
Abstract
Antibody technology is widely used in the fields of biomedical and clinical therapies. Nonetheless, the complex in vitro expression of recombinant proteins, long production cycles, and harsh storage conditions have limited their applications in medicine, especially in clinical therapies. Recently, this dilemma has been overcome to a certain extent by the development of mRNA delivery systems, in which antibody-encoding mRNAs are enclosed in nanomaterials and delivered to the body. On entering the cytoplasm, the mRNAs immediately bind to ribosomes and undergo translation and post-translational modifications. This process produces monoclonal or bispecific antibodies that act directly on the patient. Additionally, it eliminates the cumbersome process of in vitro protein expression and extends the half-life of short-lived proteins, which significantly reduces the cost and duration of antibody production. This review focuses on the benefits and drawbacks of mRNA antibodies compared with the traditional in vitro expressed antibodies. In addition, it elucidates the progress of mRNA antibodies in the prevention of infectious diseases and oncology therapy.
Similar content being viewed by others


Introduction
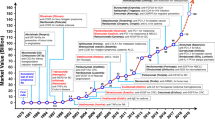
mRNA is an unstable intermediate that bridges DNA and proteins, according to the central dogma theory, genetic information is first transmitted from DNA to mRNA and then from mRNA to proteins. In this step, mRNA works as a bridge to complete the process of conversion from DNA to proteins in an organism [1]. In 1992, a study reported that injecting insulin mRNA reversed diabetes insipidus in rats to some extent [2]. Initially, mRNA therapy was expected to replace or supplement the missing or defective proteins in patients. Later, mRNA was proposed to be used as an antigen in vaccines to treat cancer and other diseases, hence RNA vaccines were created [3,4,5,6]. Since the COVID-19 outbreak, enthusiasm for mRNA delivery proteins has increased to unprecedented levels. On December 11, 2020, the Food and Drug Administration (FDA) of the United States granted an emergency use license for the COVID-19 vaccine (BNT162b2) that was based on mRNA technology and developed by Biontech Co., Ltd. and Pfizer Pharmaceutical Co., Ltd. [7, 8]. Since then, mRNA vaccines have been widely used in human population and played an important role in preventing COVID-19 spread worldwide [9, 10]. Here we summarize some of the key events in the development of mRNA delivery technology (Table 1). With the use of mRNA delivery proteins, attempts are made to use in vitro transcribed (IVT) mRNAs to express antibodies to enhance the body’s resistance to epidemics, tumors, and toxins. Unlike mRNA vaccines that deliver antigens to trigger active immunity, mRNAs encoding antibodies directly elicit passive immunity [11,12,13]. In this review, we focus on the benefits and disadvantages of delivering antibodies via mRNAs and compared them with those of the traditional methods. Their perspectives are also discussed.
Advantages and challenges of IVT mRNA delivery systems
Transient transfection with plasmid as a vector and virus-mediated stable transfection are the main methods to introduce exogenous DNA fragments into cells to obtain new phenotypes. Nonetheless, with the advent of mRNA delivery, new methods are available for cells to express exogenous proteins [27,28,29]. Here, we list the potentials and limitations of mRNA delivery systems compared with the conventional methods.
Advantages of IVT mRNA delivery systems
Advantages of IVT mRNA delivery systems compared with plasmid transfection
Plasmid transfection introduces a plasmid vector carrying exogenous DNA into a recipient cell, thereby inducing target gene overexpression in the cell. However, plasmid DNA is transcribed only during mitosis. Moreover, under normal circumstances, it is difficult for the plasmid vector to enter the nucleus. Hence, exogenous gene transcription is restricted, which significantly reduces the efficiency of protein translation. In contrast, since the mRNA delivery system is independent of the cell cycle, transient expression occurs by the cytoplasmic ribosomes; thus, it is a very efficient way to express proteins [27, 30, 31]. In addition, exogenous DNA introduction may activate the cGAS-STING signaling pathway in the cytoplasm and induce the production of type I interferons (IFN-I), thus triggering an immune response against the plasmid DNA. Besides, STING could inhibit the translation machinery to restrict the replication of diverse RNA viruses without expressing IFN-stimulated genes [32,33,34,35]. Whether or how STING influences the expression and translation of mRNA during IVT mRNA delivery is unclear and rneeds further investigation.
Advantages of IVT mRNA delivery systems compared with virus-mediated delivery
The genomes of certain viruses, such as lentiviruses, are modified to integrate exogenous genes into the host chromosome, thus causing stable protein expression. Infection with packaged viruses causes persistent transgene expression. Lentiviral vectors generally consist of two components, the packaging component and the vector component. In current systems, the original components of the virus are usually split onto different plasmids to ensure that the virus cannot be recombined. By co-transfecting packaging cells with multiple plasmids of the packaging and vector components, replication-defective lentiviral vector particles carrying the target gene can be harvested in the cell supernatant [29, 36,37,38,39]. However, since viruses randomly integrate into the host chromosomes, they increase the risk of genetic mutations. Additionally, when integrated into the tumor suppressor genes like P53, they increase the risk of cellular carcinogenesis in the host [40]. Contrastingly, since mRNA-mediated delivery is a non-integrated approach, RNA entering the nucleus is not required; thus, avoiding insertional mutagenesis caused by viral-mediated transfection.
Interestingly, certain viruses, such as the Sendai virus, use the non-integrating approach to transfer exogenous genes. Since their life cycle occurs entirely in the cytoplasm, they do not integrate into the host genome and are not affected by the cell cycle. However, residual viruses may hardly eradicate from cells [41]. While mRNAs have a short half-life in the cytoplasm and disappear gradually with cellular metabolism; hence, there is no need to specifically remove residual mRNAs [31, 42].
Advantages of IVT mRNA delivery systems compared with other protein delivery methods
Although recombinant proteins can be purified in vitro and directly imported into cells, their in vitro expression and purification is extremely tedious and complicated. Moreover, being a biological macromolecule, proteins are difficult to penetrate the cell membrane, and hence require physicochemical methods, such as electroporation or liposome encapsulation, to enter cells. Further, they may not reach their cytosolic targets even if they successfully cross the cell membrane. This may be because a significant portion of the proteins get trapped in vesicular structures, such as endosomes, and hence are unable to exert biological activity [28, 43,44,45].
Challenges of IVT mRNA delivery systems
Despite the advantages, several shortcomings limit the development and application of the mRNA delivery system. (1) mRNAs are easily degraded by nucleases in the cell or environment since they are single-stranded and less stable than double-stranded DNA. When mRNAs enter the cytoplasm, they get hydrolyzed; hence, the mRNA-delivered system cannot express long-lived proteins. (2) Since mRNAs are negatively charged, they do not easily pass through the negatively charged cell membrane. Therefore, they require specific carriers to cross the cell membrane. (3) Unmodified mRNAs may stimulate RNA receptors including RIG-I like receptors (RIG-1, LGP-2 or MDA-5) and toll-like receptors (TLR3, TLR7, or TLR8), thereby eliciting immunogenic responses and unavoidable deleterious side effects (Table 2) [23, 46,47,48,49,50,51]. Despite the existing challenges, obstacles of IVT mRNAs, such as mRNA degradation and high immunogenicity, have been gradually solved in recent years through in vitro modifications of mRNAs and optimization of mRNA purification methods. Simultaneously, the development of the nano-delivery technology enables mRNA encapsulation that promotes cellular uptake (Fig. 1) [52]. Henceforth, we focus on the status of IVT mRNA research and outline the modification, purification, and delivery methods for IVT mRNAs.

Unmodified IVT mRNAs can trigger an immune response in the body. Unmodified mRNAs have high immunogenicity that induces interferon production through activating TLR3, TLR7, and TLR8. However, in vitro modifications of mRNAs can reduce their immunogenicity to avoid the risk of triggering an immune storm in the organism
Modification, purification, and delivery of IVT mRNA
Modifications of IVT mRNAs
Post-transcriptional modifications of eukaryotic mRNAs are complex. A mature mRNA consists of a 5′ cap, a 5′ untranslated region (5′ UTR), a coding region, a 3′ untranslated region (3′ UTR), and a 3′ polyadenylate tail. The modifications shield mRNA from degradation by exonucleases. However, IVT mRNAs are transcribed from a segment of linear DNA and lack post-transcriptional modifications that directly affects mRNA stability and protein translation [53,54,55]. For example, 7-methylguanosine is attached to the first transcribed nucleotide through a 5′, 5′-triphosphate bond and protects mRNA from 5′-3′ exonucleases. Thus, the 5′ cap protects mRNA from RNase degradation. Moreover, the translation system in the cytoplasm recognizes the cap structure through the cap-binding complex (CBP). This helps the small ribosomal subunit bind to mRNA and recognize the start codon to initiate translation. Without the cap structure, CBP cannot bind to mRNA, thus translation efficiency is greatly reduced. [56,57,58,59] Therefore, artificially introducing the cap structure in IVT mRNAs can enhance their translation, improve their stability, reduce their immunogenicity, and extend their half-life. Similarly, adding the 3′ tail and modifying special bases of IVT mRNAs increase their stability and reduce their immunogenicity to avoid immune response caused by TLRs activation [60,61,62,63,64]. The sequences of COVID-19 mRNA vaccines are optimized to reduce the production of proinflammatory type I interferons [9]. For example, the uridine is replaced with purified N1-methyl-pseudouridine (1MΨ); mRNA vaccine BNT162Tech contains human α-globin RNA with optimized Kozak sequence in 5′ UTR domain, whereas mRNA vaccine CVnCoV contains artifacts from restriction and transcription site plus Kozak sequence [65].
Purification methods of IVT mRNAs
Although capping or incorporating modified nucleotides can greatly reduce the immunogenicity of mRNAs, it is hard to achieve 100% modification efficiency in vitro [66]. The unmodified mRNAs may trigger cytokine storm in the body. In addition, double-stranded RNA (dsRNA) may occur as a transcriptional byproduct and provoke an innate immune response by RNA sensors. Additionally, the remaining process-related impurities, such as protease residues, DNA templates, organic solvents, and metal ions, need to be removed. Therefore, methods for large-scale production and purification of mRNAs are critical. Common RNA purification methods are polyacrylamide gel electrophoresis, ultracentrifugation, ion exchange chromatography, hybridization affinity chromatography, reversed-phase chromatography, and HPLC-based purification methods [67,68,69,70,71,72]. These processes ensure safety for subsequent in vivo experiments. Moreover, attempts are made to reduce the immunogenicity of mRNAs and the formation of by-products for avoiding the subsequent tedious purification methods. For instance, Wu et al. used thermostable T7 RNAPs to synthesize functional mRNAs that had reduced immunogenicity and did not require a post-synthesis purification step [73]. Similarly, Xia et al. used the psychrophilic phage VSW-3 RNA polymerase to reduce terminal and full-length dsRNA byproducts in vitro transcription [74]. In conclusion, mRNA drugs should be administered with minimum innate immune effects to avoid subsequent troubles.
Delivery mode of IVT mRNAs
mRNAs have a negative charge and large molecular weight, hence do not easily cross the cell membrane [75, 76]. Recently, encapsulation with lipid nanoparticles (LNPs) is undoubtedly the most popular delivery method [77, 78]. The BNT162b2 (Pfizer/BioNTech) and mRNA-1273 (Moderna) vaccines, approved by the FDA, are mRNA vaccines encapsulated with LNPs [30, 79]. Electroporation, protamine, cationic nanoemulsion, and cationic polymer liposomes are the common delivery methods [3, 80, 81]. Selecting the appropriate vectors can effectively avoid RNA degradation, improve RNA presentation efficiency and biosafety, and promote the clinical translation of mRNA therapies (Fig. 2) [75, 82,83,84]. Here, we have compiled a selection of methods used by researchers in mRNA delivery, which contains the composition, size and type of nanoparticles used (Table 3).

Modification, purification, and delivery of IVT mRNA. In vitro transcribed mRNAs are delivered to target cells via vehicle after modifications such as capping and are translated into proteins in the cytoplasm
Applications of mRNA delivery in passive immunization
Strong immunogenicity and instability have been the major constraints to the application of mRNA delivery for a long time which have largely been overcome by technological advances. Multiple mRNA vaccines against infectious diseases and cancers showed encouraging results in animal models. Several mRNA vaccines against COVID-19 played a pivotal role in curbing the spread of human epidemics. Briefly, mRNA vaccines induce adaptive immunity in humans by delivering mRNAs encoding antigens. Recently, researchers have attempted to directly deliver mRNAs encoding antibodies to enable the body to acquire adaptive immunity (Fig. 3; Table 4). In contrast to mRNA vaccines, mRNA-encoded antibodies exhibit rapid response. Once introduced into the body, they do not have an incubation period; hence, the protective effects are immediate. In this section, we describe the recent advances in mRNA-encoded antibodies.

Schematic illustration of the mRNA antibody treatment. After being injected into the body, the mRNAs enter the cell with carriers such as LNP and bind to ribosomes to initiate translation. The antibodies produced are secreted by the cells in the extracellular compartment and travel via blood circulation to all body parts to exert their effects
Defense against viruses by delivering mRNAs encoding antibodies
Defense against SARS-CoV-2 by mRNA-encoded antibodies
Globally, > 630 million people were infected with the SARS-CoV-2 virus and the death toll reached 6.6 million by early December 2022. This epidemic swept the world and adversely affected human life [94,95,96,97,98]. Qin et al. encoded light and heavy chain mRNAs of HB27, a SARS-CoV-2 neutralizing antibody, encapsulated them in LNPs (mRNA-HB27-LNP), and successfully expressed biologically active antibodies in mice. Strikingly, mRNA-HB27-LNP has a longer circulating half-life and better prophylactic effect than the original HB27 protein. Moreover, in mice, intravenous administration of a single dose of mRNA-HB27-LNP was effective against lethal doses of MASCp36, a mouse-adapted SARS-CoV-2 strain, and did not cause significant adverse effects. After a single injection of 1 mg/kg mRNA-HB27-LNP, the antibody concentration in mice reached a maximum on day 7. The serum antibody concentration remained at 4.95 µg/mL with a mean of 179.95 µg/mL at 63 days after administration, a result that was much higher than that of an equal dose of original HB27 antibody in protein format (Fig. 4). Furthermore, mRNA-HB27-LNP is highly potent against the beta variant of SARS-CoV-2. Interestingly, prophylactic administration of mRNA-HB27-LNP protected animals in a close contact transmission model and provided long-term prophylactic efficacy against SARS-CoV-2 infection [90, 99]. Similarly, using the Venezuelan equine encephalitis virus (VEEV) replicon, Ye et al. constructed a single mRNA vector expressing both, the heavy and light chains, of the CB6 monoclonal antibody (VEEV-rep-CB6) by an alphavirus replicon particle (VRP) delivery system. The VEEV-VRP is an ideal delivery system as it has a broad range of susceptible host cells and high expression level of cytoplasmic proteins. Studies revealed that the local delivery of CB6 antibody-encoding mRNAs through intranasal administration induced antibody expression in multiple cell lines in mouse lungs, effectively blocked SARS-CoV-2 infection, reduced viral titers, and decreased damage to mouse lung tissues [100, 101].

Copyright © 2022, The Author(s)
mRNA-HB27-LNP provides a long-term protection against SARS-CoV-2 challenge in mice. a The antibody concentration of serum in mice by ELISA. Briefly, groups of 6–8-week-old ICR mice were i.v. administrated with a single dose of 1 mg/kg of HB27 (n = 4) and HB27-mRNA-LNP (n = 4), respectively. At indicated times post administration, sera of mice were measured by ELISA. Dotted lines indicate the limits of detection. b Analysis of antibody pharmacokinetics in serum after the i.v. administration with a single dose of HB27 and mRNA-HB27-LNP. Calculations were performed using WinNolin. c NT50 of serum in mice by VSV-based SARS-CoV-2 pseudovirus. Data are shown as mean ± SEM. Dashed lines represents limit of detection. d, e Experimental design. Briefly, groups of 8-month-old female BALB/c mice were i.v. administrated with a single dose of 1 mg /kg of HB27 or mRNA-HB27-LNP (n = 4 or 5) and Placebo (n = 5). Then at 7 days or 63 days post administration, mice were challenged with 6 × 103 PFU of MASCp36, respectively, and the clinical symptoms and mortality were recorded for 14 days. Survival curves of mice after lethal challenge by MASCp36 at 7 days (d) and 63 days (e) after the i.v. administration. Data were analyzed by Wilcoxon log-rank survival test (**P < 0.01). a-e Reproduced with permission from ref [90].
Defense against HIV by mRNA-encoded antibodies
VRC01 is a neutralizing anti-HIV-1 antibody [102,103,104,105]. Weissman et al. evaluated the kinetics and protective effects of the 1-methyl pseudouridine (m1Ψ)-modified and FPLC-purified mRNA-based delivery of the VRC01 antibody. Mice administered 1.4 mg/kg mRNA resulted in VRC01 antibody concentrations in plasma of 170 mg/mL at 24 h. A single intravenous injection of mRNA-VRC01-LNPs maintained high antibody levels for 5 days in mice. While successive injections of mRNA-VRC01-LNPs maintained high antibody levels for a long time, with no obvious immune inflammatory response in mice triggered by the purified mRNA-VRC01-LNPs. To determine whether mRNA-VRC01-LNPs protect animals from the HIV-1 virus, mice primed with VRC01 mRNAs to achieve high antibody titers were injected with SF162 HIV-1. The results demonstrated that HIV-1 replication was robustly inhibited. Similar attack experiments by HIV-1 JR-CSF also supported that mRNA-encoded antibodies effectively protect the organism from viral invasion [106]. Recently, some camelid antibodies have been developed against HIV [107]. Nanobodies are found in the blood of camelids and sharks, which contain only a heavy chain variable region (VHH) and two conventional CH2 and CH3 regions. VHH has the properties of high solubility, low aggregation, and resistance to high temperatures, strong acids and bases, which has a promising prospect for the development of therapeutic antibody drugs [108]. However, there wasn’t any research yet on treating HIV with mRNA-encoded camelid antibodies, which might be a new therapeutic option.
Defense against influenza a virus by mRNA-encoded antibodies
mRNAs can be used to deliver specific monoclonal antibodies as well as bispecific antibodies. Compared to conventional monoclonal antibodies, bispecific antibodies can bind two different antigenic epitopes, providing broader therapeutic effects. They could enhance the ability of immune cells to kill target cells because they could target both cell types [109,110,111,112]. Saelens et al. developed a bispecific VHH antibody (RiboBiFE) that specifically binds to the activating mouse Fcg receptor IV (FcgRIV) and the ectodomain of the conserved influenza A matrix protein 2 (M2e). Thus, the antibody selectively recruits the innate immune cells to influenza A virus-infected cells [113, 114]. The bispecific VHH antibodies were successfully produced in mice lungs by formulating the mRNA encoding RiboBiFE into DOTAP/cholesterol nanoparticles and intrabronchial drops. The mRNA-RiboBiFE was present for a greater duration in the lungs compared with the protein-based RiboBiFE. Mice treated with mRNA-RiboBiFEs were significantly better protected against death caused by influenza virus infection compared to negative controls. In addition, these bispecific VHH antibodies greatly reduced the morbidity caused by influenza A virus attack, which provides a new strategy against them [89, 108, 115, 116].
Defense against Zika virus by mRNA-encoded antibodies
Zika virus (ZIKV) is a single-stranded RNA virus that primarily transmits via mosquitoes [117,118,119]. ZIKV-117 is a potent neutralizing mAb with broad activity against the African and Asian lineages of ZIKV [120]. Van Hoeven N et al. intramuscularly injected mRNA-encoded ZIKV-117 to combat ZIKV transmission. For effective expression of mRNA antibodies in vivo, researchers used a replicating viral RNA (ZIKV-117 repRNA) to amplify the antibody-encoding mRNAs. The repRNA increased the serum antibody concentration by > 30-fold in mice than non-replicating mRNA. In the lethal ZIKV challenge model in mice, the ZIKV-117 repRNA provided effective protection to mice. This study provides a possible scenario for future human deployment of inhibitory antibodies to curb the spread of epidemics [121].
Defense against chikungunya virus by mRNA-encoded antibodies
Chikungunya virus (CHIKV) causes an acute infectious disease and has no approved vaccine or antiviral drug [122,123,124]. Crowe et al. isolated CHKV-24, a super-neutralizing human-derived monoclonal antibody, from the B cells of a survivor naturally infected with CHIKV. The mRNAs encoding CHKV-24 antibodies were normally expressed in the sera of both, mice and nonhuman primates. This mRNA-LNP protected against CHIKV-induced arthritis, musculoskeletal diseases, and lethal attack in a mouse model and was well tolerated in crab-eating monkeys injected with CHKV-24 IgG. Notably, infusion of macaques with 0.5 mg/kg CHKV-24 mRNA achieved a mean maximal mAb concentration of 10.1–35.9 micrograms per milliliter, with a half-life of 23 days. This suggested that it may be feasible to treat humans by injecting CHIKV antibodies-encoding mRNAs [125]. Subsequently, Zaks et al. conducted a phase I human randomized placebo-controlled proof-of-concept trial between January 2019 and June 2020 to assess the safety and pharmacology of mRNA-1944 (mRNA-CHKV-24). The results revealed that two different mRNAs encoding the heavy and light chains of CHKV-24 IgG produced functionally neutralizing antibodies. In 28 actively treated participants, a single dose of mRNA-1944 at 0.1, 0.3, and 0.6 mg/kg resulted in a dose-related increase in CHKV-24 IgG serum levels. Peak CHKV-24 IgG levels exceeded 1 µg/mL at all doses with a overall mean terminal half-life (t1/2) of approximately 69 days. The mRNA-encoded antibodies could safely achieve the expected therapeutically relevant serum concentrations. This indicates that encoding different classes of antibodies by mRNAs has the same potential in treating various infectious diseases other than Chikungunya [88].
Defense against chronic hepatitis B virus by mRNA-encoded antibodies
The Hepatitis B virus (HBV) causes chronic hepatitis B (CHB). Globally, there are more than hundreds of millions of patients with chronic HBV infection [126, 127]. Ying et al. used mRNA drugs to encode three anti-HBsAg antibodies, namely, G12-scFv, G12-scFv-Fc, and G12-IgG genes, for the durable suppression of HBsAg. These mRNA drugs demonstrated better efficacy than exogenous G12 antibodies in an HBV-infected mouse model. Although the three mRNA drugs had different blood concentrations, terminal elimination half-life (t1/2), and EC50 of anti-HBs, they provided sustained and effective passive immunity in mice. A single dose of mRNA-G12-LNP in mice significantly reduced HBsAg serum levels within 30 days. In contrast, the exogenous antibodies lost their effect of reducing HBsAg levels after 9 days. These findings emphasize that antibody-encoding mRNAs have great potential to combat HBV infection [128, 129].
Defense against the respiratory syncytial virus by mRNA-encoded antibodies
Respiratory infections cause millions of hospitalizations and deaths worldwide each year. Palivizumab is a broad-spectrum neutralizing antibody against the respiratory syncytial virus (RSV) and the only FDA-approved treatment for high-risk populations [130,131,132,133,134]. Santangelo et al. were the first to express synthetic mRNAs encoding intact palivizumab (secreted form, called sPali) in the lungs via an endotracheal aerosol. Later, a glycosylated phosphatidylinositol (GPI) membrane anchor sequence from the decay-accelerating factor (DAF) was attached to the heavy chain mRNA of palivizumab (anchored form, termed aPali). Both sPali and aPali forms effectively prevented infection in a mouse RSV model, and most mRNA antibodies did not alter the baseline cytokine levels. Subsequently, the authors expressed two types of RSV VHH antibodies, namely, RSV aVHH and RSV sVHH, in a homogeneous manner. mRNA-aVHH significantly inhibited RSV 7 days after transfection, and it could be present in the lungs for at least 28 days, providing long-lasting protection to mice. RSV aVHH significantly inhibited RSV and persisted in the lungs for a long, providing long-lasting protection to mice. Overall, these data suggested that mRNA-encoded antibodies prevent RSV infection, with membrane-anchored antibodies exerting a more dramatic effect than the cellular forms [135].
Tumor treatment by delivery of mRNAs encoding antibodies
Delivery of mRNAs encoding anti-PD-1 monoclonal antibody for tumor treatment
Immune checkpoints are a class of inhibitory molecules distributed on the surface of the cell membrane of immune cells, which transmit inhibitory signals to the immune cells by binding to ligands. When tumor cells express ligand molecules to interact with the immune checkpoints on the surface of the cell membrane, the immune system is not able to recognize these tumor cells, which contributes to the immune escape. The basic principle of immune checkpoint blockade therapy is to block the binding of immune checkpoints to their associated ligands through the use of immune checkpoint inhibitors (such as monoclonal antibody) [136,137,138]. PD-1 is an important immune checkpoint mainly expressed on activated T cells and binds to PD-L1 and PD-L2 ligands. Tumors evade immune cell pursuit by expressing PD-L1 on the cell surface and the PD-1/PD-L1 pathway is an important mechanism by which tumors promote immune escape [139, 140]. Pembrolizumab is an anti-PD-1 monoclonal antibody that exhibits significant antitumor efficacy and a favorable safety profile. It was approved for marketing by the FDA in 2014 [141, 142]. In June 2023, Moderna and Merck announce mRNA-4157 (V940) in combination with pembrolizumab demonstrated a statistically significant and clinically meaningful improvement in distant metastasis-free survival in patients with high-risk stage III/IV melanoma following complete resection versus pembrolizumab. This suggests that development of new oncology therapies based on pembrolizumab is possible [143, 144]. Shang et al. developed an LNP-based IVT-mRNA delivery system for delivering full-length pembrolizumab monoclonal antibodies. The results showed that in vitro pembrolizumab-mRNA has similar biological activities and functions in terms of affinity, binding specificity, blocking ability of PD-1 and PD-L1/L2, and enhancement of T cell function compared with commercial pembrolizumab. Following intravenous administration of a single dose of 2 mg/kg of mRNA-LNPs to mice, Pembrolizumab in serum exceeded 25 µg/mL for a duration of more than 35 days. In mouse experiments, the therapeutic effects of pembrolizumab-mRNAs were superior to that of protein-derived pembrolizumab. The tumors completely disappeared in five of the 10 mice injected with 2.0 mg/kg mRNA-LNPs, and there were no obvious side effects during the experiment. Moreover, in the assessment of therapeutic immunomodulation, flow cytometric analysis showed T cell activation in the experimental group. These results suggested that pembrolizumab-mRNA played a positive role in treating tumors [145]. Of course, although immune checkpoint blockade therapy is a promising tumor treatment method, it still has certain limitations. Immune checkpoint blockade therapy may cause immune-related adverse events (irAEs), hyperprogression or pseudoprogression [146]. Therefore, combination of multiple inhibitors may have better tumor-killing effects. For example, the marketed drug Opdualag (Nivolumab + Relatlimab) is combined with two immune checkpoint inhibitors, PD-1 and LAG-3, in order to obtain better anti-tumor effects [147].
Delivery of mRNAs encoding anti-HER2 monoclonal antibody for tumor treatment
Human epidermal growth factor receptor 2 (HER2) is a proto-oncogene with tyrosine kinase activity. Its overexpression leads to abnormal tumor cell proliferation [148, 149]. Trastuzumab is a humanized IgG1 monoclonal antibody that binds HER2 and exerts antitumor effects [150, 151]. Rybakova et al. designed and optimized an IVT mRNA delivery system using liver-targeted LNPs for in vivo delivery of trastuzumab-mRNA. According to the LC-MS analysis, the amino acid sequence of the trastuzumab-mRNA-encoded antibody was consistent with that of trastuzumab. Moreover, trastuzumab-mRNA had better pharmacokinetics than trastuzumab (Herceptin). Administration of 2 mg/kg mRNA to mice resulted in serum trastuzumab protein levels of approximately 40 mg/mL at 24 h, reaching 57.5 ± 7.6 mg/mL at 7 days post-injection. In contrast, serum clearance (Cl) and steady-state volume of distribution (Vss) were approximately 5-fold higher after injection with Herceptin than after injection of trastuzumab mRNA-LNPs at 30 days. Additionally, trastuzumab isolated from the sera of mice injected with IVT mRNA-LNP maintained specificity for HER2 as well as ADCC function. The full-sized antibodies produced in the livers of these mice effectively inhibited the growth of solid tumors as well as prolonged the survival of animals with HER2-positive breast cancer. Interestingly, the authors did not observe any significant toxic reactions during this process [152].
Delivery of mRNAs encoding bispecific antibodies to treat tumors
Bispecific antibodies are a bridge between target and functional cells, and stimulate a direct immune response; thus, they have promising applications in tumor immunotherapy. However, their complex manufacturing processes, short half-life, and harsh storage conditions greatly limit their clinical applications [110, 153, 154]. RiboMAbs are bispecific antibodies that bind CD3, a T-cell receptor-associated molecule, and three tumor-associated antigens (TAAs). Sahin et al. used a modified IVT mRNA for delivering RiboMAbs. This enabled sustained endogenous synthesis of antibodies that have higher terminal elimination half-lives than conventional antibodies. At the cellular level, RiboMAbs recruit peripheral blood mononuclear cells (PBMCs) to tumor cells and induce their activation ultimately causing tumor cell lysis. The RiboMAbs produced in vivo successfully eliminated the human breast cancer xenograft in NSG mice with better therapeutic efficacy than the same type of antibody purified in vitro. Notably, human PBMCs did not systemically release proinflammatory cytokines in the transplanted NSG mice, which suggests that non-specific T cell were not activated [91].
Delivery of mRNAs encoding bispecific antibodies in combination with other relevant drugs to treat tumors
Tumor-associated macrophages (TAMs) are highly concentrated and play an important role in immunosuppressing liver malignancies [155,156,157]. Liu et al. showed that CCL2 and CCL5 are important chemokines that trigger tumor-infiltrating monocytes in patients with hepatocellular carcinoma. Additionally, they attract TAM invasion and induce their differentiation to the pro-oncogenic M2 phenotype. The researchers designed a bispecific single-domain antibody for simultaneously blocking CCL2 and CCL5 (BisCCL2/5i) to reverse this immunosuppressive process. In their study, mRNAs encoding BisCCL2/5I were delivered to liver malignancies via liver-homing MC3 LNPs. A highly potent signal peptide at the N-terminal of BisCCL2/5I mediated efficient antibody secretion from the cytoplasm to the local tumor microenvironment (TME). These findings imply that BisCCL2/5i mRNA-LNPs can effectively polarize the pro-cancer M2 macrophages to the cancer-suppressive M1 macrophages and thus shift the TME to anti-tumor immunity. Interestingly, BisCCL2/5i mRNAs had a more significant effect than combined anti-CCL2 and anti-CCL5 antibodies or small molecule antagonists. Subsequently, the authors wrapped BisCCL2/5i and PD-1 ligand (PD-LI) antibody mRNAs in LNPs and administered it to mice in the same manner [158]. BisCCL2/5i along with PD-LI antibody produced a robust anti-cancer response in a mouse model of primary liver cancer as well as colorectal and pancreatic cancer with liver metastases, and achieved long-term survival of the samples. Further, the authors determined the applicability of BisCCL2/5i mRNA-LNP and PDLI mRNA-LNP delivery strategies by testing their safety in an in situ hepatocellular carcinoma model and observed no significant associated toxicities. These results suggested that the synergistic effect of dual blockade of CCL2/CCL5 by BisCCL2/5i mRNA-LNPs with PD-LI treatment can be extended to various secondary liver malignancies [159]. These findings provide a reference for the use of mRNA antibodies along with other drugs to treat the disease.
Other medical applications for the delivery of mRNA encoding antibodies
In addition to the use of mRNA antibodies to prevent viral infections and treat tumors, some researchers have tried to apply mRNA antibodies in anti-toxin and anti-bacterial infections. Thran et al. presented the results of a BoNT/A challenge experiments, where mice injected intravenously with BoNT/A were quickly poisoned and died, whereas treatment with mRNA antibodies (VNA-BoNTA-LNP) within 6 h could effectively prevent death. This suggests that mRNA antibodies have potential antitoxin capabilities [160]. Moreover, a recent study by Moderna’s team showed that mRNA delivery of IgA type antibodies (mRNA-Sal4 and mRNA-CAM003) were effective in preventing infection of mice with Salmonella and Pseudomonas aeruginosa. IgA is challenging to translate clinically due to its highly glycosylated and protease-sensitive nature. Compared to recombinant protein antibodies, mRNA encoded IgA has a better pharmacokinetic profile, and this option may provide a novel idea for the development of short-lived protein drugs [161].
Discussion
The introduction of hybridoma technology in 1975 accelerated the development of the antibody industry and numerous researchers focused on this field. The monoclonal antibody technology has recently developed rapidly and is widely used in several biomedical and clinical fields [112, 162, 163]. After hybridoma technology, new methods of antibody preparation, such as phage display technology, natural whole human library technology, and single B-cell technology, have emerged. Although these methods continuously improve, antibody production costs are still high. Fortunately, the use of mRNA antibodies can overcome this challenge. The antibody-encoding mRNAs are transiently expressed by ribosomes and the antibodies produced can act directly on the patient; thus, greatly reducing the cost and duration of antibody production [11, 13].
Despite the advantages of mRNA antibodies, the mRNA delivery technology was not originally designed for passive immunotherapy. After almost > 30 years of development, mRNA biologics are being developed primarily for prophylactic vaccination against certain potentially infectious diseases or cancer [164]. The most typical case is COVID-19 prevention using the mRNA vaccines. Here, the spike protein-encoding mRNAs deliver antigenic information to the antigen-presenting cells for triggering the body’s immune response, which allows the body to develop resistance against pathogens [165,166,167]. The development of vaccines has played a significant role in preventing the spread of infectious diseases in humans. Nonetheless, this approach of delivering antigens for inducing active immunity in the body has certain limitations. For instance, antibody production to fight against invading pathogens takes time after the first vaccination, which can be fatal for some viruses at high risk of transmission [168]. Moreover, for patients who are already affected by a disease, vaccines that focus on prevention cannot solve the problem. In such situations, delivering highly effective monoclonal or bispecific antibodies via mRNA for rapidly inducing acquired immunity against viral or tumor cells is certainly a highly effective therapeutic approach [12, 169, 170]. However, the research on mRNA-delivered antibodies is currently limited and experimental data in large mammals are still lacking. Nevertheless, the entry of mRNA CHKV-24 (NCT03829384), a monoclonal antibody against chikungunya virus, into Phase I clinical trials has taken another substantial step towards treating human diseases [88].
Conclusively, mRNA antibody drugs are a therapeutic alternative to traditional protein antibodies; yet, they face many challenges to truly enter the public eye. In recent years, in addition to mRNA drugs, some drugs regarding non-coding RNAs (like microRNAs or siRNAs) have been under development. Certain non-coding RNAs are thought to be pervasive regulators of multiple cancer hallmarks. Moreover, non-coding RNAs can play a major role in resistance to different cancer therapies by reorganizing the necessary signaling pathways [171]. For example, an agent developed against miR-16 for the treatment of Malignant pleural mesothelioma and non-small cell lung cancer has now completed phase I clinical trials [172]. Delivery of non-coding RNAs can be achieved by nanovectors, viral transduction, introduction of chemical modifications, or binding to biomolecules to achieve effective intracellular delivery and thereby facilitate receptor-mediated uptake [173, 174]. Furthermore, how to optimize them for clinical applications is a major dilemma for researchers. With technological advancements and research progress, mRNA antibody drugs may truly enter people’s lives in the future.
Availability of data and materials
Not applicable.
Abbreviations
- IVT mRNA:
-
In vitro transcribed mRNA
- TLR:
-
Toll-like receptor
- HPLC:
-
High Performance Liquid Chromatography
- FPLC:
-
Fast protein liquid chromatography
- RNAP:
-
RNA polymerase
- VEEV:
-
Venezuelan equine encephalitis virus
- DOTAP:
-
1,2-Dioleoyl-3-trimethylammonium-propane
- DSPC:
-
1, 2-distearoyl-sn-glycero-3-phosphocholine
- S.C.:
-
Subcutaneous injection
- I.C.V.:
-
Intracerebroventricular administration
- I.V.:
-
Intravenous injection
- I.T.:
-
Intratracheally administration
- VHH:
-
Variable domain of heavy chain of heavy chain antibody
- scFv:
-
Single chain antibody fragment
- PD-1:
-
Programmed cell death protein 1
- PD-L1:
-
Programmed cell death 1 ligand 1
- LC-MS:
-
Liquid Chromatograph Mass Spectrometer
- ADCC:
-
Antibody-dependent cell-mediated cytotoxicity
- STm:
-
Salmonella enterica serovar Typhimurium
- PA:
-
Pseudomonas aeruginosa
- BoNT/A:
-
Botulinum neurotoxin serotype A
- VNA:
-
VHH-based neutralizing agent
References
Crick F. Central dogma of molecular biology. Nature. 1970;227:561–3.
Jirikowski GF, Sanna PP, Maciejewski-Lenoir D, Bloom FE. Reversal of diabetes insipidus in Brattleboro rats: intrahypothalamic injection of vasopressin mRNA. Science. 1992;255:996–8.
Verbeke R, Lentacker I, De Smedt SC, Dewitte H. Three decades of messenger RNA vaccine development. Nano Today. 2019;28: 100766.
Pardi N, Hogan MJ, Porter FW, Weissman D. mRNA vaccines - a new era in vaccinology. Nat Rev Drug Discov. 2018;17:261–79.
Pardi N, Hogan MJ, Weissman D. Recent advances in mRNA vaccine technology. Curr Opin Immunol. 2020;65:14–20.
Wang Y, Zhang Z, Luo J, Han X, Wei Y, Wei X. mRNA vaccine: a potential therapeutic strategy. Mol Cancer. 2021;20:33.
Lamb YN. BNT162b2 mRNA COVID-19 vaccine: first approval. Drugs. 2021;81:495–501.
Pfizer-BioNTech. COVID-19 vaccine emergency use authorization review memorandum. Available at: https://www.fda.gov/media/144416/download.
Verbeke R, Lentacker I, De Smedt SC, Dewitte H. The dawn of mRNA vaccines: the COVID-19 case. J Control Release. 2021;333:511–20.
Huang X, Kong N, Zhang X, Cao Y, Langer R, Tao W. The landscape of mRNA nanomedicine. Nat Med. 2022;28:2273–87.
Schlake T, Thran M, Fiedler K, Heidenreich R, Petsch B, Fotin-Mleczek M. mRNA: a novel avenue to antibody therapy? Mol Ther. 2019;27:773–84.
Schlake T, Thess A, Thran M, Jordan I. mRNA as novel technology for passive immunotherapy. Cell Mol Life Sci. 2019;76:301–28.
Van Hoecke L, Roose K. How mRNA therapeutics are entering the monoclonal antibody field. J Transl Med. 2019;17:54.
Brenner S, Jacob F, Meselson M. An unstable intermediate carrying information from genes to ribosomes for protein synthesis. Nature. 1961;190:576–81.
Lockard RE, Lingrel JB. The synthesis of mouse hemoglobin beta-chains in a rabbit reticulocyte cell-free system programmed with mouse reticulocyte 9S RNA. Biochem Biophys Res Commun. 1969;37:204–12.
Dimitriadis GJ. Translation of rabbit globin mRNA introduced by liposomes into mouse lymphocytes. Nature. 1978;274:923–4.
Melton DA, Krieg PA, Rebagliati MR, Maniatis T, Zinn K, Green MR. Efficient in vitro synthesis of biologically active RNA and RNA hybridization probes from plasmids containing a bacteriophage SP6 promoter. Nucleic Acids Res. 1984;12:7035–56.
Malone RW, Felgner PL, Verma IM. Cationic liposome-mediated RNA transfection. Proc Natl Acad Sci U S A. 1989;86:6077–81.
Wolff JA, Malone RW, Williams P, Chong W, Acsadi G, Jani A, Felgner PL. Direct gene transfer into mouse muscle in vivo. Science. 1990;247:1465–8.
Martinon F, Krishnan S, Lenzen G, Magné R, Gomard E, Guillet JG, Lévy JP, Meulien P. Induction of virus-specific cytotoxic T lymphocytes in vivo by liposome-entrapped mRNA. Eur J Immunol. 1993;23:1719–22.
Conry RM, LoBuglio AF, Wright M, Sumerel L, Pike MJ, Johanning F, Benjamin R, Lu D, Curiel DT. Characterization of a messenger RNA polynucleotide vaccine vector. Cancer Res. 1995;55:1397–400.
Heiser A, Coleman D, Dannull J, Yancey D, Maurice MA, Lallas CD, Dahm P, Niedzwiecki D, Gilboa E, Vieweg J. Autologous dendritic cells transfected with prostate-specific antigen RNA stimulate CTL responses against metastatic prostate tumors. J Clin Invest. 2002;109:409–17.
Karikó K, Buckstein M, Ni H, Weissman D. Suppression of RNA recognition by toll-like receptors: the impact of nucleoside modification and the evolutionary origin of RNA. Immunity. 2005;23:165–75.
Warren L, Manos PD, Ahfeldt T, Loh YH, Li H, Lau F, Ebina W, Mandal PK, Smith ZD, Meissner A, et al. Highly efficient reprogramming to pluripotency and directed differentiation of human cells with synthetic modified mRNA. Cell Stem Cell. 2010;7:618–30.
Sahin U, Derhovanessian E, Miller M, Kloke BP, Simon P, Löwer M, Bukur V, Tadmor AD, Luxemburger U, Schrörs B, et al. Personalized RNA mutanome vaccines mobilize poly-specific therapeutic immunity against cancer. Nature. 2017;547:222–6.
Coronavirus (COVID-19) CBER-regulated biologics. Available at: https://www.fda.gov/vaccines-blood-biologics/industry-biologics/coronavirus-covid-19-cber-regulated-biologics.
Liu MA. A comparison of plasmid DNA and mRNA as vaccine technologies. Vaccines (Basel). 2019;7:37.
Lee YW, Luther DC, Kretzmann JA, Burden A, Jeon T, Zhai S, Rotello VM. Protein delivery into the cell cytosol using non-viral nanocarriers. Theranostics. 2019;9:3280–92.
Milone MC, O’Doherty U. Clinical use of lentiviral vectors. Leukemia. 2018;32:1529–41.
Li M, Li Y, Li S, Jia L, Wang H, Li M, Deng J, Zhu A, Ma L, Li W, et al. The nano delivery systems and applications of mRNA. Eur J Med Chem. 2022;227: 113910.
Steinle H, Behring A, Schlensak C, Wendel HP, Avci-Adali M. Concise review: application of in vitro transcribed messenger RNA for cellular engineering and reprogramming: progress and challenges. Stem Cells. 2017;35:68–79.
Kobiyama K, Jounai N, Aoshi T, Tozuka M, Takeshita F, Coban C, Ishii KJ. Innate immune signaling by, and genetic adjuvants for DNA vaccination. Vaccines (Basel). 2013;1:278–92.
Hopfner KP, Hornung V. Molecular mechanisms and cellular functions of cGAS-STING signalling. Nat Rev Mol Cell Biol. 2020;21:501–21.
Fu Y, Fang Y, Lin Z, Yang L, Zheng L, Hu H, Yu T, Huang B, Chen S, Wang H, et al. Inhibition of cGAS-mediated interferon response facilitates transgene expression. Science. 2020;23: 101026.
Franz KM, Neidermyer WJ, Tan YJ, Whelan SPJ, Kagan JC. STING-dependent translation inhibition restricts RNA virus replication. Proc Natl Acad Sci U S A. 2018;115:E2058-e2067.
Fus-Kujawa A, Prus P, Bajdak-Rusinek K, Teper P, Gawron K, Kowalczuk A, Sieron AL. An overview of methods and tools for transfection of eukaryotic cells in vitro. Front Bioeng Biotechnol. 2021;9: 701031.
Ferreira MV, Cabral ET, Coroadinha AS. Progress and perspectives in the development of lentiviral vector producer cells. Biotechnol J. 2021;16: e2000017.
Ni R, Zhou J, Hossain N, Chau Y. Virus-inspired nucleic acid delivery system: linking virus and viral mimicry. Adv Drug Deliv Rev. 2016;106:3–26.
Hendrie PC, Russell DW. Gene targeting with viral vectors. Mol Ther. 2005;12:9–17.
Kanapathipillai M. Treating p53 mutant aggregation-associated cancer. Cancers (Basel). 2018;10:154.
Nakanishi M, Otsu M. Development of Sendai virus vectors and their potential applications in gene therapy and regenerative medicine. Curr Gene Ther. 2012;12:410–6. https://doi.org/10.2174/156652312802762518
Sahin U, Kariko K, Tureci O. mRNA-based therapeutics–developing a new class of drugs. Nat Rev Drug Discov. 2014;13:759–80.
Chau C, Actis P, Hewitt E. Methods for protein delivery into cells: from current approaches to future perspectives. Biochem Soc Trans. 2020;48:357–65.
Fu A, Tang R, Hardie J, Farkas ME, Rotello VM. Promises and pitfalls of intracellular delivery of proteins. Bioconjug Chem. 2014;25:1602–8.
Oliver KH, Warzecha. Pharmaceutical biotechnology: drug discovery and clinical applications. 2nd ed. Hoboken: Wiley; 2012. p. 201–56.
Isaacs A, Cox RA, Rotem Z. Foreign nucleic acids as the stimulus to make interferon. Lancet. 1963;2:113–6.
Alexopoulou L, Holt AC, Medzhitov R, Flavell RA. Recognition of double-stranded RNA and activation of NF-kappaB by toll-like receptor 3. Nature. 2001;413:732–8.
Diebold SS, Kaisho T, Hemmi H, Akira S, Reis e Sousa C. Innate antiviral responses by means of TLR7-mediated recognition of single-stranded RNA. Science. 2004;303:1529–31.
Heil F, Hemmi H, Hochrein H, Ampenberger F, Kirschning C, Akira S, Lipford G, Wagner H, Bauer S. Species-specific recognition of single-stranded RNA via toll-like receptor 7 and 8. Science. 2004;303:1526–9.
Loo YM, Gale M Jr. Immune signaling by RIG-I-like receptors. Immunity. 2011;34:680–92.
Mu X, Hur S. Immunogenicity of in vitro-transcribed RNA. Acc Chem Res. 2021;54:4012–23.
Gomez-Aguado I, Rodriguez-Castejon J, Vicente-Pascual M, Rodriguez-Gascon A, Solinis MA, Del Pozo-Rodriguez A. Nanomedicines to deliver mRNA: state of the art and future perspectives. Nanomaterials (Basel). 2020;10: 364.
Merrick WC, Pavitt GD. Protein synthesis initiation in eukaryotic cells. Cold Spring Harb Perspect Biol. 2018;10: a033092.
Wilusz CJ, Wormington M, Peltz SW. The cap-to-tail guide to mRNA turnover. Nat Rev Mol Cell Biol. 2001;2:237–46.
Roundtree IA, Evans ME, Pan T, He C. Dynamic RNA modifications in gene expression regulation. Cell. 2017;169:1187–200.
Ramanathan A, Robb GB, Chan SH. mRNA capping: biological functions and applications. Nucleic Acids Res. 2016;44:7511–26.
Shanmugasundaram M, Senthilvelan A, Kore AR. Recent advances in modified cap analogs: synthesis, biochemical properties, and mRNA based vaccines. Chem Rec. 2022;22: e202200005.
Pelletier J, Schmeing TM, Sonenberg N. The multifaceted eukaryotic cap structure. Wiley Interdiscip Rev RNA. 2021;12: e1636.
Topisirovic I, Svitkin YV, Sonenberg N, Shatkin AJ. Cap and cap-binding proteins in the control of gene expression. Wiley Interdiscip Rev RNA. 2011;2:277–98.
Andries O, Mc Cafferty S, De Smedt SC, Weiss R, Sanders NN, Kitada T. N(1)-methylpseudouridine-incorporated mRNA outperforms pseudouridine-incorporated mRNA by providing enhanced protein expression and reduced immunogenicity in mammalian cell lines and mice. J Control Release. 2015;217:337–44.
Pardi N, Hogan MJ, Naradikian MS, Parkhouse K, Cain DW, Jones L, Moody MA, Verkerke HP, Myles A, Willis E, et al. Nucleoside-modified mRNA vaccines induce potent T follicular helper and germinal center B cell responses. J Exp Med. 2018;215:1571–88.
Kormann MS, Hasenpusch G, Aneja MK, Nica G, Flemmer AW, Herber-Jonat S, Huppmann M, Mays LE, Illenyi M, Schams A, et al. Expression of therapeutic proteins after delivery of chemically modified mRNA in mice. Nat Biotechnol. 2011;29:154–7.
Kariko K, Muramatsu H, Welsh FA, Ludwig J, Kato H, Akira S, Weissman D. Incorporation of pseudouridine into mRNA yields superior nonimmunogenic vector with increased translational capacity and biological stability. Mol Ther. 2008;16:1833–40.
Leppek K, Das R, Barna M. Functional 5’ UTR mRNA structures in eukaryotic translation regulation and how to find them. Nat Rev Mol Cell Biol. 2018;19:158–74.
Wang Z, Ma W, Fu X, Qi Y, Zhao Y, Zhang S. Development and applications of mRNA treatment based on lipid nanoparticles. Biotechnol Adv. 2023;65: 108130.
Vlatkovic I, Ludwig J, Boros G, Szabo GT, Reichert J, Buff M, Baiersdorfer M, Reinholz J, Mahiny AJ, Sahin U, Kariko K. Ribozyme assays to quantify the capping efficiency of in vitro-transcribed mRNA. Pharmaceutics. 2022;14: 328.
Baiersdorfer M, Boros G, Muramatsu H, Mahiny A, Vlatkovic I, Sahin U, Kariko K. A facile method for the removal of dsRNA contaminant from in vitro-transcribed mRNA. Mol Ther Nucleic Acids. 2019;15:26–35.
Baronti L, Karlsson H, Marusic M, Petzold K. A guide to large-scale RNA sample preparation. Anal Bioanal Chem. 2018;410:3239–52.
Nelissen FH, Leunissen EH, van de Laar L, Tessari M, Heus HA, Wijmenga SS. Fast production of homogeneous recombinant RNA-towards large-scale production of RNA. Nucleic Acids Res. 2012;40:e102.
Jasinski DL, Schwartz CT, Haque F, Guo P. Large scale purification of RNA nanoparticles by preparative ultracentrifugation. Methods Mol Biol. 2015;1297:67–82.
Kariko K, Muramatsu H, Ludwig J, Weissman D. Generating the optimal mRNA for therapy: HPLC purification eliminates immune activation and improves translation of nucleoside-modified, protein-encoding mRNA. Nucleic Acids Res. 2011;39:e142.
Weissman D, Pardi N, Muramatsu H, Kariko K. HPLC purification of in vitro transcribed long RNA. Methods Mol Biol. 2013;969:43–54.
Wu MZ, Asahara H, Tzertzinis G, Roy B. Synthesis of low immunogenicity RNA with high-temperature in vitro transcription. RNA. 2020;26:345–60.
Xia H, Yu B, Jiang Y, Cheng R, Lu X, Wu H, Zhu B. Psychrophilic phage VSW-3 RNA polymerase reduces both terminal and full-length dsRNA byproducts in in vitro transcription. RNA Biol. 2022;19:1130–42.
Liang Y, Huang L, Liu T. Corrigendum: development and delivery systems of mRNA vaccines. Front Bioeng Biotechnol. 2021;9: 766764.
Kowalski PS, Rudra A, Miao L, Anderson DG. Delivering the messenger: advances in technologies for therapeutic mRNA delivery. Mol Ther. 2019;27:710–28.
Tenchov R, Bird R, Curtze AE, Zhou Q. Lipid nanoparticles-from liposomes to mRNA vaccine delivery, a landscape of research diversity and advancement. ACS Nano. 2021. https://doi.org/10.1021/acsnano.1c04996.
Pardi N, Tuyishime S, Muramatsu H, Kariko K, Mui BL, Tam YK, Madden TD, Hope MJ, Weissman D. Expression kinetics of nucleoside-modified mRNA delivered in lipid nanoparticles to mice by various routes. J Control Release. 2015;217:345–51.
Vlatkovic I. Non-immunotherapy application of LNP-mRNA: maximizing efficacy and safety. Biomedicines. 2021;9: 530.
Ibba ML, Ciccone G, Esposito CL, Catuogno S, Giangrande PH. Advances in mRNA non-viral delivery approaches. Adv Drug Deliv Rev. 2021;177: 113930.
Xiao Y, Tang Z, Huang X, Chen W, Zhou J, Liu H, Liu C, Kong N, Tao W. Emerging mRNA technologies: delivery strategies and biomedical applications. Chem Soc Rev. 2022;51:3828–45.
Shuai Q, Zhu F, Zhao M, Yan Y. mRNA delivery via non-viral carriers for biomedical applications. Int J Pharm. 2021;607: 121020.
Dilliard SA, Cheng Q, Siegwart DJ. On the mechanism of tissue-specific mRNA delivery by selective organ targeting nanoparticles. Proc Natl Acad Sci USA. 2021. https://doi.org/10.1073/pnas.2109256118.
Uchida S, Perche F, Pichon C, Cabral H. Nanomedicine-based approaches for mRNA delivery. Mol Pharm. 2020;17:3654–84.
Lin CY, Perche F, Ikegami M, Uchida S, Kataoka K, Itaka K. Messenger RNA-based therapeutics for brain diseases: an animal study for augmenting clearance of beta-amyloid by intracerebral administration of neprilysin mRNA loaded in polyplex nanomicelles. J Control Release. 2016;235:268–75.
Ramaswamy S, Tonnu N, Tachikawa K, Limphong P, Vega JB, Karmali PP, Chivukula P, Verma IM. Systemic delivery of factor IX messenger RNA for protein replacement therapy. Proc Natl Acad Sci U S A. 2017;114:E1941-1950.
Riley RS, Kashyap MV, Billingsley MM, White B, Alameh MG, Bose SK, Zoltick PW, Li H, Zhang R, Cheng AY, et al. Ionizable lipid nanoparticles for in utero mRNA delivery. Sci Adv. 2021;7:7.
August A, Attarwala HZ, Himansu S, Kalidindi S, Lu S, Pajon R, Han S, Lecerf JM, Tomassini JE, Hard M, et al. A phase 1 trial of lipid-encapsulated mRNA encoding a monoclonal antibody with neutralizing activity against Chikungunya virus. Nat Med. 2021;27:2224–33.
Van Hoecke L, Verbeke R, De Vlieger D, Dewitte H, Roose K, Van Nevel S, Krysko O, Bachert C, Schepens B, Lentacker I, Saelens X. mRNA encoding a bispecific single domain antibody construct protects against influenza A virus infection in mice. Mol Ther Nucleic Acids. 2020;20:777–87.
Deng YQ, Zhang NN, Zhang YF, Zhong X, Xu S, Qiu HY, Wang TC, Zhao H, Zhou C, Zu SL, et al. Lipid nanoparticle-encapsulated mRNA antibody provides long-term protection against SARS-CoV-2 in mice and hamsters. Cell Res. 2022;32:375–82.
Stadler CR, Bahr-Mahmud H, Celik L, Hebich B, Roth AS, Roth RP, Kariko K, Tureci O, Sahin U. Elimination of large tumors in mice by mRNA-encoded bispecific antibodies. Nat Med. 2017;23:815–7.
Liu S, Cheng Q, Wei T, Yu X, Johnson LT, Farbiak L, Siegwart DJ. Membrane-destabilizing ionizable phospholipids for organ-selective mRNA delivery and CRISPR-Cas gene editing. Nat Mater. 2021;20:701–10.
Qiu M, Glass Z, Chen J, Haas M, Jin X, Zhao X, Rui X, Ye Z, Li Y, Zhang F, Xu Q. Lipid nanoparticle-mediated codelivery of Cas9 mRNA and single-guide RNA achieves liver-specific in vivo genome editing of Angptl3. Proc Natl Acad Sci USA. 2021. https://doi.org/10.1073/pnas.2020401118.
Harrison AG, Lin T, Wang P. Mechanisms of SARS-CoV-2 transmission and pathogenesis. Trends Immunol. 2020;41:1100–15.
V’Kovski P, Kratzel A, Steiner S, Stalder H, Thiel V. Coronavirus biology and replication: implications for SARS-CoV-2. Nat Rev Microbiol. 2021;19:155–70.
Kirtipal N, Bharadwaj S, Kang SG. From SARS to SARS-CoV-2, insights on structure, pathogenicity and immunity aspects of pandemic human coronaviruses. Infect Genet Evol. 2020;85: 104502.
Tao K, Tzou PL, Nouhin J, Gupta RK, de Oliveira T, Kosakovsky Pond SL, Fera D, Shafer RW. The biological and clinical significance of emerging SARS-CoV-2 variants. Nat Rev Genet. 2021;22:757–73.
Yang H, Rao Z. Structural biology of SARS-CoV-2 and implications for therapeutic development. Nat Rev Microbiol. 2021;19:685–700.
Zhu L, Deng YQ, Zhang RR, Cui Z, Sun CY, Fan CF, Xing X, Huang W, Chen Q, Zhang NN, et al. Double lock of a potent human therapeutic monoclonal antibody against SARS-CoV-2. Natl Sci Rev. 2021;8: nwaa297.
Li JQ, Zhang ZR, Zhang HQ, Zhang YN, Zeng XY, Zhang QY, Deng CL, Li XD, Zhang B, Ye HQ. Intranasal delivery of replicating mRNA encoding neutralizing antibody against SARS-CoV-2 infection in mice. Signal Transduct Target Ther. 2021;6:369.
Shi R, Shan C, Duan X, Chen Z, Liu P, Song J, Song T, Bi X, Han C, Wu L, et al. A human neutralizing antibody targets the receptor-binding site of SARS-CoV-2. Nature. 2020;584:120–4.
Zhou T, Georgiev I, Wu X, Yang ZY, Dai K, Finzi A, Kwon YD, Scheid JF, Shi W, Xu L, et al. Structural basis for broad and potent neutralization of HIV-1 by antibody VRC01. Science. 2010;329:811–7.
Karuna ST, Corey L. Broadly neutralizing antibodies for HIV prevention. Annu Rev Med. 2020;71:329–46.
Walsh SR, Seaman MS. Broadly neutralizing antibodies for HIV-1 prevention. Front Immunol. 2021;12: 712122.
Morris L, Mkhize NN. Prospects for passive immunity to prevent HIV infection. PLoS Med. 2017;14: e1002436.
Pardi N, Secreto AJ, Shan X, Debonera F, Glover J, Yi Y, Muramatsu H, Ni H, Mui BL, Tam YK, et al. Administration of nucleoside-modified mRNA encoding broadly neutralizing antibody protects humanized mice from HIV-1 challenge. Nat Commun. 2017;8: 14630.
Weiss RA, Verrips CT. Nanobodies that neutralize HIV. Vaccines (Basel). 2019;7:77.
Muyldermans S. Nanobodies: natural single-domain antibodies. Annu Rev Biochem. 2013;82:775–97.
Thakur A, Huang M, Lum LG. Bispecific antibody based therapeutics: strengths and challenges. Blood Rev. 2018;32:339–47.
Suurs FV, Lub-de Hooge MN, de Vries EGE, de Groot DJA. A review of bispecific antibodies and antibody constructs in oncology and clinical challenges. Pharmacol Ther. 2019;201:103–19.
Tian Z, Liu M, Zhang Y, Wang X. Bispecific T cell engagers: an emerging therapy for management of hematologic malignancies. J Hematol Oncol. 2021;14:75.
Buss NA, Henderson SJ, McFarlane M, Shenton JM, de Haan L. Monoclonal antibody therapeutics: history and future. Curr Opin Pharmacol. 2012;12:615–22.
Lowen AC. Constraints, drivers, and implications of influenza A virus reassortment. Annu Rev Virol. 2017;4:105–21.
Long JS, Mistry B, Haslam SM, Barclay WS. Host and viral determinants of influenza a virus species specificity. Nat Rev Microbiol. 2019;17:67–81.
Muyldermans S. Applications of nanobodies. Annu Rev Anim Biosci. 2021;9:401–21.
Muyldermans S. A guide to: generation and design of nanobodies. FEBS J. 2021;288:2084–102.
Musso D, Gubler DJ. Zika virus. Clin Microbiol Rev. 2016;29:487–524.
Baud D, Gubler DJ, Schaub B, Lanteri MC, Musso D. An update on Zika virus infection. Lancet. 2017;390:2099–109.
Miner JJ, Diamond MS. Zika virus pathogenesis and tissue tropism. Cell Host Microbe. 2017;21:134–42.
Sapparapu G, Fernandez E, Kose N, Bin C, Fox JM, Bombardi RG, Zhao H, Nelson CA, Bryan AL, Barnes T, et al. Neutralizing human antibodies prevent Zika virus replication and fetal disease in mice. Nature. 2016;540:443–7.
Erasmus JH, Archer J, Fuerte-Stone J, Khandhar AP, Voigt E, Granger B, Bombardi RG, Govero J, Tan Q, Durnell LA, et al. Intramuscular delivery of replicon RNA encoding ZIKV-117 human monoclonal antibody protects against Zika virus infection. Mol Ther Methods Clin Dev. 2020;18:402–14.
Silva LA, Dermody TS. Chikungunya virus: epidemiology, replication, disease mechanisms, and prospective intervention strategies. J Clin Invest. 2017;127:737–49.
Burt FJ, Chen W, Miner JJ, Lenschow DJ, Merits A, Schnettler E, Kohl A, Rudd PA, Taylor A, Herrero LJ, et al. Chikungunya virus: an update on the biology and pathogenesis of this emerging pathogen. Lancet Infect Dis. 2017;17:e107-17.
Weaver SC, Lecuit M. Chikungunya virus and the global spread of a mosquito-borne disease. N Engl J Med. 2015;372:1231–9.
Kose N, Fox JM, Sapparapu G, Bombardi R, Tennekoon RN, de Silva AD, Elbashir SM, Theisen MA, Humphris-Narayanan E, Ciaramella G, et al. A lipid-encapsulated mRNA encoding a potently neutralizing human monoclonal antibody protects against chikungunya infection. Sci Immunol. 2019;4:4.
Correction to Lancet Glob Health. 2017; 5: e1192–207. Lancet Glob Health. 2018; 6:e36.
Revill PA, Chisari FV, Block JM, Dandri M, Gehring AJ, Guo H, Hu J, Kramvis A, Lampertico P, Janssen HLA, et al. A global scientific strategy to cure hepatitis B. Lancet Gastroenterol Hepatol. 2019;4:545–58.
Wang W, Sun L, Li T, Ma Y, Li J, Liu Y, Li M, Wang L, Li C, Xie Y, et al. A human monoclonal antibody against small envelope protein of hepatitis B virus with potent neutralization effect. MAbs. 2016;8:468–77.
Chen B, Chen Y, Li J, Wang C, Song W, Wen Y, Lin J, Wu Y, Ying T. A single dose of Anti-HBsAg antibody-encoding mRNA-LNPs suppressed HBsAg expression: a potential cure of chronic hepatitis B virus infection. MBio. 2022;13:e0161222.
Battles MB, McLellan JS. Respiratory syncytial virus entry and how to block it. Nat Rev Microbiol. 2019;17:233–45.
Russell CD, Unger SA, Walton M, Schwarze J. The human immune response to respiratory syncytial virus infection. Clin Microbiol Rev. 2017;30:481–502.
Griffiths C, Drews SJ, Marchant DJ. Respiratory syncytial virus: infection, detection, and new options for prevention and treatment. clin microbiol rev. 2017;30:277–319.
Garegnani L, Styrmisdottir L, Roson Rodriguez P, Escobar Liquitay CM, Esteban I, Franco JV. Palivizumab for preventing severe respiratory syncytial virus (RSV) infection in children. Cochrane Database Syst Rev. 2021;11:CD013757.
Robinson KA, Odelola OA, Saldanha IJ. Palivizumab for prophylaxis against respiratory syncytial virus infection in children with cystic fibrosis. Cochrane Database Syst Rev. 2016;7:CD007743.
Tiwari PM, Vanover D, Lindsay KE, Bawage SS, Kirschman JL, Bhosle S, Lifland AW, Zurla C, Santangelo PJ. Engineered mRNA-expressed antibodies prevent respiratory syncytial virus infection. Nat Commun. 2018;9:3999.
Heinhuis KM, Ros W, Kok M, Steeghs N, Beijnen JH, Schellens JHM. Enhancing antitumor response by combining immune checkpoint inhibitors with chemotherapy in solid tumors. Ann Oncol. 2019;30:219–35.
Armand P. Immune checkpoint blockade in hematologic malignancies. Blood. 2015;125:3393–400.
Chen DS, Mellman I. Elements of cancer immunity and the cancer-immune set point. Nature. 2017;541:321–30.
Keir ME, Butte MJ, Freeman GJ, Sharpe AH. PD-1 and its ligands in tolerance and immunity. Annu Rev Immunol. 2008;26:677–704.
Ohaegbulam KC, Assal A, Lazar-Molnar E, Yao Y, Zang X. Human cancer immunotherapy with antibodies to the PD-1 and PD-L1 pathway. Trends Mol Med. 2015;21:24–33.
Poole RM. Pembrolizumab: first global approval. Drugs. 2014;74:1973–81.
England CG, Ehlerding EB, Hernandez R, Rekoske BT, Graves SA, Sun H, Liu G, McNeel DG, Barnhart TE, Cai W. Preclinical pharmacokinetics and biodistribution studies of 89Zr-labeled pembrolizumab. J Nucl Med. 2017;58:162–8.
Moderna and Merck Announce. mRNA-4157 (V940) in combination with KEYTRUDA(R) (pembrolizumab) demonstrated a statistically signiícant and clinically meaningful improvement in distant metastasis-free survival in patients with high-risk stage III/IV melanoma following complete resection versus KEYTRUDA. Available at: https://investors.modernatx.com/news/default.aspx.
Khattak A, Weber JS, Meniawy T, Taylor MH, Ansstas G, Kim KB, McKean M, Long GV, Sullivan RJ, Faries MB, et al. Distant metastasis-free survival results from the randomized, phase 2 mRNA-4157-P201/KEYNOTE-942 trial. J Clin Oncol. 2023;41:LBA9503-9503.
Wu L, Wang W, Tian J, Qi C, Cai Z, Yan W, Xuan S, Shang A. Intravenous delivery of RNA encoding anti-PD-1 human monoclonal antibody for treating intestinal cancer. J Cancer. 2022;13:579–88.
de Miguel M, Calvo E. Clinical challenges of immune checkpoint inhibitors. Cancer Cell. 2020;38:326–33.
Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, Cowey CL, Schadendorf D, Wagstaff J, Dummer R, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2019;381:1535–46.
Loibl S, Gianni L. HER2-positive breast cancer. Lancet. 2017;389:2415–29.
Oh DY, Bang YJ. HER2-targeted therapies - a role beyond breast cancer. Nat Rev Clin Oncol. 2020;17:33–48.
Keam SJ. Trastuzumab deruxtecan: first approval. Drugs. 2020;80:501–8.
Maximiano S, Magalhaes P, Guerreiro MP, Morgado M. Trastuzumab in the treatment of breast cancer. BioDrugs. 2016;30:75–86.
Rybakova Y, Kowalski PS, Huang Y, Gonzalez JT, Heartlein MW, DeRosa F, Delcassian D, Anderson DG. mRNA delivery for therapeutic Anti-HER2 antibody expression in vivo. Mol Ther. 2019;27:1415–23.
Wu Z, Cheung NV. T cell engaging bispecific antibody (T-BsAb): from technology to therapeutics. Pharmacol Ther. 2018;182:161–75.
Li H, Er Saw P, Song E. Challenges and strategies for next-generation bispecific antibody-based antitumor therapeutics. Cell Mol Immunol. 2020;17:451–61.
Pan Y, Yu Y, Wang X, Zhang T. Tumor-associated macrophages in tumor immunity. Front Immunol. 2020;11: 583084.
Cassetta L, Pollard JW. Tumor-associated macrophages. Curr Biol. 2020;30:R246-248.
Yang H, Zhang Q, Xu M, Wang L, Chen X, Feng Y, Li Y, Zhang X, Cui W, Jia X. CCL2-CCR2 axis recruits tumor associated macrophages to induce immune evasion through PD-1 signaling in esophageal carcinogenesis. Mol Cancer. 2020;19:41.
Song W, Shen L, Wang Y, Liu Q, Goodwin TJ, Li J, Dorosheva O, Liu T, Liu R, Huang L. Synergistic and low adverse effect cancer immunotherapy by immunogenic chemotherapy and locally expressed PD-L1 trap. Nat Commun. 2018;9:2237.
Wang Y, Tiruthani K, Li S, Hu M, Zhong G, Tang Y, Roy S, Zhang L, Tan J, Liao C, Liu R. mRNA delivery of a bispecific single-domain antibody to polarize tumor-associated macrophages and synergize immunotherapy against liver malignancies. Adv Mater. 2021;33: e2007603.
Thran M, Mukherjee J, Ponisch M, Fiedler K, Thess A, Mui BL, Hope MJ, Tam YK, Horscroft N, Heidenreich R, et al. mRNA mediates passive vaccination against infectious agents, toxins, and tumors. EMBO Mol Med. 2017;9:1434–47.
Deal CE, Richards AF, Yeung T, Maron MJ, Wang Z, Lai Y-T, Fritz BR, Himansu S, Narayanan E, Liu D et al. mRNA delivery of dimeric human IgA protects mucosal tissues from bacterial infection. bioRxiv. 2023.
Ecker DM, Jones SD, Levine HL. The therapeutic monoclonal antibody market. MAbs. 2015;7:9–14.
Grilo AL, Mantalaris A. The increasingly human and profitable monoclonal antibody market. Trends Biotechnol. 2019;37:9–16.
Sufian MA, Ilies MA. Lipid-based nucleic acid therapeutics with in vivo efficacy. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2023;15: e1856.
Fiolet T, Kherabi Y, MacDonald CJ, Ghosn J, Peiffer-Smadja N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: a narrative review. Clin Microbiol Infect. 2022;28:202–21.
Skowronski DM, De Serres G. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2021;384:1576–7.
Tregoning JS, Flight KE, Higham SL, Wang Z, Pierce BF. Progress of the COVID-19 vaccine effort: viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat Rev Immunol. 2021;21:626–36.
Wang L, Wu JT. Characterizing the dynamics underlying global spread of epidemics. Nat Commun. 2018;9:218.
Patel A, Bah MA, Weiner DB. In vivo delivery of nucleic acid-encoded monoclonal antibodies. BioDrugs. 2020;34:273–93.
Sanz L, Alvarez-Vallina L. Engineered mRNA and the rise of next-generation antibodies. Antibodies (Basel). 2021;10:37.
Chen B, Dragomir MP, Yang C, Li Q, Horst D, Calin GA. Targeting non-coding RNAs to overcome cancer therapy resistance. Signal Transduct Target Ther. 2022;7:121.
van Zandwijk N, Pavlakis N, Kao SC, Linton A, Boyer MJ, Clarke S, Huynh Y, Chrzanowska A, Fulham MJ, Bailey DL, et al. Safety and activity of microRNA-loaded minicells in patients with recurrent malignant pleural mesothelioma: a first-in-man, phase 1, open-label, dose-escalation study. Lancet Oncol. 2017;18:1386–96.
Diener C, Keller A, Meese E. Emerging concepts of miRNA therapeutics: from cells to clinic. Trends Genet. 2022;38:613–26.
Shah MY, Ferrajoli A, Sood AK, Lopez-Berestein G, Calin GA. microRNA therapeutics in cancer - an emerging concept. EBioMedicine. 2016;12:34–42.
Acknowledgements
The Figs. 1, 2 and 3 were created by Figdraw and Biorender, and Fig. 4 is cited in Ref [90]. We sincerely thank colleagues in the Qi Chen lab for their discussion and support. The authors are sincerely grateful to the editors of the Journal of Translational Medicine and two anonymous reviewers who provided valuable suggestions for this study.
Funding
This work was supported by the following funding sources: Natural Science Foundation of the Fujian Province, China (Grant No.2021J01206).
Author information
Authors and Affiliations
Contributions
Y.Z. planned the manuscript. YZ and LG conducted the literature search and drafted the manuscript. QC and FY revised the manuscript. All authors contributed to manuscript revision and approved the submitted version.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors report no conflicts of interest in this work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhao, Y., Gan, L., Ke, D. et al. Mechanisms and research advances in mRNA antibody drug-mediated passive immunotherapy. J Transl Med 21, 693 (2023). https://doi.org/10.1186/s12967-023-04553-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-023-04553-1