
Abstract
Background
The chronic digestive condition gallstones is quite common around the world, the development of which is closely related to oxidative stress, inflammatory response and abnormalities of lipid metabolism. In the last few years, as a novel biomarker of lipid metabolism, the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) has garnered significant interest. However, its relationship with gallstones has not been studied yet.
Methods
3,772 people, all under 50, were included in this study, and their full data came from the National Health and Nutrition Examination Survey (NHANES) database for the years 2017–2020. Information on gallstones was obtained through self-reported questionnaires. Smoothed curve fitting multifactorial logistic regression was utilized to evaluate the connection of NHHR with gallstone formation incidence. Subsequently, subgroup analysis and interaction tests were applied. Finally, to create a prediction model, logistic regression and feature screening by last absolute shrinkage and selection operator (LASSO) were used. The resulting model was displayed using a nomogram.
Results
In multivariate logistic regression that accounted for all factors, there was a 77% increase in the likelihood of gallstones for every unit rise in lnNHHR (OR 1.77 [CI 1.11–2.83]). Following NHHR stratification, the Q4 NHHR level was substantially more linked to the risk of gallstones than the Q1 level (OR 1.86 [CI 1.04–3.32]). This correlation was stronger in women, people under 35, smokers, abstainers from alcohol, non-Hispanic White people, those with excessively high cholesterol, people with COPD, and people without diabetes. After feature screening, a predictive model and visualized nomogram for gallstones were constructed with an AUC of 0.785 (CI 0.745–0.819), which was assessed by DCA to be clinically important.
Conclusion
In the group of people ≤ 50 years of age, elevated NHHR levels were substantially linked to a higher incidence of gallstones. This correlation was stronger in several specific groups such as females, under 35 years of age, smokers, and so on. Predictive models constructed using the NHHR have potential clinical value in assessing gallstone formation.
Similar content being viewed by others


Introduction
Gallstones, a globally prevalent chronic disorder of the digestive system, exhibit pronounced geographic variations in their incidence, displaying distinct epidemiological patterns across diverse countries and regions [1]. According to data from epidemiologic surveys in the US, its domestic prevalence is up to 10–15%, with differences in multiple dimensions, such as gender, age, and lifestyle, with a high prevalence of [2,3,4]. In particular, middle-aged women have a significantly higher prevalence than young men, which may be related to changes in their estrogen levels, which can reduce the contractile function of the gallbladder and thus increase risk [5]. In addition, with the change of lifestyle, young people have fast food consumption, fried food consumption, richer fat food consumption, richer cholesterol food consumption, stay up late and other bad habits, so that young people are generally obese, further contributing to the prevalence of gallstones tends to be younger [6,7,8]. It has been established that gallstones pose a serious risk for cardiovascular disease, which further impacts the social workforce and raises the expense of healthcare [9, 10]. Therefore, it is particularly important to predict the prevalence of gallstones in young and middle-aged people and to prevent them in clinical practice.
It is well known that gallstones can be categorized into calcium bilirubinate stones, cholesterol stones, and mixed stones according to their composition [11]. Among them, cholesterol stones are predominant (70%) and are mainly formed due to the imbalance in the concentration ratio of the three components: cholesterol, bile salts and lecithin, which causes cholesterol to precipitate out of bile [12, 13]. Existing studies reveal that the development of gallstones is closely related to oxidative stress and inflammatory response [14]. Disorders of lipid metabolism have also been shown to be a key factor in gallstone formation [15]. The discovery by Liu et al. that a larger ratio of monocytes to high-density lipoprotein cholesterol was linked to a higher incidence of gallstones emphasizes the critical role that lipids play in the development of gallstones [16].
In recent years, the ratio of non-high-density lipoprotein cholesterol (NHDL-C) to high-density lipoprotein cholesterol (HDL-C) is known as the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR), and it has garnered interest as a developing biomarker [17]. Among them, NHDL-C, which is mostly made up of more than 70% low-density lipoprotein cholesterol (LDL-C), is useful in the diagnosis of hyperlipoproteinemia and coronary artery disease, and lowering NHDL-C levels is thought to be one of the most crucial objectives of preventing cardiovascular disease [18, 19]. As of right now, research indicates that NHHR has a significant role in the emergence of metabolic diseases like kidney stones, osteoporosis, type 2 diabetes, and cardiovascular diseases [20,21,22].
Given its excellence in metabolic disease prediction, we utilized information from the 2017-March 2020 National Health and Nutrition Examination Survey (NHANES). Clarifying the relationship between NHHR levels and the occurrence of gallstones in young and middle-aged US adults was the primary objective of the research, which also evaluated the potential of NHHR as a predictive model for gallstones occurrence.
Materials and methods
Research design
NHANES is an epidemiological study organized by the National Center for Health Statistics (NCHS) and approved by Ethics Committee. Each participant gave written, informed permission. NHANES comprises five components: demographic information, physiological measurements, laboratory test data, health questionnaires, and nutritional surveys. Researchers can apply for access to the NHANES database, enabling the establishment of several health-related policies and research projects [23].
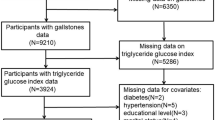
Using data from 2017 through March 2020, our study aimed to assess the predictive utility of NHHR for gallstone development and explore the correlation between NHHR and gallstone prevalence. Initially, this phase of the study included 15,560 participants. However, we excluded middle-aged and older participants over 50 years of age. Furthermore, 2,911 individuals and 4,036 participants were eliminated for lacking gallstone data and cholesterol data, respectively. In the end, 3,772 people were part of the research. Fig. 1 illustrates the specific screening process.

Flowchart of the participants’ selection from NHANES 2017–2020
Definition of NHHR and gallstones
In the NHANES program, participants had venous blood samples drawn in a fasting state, with results derived using a Roche Cobas 6000 (c501 module) analyzer, all in accordance with international standards [24]. The definition of NHHR was given as the ratio of non-high-density lipoprotein cholesterol (NHDL-C) to high-density lipoprotein cholesterol (HDL-C), where NHDL-C was determined by subtracting the HDL-C level from the overall cholesterol amount [25]. Based on the query, gallstone statistics were taken from the MCQ questionnaire, “Has a doctor or other health professional ever told you that you have gallstones?” to ascertain whether gallstones are present [26].
Relevant covariates
Drawing upon prior research, we selected some of the confounding variables with possible effects to be included in our study [26, 27]. Three major segments were included, baseline demographic data, such as gender, age, race, education level, and poverty income ratio (PIR); laboratory and test data, such as total cholesterol (mmol/L), HDL-C (mmol/L), sedentary time (minutes), body mass index (BMI, kg/m2), alanine aminotransferase (ALT, U/L); and disease and health data such as smoking status, alcohol consumption, diabetes mellitus, coronary heart disease (CHD), heart attack, chronic obstructive pulmonary disease (COPD), physical activity, and hypertension. For clarity and precision, the specific definitions of select variables are illustrated in Fig. 2, further comprehensive information is available at https://www.cdc.gov/nchs/nhanes/.

Definition of some of the covariates
Statistical analysis
Considering that the NHANES program employs a sample-weighted statistical method. For our statistical analyses, based on the NHHR’s quartile level, we divided the participants into 4 groups. We then used a weighted chi-square test for categorical variables and a weighted Student’s t-test for continuous variables. On the other hand, continuous variables were presented as means with standard error and categorical data as percentages. Missing covariates were addressed by performing multiple imputations with five replications, a chained equation method was used to handle missing data across these replications [28]. To further ensure the robustness of the study, the NHHR was ln-transformed to ensure its normal distribution. Second, to determine whether NHHR and gallstones are related, we created 3 models (one unadjusted for covariates, one adjusted for population baseline data, and one adjusted for all covariates), explored their correlation using multivariate logistic regression, and established a linear correlation between NHHR and gallstones using smoothed curve fitting. In addition, to look into the connection between NHHR and gallstones in more detail across groups, we conducted subgroup analysis and interaction tests. Next, before creating the prediction model, we filtered the relevant variables using univariate logistic regression, binary logistic regression, and least absolute shrinkage and selection operator (LASSO). Additionally, we evaluated the model value using the decision curve analysis (DCA) and receiver operating characteristic (ROC) curve. Lastly, we utilized nomogram to show the prediction model.
The R program (4.3.1) was utilized for our study, and statistical significance was defined as P < 0.05 (two-sided).
Results
Features of participants
After applying our criterion for exclusion, a group of 3,772 individuals was selected for inclusion in this comprehensive study. Table 1 succinctly outlines the demographic profiles and pertinent covariate characteristics of these participants, stratified according to quartiles of NHHR. The participants’ average age was 34.69 years, with an 8.78-year standard deviation, comprising 48.13% males and 51.87% females, reflecting a well-balanced gender distribution. Through rigorous comparative analyses, we uncovered significant associations between NHHR and a multitude of variables. Specifically, individuals with higher NHHR quartiles exhibited a tendency towards advanced age, elevated levels of ALT and BMI, indicating potential metabolic disturbances. Meanwhile, they were more likely to experience conditions including gallstones, COPD, myocardial infarction, hypertension, and coronary heart disease. Furthermore, a noteworthy trend emerged, women, individuals who were less physically active, and smokers were more inclined to have higher NHHR values.
The association of gallstone with NHHR
Table 2 presents our findings from using multivariate logistic regression to investigate the relationship with NHHR of gallstones. There was a significant positive connection found with lnNHHR of gallstones in model 2 (OR 1.80 [CI 1.22–2.66]) and model 3 (OR 1.77 [CI 1.11–2.83]). It indicated that in the fully adjusted model, the chance of getting gallstones rose by 77% for each unit rise in ln-transformed NHHR. Further sensitivity analysis showed that this association remained statistically significant when stratified by quartiles of NHHR (p-trend < 0.05). Participants in the NHHR Q4 exhibited a considerably higher chance of developing gallstones than those in the Q1 (OR 1.86 [CI 1.04–3.32]) in the fully adjusted model, indicating an 86% increased risk of developing gallstones. Meanwhile, the smoothed curve fitting results further supported the linear positive connection linking NHHR to gallstones (Fig. 3).

Smooth curve fitting for probing NHHR and gallstones
Subgroup analyses
To delve deeper into the nexus between NHHR and gallstones, we stratified participants based on gender, age, race, and health parameters (encompassing smoking status, alcohol consumption, COPD, and total cholesterol levels), and subsequent multivariate logistic regression analyses were conducted (Fig. 4). Our findings revealed a significant interaction (p-interaction ≤ 0.05) between lnNHHR and gallstones, contingent upon age and racial categories. Specifically, among individuals aged 35 years or younger, every unit increment in lnNHHR was linked to a substantial 226% rise in the likelihood of gallstone development (OR 3.26 [CI 1.62–6.59]). Conversely, this positive correlation was not evident in individuals older than 35 years. Furthermore, gallstones and lnNHHR were shown to have a strong and statistically significant positive correlation in both the “Non-Hispanic White” and “Other” ethnic groups.

Subgroup analyses of the association between NHHR and gallstones
LASSO regression for feature screening
To construct the final predictive model, we refined the initial screening of clinical variables using LASSO regression analysis. Eleven relevant variables (log of best λ = -5.696) were screened for gender, age, race, education level, smoking, BMI, CHD, COPD, diabetes, ALT, and total cholesterol (Fig. 5).

Characteristics used to predict gallstones by LASSO regression screening. (A) Regression coefficient profiles. Each curve indicates the trajectory of each feature coefficient; (B) LASSO regression cross-validation profile. Each red dot indicates the mean square error (MSE) for each value of λ. The vertical coordinate is the coefficient value, the horizontal coordinate (upper) is the number of nonzero coefficients in the model, and the horizontal coordinate (lower) is the logarithmic value of the regularization parameter λ. The dashed line on the left indicates the minimum value of λ (λmin, log(λ)=-5.696). For prediction of gallstones, we used λmin as a variable screen. Eleven characteristics were selected: gender, age, race, education level, smoking, BMI, CHD, COPD, diabetes, ALT, and total cholesterol
Logistic regression for further feature screening
In addition, we applied logistic regression analyses to further screen the clinical features derived from the LASSO regression analysis. Table 3 displays the findings of univariate logistic regression determined the following variables as being associated with the incidence of gallstones: gender, age, race, BMI, COPD, and diabetes. Subsequent multivariate logistic regression analyses indicated that seven variables, including gender, age, race, education level, BMI, COPD, and diabetes, were independent risk factors for their development (Table 3).
ROC curve for prediction modeling
Integrating the results of LASSO regression and logistic regression analyses, we screened six key variables, including gender, age, race, BMI, COPD, and diabetes, to be synergized with NHHR to construct the final prediction model. As shown in Fig. 6, our model demonstrated robust predictive performance, achieving an AUC of 0.785 (CI 0.745–0.819). It demonstrated a sensitivity of 73.89% and a specificity of 71.22%. Further DCA analysis also argued that the present model has significant clinical applications within a wide range of probability thresholds.

Performance evaluation of a predictive gallstones model. (A) ROC curve. The AUC of the model was 0.785 (CI 0.745–0.819), the specificity and sensitivity of the model were 73.89% and 71.22%, respectively. (B) Decision curve analysis (DCA). Red line for the net benefit of the predictive model, and the black line indicates that the predictive model was not used
Construction of the nomogram for prediction
Finally, we used the features in the final prediction model (gender, age, race, BMI, COPD, diabetes, and NHHR) to construct nomogram to provide an intuitively easy-to-understand and clinically user-friendly visualization tool for predicting gallstones (Fig. 7). Each feature in the graph is assigned a score value, and by adding up these scores, which represent the intensity of different risk factors, the magnitude of the likelihood that a subject will develop gallstones can be visualized and revealed.

Nomogram used to predict gallstone risk. The horizontal line at the top is the column of scores, and the total score based on the sum of the itemized scores is the risk of developing gallstones. Gender, age, race, BMI, COPD, diabetes, and NHHR are indicators of the individual scores. Within race, 1 indicates “Mexican American,” 2 indicates “Other Hispanic,” 3 indicates “Non-Hispanic White,” 4 indicates “Non-Hispanic Black”, and 5 indicates “Other Race”
Discussion
This study utilized the 2017–2020 NHANES data for a broad, multi-ethnic, cross-sectional study of individual adults under the age of 50 in US, in order to assess the association linking NHHR with gallstones. As a result of the study, we discovered that higher levels of NHHR were strongly correlated with an increased risk of gallstone formation. Even after controlling for pertinent factors, this connection remained. And, it was more pronounced in women under 35, smokers, abstainers, non-Hispanic White people, those with excessively high cholesterol, COPD, and without diabetes. In addition, we screened characteristic clinical variables and constructed a model to predict gallstones, and ROC and DCA curves confirmed its clinical value, which nomogram further visualized and applied.
Previous studies have explored in detail the potential association of LDL-C and HDL-C with gallstone formation. According to studies on the relationship between triglycerides, LDL-C, and total bile acids by Zeng et al., among them, gallstone risk was positively connected with high levels of LDL-C [29]. Similarly, based on a case-control research, Zhao and colleagues determined that elevated LDL-C values significantly increase the risk of gallstone formation [30]. A crucial step in the etiology of cholesterol stones is cholesterol oversaturation in the bile, which is caused by elevated LDL-C levels. In contrast to HDL-C, which is known for its protective effects against cardiovascular disease, Chen et al. have offered the insight that HDL-C levels are linearly and negatively correlated with the risk of cholelithiasis. This finding may be because HDL-C has anti-inflammatory and a role in facilitating cholesterol efflux from peripheral tissues [31]. In light of these findings, lipid metabolism plays a major part in the development and production of gallstones, controlling lipid profiles may be a keystone prevention strategy [32].
However, there are also many contradictions in previous studies. Animal experiments have shown that diets rich in LDL-C and low in HDL-C can reduce and eliminate the occurrence of pathologies such as gallstones [33]. Meanwhile, Chen et al.‘s research demonstrated the non-linearity of the link between total cholesterol and gallstones, and that within a certain range, lower cholesterol levels rather increase the risk of gallstones, a finding that is contrary to the traditional view [31]. We hypothesized that these differences may be caused by factors such as different testing instruments, changes in the study population and uncritical research assumptions. In recent years, the NHHR has received widespread attention as a new metric for assessing the risk of lipid-related diseases. It includes not only risky NHDL-C, but also protective HDL-C, providing a more comprehensive view of lipid homeostasis and its health effects [34, 35]. Therefore, investigating the connection between NHHR and gallstone formation may offer new perspectives to help us better understand the interactions between lipid metabolism and gallstone disease, thereby improving the prediction of gallstone risk and management strategies.
It is well known that the high-risk group for gallstones is middle-aged women, and obesity, smoking, alcohol consumption and diabetes are independent contributing factors to their development [36]. Nevertheless, our study’s findings demonstrated that women under the age of 35 had a stronger correlation between NHHR and gallstones, and the prevalence of gallstones seems to show a trend of younger age, which we hypothesize may be influenced by factors such as high stress in modern young people’s lives, excessive late nights, and dietary irregularities, but the effect of age on gallstone formation is still controversial. Secondly, the present research discovered that NHHR was linked to an increased occurrence of gallstones in participants who refrained from alcohol consumption, which is not quite in line with traditional beliefs, but is consistent with recent findings [26, 37, 38]. This is associated with alcohol’s ability to reduce serum cholesterol saturation, increase HDL-C levels and promote gallbladder motility [39,40,41]. Furthermore, in patients who were not diabetics, we discovered that NHHR was linked to a higher incidence of gallstones. Chen et al. have suggested that type 2 diabetics possess a notably higher chance of gallstones, however, type 1 diabetics between the ages of 20–40 years have a reduced risk of gallstones [42]. Ratheesh et al. also observed that the incidence of gallstones was notably greater in individuals with diabetes than in individuals without the disease [43]. But taking into account that our study did not classify diabetes mellitus and that the majority of the study person was between the ages of 20 and 40. Therefore, this conclusion of our study may be influenced by the specific typology of diabetes mellitus, and there is still no definitive study showing the association between diabetes mellitus and gallstones [44]. However, it is worth our attention that lipid metabolism disorders (e.g. hypercholesterolemia and hypertriglyceridemia) are closely associated with insulin resistance, and high levels of NHHR participants are often consistent with a diagnosis of lipid metabolism disorders. Furthermore, it has long been known that insulin resistance lowers the synthesis of bile acid synthase and increases the release of biliary cholesterol, thus predisposing patients to bile salt deposition and further increasing the risk of gallstones [45]. Thus, participants may not be diabetic but have developed insulin resistance due to disorders of lipid metabolism. This supports our hypothesis that individuals without diabetes who have high NHHR levels are much more likely to develop gallstones. In addition, our research also found that participants with COPD had a higher incidence of gallstones when their NHHR levels were elevated; there are no studies confirming a direct relationship between the two, but we hypothesize that the association between NHHR and gallstones is primarily influenced by the systemic inflammatory response caused by COPD [44].
Given these insights, lipid metabolism plays an important role in gallstone formation. Considering that long-lasting gallstones are highly susceptible to gallbladder cancer and increase the likelihood of cardiovascular disease. Thus, a strong basis for gallstone prevention and therapy may be established by keeping an eye on and controlling lipids during the formation of gallstones, therefore lowering the prevalence of cardiovascular disease and raising patients’ quality of life.
Advantages and limitations
This research provides a number of advantages. First, we selected participants from the NHANES database for the study, which provides a large number of representative samples, and the collection of the samples applied a standardized process and was supervised by the government, which provides a solid foundation for the generalization of our conclusions to a larger population. Second, we conducted subgroup analyses and interaction tests for some of the clinical variables to explore the differences between different populations. Finally, we used LASSO and logistic regression to screen the characteristic variables and constructed a predictive model for the first time, aiming to effectively promote the early detection and prevention of gallstones in young and middle-aged patients. However, it is undeniable that our study still has limitations. First, it is now unable to show a causal link between NHHR and gallstones since the study is cross-sectional, and cohort studies required to investigate the association in more detail. Secondly, although we referenced multiple clinical variables that may be associated with gallstones, the impact of all possible circumstances could not be entirely excluded (e.g. genetic factors). In addition, the population of this study was predominantly American, thus there may be disparities in applying the findings of this study to other racial groups. Finally, much of the health information involved in the study relied on self-reported questionnaires, and participant concealment and recall bias might have elicited some of the false associations. Concurrently, some patients in the general population suffer from “asymptomatic gallstones,” which are often unbeknownst to them and may consequently be reported with potential research bias. In view of the above advantages and disadvantages, to further assess and confirm our findings, a multicenter investigation must be carried out in the future.
Conclusion
Overall, among persons 50 years of age and younger, our study found a substantial correlation between NHHR and gallstone risk. This correlation was stronger in women, those under 35, smoked, did not consume alcohol, were non-Hispanic white, had abnormally elevated cholesterol, had COPD, and did not have diabetes. Also, combining NHHR with relevant clinical characteristics (gender, age, race, BMI, COPD, diabetes) allows for the construction of a simple model to predict gallstone risk.
Data availability
The study’s supporting dataset is available at https://wwwn.cdc.gov/nchs/nhanes/. Anyone can access and download.
Abbreviations
- NHHR:
-
NHDL-C to HDL-C ratio
- PIR:
-
Poverty income ratio
- NHDL-C:
-
Non-high-density lipoprotein cholesterol
- HDL-C:
-
High-density lipoprotein cholesterol
- NHANES:
-
National Health and Nutrition Examination Survey
- ALT:
-
Alanine aminotransferase
- CHD:
-
Coronary heart disease
- BMI:
-
Body mass index
- COPD:
-
Chronic obstructive pulmonary disease
References
Stinton LM, Shaffer EA. Epidemiology of gallbladder disease: cholelithiasis and cancer. Gut Liver. 2012;6:172–87. https://doi.org/10.5009/gnl.2012.6.2.172.
Luo X, Yang W, Joshi AD, Wu K, Simon TG, Yuan C, Jin L, Long L, Kim MN, Lo CH, et al. Gallstones and risk of cancers of the liver, biliary tract and pancreas: a prospective study within two U.S. cohorts. Br J Cancer. 2022;127:1069–75. https://doi.org/10.1038/s41416-022-01877-5.
Shabanzadeh DM. Incidence of gallstone disease and complications. Curr Opin Gastroenterol. 2018;34:81–9. https://doi.org/10.1097/mog.0000000000000418.
Chen L, Yang H, Li H, He C, Yang L, Lv G. Insights into modifiable risk factors of cholelithiasis: a mendelian randomization study. Hepatology. 2022;75:785–96. https://doi.org/10.1002/hep.32183.
Everhart JE, Khare M, Hill M, Maurer KR. Prevalence and ethnic differences in gallbladder disease in the United States. Gastroenterology. 1999;117:632–9. https://doi.org/10.1016/s0016-5085(99)70456-7.
Di Ciaula A, Wang DQ, Portincasa P. Cholesterol cholelithiasis: part of a systemic metabolic disease, prone to primary prevention. Expert Rev Gastroenterol Hepatol. 2019;13:157–71. https://doi.org/10.1080/17474124.2019.1549988.
Kubica K, Balbus J. A computer study of the risk of cholesterol gallstone associated with obesity and normal weight. Sci Rep. 2021;11:8868. https://doi.org/10.1038/s41598-021-88249-w.
Di Ciaula A, Garruti G, Frühbeck G, De Angelis M, de Bari O, Wang DQ, Lammert F, Portincasa P. The role of Diet in the pathogenesis of cholesterol gallstones. Curr Med Chem. 2019;26:3620–38. https://doi.org/10.2174/0929867324666170530080636.
Sandler RS, Everhart JE, Donowitz M, Adams E, Cronin K, Goodman C, Gemmen E, Shah S, Avdic A, Rubin R. The burden of selected digestive diseases in the United States. Gastroenterology. 2002;122:1500–11. https://doi.org/10.1053/gast.2002.32978.
Zheng Y, Xu M, Li Y, Hruby A, Rimm EB, Hu FB, Wirth J, Albert CM, Rexrode KM, Manson JE, Qi L. Gallstones and risk of Coronary Heart Disease: prospective analysis of 270 000 men and women from 3 US cohorts and Meta-analysis. Arterioscler Thromb Vasc Biol. 2016;36:1997–2003. https://doi.org/10.1161/atvbaha.116.307507.
Portincasa P, Di Ciaula A, Bonfrate L, Stella A, Garruti G, Lamont JT. Metabolic dysfunction-associated gallstone disease: expecting more from critical care manifestations. Intern Emerg Med. 2023;18:1897–918. https://doi.org/10.1007/s11739-023-03355-z.
(EASL) EAftSotL. EASL Clinical Practice guidelines on the prevention, diagnosis and treatment of gallstones. J Hepatol. 2016;65:146–81. https://doi.org/10.1016/j.jhep.2016.03.005.
Lammert F, Gurusamy K, Ko CW, Miquel JF, Méndez-Sánchez N, Portincasa P, van Erpecum KJ, van Laarhoven CJ, Wang DQ. Gallstones. Nat Rev Dis Primers. 2016;2:16024. https://doi.org/10.1038/nrdp.2016.24.
Rege RV, Prystowsky JB. Inflammation and a thickened mucus layer in mice with cholesterol gallstones. J Surg Res. 1998;74:81–5. https://doi.org/10.1006/jsre.1997.5213.
Liu Z, Kemp TJ, Gao YT, Corbel A, McGee EE, Wang B, Shen MC, Rashid A, Hsing AW, Hildesheim A, et al. Association of circulating inflammation proteins and gallstone disease. J Gastroenterol Hepatol. 2018;33:1920–4. https://doi.org/10.1111/jgh.14265.
Liu X, Yan G, Xu B, Sun M. Association between monocyte-to-high-density lipoprotein-cholesterol ratio and gallstones in U.S. adults: findings from the National Health and Nutrition Examination Survey 2017–2020. Lipids Health Dis. 2024;23:173. https://doi.org/10.1186/s12944-024-02166-1.
Hong H, He Y, Gong Z, Feng J, Qu Y. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and kidney stones: a cross-sectional study. Lipids Health Dis. 2024;23:102. https://doi.org/10.1186/s12944-024-02089-x.
Blaha MJ, Blumenthal RS, Brinton EA, Jacobson TA. The importance of non-HDL cholesterol reporting in lipid management. J Clin Lipidol. 2008;2:267–73. https://doi.org/10.1016/j.jacl.2008.06.013.
Cheng Q, Sun J, Zhong H, Wang Z, Liu C, Zhou S, Deng J. Research trends in lipid-lowering therapies for coronary heart disease combined with hyperlipidemia: a bibliometric study and visual analysis. Front Pharmacol. 2024;15:1393333. https://doi.org/10.3389/fphar.2024.1393333.
Tan MY, Weng L, Yang ZH, Zhu SX, Wu S, Su JH. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio with type 2 diabetes mellitus: recent findings from NHANES 2007–2018. Lipids Health Dis. 2024;23:151. https://doi.org/10.1186/s12944-024-02143-8.
Wang J, Li S, Pu H, He J. The association between the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and the risk of osteoporosis among U.S. adults: analysis of NHANES data. Lipids Health Dis. 2024;23:161. https://doi.org/10.1186/s12944-024-02152-7.
Hodkinson A, Tsimpida D, Kontopantelis E, Rutter MK, Mamas MA, Panagioti M. Comparative effectiveness of statins on non-high density lipoprotein cholesterol in people with diabetes and at risk of cardiovascular disease: systematic review and network meta-analysis. BMJ. 2022;376:e067731. https://doi.org/10.1136/bmj-2021-067731.
Hoffman HJ, Rawal S, Li CM, Duffy VB. New chemosensory component in the U.S. National Health and Nutrition Examination Survey (NHANES): first-year results for measured olfactory dysfunction. Rev Endocr Metab Disord. 2016;17:221–40. https://doi.org/10.1007/s11154-016-9364-1.
Hu H, Fukunaga A, Yokoya T, Nakagawa T, Honda T, Yamamoto S, Okazaki H, Miyamoto T, Sasaki N, Ogasawara T, et al. Non-high-density Lipoprotein Cholesterol and risk of Cardiovascular Disease: the Japan Epidemiology Collaboration on Occupational Health Study. J Atheroscler Thromb. 2022;29:1295–306. https://doi.org/10.5551/jat.63118.
Xu J, Peng H, Ma Q, Zhou X, Xu W, Huang L, Hu J, Zhang Y. Associations of non-high density lipoprotein cholesterol and traditional blood lipid profiles with hyperuricemia among middle-aged and elderly Chinese people: a community-based cross-sectional study. Lipids Health Dis. 2014;13:117. https://doi.org/10.1186/1476-511x-13-117.
Wang J, Sun YX, Xiang S, Yang C, Li XJ, Zhang MQ, Li YJ, Li XX, Qiu ZK. The association between blood heavy metals and gallstones: a cross-sectional study. Sci Total Environ. 2023;904:166735. https://doi.org/10.1016/j.scitotenv.2023.166735.
Fu C, Li X, Wang Y, Chen J, Yang Y, Liu K. Association between triglyceride glucose index-related indices with gallstone disease among US adults. Lipids Health Dis. 2024;23:203. https://doi.org/10.1186/s12944-024-02194-x.
Farrar D, Fairley L, Santorelli G, Tuffnell D, Sheldon TA, Wright J, van Overveld L, Lawlor DA. Association between hyperglycaemia and adverse perinatal outcomes in south Asian and white British women: analysis of data from the born in Bradford cohort. Lancet Diabetes Endocrinol. 2015;3:795–804. https://doi.org/10.1016/s2213-8587(15)00255-7.
Zeng D, Wu H, Huang Q, Zeng A, Yu Z, Zhong Z. High levels of serum triglyceride, low-density Lipoprotein Cholesterol, total bile acid, and total bilirubin are risk factors for gallstones. Clin Lab. 2021;67. https://doi.org/10.7754/Clin.Lab.2021.201228.
Zhao G, Shi R, Ma M, Lin H, Zhang J, Sheng B. Elevated LDL-c may warn of the risk of gallbladder stones in the patients with metabolic dysfunction-associated steatotic liver disease: a case-control study. Clin Res Hepatol Gastroenterol. 2024;48:102363. https://doi.org/10.1016/j.clinre.2024.102363.
Chen L, Qiu W, Sun X, Gao M, Zhao Y, Li M, Fan Z, Lv G. Novel insights into causal effects of serum lipids and lipid-modifying targets on cholelithiasis. Gut. 2024;73:521–32. https://doi.org/10.1136/gutjnl-2023-330784.
Zhang M, Mao M, Zhang C, Hu F, Cui P, Li G, Shi J, Wang X, Shan X. Blood lipid metabolism and the risk of gallstone disease: a multi-center study and meta-analysis. Lipids Health Dis. 2022;21:26. https://doi.org/10.1186/s12944-022-01635-9.
Nishina PM, Verstuyft J, Paigen B. Synthetic low and high fat diets for the study of atherosclerosis in the mouse. J Lipid Res. 1990;31:859–69.
Wang Z, Wu M, Du R, Tang F, Xu M, Gu T, Yang Q. The relationship between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and hyperuricaemia. Lipids Health Dis. 2024;23:187. https://doi.org/10.1186/s12944-024-02171-4.
Pan X, Zhang X, Wu X, Zhao Y, Li Y, Chen Z, Hu Y, Cao X. Association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and obstructive sleep apnea: a cross-sectional study from NHANES. Lipids Health Dis. 2024;23:209. https://doi.org/10.1186/s12944-024-02195-w.
Maurer KJ, Carey MC, Fox JG. Roles of infection, inflammation, and the immune system in cholesterol gallstone formation. Gastroenterology. 2009;136:425–40. https://doi.org/10.1053/j.gastro.2008.12.031.
Cha BH, Jang MJ, Lee SH. Alcohol consumption can reduce the risk of Gallstone Disease: a systematic review with a dose-response Meta-analysis of Case-Control and Cohort studies. Gut Liver. 2019;13:114–31. https://doi.org/10.5009/gnl18278.
Wang J, Duan X, Li B, Jiang X. Alcohol consumption and risk of gallstone disease: a meta-analysis. Eur J Gastroenterol Hepatol. 2017;29:e19–28. https://doi.org/10.1097/meg.0000000000000803.
Katsika D, Tuvblad C, Einarsson C, Lichtenstein P, Marschall HU. Body mass index, alcohol, tobacco and symptomatic gallstone disease: a Swedish twin study. J Intern Med. 2007;262:581–7. https://doi.org/10.1111/j.1365-2796.2007.01860.x.
Langer RD, Criqui MH, Reed DM. Lipoproteins and blood pressure as biological pathways for effect of moderate alcohol consumption on coronary heart disease. Circulation. 1992;85:910–5. https://doi.org/10.1161/01.cir.85.3.910.
Probert CS, Emmett PM, Heaton KW. Some determinants of whole-gut transit time: a population-based study. QJM. 1995;88:311–5.
Chen CH, Lin CL, Hsu CY, Kao CH. Association between Type I and II diabetes with Gallbladder Stone Disease. Front Endocrinol (Lausanne). 2018;9:720. https://doi.org/10.3389/fendo.2018.00720.
Ratheesh R, Ulrich MT, Ghozy S, Al-Jaboori M, Nayak SS. The association between diabetes and gallstones: a nationwide population-based cohort study. Prz Gastroenterol. 2023;18:292–9. https://doi.org/10.5114/pg.2023.131395.
Meng C, Liu K. Higher levels of systemic immune-inflammatory index are associated with the prevalence of gallstones in people under 50 years of age in the United States: a cross-sectional analysis based on NHANES. Front Med (Lausanne). 2023;10:1320735. https://doi.org/10.3389/fmed.2023.1320735.
Biddinger SB, Haas JT, Yu BB, Bezy O, Jing E, Zhang W, Unterman TG, Carey MC, Kahn CR. Hepatic insulin resistance directly promotes formation of cholesterol gallstones. Nat Med. 2008;14:778–82. https://doi.org/10.1038/nm1785.
Acknowledgements
We are appreciative of the NHANES program’s founders and participants.
Funding
This research was funded by Shaanxi Social Development Funding (No. 2017SF-134 and No. S2024-YF-ZDXM-SF-0376) and Shaanxi Science Funding (No.2020JQ-553) and Natural Science Project of Xi’an Jiaotong University (No. YXJLRH2022073).
Author information
Authors and Affiliations
Contributions
QC, ZW: wrote the initial draft after doing a statistical analysis; HZ, SZ: cleaned the data; CL, JS, SZ: checked the content for errors; JD: study design, examined and revised the manuscript, and was in charge of the finished product. Permission from each author was obtained before submitting the completed work.
Corresponding author
Ethics declarations
Ethics approval
The NHANES study was reviewed and approved by the NCHS Research Ethics Review Board.
Consent to participate
Every participant provided written, informed permission.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cheng, Q., Wang, Z., Zhong, H. et al. Association of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and gallstones among US adults aged ≤ 50 years: a cross-sectional study from NHANES 2017–2020. Lipids Health Dis 23, 265 (2024). https://doi.org/10.1186/s12944-024-02262-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-024-02262-2