375–88. https://doi.org/10.1016/j.jacc.2020.11.046.
Montecucco F, Liberale L, Bonaventura A, Vecchiè A, Dallegri F, Carbone F. The role of inflammation in cardiovascular outcome. Curr Atheroscler Rep. 2017;19:11. https://doi.org/10.1007/s11883-017-0646-1.
Kain V, Halade GV. Role of neutrophils in ischemic heart failure. Pharmacol Ther. 2020;205:107424. https://doi.org/10.1016/j.pharmthera.2019.107424.
Döring Y, Drechsler M, Soehnlein O, Weber C. Neutrophils in atherosclerosis: from mice to man. Arterioscler Thromb Vasc Biol. 2015;35:288–95. https://doi.org/10.1161/atvbaha.114.303564.
Döring Y, Soehnlein O, Weber C. Neutrophil Extracellular Traps in Atherosclerosis and Atherothrombosis. Circ Res. 2017;120:736–43. https://doi.org/10.1161/circresaha.116.309692.
Wang XS, Kim HB, Szuchman-Sapir A, McMahon A, Dennis JM, Witting PK. Neutrophils recruited to the myocardium after acute experimental myocardial infarct generate hypochlorous acid that oxidizes cardiac myoglobin. Arch Biochem Biophys. 2016;612:103–14. https://doi.org/10.1016/j.abb.2016.10.013.
Tran-Dinh A, Diallo D, Delbosc S, Varela-Perez LM, Dang QB, Lapergue B, et al. HDL and endothelial protection. Br J Pharmacol. 2013;169:493–511. https://doi.org/10.1111/bph.12174.
Soria-Florido MT, Schröder H, Grau M, Fitó M, Lassale C. High density lipoprotein functionality and cardiovascular events and mortality: a systematic review and meta-analysis. Atherosclerosis. 2020;302:36–42. https://doi.org/10.1016/j.atherosclerosis.2020.04.015.
Nazir S, Jankowski V, Bender G, Zewinger S, Rye KA, van der Vorst EPC. Interaction between high-density lipoproteins and inflammation: Function matters more than concentration! Adv Drug Deliv Rev. 2020;159:94–119. https://doi.org/10.1016/j.addr.2020.10.006.
Liu Z, Fan Q, Wu S, Wan Y, Lei Y. Compared with the monocyte to high-density lipoprotein ratio (MHR) and the neutrophil to lymphocyte ratio (NLR), the neutrophil to high-density lipoprotein ratio (NHR) is more valuable for assessing the inflammatory process in Parkinson’s disease. Lipids Health Dis. 2021;20:35. https://doi.org/10.1186/s12944-021-01462-4.
Li M, Feng S, Zhan X, Peng F, Feng X, Zhou Q, et al. Neutrophil to high-density lipoprotein ratio associates with higher all-cause mortality and new onset cardiovascular events in peritoneal dialysis patients. IntUrol Nephrol. 2022. https://doi.org/10.1007/s11255-022-03202-8
Paneni F, Beckman JA, Creager MA, Cosentino F. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. Eur Heart J. 2013;34:2436–43. https://doi.org/10.1093/eurheartj/eht149.
Shi Y, Cosentino F, Camici GG, Akhmedov A, Vanhoutte PM, Tanner FC, et al. Oxidized low-density lipoprotein activates p66Shc via lectin-like oxidized low-density lipoprotein receptor-1, protein kinase C-beta, and c-Jun N-terminal kinase kinase in human endothelial cells. Arterioscler Thromb Vasc Biol. 2011;31:2090–7. https://doi.org/10.1161/atvbaha.111.229260.
Acknowledgments
We thank the patient advisers for providing their information. We would like to thank Editage (www.editage.cn) for English language editing.
Funding
This work was supported by CAMS Innovation Fund for Medical Sciences (No. 2021-1-I2M-007), National Natural Science Foundation of China (No. 81825002, No. 81800367), Beijing Outstanding Young Scientist Program (No. BJJWZYJH01201910023029), Capital Clinical Diagnosis and Treatment Technology Research and Demonstration Application Project of Beijing Science and Technology Commission (No. Z191100006619106), AI+ Health Collaborative Innovation Cultivation Project of Beijing Science and Technology Commission (No. Z201100005620006).
Author information
Authors and Affiliations
Contributions
YM Z, J C, and SL W planned the study; SL L, BY F, and QR S conducted the survey; BY F analyzed the data; and SL L wrote the article. YM Z and SL W contributed to drafting the manuscript. All authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study complied with the principles of the Declaration of Helsinki and was approved by the ethics committee of Kailuan Hospital. Written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplement Table 1. Relation of the NHR level and all-cause mortality in univariate and multivariate survival analysis. Supplement Table 2. Increased FBG is associated with all-cause mortality in normoglycemic individuals. Supplement Table 3. NHR levels in relation to all-cause mortality in patients with pre-diabetes.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, SL., Feng, BY., Song, QR. et al. Neutrophil to high-density lipoprotein cholesterol ratio predicts adverse cardiovascular outcomes in subjects with pre-diabetes: a large cohort study from China. Lipids Health Dis 21, 86 (2022). https://doi.org/10.1186/s12944-022-01695-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-022-01695-x