
Abstract
Background
Higher intakes of dietary antioxidants have been linked to a lower type 2 diabetes mellitus (T2DM) risk. However, few studies have comprehensively examined the overall dietary antioxidant capacity, assessed by dietary antioxidant quality scores (DAQS) and dietary total antioxidant capacity (DTAC), related to T2DM risk, especially in populations consuming relatively monotonous diets. This study aimed to evaluate the associations of DAQS, DTAC, and T2DM among rural Chinese adults.
Methods
Data from 12,467 participants from the Natural Population Cohort of Northwest China: Ningxia Project was analyzed. Dietary intake was assessed using a validated semi-quantitative food frequency questionnaire. DAQS were calculated based on vitamins A, C, and E, zinc (Zn), and selenium (Se) intake. DTAC was estimated using the ferric-reducing ability of plasma assay. Logistic regression models were used to evaluate the associations of DAQS and DTAC with T2DM risk. Restricted cubic splines were used to assess potential non-linear relationships between DTAC and T2DM.
Results
T2DM was observed in 1,238 (9.9%) participants. After adjusting for confounders, compared to the lowest tertiles (T1) of DAQS, the odds ratios (ORs) for T2DM were 1.03 (95% CI 0.82–1.30) in T2 and 0.85 (95% CI 0.68–1.06) in T3 (P = 0.010). Compared to T1, the ORs for T2DM in the highest T3 were 0.78 (95% CI 0.67–0.91, P-trend = 0.008) for vitamin A, 1.34 (95% CI 1.15–1.56, P-trend < 0.001) for vitamin E, 0.83 (95% CI 0.71–0.97, P-trend = 0.007) for Se, and 0.86 (95% CI 0.74–1.01, P-trend = 0.033) for Zn. Compared to the lowest quartile(Q1) of DTAC, the OR in the highest Q4 was 0.96 (95% CI 0.80–1.17, P-trend = 0.024) for T2DM. A non-linear relationship was observed between DATC and T2DM.
Conclusion
Higher DAQS and DATC were associated with a lower T2DM risk, suggesting that consuming antioxidant-rich foods may reduce the T2DM risk.
Similar content being viewed by others

Introduction
Type 2 diabetes mellitus (T2DM) is a prevalent metabolic disorder characterized by elevated blood glucose levels resulting from impaired insulin secretion, action, or both [1]. According to the International Diabetes Federation, the prevalence of diabetes is rising rapidly worldwide, with over 537 million adults having diabetes. In 2021, diabetes and related complications resulted in 6.7 million deaths worldwide; China has the largest diabetes epidemic in the world, with approximately 141 million people with diabetes [2].
The etiology of T2DM is complex, and its precise pathogenesis remains unclear. Recent evidence indicates that oxidative stress plays a causal and consequential role in many chronic diseases, including T2DM [3,4,5,6]. This arises from an imbalance between oxygen-free radical production and antioxidant defenses [7]. Imbalances in reactive oxygen species-mediated redox reactions can lead to chronic cardiovascular diseases, T2DM, cancer, and other disorders [8,9,10]. One study showed that elevated oxidative stress is a key factor in T2DM onset and progression, often coinciding with increased free radical generation or impairment of antioxidant systems [10]. This disrupts the balance between free radical formation and protection within cells, damaging biomolecules, including lipids, proteins, and DNA [9, 11]. In addition to oxidative stress, dietary habits are another modifiable factor that influences the progression of T2DM. One report suggested [12] that diets that regularly incorporate whole grains, fruits, vegetables, nuts, and seeds could prevent one-fifth of deaths globally. These foods contain not only dietary fiber but also antioxidants. Antioxidants neutralize free radicals at the cellular level to maintain homeostasis [13]. Some antioxidants are derived from non-enzymatic sources such as vitamins, minerals, and bioactive compounds, which are crucial in combating oxidation and oxidative stress [14,15,16]. Therefore, dietary antioxidant intake may protect against oxidative stress [17]. However, no single antioxidant reflects the total antioxidant capacity of a diet. Hence, indices to determine overall dietary antioxidant capacity are highly valuable [18]. Based on this, dietary total antioxidant capacity (DTAC) has been utilized as a useful tool to quantify dietary antioxidant content [19]. One study that investigated the association between DTAC and plasma antioxidant levels showed a strong correlation between DTAC and plasma antioxidant status [20]. Estimating total antioxidant capacity from an entire diet involves linking the total antioxidant capacity value for each food item with the amount consumed, considering the synergistic effects of dietary antioxidants rather than the effect of single antioxidants. Additionally, dietary antioxidant quality scores (DAQS) [21] are indicators used to assess dietary antioxidant status based on the daily intake of major proven antioxidant nutrients (vitamins A, C, and E, zinc [Zn], and selenium [Se]). The calculation assigns a value of 0 or 1 by comparing the intake and recommended nutrient intake (RNI) and summing the values. DAQS are sensitive and accurate [22]. Further research on indices, such as DTAC and DAQS, can provide greater insights into assessing overall dietary antioxidant capacity and guiding nutritional strategies for managing oxidative stress linked to chronic diseases.
Most studies on dietary antioxidants have focused on exploring the relationship between DAQS and various health outcomes, including bone density [22], cancer [23], cardiorespiratory fitness [24], blood pressure [25], and metabolic syndrome (MetS) [26]. Studies of disease associations with DTAC have mainly focused on hypertension [27], cardiovascular disease [13], MetS [28], and cancer [29].The findings on the relationship between DTAC and health outcomes in diabetic patients have been varied. Some studies have found that adherence to a high DTAC diet improved diabetes complications and atherosclerosis [30], reduced risks of conditions like non-alcoholic fatty liver disease [31] and gestational diabetes [32], while some case-control studies found no associations with outcomes like chronic kidney disease [33]. In China, findings on the association between dietary antioxidants and T2DM remain limited. Human nutrition science has shifted from emphasizing specific nutrients to focusing on overall dietary quality. Given the substantial differences in dietary habits and eating patterns and the relatively monotonous diet of rural populations, it is particularly important to study the relationship between overall dietary antioxidant intake and T2DM risk in the Chinese population.
Therefore, this study aimed to evaluate the associations between DAQS, DTAC, and T2DM in participants in rural Northwest Chinese populations with relatively monotonous diets.
Materials and methods
Study population
The data utilized in this cross-sectional study were obtained from the Natural Population Cohort of Northwest China: the Ningxia Project, an ongoing population-based prospective cohort study. The study design has been previously described [34]. Briefly, 15,802 participants from Wuzhong City and Shizuishan City in the Ningxia Hui Autonomous Region of China participated in baseline surveys between March 2018 and May 2019. Demographic information, semi-quantitative food frequency questionnaire (SQFFQ), and blood biochemical measurements were collected from all participants. We excluded 1 936 participants due to incomplete dietary data, and 548 with missing fasting blood glucose(FBG), 848 with missing covariate data, and 3 who reported energy intake levels < 500 kcal or > 5000 kcal. Finally, our analytical sample comprised 12,467 participants. This study was approved by the Ethics Committee of Ningxia Medical University (No. 2018-012), and all participants provided written informed consent.
General information and anthropometric measurement
General demographic information (sex and age), behavioral lifestyle factors (including smoking, alcohol consumption, and physical activity), medical history, and medication use were collected from the participants through face-to-face interviews by questionnaires. Bioelectrical impedance analysis (InBody 370 system; Biospace, Seoul, Korea) was conducted to measure waist circumference (WC) and body mass index (BMI). Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured using OMRON electronic monitors (model HEM-7124; OMRON, Tokyo, Japan). Participants sat for 5 min before obtaining two measurements at 3 to 5 min intervals. The average of the two values was used for analysis.
Biochemical measurements
Blood samples were collected from the participants in the morning after fasting for over 8 h. The samples were processed within 2 h of collection to separate serum. FBG, total cholesterol (TC), triglycerides (TG), high-density lipoprotein-cholesterol (HDL-C), and low-density lipoprotein-cholesterol (LDL-C) were analyzed on the same day using an automatic biochemical analyzer (BS-430; Mindray, Shenzhen, China).
Dietary surveys and DAQS and DTAC assessments
Dietary intake was assessed using a validated 69-item SQFFQ [35]. Participants reported their average consumption frequency over the past year for each food item with frequency choices of never or seldom, 1–3 times per month, 1–3 times per week, 4–6 times per week, or day. The frequency choices were assigned the following weights: 0, 0.07, 0.29, 0.71, or 1, respectively. The energy and nutrient content per 100 gram of each food item was determined using nutrition analysis software (Nutrition and Food Safety Institute, Chinese Center for Disease Control and Prevention, version 2.7.5.(k)). Daily energy and nutrient intake was calculated by multiplying the frequency weight by the reported amount consumed, which was then multiplied by the energy/nutrient density per gram for each food item. The nutrient intake was adjusted using the residual method.
DAQS were calculated based on the intake of five key antioxidant nutrients [21]: vitamins A, C, and E, Zn, and Se. The intake of these nutrients was compared with the RNI or adequate intake (AI) for the Chinese population, published by the China Nutrition Society in June 2013. Each nutrient was evaluated individually and assigned a score of 0 or 1. A score of 0 was given if the intake was less than two-thirds of the RNI (or AI). A score of 1 was assigned if the intake was greater than or equal to two-thirds of the RNI (or AI). The scores for the five nutrients were summed to obtain the total DAQS, ranging from 0 (poor quality) to 5 (high quality). The daily intake of antioxidant nutrients in the study population is shown in Table S1 (Additional file 1: Table S1).
To calculate the DTAC, the daily intake of each food item was multiplied by its antioxidant potential, and the results were summed to obtain the DTAC for each participant. The antioxidant potential of foods was determined using the ferric-reducing ability of plasma assay, as published in the Antioxidant Food Table by Carlsen et al., which contains the antioxidant contents of over 3100 types of foods and beverages [19]. The antioxidant value of the nearest comparable food was assigned for any food item without available antioxidant data. The total DTAC for each participant was calculated by multiplying the daily intake of each food by its antioxidant potential value and summing all foods consumed. The contributions of the 18 matched food items to the antioxidant indicators are shown in Table S2 (Additional file 1: Table S2).
Definition of variables
T2DM was defined based on the following criteria according to the Guidelines for the Prevention and Treatment of T2DM in China (2020 edition): FBG ≥ 7.0 mmol/L; self-reported previous diagnosis of T2DM; or current use of glucose-lowering medication. Physical activity was categorized as low, moderate, or high and was assessed using the International Physical Activity Questionnaire [36]. For smoking and alcohol consumption, non-users were defined as having had no use in the past year, while any other frequency of use was defined as yes. Health supplement intake was defined as the consumption of at least one of the following: fish oil/cod liver oil, vitamins, calcium/iron/Zn, ginseng products, or other supplements.
Statistical analysis
Participants were categorized into tertiles (T1-T3) based on DAQS and into quartiles(Q1-Q4) based on DTAC. Continuous variables, including age, WC, BMI, SBP, DBP, FBG, TC, TG, HDL-C, and LDL-C, are presented as mean ± standard deviation (SD) for normally distributed variables and compared between groups using Analysis of Variance (ANOVA). Categorical variables, including sex, smoking, alcohol consumption, education level, physical activity, disease of hypertension, and T2DM, are presented as numbers (%) and compared between groups using Chi-square tests. Associations between DAQS, DTAC, and T2DM were evaluated using logistic regression models after adjusting for confounders. The results are expressed as odds ratios (ORs) and 95% confidence intervals (CIs). P for trends were tested using the median of each category as a continuous variable. Furthermore, a restricted cubic spline was used to evaluate the nonlinear association between DTAC and T2DM by setting DTAC-restricted nodes to the 5th, 35th, 65th, and 95th percentiles in R software version 4.2.3. Other statistical analyses were performed using SPSS software version 23.0 (SPSS Inc., Chicago, IL, USA) and P < 0.05 was considered statistically significant.
Results
Of the 12,467 participants, 1 238 had T2DM, with a prevalence of 9.9%. As shown in Table 1, with increasing DAQS tertiles, there was a decreasing trend in age, WC, SBP, DBP and T2DM prevalence (P < 0.01). Similarly, with increasing DTAC levels, there was a decreasing trend in TC levels (P < 0.01) (Table 2). In addition, the differences in sex, education level, physical activity, smoking, alcohol consumption, TG, LDL-C, and HDL-C levels were statistically significant across DAQS and DTAC groups(P < 0.01) (Tables 1 and 2).
Tables 3 and 4 present the logistic regression analysis to explore the associations between DAQS, DTAC, and T2DM. As shown in Table 3, for DAQS, compared to the lowest T1, the unadjusted OR for T2DM in the highest T3 was 0.80 (95% CI 0.66–0.98, P = 0.002). After adjusting for potential confounding factors, the ORs for T2DM in T3 remained statistically significant, with values 0.84 (95% CI 0.68–1.05, P = 0.007) in Model 2 and 0.85 (95% CI 0.68–1.06, P = 0.010) in Model 3. Additionally, compared to the lowest T1, the adjusted ORs for T2DM in T3 were 0.78 (95% CI 0.67–0.91, P-trend = 0.008) for vitamins A, 0.83 (95% CI 0.71–0.97, P-trend = 0.007) for Se, and 0.86 (95% CI 0.74–1.01, P-trend = 0.033) for Zn. However, with increasing levels of vitamin E, the adjusted ORs for T2DM increased to 1.19 (95% CI 1.02–1.39) in T2 and 1.34 (95% CI 1.15–1.56) in T3(P-trend < 0.001).
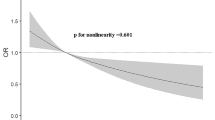
Compared to the lowest Q4 in Table 4, as DTAC levels increased, the ORs for T2DM were 1.51 (95% CI 1.27–1.79), 1.39 (95% CI 1.16–1.66) and 0.96 (95% CI 0.80–1.17), respectively, (P-trend = 0.024). Furthermore, the restricted cubic spline showed a nonlinear relationship between DTAC and T2DM (Fig. 1).

Restricted cubic spline of the relationship of T2DM with DTAC
The dash line represents the OR equal to 1. The ORs was adjusted for age, sex, smoking status, alcohol consumption, physical activity,BMI, WC, TG, HDL-C hypertension and health supplement intake
Discussion
This cross-sectional study found that higher intakes of DAQS and DTAC were associated with a lower risk of T2DM. Intake of certain individual nutrients, including vitamin A, Se, and Zn, can also be associated with reduced T2DM risk.
Recent research has emphasized the effect of specific antioxidant nutrients on health. However, information on the cumulative and interactive effects of dietary antioxidants is limited. Similarly, minimal research has been conducted on the relationship between DAQS and T2DM risk. Further studies on the association between total antioxidant vitamin and mineral intakes and T2DM are warranted. One prospective cohort study [37] that investigated DAQS and all-cause and cause-specific mortality among adults with T2DM found higher DAQS significantly correlated with reduced all-cause mortality (HR=0.70, 95% CI 0.53–0.92 for the highest vs. the lowest DAQS quartiles). This indicates that adequate intake of antioxidant micronutrients may reduce mortality in patients with T2DM. However, in a study that involved an obese Iranian population, [25] higher DAQS were only positively associated with a lower DBP, with no significant relationships observed between DAQS and serum lipids, glycemic markers, or insulin resistance biomarkers. A randomized, double-blind, placebo-controlled primary prevention trial undertaken in France examined the effects of 7.5 years of antioxidant supplementation on the incidence of MetS [38]. The correlations between baseline serum antioxidant levels and prospective MetS risk were also assessed. MetS incidence was negatively associated with baseline serum-carotene and vitamin C levels but positively associated with Zn levels. Although not statistically significant, increased baseline vitamin E and Se levels were associated with an increased risk of MetS. Another analysis of European populations found a strong negative association between plasma vitamin C levels and T2DM risk [39]. Compared with the bottom quintile of plasma vitamin C, the top quintile had 62% lower odds of developing T2DM. However, a study that involved Lebanese adults found that plasma Se levels were positively correlated with all MetS components, including glucose (r = 0.105, P = 0.037) [40]. In contrast, plasma Zn levels did not correlate with any of these components. Therefore, findings from research on various nutrients and T2DM risk are inconsistent. Here, we found vitamin A, Se, Zn (only in Models 1 and 3) and DAQS to be negatively correlated with T2DM risk, while vitamins C (only in Model 2) and E were positively correlated. Compared with the Chinese RNI, the highest tertile had higher vitamin A and Se levels. Antioxidants are primarily derived from animal organs, seafood, and meat. However, this study group had high vitamin A intake due to the consumption of animal organs and red meat, and some studies have suggested uncertainty about how T2DM affects vitamin A metabolism [41]. Dietary vitamin A intake in patients with T2DM may vary depending on factors such as the study population, dietary habits, food diversity, regional socioeconomic status, and genetics. Vitamin E is a fat-soluble vitamin primarily obtained from vegetable oils, nuts, and seeds. In our study population, the vitamin E levels in the lowest tertile group were significantly higher than the AI of 14 mg for Chinese residents because of the large amounts of oil and salt used in cooking. Regardless of sex, 0% of the participants had vitamin E levels below two-thirds of the AI. While one study showed that vitamin E intake reduced the T2DM risk [42], another study showed that high doses may promote oxidative stress [43]. This may explain the positive correlation between vitamin E levels and T2DM risk observed in our study. Vitamin C is a water-soluble vitamin primarily obtained from fruits and vegetables. Our study participants had a low intake of these food sources, with male and female participants having intakes below two-thirds of the RNI at 73.8% and 71.2%, respectively. Research suggests that FFQs may overestimate fruit and vegetable consumption compared with more detailed dietary assessments [44]. Therefore, the actual intake of fruits and vegetables, and thus vitamin C, in our participants was likely to be even lower than that suggested by the results, indicating that more individuals had inadequate vitamin C intake below two-thirds of the RNI. A study [45] have indicated that vitamin C intake and serum vitamin C levels were negatively correlated with fasting blood glucose. Low vitamin C intake and/or insufficient serum levels can increase mortality risk in patients with T2DM (HR 1.25, 95% CI 1.05–1.49 and 1.84, 95% CI 1.10–3.08). The study recommends vitamin C intake, including supplementing 500–1000 mg/day of vitamin C, as potentially more beneficial for American adults with diabetes or prediabetes. Based on this study, we speculate that this may be why the vitamin C results were not significant. If adequate vitamin C intake is consumed, it may be inversely associated with the risk of developing T2DM. Currently, research findings on Zn are inconsistent. A randomized trial [37] found that Zn was positively associated with the risk of MetS. However, prospective evidence showed [46] an inverse association between Zn intake and T2DM risk. A clinical controlled trial found [47] that Zn supplementation reduced blood glucose and insulin resistance while improving β-cell function. Another clinical controlled trial [48] in obese women came to the same conclusion. In our study, we also found that Zn was inversely associated with the risk of T2DM (only significant in Model 1 and Model 3).
The epidemiological evidence on the relationship between DTAC and T2DM risk is limited. However, some large cohort studies have reported such correlations. One prospective study in French women found that high DTAC levels were associated with lower T2DM risk (HR=0.73, highest quintile) [49]. Another cohort study that involved adults aged ≥ 45 years also found that a higher DTAC correlated with a lower T2DM risk [50]. That study observed a correlation between DTAC and prediabetes in men but not in women, whereas the association with insulin resistance was slightly stronger in women. This potential sex difference may be related to differences in visceral fat. A Hertfordshire cohort study in the British population found negative correlations between DTAC and fasting insulin, insulin resistance, and glucose tolerance using four DTAC measurement methods [51]. However, all the aforementioned studies were conducted involving non-Chinese populations, and currently, evidence regarding the association between DTAC use and T2DM risk in Chinese populations is lacking. In this study, although the risk of T2DM gradually decreased with increasing DTAC levels, DTAC was a risk factor for T2DM in the Q2 and Q3 groups and only a protective factor in the highest quartile Q4 group. There are two potential reasons for this finding. First, the dietary patterns in populations assessed in other studies differ greatly from those in our study region. In those previous study populations, more antioxidant-rich foods, such as coffee, nuts, red wine, deep-sea fish, and olive oil, were consumed; however, our study population rarely consumed these types of antioxidants. A study conducted among the Polish population found a significant inverse relationship between DTAC and prediabetes prevalence, with the Q1 group having < 8.37 mmol/day and the Q4 group having > 14.51 mmol/day [52]; whereas our study had significantly lower DTAC values, with only < 1.34 mmol/day in the Q1 group and > 4.06 mmol/day in the Q4 group. Second, while databases used to assess the total antioxidant content of the diet have been established in many other countries, some foods lack accurate antioxidant potential values, with similar foods being used as substitutes. Accordingly, further research is warranted to investigate the effects of DAQS and DTAC on T2DM in different populations.
Our study provides epidemiological evidence concerning the relationship between antioxidants, DAQS, DTAC, and T2DM risk in the dietary intake of the Chinese population. However, our study has some limitations. First, because our study participants were from rural areas in Northwest China, their daily food consumption was relatively uniform and single, which may limit the generalizability of the results. Second, we used an SQFFQ to estimate the participants’ dietary intake frequency over the past year, which may introduce subjective recall bias and pose challenges in accurately assessing dietary habits. Third, although we extensively adjusted for all potential confounding variables, we cannot completely exclude unmeasured confounding factors. Finally, as with all cross-sectional studies, we could not establish a causal relationship between the DAQS, DTAC, and T2DM.
In this study of rural populations in northwest China, significant inverse associations were observed between DAQS, DTAC and decreased risk of T2DM. A non-linear relationship was found between DATC and T2DM. These findings suggest that incorporating antioxidant-rich foods into the diet may help reduce the risk of T2DM.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- T2DM:
-
Type 2 diabetes mellitus
- DAQS:
-
Dietary antioxidant quality scores
- DTAC:
-
Dietary total antioxidant capacity
- Zn:
-
Zinc
- Se:
-
Selenium
- RNI:
-
Recommended nutrient intake
- MetS:
-
Metabolic syndrome
- SQFFQ:
-
Semi-quantitative food frequency questionnaire
- FBG:
-
Fasting blood glucose
- WC:
-
Waist circumference
- BMI:
-
Body mass index
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- HDL-C:
-
High-density lipoprotein-cholesterol
- LDL-C:
-
Low-density lipoprotein-cholesterol
- AI:
-
Adequate intake
- ORs:
-
Odds ratios
- CIs:
-
Confidence intervals
References
Tamarai K, Bhatti JS, Reddy PH. Molecular and cellular bases of diabetes: focus on type 2 diabetes mouse model-TallyHo. Biochim Biophys Acta Mol Basis Dis. 2019;1865(9):2276–84.
International Diabetes Federation. Homepage [Available from: https://diabetesatlas.org/.
Vassalle C, Maltinti M, Sabatino L. Targeting oxidative stress for Disease Prevention and Therapy: where do we stand, and where do we go from Here. Molecules. 2020;25(11).
Eruygur NK, Taslimi UM, Atas P, Tekin M, Gulcin M. I. Screening the in vitro antioxidant, antimicrobial, anticholinesterase, antidiabetic activities of endemic Achillea cucullata (Asteraceae) ethanol extract. South Afr J Bot. 2019;120.
Durmaz L, Erturk A, Akyüz M, Polat Kose L, Uc EM, Bingol Z et al. Screening of Carbonic anhydrase, acetylcholinesterase, butyrylcholinesterase, and α-Glycosidase enzyme Inhibition effects and antioxidant activity of Coumestrol. Molecules. 2022;27(10).
Durmaz L, Kiziltas H, Guven L, Karagecili H, Alwasel S, Gulcin İ. Antioxidant, antidiabetic, anticholinergic, and Antiglaucoma effects of Magnofluorine. Molecules. 2022;27(18).
Rahimi R, Nikfar S, Larijani B, Abdollahi M. A review on the role of antioxidants in the management of diabetes and its complications. Biomed Pharmacother. 2005;59(7):365–73.
Heitzer T, Schlinzig T, Krohn K, Meinertz T, Münzel T. Endothelial dysfunction, oxidative stress, and risk of cardiovascular events in patients with coronary artery disease. Circulation. 2001;104(22):2673–8.
Jelic MD, Mandic AD, Maricic SM, Srdjenovic BU. Oxidative stress and its role in cancer. J Cancer Res Ther. 2021;17(1):22–8.
Maritim AC, Sanders RA, Watkins JB 3. Diabetes, oxidative stress, and antioxidants: a review. J Biochem Mol Toxicol. 2003;17(1):24–38.
Tu W, Wang H, Li S, Liu Q, Sha H. The anti-inflammatory and anti-oxidant mechanisms of the Keap1/Nrf2/ARE Signaling Pathway in Chronic diseases. Aging Dis. 2019;10(3):637–51.
Evans DB, Etienne C. Health systems financing and the path to universal coverage. Bull World Health Organ. 2010;88(6):402.
da Silva A, Caldas APS, Pinto SL, Hermsdorff HHM, Marcadenti A, Bersch-Ferreira ÂC, et al. Dietary total antioxidant capacity is inversely associated with cardiovascular events and cardiometabolic risk factors: a cross-sectional study. Nutrition. 2021;89:111140.
Leyla PK, Zeynebe B, Ruya K, Hulya CGA, Lokman A. Anticholinergic and antioxidant activities of avocado (Folium Perseae) leaves– phytochemical content by LC-MS/MS analysis. Int J Food Prop. 2020;23(1):878–93.
Durmaz L, Karagecili H, Gulcin İ. Evaluation of Carbonic anhydrase, acetylcholinesterase, butyrylcholinesterase, and α-Glycosidase inhibition effects and antioxidant activity of Baicalin Hydrate. Life (Basel). 2023;13(11).
Karagecili H, Yılmaz MA, Ertürk A, Kiziltas H, Güven L, Alwasel SH et al. Comprehensive Metabolite profiling of Berdav Propolis using LC-MS/MS: determination of antioxidant, anticholinergic, Antiglaucoma, and Antidiabetic effects. Molecules. 2023;28(4).
de la Iglesia R, Lopez-Legarrea P, Celada P, Sánchez-Muniz FJ, Martinez JA, Zulet MA. Beneficial effects of the RESMENA dietary pattern on oxidative stress in patients suffering from metabolic syndrome with hyperglycemia are associated to dietary TAC and fruit consumption. Int J Mol Sci. 2013;14(4):6903–19.
Ha K, Kim K, Sakaki JR, Chun OK. Relative validity of Dietary total antioxidant capacity for Predicting all-cause mortality in comparison to Diet Quality indexes in US adults. Nutrients. 2020;12(5).
Carlsen MH, Halvorsen BL, Holte K, Bøhn SK, Dragland S, Sampson L, et al. The total antioxidant content of more than 3100 foods, beverages, spices, herbs and supplements used worldwide. Nutr J. 2010;9:3.
Wang Y, Yang M, Lee SG, Davis CG, Koo SI, Chun OK. Dietary total antioxidant capacity is associated with diet and plasma antioxidant status in healthy young adults. J Acad Nutr Diet. 2012;112(10):1626–35.
Tur JA, Serra-Majem L, Romaguera D, Pons A. Does the diet of the balearic population, a Mediterranean type diet, still provide adequate antioxidant nutrient intakes? Eur J Nutr. 2005;44(4):204–13.
Rivas A, Romero A, Mariscal-Arcas M, Monteagudo C, López G, Lorenzo ML, et al. Association between dietary antioxidant quality score (DAQs) and bone mineral density in Spanish women. Nutr Hosp. 2012;27(6):1886–93.
Pascual-Geler M, Robles-Fernandez I, Monteagudo C, Lopez-Guarnido O, Rodrigo L, Gálvez-Ontiveros Y, et al. Impact of oxidative stress SNPs and dietary antioxidant quality score on prostate cancer. Int J Food Sci Nutr. 2020;71(4):500–8.
Shahinfar H, Shahavandi M, Jibril AT, Djafarian K, Clark CCT, Shab-Bidar S. The Association between dietary antioxidant quality score and Cardiorespiratory Fitness in Iranian adults: a cross-sectional study. Clin Nutr Res. 2020;9(3):171–81.
Nikrad N, Shakarami A, Tousi AZ, Farhangi MA, Ardekani AM, Jafarzadeh F. Dietary antioxidant quality score (DAQS), serum lipids, markers of glucose homeostasis, blood pressure and anthropometric features among apparently metabolically healthy obese adults in two metropolises of Iran (Tabriz and Tehran): a cross-sectional study. BMC Endocr Disord. 2023;23(1):157.
Shahavandi M, Shahinfar H, Payande N, Sheikhhossein F, Djafarian K, Shab-Bidar S. The association between dietary antioxidant quality score with metabolic syndrome and its components in Iranian adults: a cross-sectional study. Food Sci Nutr. 2021;9(2):994–1002.
Villaverde P, Lajous M, MacDonald CJ, Fagherazzi G, Bonnet F, Boutron-Ruault MC. High dietary total antioxidant capacity is associated with a reduced risk of hypertension in French women. Nutr J. 2019;18(1):31.
Farhangi MA. Dietary total antioxidant capacity significantly interacts with 6-P21 rs2010963 gene polymorphisms in terms of cardio-metabolic risk factors in patients with metabolic syndrome. BMC Res Notes. 2020;13(1):145.
Yu YC, Paragomi P, Wang R, Jin A, Schoen RE, Sheng LT, et al. Composite dietary antioxidant index and the risk of colorectal cancer: findings from the Singapore Chinese Health Study. Int J Cancer. 2022;150(10):1599–608.
Jafari Azad B, Yaseri M, Daneshzad E, Koohdani F. Interaction between apo A-II -265T > C polymorphism and dietary total antioxidant capacity on some anthropometric indices and serum lipid profile in patients with type 2 diabetes mellitus. J Nutr Sci. 2021;10:e9.
Salavatizadeh M, Soltanieh S, Poustchi H, Yari Z, Shabanpur M, Mansour A, et al. Dietary total antioxidant capacity is inversely associated with the odds of non-alcoholic fatty liver disease in people with type-2 diabetes. Front Nutr. 2022;9:1037851.
Daneshzad E, Tehrani H, Bellissimo N, Azadbakht L. Dietary total antioxidant capacity and gestational diabetes Mellitus: a case-control study. Oxid Med Cell Longev. 2020;2020:5471316.
Abbasi M, Daneshpour MS, Hedayati M, Mottaghi A, Pourvali K, Azizi F. Dietary total antioxidant capacity and the risk of chronic kidney disease in patients with type 2 diabetes: a nested case-control study in the Tehran lipid glucose study. J Ren Nutr. 2019;29(5):394–8.
Yang C, Liu X, Li J, Yan N, Dang Y, Chang Z, et al. Association of Serum Vitamin D and estradiol levels with metabolic syndrome in Rural women of Northwest China: a cross-sectional study. Metab Syndr Relat Disord. 2022;20(3):182–9.
Yan N, Li N, Liu W, Li X, Liu X, Zhang P, et al. Validity and reliability of a semi-quantitative food frequency questionnaire in groups at high risk for cardiovascular diseases. Nutr J. 2022;21(1):63.
Patterson E. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)-Short and Long Forms. 2005.
Wang W, Wang X, Cao S, Duan Y, Xu C, Gan D, et al. Dietary antioxidant indices in relation to all-cause and cause-specific mortality among adults with diabetes: a prospective cohort study. Front Nutr. 2022;9:849727.
Czernichow S, Vergnaud AC, Galan P, Arnaud J, Favier A, Faure H, et al. Effects of long-term antioxidant supplementation and association of serum antioxidant concentrations with risk of metabolic syndrome in adults. Am J Clin Nutr. 2009;90(2):329–35.
Harding AH, Wareham NJ, Bingham SA, Khaw K, Luben R, Welch A, et al. Plasma vitamin C level, fruit and vegetable consumption, and the risk of new-onset type 2 diabetes mellitus: the European prospective investigation of cancer–Norfolk prospective study. Arch Intern Med. 2008;168(14):1493–9.
Obeid O, Elfakhani M, Hlais S, Iskandar M, Batal M, Mouneimne Y, et al. Plasma copper, zinc, and selenium levels and correlates with metabolic syndrome components of Lebanese adults. Biol Trace Elem Res. 2008;123(1–3):58–65.
Zhang Y, Wang T, Hu X, Chen G. Vitamin A and diabetes. J Med Food. 2021;24(8):775–85.
Montonen J, Knekt P, Järvinen R, Reunanen A. Dietary antioxidant intake and risk of type 2 diabetes. Diabetes Care. 2004;27(2):362–6.
Aggarwal BB, Sundaram C, Prasad S, Kannappan R. Tocotrienols, the vitamin E of the 21st century: its potential against cancer and other chronic diseases. Biochem Pharmacol. 2010;80(11):1613–31.
Bingham SA. Dietary assessments in the European prospective study of diet and cancer (EPIC). Eur J Cancer Prev. 1997;6(2):118–24.
Sun H, Karp J, Sun KM, Weaver CM, Decreasing Vitamin C, Intake. Low serum vitamin C level and risk for US adults with diabetes. Nutrients. 2022;14:19.
Sun Q, van Dam RM, Willett WC, Hu FB. Prospective study of zinc intake and risk of type 2 diabetes in women. Diabetes Care. 2009;32(4):629–34.
Ranasinghe P, Wathurapatha WS, Galappatthy P, Katulanda P, Jayawardena R, Constantine GR. Zinc supplementation in prediabetes: a randomized double-blind placebo-controlled clinical trial. J Diabetes. 2018;10(5):386–97.
Marreiro DN, Geloneze B, Tambascia MA, Lerário AC, Halpern A, Cozzolino SM. Effect of zinc supplementation on serum leptin levels and insulin resistance of obese women. Biol Trace Elem Res. 2006;112(2):109–18.
Mancini FR, Affret A, Dow C, Balkau B, Bonnet F, Boutron-Ruault MC, et al. Dietary antioxidant capacity and risk of type 2 diabetes in the large prospective E3N-EPIC cohort. Diabetologia. 2018;61(2):308–16.
van der Schaft N, Schoufour JD, Nano J, Kiefte-de Jong JC, Muka T, Sijbrands EJG, et al. Dietary antioxidant capacity and risk of type 2 diabetes mellitus, prediabetes and insulin resistance: the Rotterdam Study. Eur J Epidemiol. 2019;34(9):853–61.
Okubo H, Syddall HE, Phillips DI, Sayer AA, Dennison EM, Cooper C, et al. Dietary total antioxidant capacity is related to glucose tolerance in older people: the Hertfordshire Cohort Study. Nutr Metab Cardiovasc Dis. 2014;24(3):301–8.
Cyuńczyk M, Zujko ME, Jamiołkowski J, Zujko K, Łapińska M, Zalewska M et al. Dietary total antioxidant capacity is inversely Associated with prediabetes and Insulin Resistance in Bialystok PLUS Population. Antioxid (Basel). 2022;11(2).
Acknowledgements
We thank all participants and staff working for the China Northwest Natural Population Cohort, Ningxia Project.
Funding
This study was supported by the Natural Science Foundation of Ningxia Province(2023AAC03163); National Natural Science Foundation of China(grant number 82060592); the Key Research and Development Program of Ningxia Hui Autonomous Region(2021BEG02026); the National Key Research and Development Project Ningxia cohort from China Northwest Cohort(2017YFC0907204).
Author information
Authors and Affiliations
Contributions
YZ and YZ conceived and designed the research. XL, YX, YZ, QW, JQ, JZ and CY contributed to collect the data. XL and YX conducted experiments, analyzed data and drafted the manuscript. YZ and YZ contributed to revising the paper. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Ningxia Medical University (No. 2018-012).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
12986_2024_786_MOESM1_ESM.docx
Supplementary Material: Table S1. Daily intake of the antioxidant nutrients in the study population; Table S2. Food contributors to the dietary total antioxidant capacity.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, X., Xue, Y., Zhang, Y. et al. Association between dietary antioxidant capacity and type 2 diabetes mellitus in Chinese adults: a population-based cross-sectional study. Nutr Metab (Lond) 21, 16 (2024). https://doi.org/10.1186/s12986-024-00786-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12986-024-00786-z