
Abstract
Background
In assessing the effects of smoking cessation on endothelial function, low-flow-mediated constriction (L-FMC) may provide complementary information to flow-mediated dilation (FMD). However, the value of flow-mediated total dilation (FMTD), an index that incorporates L-FMC into FMD, remains underreported. We aimed to evaluate the effect of smoking cessation on endothelial function, as assessed by FMD and FMTD, and clarify its associated clinical factors.
Methods
We enrolled 118 consecutive current smokers without previous coronary artery disease (72.9% were men; age: 59 ± 11 years) who underwent smoking cessation treatment. The clinical variables %FMD, %L-FMC, and %FMTD were examined before and 20 weeks after treatment initiation. A multivariate linear regression model was used to investigate the effects of smoking cessation on %FMD and %FMTD and the interaction between smoking cessation and baseline clinical variables.
Results
After 20 weeks, 85 smokers (69.4% were men; age: 59 ± 12 years) ceased smoking (abstainers), whereas 33 smokers (81.8% were men; age: 58 ± 11 years) did not (continued smokers). The estimated group differences (abstainers - continued smokers) in changes in the %FMD and %FMTD were 0.77% (95% confidence interval [CI], -0.22–1.77%; p = 0.129) and 1.17% (95% CI, 0.16–2.18%; p = 0.024), respectively. Smoking cessation-associated improvement in %FMTD was greater in women than in men (5.41% [95% CI, 3.15–7.67%] versus 0.24% [95% CI, -0.81–1.28%]; p-value for interaction, < 0.001). Additionally, a greater %FMTD improvement was observed in patients who smoked fewer cigarettes per day (p-value for interaction, 0.042) and those who had a smaller resting baseline lumen diameter (Dbase) (p-value for interaction, 0.023).
Conclusions
Smoking cessation was associated with an improvement in %FMTD. Sex, cigarettes smoked per day, and Dbase significantly affected this improvement. The FMTD may help in risk stratification after smoking cessation.
Similar content being viewed by others

Background
Smoking predisposes individuals to endothelial dysfunction and eventually to arteriosclerosis; it is regarded as a major risk factor for cardiovascular disease (CVD) [1,2,3]. Therefore, smoking cessation remains the most crucial intervention in preventive and pre-emptive medicine [4, 5].
Endothelial dysfunction is an important factor in the development of atherosclerosis, which precedes the asymptomatic structural vascular alterations and clinical manifestations of CVD. Flow-mediated dilation (FMD) of the brachial artery is an endothelium-dependent, largely nitric oxide (NO)-mediated, dilatation of the conduit arteries in response to an imposed increase in blood flow and shear stress [6]. Thus, FMD is used to assess endothelial function [6, 7]. Smoking intensity is independently associated with endothelial function, as evaluated by measuring FMD [8], which improves after smoking cessation [9,10,11]. However, the effects of smoking cessation on endothelial function are not always consistent and may differ according to an individual’s sex, age, past smoking levels, duration of smoking cessation, and background [12].
Vasoconstriction during the low-flow state, also known as low-flow-mediated constriction (L-FMC), has recently been introduced and proven useful in patients with cardiovascular risk [13, 14]. L-FMC is an endothelial response to reduced blood flow due to forearm compression (resting shear stress) and is induced by several factors such as the release of endothelin-1 and inhibition of the release of cyclooxygenase-dependent products [15, 16]. L-FMC and FMD complement each other, and flow-mediated total dilation (FMTD), an index that incorporates L-FMC into FMD, has been proposed to assess endothelial function. Furthermore, the association between FMTD and cardiovascular risk has been closely examined [17, 18]; we demonstrated that FMTD may be a good alternative to FMD for estimating cardiovascular risk in smokers [18].
When assessing the effects of smoking cessation on endothelial function, L-FMC may provide complementary information to that of FMD. However, no previous study has evaluated the incorporation of the L-FMC index before and after smoking cessation. Thus, we aimed to evaluate the effect of smoking cessation on endothelial function, as assessed by FMD and FMTD, and clarify the associated clinical factors affecting endothelial function response.
Methods
Study population
Consecutive current smokers without a history of coronary artery disease (CAD), who visited our smoking cessation outpatient department and received smoking cessation treatment between April 2010 and July 2017, were enrolled. The inclusion criteria were (1) aged ≥ 20 years, (2) a Brinkman index (number of cigarettes per day × years of smoking) ≥ 200, (3) a nicotine-dependence score ≥ 5 (Tobacco Dependence Screener), and (4) motivation to quit smoking. The criteria complied with the Japanese drug use system for nicotine-dependent outpatients. Smokers with insulin-treated diabetes mellitus and previous CAD were excluded. We used varenicline (a partial agonist of alpha-4 beta-2 nicotinic receptors) to aid in smoking cessation.
Study protocol
For all enrolled participants, FMD and FMTD were measured once at baseline, before initiating the smoking cessation treatment. After vascular tests and venous blood collection at baseline, varenicline was administered and then titrated up as follows: 0.5 mg once daily for 3 days followed by 0.5 mg twice daily for 4 days and finally 1.0 mg twice daily for 11 weeks. Varenicline was discontinued at week 12. All patients were advised to visit our smoking cessation clinic at weeks 2, 4, 8, 12, and 20. Self-reported smoking status, adverse event information, body weight, and exhaled carbon monoxide (CO) concentrations were assessed at each visit. Smoking cessation was confirmed by the participants’ self-reported smoking status and an exhaled CO level ≤ 3 ppm at week 20 [19, 20]. Venous blood was collected and the FMD and FMTD were measured again at week 20. Smoking cessation at week 12 but resumption at week 20 was considered unsuccessful smoking cessation in this study. Patients who were followed up at week 20 were analysed.
Measurement of FMD, L-FMC, and FMTD
FMD was measured according to the guidelines for FMD assessment at baseline and week 20 [21]. All participants were required to fast for at least 12 h; avoid heavy exercise for at least 24 h; avoid consuming caffeine-containing products, alcohol, and antioxidant vitamins for at least 6 h; withhold all drugs for at least 12 h; and sleep soundly for at least 6 h the night before the measurement. For premenopausal female participants, examinations were performed during the menstrual period. All participants rested in a sitting position in a quiet, dimmed, temperature-controlled room (22–25 °C) for 15 min and were subsequently placed in a supine position for 15 min. Brachial artery measurements were performed between 7:00 and 11:59 a.m.
We used a 10-MHz H-type probe (UNEXEF; UNEX, Nagoya, Japan) equipped with a semiautomatic vessel wall tracking software that provided one longitudinal image, two short-axis B-mode images, and one processed A-mode line image of the brachial artery [22]. Through continuous and simultaneous monitoring, two B-mode short-axis vessel images were obtained using the edge-detection method, which was designed to maintain the same brachial artery position by adjusting the deviation of the probe position before and after forearm compression. The centre of the brachial artery and the positional stability of the A-mode lines were preserved throughout the FMD examination. A-mode lines were used to automatically measure vessel lumens on longitudinal images. A total of 41 A-mode lines, including 20 bilateral points surrounding the designated point, were measured at 0.15-mm intervals to precisely measure the vessel lumen. The measured values were averaged and presented in the images. Electrocardiogram gating was used during image acquisition, in which the onset of the R-wave was used to identify end diastole. A B-mode edge detection method was designed to automatically maintain the same position in the brachial artery by adjusting the deviation in the probe position before and after forearm compression to precisely measure the vessel lumen [21]. After determining the probe position at which the clearest baseline image could be obtained, an occlusive cuff was wrapped around the forearm with the proximal edge of the cuff at the elbow. The forearm cuff was inflated to a systolic blood pressure (SBP) of at least 50 mm Hg for 5 min. Longitudinal images of the brachial artery were automatically and continuously recorded from 0 s after cuff inflation to 5 min after cuff release.
L-FMC was defined as vasoconstriction during the 30 s before cuff release (Fig. 1) [12]. The presence of L-FMC was defined as L-FMC of 0.05 mm based on our previous study, which demonstrated that the intra-observer mean difference for lumen diameter measurements was 0.021 ± 0.016 mm using the same ultrasound system [20]. We calculated the %L-FMC as the change from the resting baseline lumen diameter (Dbase) to the minimum lumen diameter during the 30 s before cuff release (Dmin) divided by the Dbase.

A representative case with the presence of L-FMC. This patient demonstrated vasoconstriction of no less than 0.05 mm during the last 30 s before cuff release. %FMD and %FMTD were calculated as 3.23% and 6.45%, respectively. Dbase = resting baseline lumen diameter; Dmax = the lumen diameter of the hyperemic state; Dmin = minimum lumen diameter during the last 30 s before cuff release; L-FMC = low-flow-mediated constriction; FMD = flow-mediated dilation; FMTD = flow-mediated total dilation
The percentage of maximum change from Dbase to the hyperaemic state (Dmax) divided by Dbase was defined as %FMD (Fig. 1). The sum of the %FMD and absolute %L-FMC values was defined as %FMTD, which was calculated as the percentage of the maximum change from Dmin to Dmax divided by Dbase (Fig. 1) [14]. These indices were calculated using the following formulas:
Clinical data and definition
Laboratory data were obtained using fasting blood samples collected on the same day as the FMD measurements. Hypertension was defined as a SBP ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg, and/or antihypertensive medication use. Diabetes mellitus was defined as a fasting blood glucose level ≥ 126 mg/dL, glycosylated haemoglobin ≥ 6.5%, and/or use of an oral hypoglycaemic agent. Dyslipidaemia was defined as high-density lipoprotein cholesterol (HDL-C) levels < 40 mg/dL, low-density lipoprotein cholesterol levels ≥ 140 mg/dL, triglyceride levels ≥ 150 mg/dL, and/or use of a lipid-lowering medication. The change was defined as the value at week 20 minus the value at baseline, and the difference was defined as the value in abstainers minus the value in continued smokers.
Statistical analysis
The participants’ clinical characteristics are presented as mean ± standard deviation for continuous variables and as percentage (number) for categorical variables. Student’s t-test was used to compare continuous variables, and the χ2 test was used to compare categorical variables (men vs. women) at baseline. The change in each clinical parameter from baseline to week 20 was compared between smokers who successfully ceased smoking and those who did not using the Student’s t-test. A linear regression model was used to investigate the effect of smoking cessation on endothelial function as assessed by %FMD and %FMTD. In the linear regression model, we included changes in %FMD and %FMTD as dependent variables and success in smoking cessation (yes or no) and adjustment variables (sex, age, body mass index [BMI], cigarettes smoked per day, hypertension, and Dbase at baseline) as explanatory variables. Another model was developed to examine the interactions between successful smoking cessation and each factor. Statistical analyses were performed using SPSS software (version 28.0; SPSS, IBM Corp., Inc., Chicago, IL, USA) and R version 3.4.4 (R Foundation for Statistical Computing, Vienna, Austria). A p-value < 0.05 was defined as statistically significant.
Results
Patient characteristics
We included 118 participants who were followed-up for 20 weeks after the initiation of the smoking cessation treatment. Their baseline characteristics (72.9% were men; age: 59 ± 11 years) are shown in Table 1. Regarding antihypertensive medications, 27 smokers (23%) used calcium channel blockers, 22 (19%) used renin-angiotensin system inhibitors, and 2 (2%) used beta-blockers. At baseline, L-FMC was demonstrated in 33.9% of the smokers; %FMD was 4.05% ± 2.13%, and %FMTD was 5.21% ± 2.54%. No significant differences were observed between men and women except for BMI, HDL-C levels, Dbase, and brachial artery intima-media thickness.
Changes in clinical parameters
At week 20, 85 smokers (male: 69.4% were men; age: 59 ± 12 years) successfully ceased smoking (abstainers), whereas 33 smokers (81.8% were men; age: 58 ± 11 years) did not (continued smokers). The clinical parameters of abstainers and continued smokers at baseline and at week 20 are presented in Table 2. No significant differences were observed between abstainers and continued smokers, except for changes in SBP and HDL-C levels.
Effects of smoking cessation on endothelial function
At week 20, 27.1% of the abstainers demonstrated L-FMC, with %FMD and %FMTD values of 4.89% ± 2.22% and 5.77% ± 2.91%, respectively. In continued smokers, L-FMC was demonstrated in 24.2%, with %FMD and %FMTD values of 4.38% ± 2.91% and 4.86% ± 3.11%, respectively (Table 2). After adjusting for sex, age, BMI, cigarettes smoked per day, hypertension, and Dbase at baseline, the estimated group differences (abstainers - continued smokers) in changes in the %FMD and %FMTD were 0.77% (95% confidence interval [CI], -0.22–1.77%; p = 0.129) and 1.17% (95% CI, 0.16–2.18%; p = 0.024), respectively (Fig. 2; Table 3).

The estimated changes in %FMD and %FMTD in abstainers and continued smokers. A linear regression model included changes in %FMD (A) and %FMTD (B) as dependent variables and success in smoking cessation (yes or no) and adjustment variables (sex, age, body mass index, cigarettes per day, hypertension, and Dbase at baseline) as explanatory variables. Dbase = resting baseline lumen diameter; FMD = flow-mediated dilation; FMTD = flow-mediated total dilation
Interaction between smoking cessation and each factor
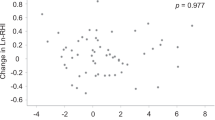
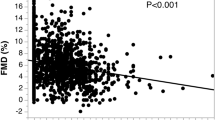
The interaction between smoking cessation and each factor after adjusting for sex, age, BMI, cigarettes smoked per day, hypertension, and Dbase at baseline is presented in Table 3; Fig. 3. No significant interaction was observed between smoking cessation and any of the factors affecting the %FMD. Conversely, smoking cessation-associated improvement in %FMTD was greater in women than in men (5.41% [95% CI, 3.15–7.67%] versus 0.24% [95% CI, -0.81–1.28%]; p-value for interaction, < 0.001). Additionally, a greater %FMTD improvement was observed in patients who smoked fewer cigarettes per day (p-value for interaction, 0.042) and had a smaller Dbase (p-value for interaction, 0.023). No significant interactions were observed between smoking cessation and other clinical factors, including age, BMI, or hypertension at baseline.

Interaction between smoking cessation and each clinical factor. A linear regression model was used after adjusting for sex, age, body mass index, cigarettes smoked per day, hypertension, and Dbase. Dbase = resting baseline lumen diameter; FMD = flow-mediated dilation; FMTD = flow-mediated total dilation
Discussion
This study demonstrated that smoking cessation was associated with improvement in %FMTD; however, %FMD was not significantly different at 20 weeks after treatment initiation. In addition, smoking cessation-associated improvement in %FMTD was greater in women than in men, as well as in patients who smoked fewer cigarettes per day and those with a smaller Dbase. To the best of our knowledge, this is the first study to assess the effects of smoking cessation on endothelial function using the FMTD.
A previous study showed that smoking cessation for 1 year improved endothelial function as assessed by FMD [9]. Another study also supported the notion of partial reversibility of smoking-induced endothelial dysfunction, showing that endothelial function in former smokers, as assessed by FMD, was impaired compared to that in normal non-smoking controls [8]. Moreover, the maximum improvement in vascular function after environmental cigarette smoke withdrawal was observed more than 2 years after smoking cessation [23], and years since quitting significantly improved atherosclerotic CVD risk prediction [7]. These findings suggest that a longer smoking cessation period results in more evident improvements in endothelial function after smoking cessation. In short-term evaluations, some studies have reported increased %FMD in abstainers [10, 11, 24, 25]; however, the results are not always consistent and may differ according to sex, age, past smoking levels, duration of cessation, and individual background [12]. In short-term evaluations, the effects of smoking cessation analysed using multivariate analysis with continued smokers as the control group have not yet been fully elucidated. The lack of a significant association between the %FMD and successful smoking cessation in our study may be partly attributable to the short evaluation period.
Smoking-induced endothelial dysfunction is associated with multiple factors, including decreased plasma NO concentration, enhanced oxidative damage, and impaired prostacyclin production [26,27,28,29]. Several previous studies have investigated whether FMD measurement alone can adequately reflect endothelial responsiveness to altered haemodynamic stimuli [30], as it mainly measures the NO-dependent part of endothelial function [21]. Simultaneous measurement of L-FMC, which appears to be NO-independent, has been proposed [31, 32]. L-FMC is induced by several factors such as the release of endothelin-1 and inhibition of the release of cyclooxygenase-dependent products [15]. FMTD has also been proposed and shown to be superior to FMD in estimating the cardiovascular risk in both smokers and non-smokers [17, 18]. In our study, the L-FMC responses tended to be attenuated after treatment in both abstainers and smokers. As the presence of L-FMC has been reported to be associated with a lower BMI in smokers [18], L-FMC attenuation might be, in part, due to increased BMI after treatment. Another study showed a reduced L-FMC response in smokers [14]. In abstainers, smoking cessation was expected to have a positive effect on L-FMC responses. Therefore, the complementary value of L-FMC in assessing the effect of smoking cessation achievement on endothelial function may explain our finding that changes in %FMTD, rather than in %FMD, were significantly associated with smoking cessation.
Smoking approximately one cigarette per day increases the risk of developing coronary heart disease [33]. However, smoking cessation, but not smoking reduction, is associated with reduced CVD risk [34], further emphasising the importance of successful smoking cessation to reduce the risk of CVD. After smoking cessation, pack-years smoked may play an important role in estimating CVD risk [35], and smoking cessation benefits may depend on past smoking levels [36]. Our study showed greater smoking cessation-associated %FMTD improvement in patients who smoked fewer cigarettes per day. These findings suggest that smoking-induced endothelial dysfunction reversibility is dependent on past smoking levels; thus, patients who smoked more cigarettes per day had less endothelial function improvement after smoking cessation.
A recent study demonstrated that excess CVD risk among former heavy smokers compared with never smokers can persist for up to 16 years after cessation [37]. However, data on how sex may influence the risk of CVD in former smokers compared with current smokers are limited because most large prospective studies with data on smoking cessation have focused heavily on men [38]. Smoking is a greater risk factor for CVD in women than in men [39, 40], and the possible underlying mechanism may involve endothelial function [41]. The chemical constituents of cigarette smoke have high oxidant and inflammatory effects that can potentiate an inflammatory response, and women may extract a greater quantity of toxic agents from the same number of cigarettes than do men [42, 43]. However, our study showed greater smoking cessation-associated %FMTD improvement in women than in men, suggesting that women smokers may benefit more at 20 weeks after the initiation of smoking cessation treatment. Although the precise mechanism is unknown, cigarette smoke exposure increases oxidative stress, whereas smoking cessation reduces oxidative damage in endothelial cells [9, 44]. These characteristics of endothelial damage associated with smoking may partially account for the results of the present study.
Large lumen diameters are mostly accompanied by low basal tone and are prone to constriction under low-flow conditions, as indicated by L-FMC [30]. Moreover, restructuring the cellular and non-cellular components of the vessel wall in response to long-term changes in haemodynamic conditions and/or chronic atherogenic exposure may change the vessel luminal diameter [45]. An enlarged brachial artery diameter has been described as a significant predictor of cardiovascular events in a population-based cohort study [46]. Our study showed greater smoking cessation-associated %FMTD improvement in patients with smaller baseline brachial artery diameters. These findings suggest that patients with advanced vascular morphological changes have less responsive endothelial function after smoking cessation.
Endothelial function measurements can be used to monitor responses to lifestyle changes, and patients whose endothelial function does not improve with interventions may be at considerable risk of further adverse events [6, 47]. These studies support the potential use of repeated endothelial function assessments, rather than a single measure, to predict future cardiovascular events [48]. In cross-sectional studies, the FMTD can better indicate the estimated CVD risk in both smokers and non-smokers in primary prevention settings [17, 18]. L-FMC may provide complementary and additive information to that of FMD on how individual endothelial function responds to smoking cessation treatment; however, no previous studies have investigated this possibility. Our study results suggest that FMTD can be a better indicator of the effects of smoking cessation on endothelial function and identify the clinical factors that interact with these effects, which may help in risk stratification after cessation.
The present study has certain limitations. First, although we enrolled consecutive smokers who visited the smoking cessation outpatient department, completed smoking cessation treatment, and were evaluated for endothelial function, the number of enrolled participants were few to adjust for all covariates to correctly estimate changes in the %FMD and %FMTD. Further prospective studies with a larger number of participants are necessary to clarify the effects of smoking cessation on the L-FMC index. Second, 27 smokers (23%) used calcium channel blockers, 22 (19%) used renin-angiotensin system inhibitors, and two (2%) used beta-blockers. Any of the patients were not using nebivolol. In this study, all participants were required to withhold all medications for at least 12 h before endothelial function measurements. However, the possibility that medications affected endothelial function cannot be completely eliminated. Additionally, we enrolled participants who used varenicline as a smoking cessation aid. To minimise the effect of varenicline on endothelial function, we set the time to determine the effect at week 20, which was 8 weeks after participants completed 12 weeks of the smoking cessation program. However, to accurately assess the effect of smoking cessation on endothelial function, it is necessary to evaluate participants who achieved smoking cessation without using any pharmacotherapies. Further examinations are warranted to clarify the impact of smoking cessation on the L-FMC-incorporated index over a longer period and the association between endothelial responsiveness to smoking cessation treatment and future cardiovascular events.
Conclusions
Smoking cessation was significantly associated with %FMTD but not with %FMD improvement at 20 weeks after treatment initiation. In addition, greater smoking cessation-associated %FMTD improvements were noted in women, those who smoked fewer cigarettes per day, and those who had a smaller Dbase. FMTD may be a better indicator to assess the effects of smoking cessation on endothelial function and identify the clinical factors that interact with its effects, which is important in risk stratification after cessation. Further prospective studies with larger sample sizes and longer follow-up periods are required to confirm our findings.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Teo KK, Ounpuu S, Hawken S, et al. INTERHEART Study investigators. Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART study: a case-control study. Lancet. 2006;368:647–58.
Wald NJ, Hackshaw AK. Cigarette smoking: an epidemiological overview. Br Med Bull. 1996;52:3–11.
Nyboe J, Jensen G, Appleyard M, Schnohr P. Smoking and the risk of first acute myocardial infarction. Am Heart J. 1991;122:438–47.
Jha P, Peto R. Global effects of smoking, of quitting, and of taxing tobacco. N Engl J Med. 2014;370:60–8.
Feeman WE Jr. The role of cigarette smoking in atherosclerotic disease: an epidemiologic analysis. J Cardiovasc Risk. 1999;6:333–6.
Thijssen DHJ, Bruno RM, van Mil ACCM, Holder SM, Faita F, Greyling A, et al. Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur Heart J. 2019;40:2534–47.
Kitta Y, Obata JE, Nakamura T, Hirano M, Kodama Y, Fujioka D, et al. Persistent impairment of endothelial vasomotor function has a negative impact on outcome in patients with coronary artery disease. J Am Coll Cardiol. 2009;53:323–30.
Celermajer DS, Sorensen KE, Georgakopoulos D, Bull C, Thomas O, Robinson J, et al. Cigarette smoking is associated with dose-related and potentially reversible impairment of endothelium-dependent dilation in healthy young adults. Circulation. 1993;88:2149–55.
Johnson HM, Gossett LK, Piper ME, Aeschlimann SE, Korcarz CE, Baker TB, Fiore MC, et al. Effects of smoking and smoking cessation on endothelial function: 1-year outcomes from a randomized clinical trial. J Am Coll Cardiol. 2010;55:1988–95.
Kato T, Umeda A, Miyagawa K, Takeda H, Adachi T, Toyoda S, et al. Varenicline-assisted smoking cessation decreases oxidative stress and restores endothelial function. Hypertens Res. 2014;37:655–8.
Fukumoto K, Takemoto Y, Norioka N, Takahashi K, Namikawa H, Tochino Y, et al. Predictors of the effects of smoking cessation on the endothelial function of conduit and digital vessels. Hypertens Res. 2021;44:63–70.
Higashi Y. Smoking cessation and vascular endothelial function. Hypertens Res. 2023;46:2670–8.
Harrison M, Parkhurst K, Tarumi T, Lin HF, Tanaka H. Low flow-mediated constriction: prevalence, impact and physiological determinant. Clin Physiol Funct Imaging. 2011;31:394–8.
Gori T, Dragoni S, Lisi M, Di Stolfo G, Sonnati S, Fineschi M, et al. Conduit artery constriction mediated by low flow a novel noninvasive method for the assessment of vascular function. J Am Coll Cardiol. 2008;51:1953–8.
Bellien J, Joannides R, Iacob M, Arnaud P, Thuillez C. Evidence for a basal release of a cytochrome-related endothelium-derived hyperpolarizing factor in the radial artery in humans. Am J Physiol Heart Circ Physiol. 2006;290:H1347–52.
Spieker LE, Lüscher TF, Noll G. ETA receptors mediate vasoconstriction of large conduit arteries during reduced flow in humans. J Cardiovasc Pharmacol. 2003;42:315–8.
Königstein K, Wagner J, Frei M, Knaier R, Klenk C, Carrard J, et al. Endothelial function of healthy adults from 20 to 91 years of age: prediction of cardiovascular risk by vasoactive range. J Hypertens. 2021;39:1361–9.
Norioka N, Takemoto Y, Kobayashi M, Makuuchi A, Yoshikawa J, Yamazaki Y, et al. Low-flow mediated constriction incorporated indices as indicators of cardiovascular risk in smokers. Atherosclerosis. 2016;251:132–8.
Perkins KA, Karelitz JL, Jao NC. Optimal carbon monoxide criteria to confirm 24-hr smoking abstinence. Nicotine Tob Res. 2013;15:978–82.
Cropsey KL, Trent LR, Clark CB, Stevens EN, Lahti AC, Hendricks PS. How low should you go? Determining the optimal cutoff for exhaled carbon monoxide to confirm smoking abstinence when using cotinine as reference. Nicotine Tob Res. 2014;16:1348–55.
Corretti MC, Anderson TJ, Benjamin EJ, Celermajer D, Charbonneau F, Creager MA, et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial artery reactivity Task Force. J Am Coll Cardiol. 2002;39:257–65.
Iguchi T, Takemoto Y, Shimada K, Matsumoto K, Nakanishi K, Otsuka K, et al. Simultaneous assessment of endothelial function and morphology in the brachial artery using a new semiautomatic ultrasound system. Hypertens Res. 2013;36:691–7.
Raitakari OT, Adams MR, McCredie RJ, et al. Arterial endothelial dysfunction related to passive smoking is potentially reversible in healthy young adults. Ann Intern Med. 1999;130:578–81.
Umeda A, Kato T, Yamane T, et al. Does smoking cessation with varenicline worsen vascular endothelial function? BMJ Open. 2013;3:e003052.
Kobayashi M, Takemoto Y, Norioka N, et al. Vascular functional and morphological alterations in smokers during Varenicline Therapy. Osaka City Med J. 2015;61:19–30.
Reilly M, Delanty N, Lawson JA, FitzGerald GA. Modulation of oxidant stress in vivo in chronic cigarette smokers. Circulation. 1996;94:19–25.
Node K, Kitakaze M, Yoshikawa H, Kosaka H, Hori M. Reversible reduction in plasma concentration of nitric oxide induced by cigarette smoking in young adults. Am J Cardiol. 1997;79:1538–41.
Raij L, DeMaster EG, Jaimes EA. Cigarette smoke-induced endothelium dysfunction: role of superoxide anion. J Hypertens. 2001;19:891–7.
Reinders JH, Brinkman HJ, van Mourik JA, de Groot PG. Cigarette smoke impairs endothelial cell prostacyclin production. Arteriosclerosis. 1986;6:15–23.
Gori T, Parker JD, Münzel T. Flow-mediated constriction: further insight into a new measure of vascular function. Eur Heart J. 2011;32:784–7.
Gori T, Grotti S, Dragoni S, Lisi M, Di Stolfo G, Sonnati S, et al. Assessment of vascular function: flow-mediated constriction complements the information of flow-mediated dilatation. Heart. 2010;96:141–7.
Humphreys RE, Green DJ, Cable NT, Thijssen DH, Dawson EA. Low-flow mediated constriction: the Yin to FMD’s Yang? Expert Rev Cardiovasc Ther. 2014;12:557–64.
Hackshaw A, Morris JK, Boniface S, Tang JL, Milenković D. Low cigarette consumption and risk of coronary heart disease and stroke: meta-analysis of 141 cohort studies in 55 study reports. BMJ. 2018;360:j5855.
Jeong SM, Jeon KH, Shin DW, Han K, Kim D, Park SH, et al. Smoking cessation, but not reduction, reduces cardiovascular disease incidence. Eur Heart J. 2021;42:4141–53.
Duncan MS, Greevy RA, Tindle HA, Vasan RS, Lipworth L, Aldrich MC, et al. Inclusion of Smoking Data in Cardiovascular Disease Risk Estimation. JAMA Cardiol. 2022;7:195–203.
Yang JJ, Yu D, Shu XO, Wen W, Rahman S, Abe S, et al. Reduction in total and major cause-specific mortality from tobacco smoking cessation: a pooled analysis of 16 population-based cohort studies in Asia. Int J Epidemiol. 2022;50:2070–81.
Duncan MS, Freiberg MS, Greevy RA Jr, Kundu S, Vasan RS, Tindle HA. Association of Smoking Cessation with subsequent risk of Cardiovascular Disease. JAMA. 2019;322:642–50.
Bolego C, Poli A, Paoletti R. Smoking and gender. Cardiovasc Res. 2002;53:568–76.
Njølstad I, Arnesen E, Lund-Larsen PG. Smoking, serum lipids, blood pressure, and sex differences in myocardial infarction. A 12-year follow-up of the Finnmark Study. Circulation. 1996;93:450–6.
Prescott E, Hippe M, Schnohr P, Hein HO, Vestbo J. Smoking and risk of myocardial infarction in women and men: longitudinal population study. BMJ. 1998;316:1043–7.
Vasiljevic Z, Scarpone M, Bergami M, Yoon J, van der Schaar M, Krljanac G, et al. Smoking and sex differences in first manifestation of cardiovascular disease. Atherosclerosis. 202;330:43–51.
Gambardella J, Sardu C, Sacra C, Del Giudice C, Santulli G. Quit smoking to outsmart atherogenesis: molecular mechanisms underlying clinical evidence. Atherosclerosis. 2017;257:242–5.
Woodward M, Tunstall-Pedoe H, Smith WC, Tavendale R. Smoking characteristics and inhalation biochemistry in the Scottish population. J Clin Epidemiol. 1991;44:1405–10.
Ambrose JA, Barua RS. The pathophysiology of cigarette smoking and cardiovascular disease: an update. J Am Coll Cardiol. 2004;43:1731–7.
Gibbons GH, Dzau VJ. The emerging concept of vascular remodeling. N Engl J Med. 1994;330:1431–8.
Yeboah J, Crouse JR, Hsu FC, Burke GL, Herrington DM. Brachial flow-mediated dilation predicts incident cardiovascular events in older adults: the Cardiovascular Health Study. Circulation. 2007;115:2390–7.
Flammer AJ, Anderson T, Celermajer DS, Creager MA, Deanfield J, Ganz P, et al. The assessment of endothelial function: from research into clinical practice. Circulation. 2012;126:753–67.
Alexander Y, Osto E, Schmidt-Trucksäss A, Shechter M, Trifunovic D, Duncker DJ, et al. Endothelial function in cardiovascular medicine: a consensus paper of the European Society of Cardiology Working Groups on Atherosclerosis and Vascular Biology, Aorta and Peripheral Vascular diseases, coronary Pathophysiology and Microcirculation, and thrombosis. Cardiovasc Res. 2021;117:29–42.
Acknowledgements
We would like to thank Hisako Yoshida for her technical support and advice on medical statistics and Ryoichi Kita and Yukie Imai for their excellent technical assistance. We would like to thank Honyaku Center Inc. for English language editing.
Funding
This study was supported in part by the Grants-in-Aid for Scientific Research from the Ministry of Education, Science, and Culture of Japan (15K08649, 19K07943, and 23K14742).
Author information
Authors and Affiliations
Contributions
Naoki Okuyama: Data curation, Formal analysis, Methodology, Writing-Original draft. Kazuo Fukumoto: Conceptualization, Data curation, Formal analysis, Methodology, Supervision, Writing-Original draft, Writing-review & editing. Yasuhiko Takemoto: Conceptualization, Methodology, Supervision, Writing-review & editing. Takeshi Yamauchi: Data curation. Ayako Makuuchi: Data curation. Hiroki Namikawa: Data curation. Hiromitsu Toyoda: Data curation. Yoshihiro Tochino: Data curation. Yasuhiro Izumiya: Writing-review & editing. Daiju Fukuda: Writing-review & editing. Taichi Shuto: Conceptualization, Supervision, Writing-review & editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participant
The study protocol adhered to the Declaration of Helsinki and was approved by the Ethics Committee of Osaka City University (approval nos. 1744 and 1752).
Consent for publication
Informed consent was obtained from all individual participants included in the study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original article has been updated: Table 3 caption has been updated to retain only the first sentence.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Okuyama, N., Fukumoto, K., Takemoto, Y. et al. Effects of smoking cessation on endothelial function as assessed by flow-mediated total dilation. Cardiovasc Ultrasound 22, 11 (2024). https://doi.org/10.1186/s12947-024-00329-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12947-024-00329-9