
Abstract
Background
Previous research has investigated the association between attachment styles and smoking behaviors, indicating a positive association of insecure attachment styles with nicotine dependence. However, these links were mostly explored in adolescent and student samples. Moreover, the explanatory mechanisms and the variables influencing the strength of this relationship remained understudied. In this context, the present study aims to: (1) examine the associations between attachment anxiety, avoidance, and nicotine dependence; (2) investigate the mediating role of emotion dysregulation and metacognitions about smoking; and (3) test the moderating roles of psychological capital and type of tobacco product used by the participants.
Method
This cross-sectional study was conducted on a convenience sample of 447 participants who reported smoking. The age range of participants was 18 to 64 (M = 26.76; 59.7% women). All participants have completed five questionnaires measuring nicotine dependence, adult attachment, emotion dysregulation, metacognitions about smoking, and psychological capital. They also reported the type of tobacco product commonly used: classic cigarettes, e-cigarettes, or heated tobacco products.
Results
Our findings show that the direct link between insecure attachment and nicotine dependence is rather inconsistent. However, it was mediated by the metacognitions about smoking. Psychological capital can act as a protective factor against the effects of attachment on nicotine dependence, especially for those using alternative tobacco products alongside classic cigarettes.
Conclusions
The findings highlight the possibility of developing better-tailored interventions and treatments to discourage smoking and increase smoking cessation. These should focus on eliminating the dysfunctional beliefs related to the metacognitions about smoking and on improving the levels of psychological capital. In addition, targeting attachment insecurities in early adolescence can also function as a mean to prevent smoking.
Similar content being viewed by others


Introduction
Tobacco use is recognized as a leading cause of preventable death in many countries as using combustible tobacco products is associated with pulmonary disease, cardiovascular disease, and other forms of chronic illness [1]. Moreover, in recent years, the market for products containing nicotine has become more complex after the introduction of smokeless devices (such as electronic cigarettes) and heated tobacco products. While such new devices received some attention in regard to their effects and usefulness (see Ratajczak et al., 2020 [2] and Zakiyah et al., 2021 [3] for reviews), few studies compared the psychological mechanisms leading to, maintaining, and reducing nicotine dependence among the users of various products containing nicotine. Various environmental (exposure to tobacco adverts), social (tobacco use by peers or family), genetic (genes associated with dopaminergic neurotransmitter system, cellular transport system or serotonergic neurotransmitter system, among others) and psychological factors were previously related to smoking and smoking addiction [4,5,6,7,8]. An emerging body of literature has suggested that attachment theory is well-suited for understanding various addictions, including nicotine addiction [9,10,11,12,13,14]. Past research shows the impact of attachment styles on metacognitions [15] and difficulties in the control of emotions [16, 17], which may drive smoking and other related behaviors [16, 18]. The first aim was to investigate the associations between insecure attachment, metacognitions, emotional dysregulation and nicotine dependence. Also, given the large prevalence of nicotine addiction and that most available research focused on psychological vulnerabilities to addiction, we investigated a potential protective factor that could reduce nicotine addiction. As a second aim, the study tested the moderating role of psychological capital in the aforementioned relationship, since other studies showed that it is linked with lower levels of addiction, including smoking [19]. Finally, we aim to test how these relationships differ based on the nicotine-containing products used by the participants.
Attachement and nicotine dependence
The theory of attachment represents an essential theoretical framework not only for the study of personality development, interpersonal relationships, and emotion (dys)regulation but also for addiction. Past studies reported that secure attachment is negatively associated with nicotine dependence, while insecure attachment is positively associated with nicotine dependence, early smoking onset and a higher likelihood of having a cigarette smoking experience [11, 13]. Moreover, Wise et al. [1] indicated that the prevalence of smoking among securely attached individuals (23.5%) was lower compared to that among groups with dismissing (27.8%) or fearful (30.2%) attachment styles. Another study’s findings indicated that compared to people who do not smoke, those who do smoke have a more anxious style and feel lonelier [12].
Shaver and Mikulincer [20] proposed a model that explains how the attachment works. The attachment system is activated by real or imagined stressors, which make people believe that they cannot rely on their own resources to fulfill their needs, and therefore seek the proximity of attachment figures. For more secure individuals this strategy is working, they experience a sense of security when their care needs are met. But the same strategy does not work for insecure people, who are pushed to develop secondary strategies. More avoidantly attached individuals use a deactivation strategy (for example, hyper-focusing on incompatibilities or thinking that one is better off alone) that prevents seeking support from their attachment figure. Individuals with an anxious attachment tend to use a hyperactivation strategy (for example, starting a fight) to maintain closeness, but actively seek any sign of unresponsiveness from their attachment figures. More recently, Fairbairn et al. [10] used meta-analytic techniques on 34 prospective studies to test if close relationships represent a vulnerability factor for the later development of substance use. The results indicated that insecure attachment precedes and is longitudinally associated with the development of later substance use problems, such as alcohol, marijuana, or smoking [10]. Both attachment and substance addiction are believed to involve higher-order cognitive processes centred around cognitions related to the self. Shaver et al. [21] indicated that attachment anxiety and avoidance interfere with healthy self-approval, self-acceptance, and self-compassion. At the same time, certain drugs are repeatedly used due to their ability to reduce feelings of negative self-awareness [22]. Moreover, neuroscientists have indicated the overlap of the brain systems involved in attachment and those associated with addiction (e.g., dopamine, opioids, and corticotropin-releasing factors) [23].
The mediating role of emotion dysregulation and metacognitive beliefs
Emotion dysregulation
Emotion dysregulation refers to deficits in awareness, understanding, and acceptance of emotions, as well as the ability to manage one’s emotional experience [24]. It appears more often in more insecure people, both anxious and avoidant, due to their inability to satisfy their attachment needs. This leads to use of maladaptive or rigid emotion regulation strategies to achieve one’s goals, including avoidance, denial, aggression, rumination, or venting [25]. Psychoactive substances use can also operate as an external mean of regulating emotions, showing a shift from a positive to a negative function in emotion regulation with repeated exposure [10]. Emotion dysregulation mediates the relationship between both anxious and avoidant attachment and addiction to alcohol, marijuana, and texting, indicating that insecure attachment, specifically anxious attachment and emotion dysregulation may be important psychological characteristics that increase the risk for addictive behaviors [17].
Metacognition
Metacognitive beliefs (or metacognitions) comprise knowledge, processes, and strategies that appraise, monitor, or control cognition. Most studies have shown the role of metacognitive beliefs in many psychological problems and psychopathologies, including addiction [15].
Metacognitions were shown to be related to smoking behaviors and addiction [16, 18, 26, 27], since they intensify negative emotions, which increase the likelihood to engage in the addictive behavior as a means of cognitive–affective self-regulation More recently, Spada et al. [18] diferentiated between positive (“Thinking about having a cigarette will make me feel better”) and negative (“I cannot control my thoughts of smoking”) metacognitive beliefs, which are developed and maintained in all three phases of addictive behavior: pre-engagement, engagement and post-engagement. Despite the scarce research in this specific area, it has been suggested that insecure attachment styles lead to the development of maladaptive metacognitions, which in turn lead to the engagement in dysfunctional cognitive and emotional regulation strategies [28, 29]. Also, attachment security allows people to consider negative thoughts and emotions as temporary events and explore the world with attentional flexibility [28]. In a similar study, metacognitions were found to mediate the link between attachment styles and problematic Facebook use [30].
The moderating roles of psychologial capital and type of tobacco product
Psychological capital
Psychological capital is a higher-order construct, representing a positive psychological state experienced by someone in the process of growth and development, which comprise four positive psychological resources: self-efficacy, hope, optimism, and resilience [31].
Psychological capital has strong positive associations with both psychological well-being, and subjective well-being, and negative associations with depression and anxiety [32]. Also, lower psychological capital levels predict negative emotional states, such as anxiety and exhaustion [33], while positive psychological capital may help individuals avoid negative emotions such as anxiety and uncertainty [34]. Thus, higher levels of psychological capital may provide the necessary coping resources to help individuals deal with the environmental strains leading to addictions. Indeed, psychological capital acts as a protective factor against smartphone or social media addiction and relapse tendencies among people who consume substances [35,36,37]. Moreover, optimism, as a component of psychological capital, was related to reduced smoking [19].
Type of tobacco products
In recent years, non-combustible forms of nicotine/ tobacco use, such as electronic cigarettes (e-cigarettes) and heated tobacco products (HTPs), have been introduced as potentially less-risky alternatives to traditional combusted tobacco products, including classic cigarettes. Some research reported improvements in levels of biomarkers of tobacco smoke exposure and biological effects, for both e-cigarette and HTP users [38]. While the balance of harms and benefits of these new types of smoking is constantly in debate, the dual use of these products, the high use among the young generation and among those who never smoked indicate the need for close monitoring of these new smoking products, as well as for their prevalence and user characteristics [39, 40]. There is experimental evidence showing that attachment to material objects can serve a compensatory function against the threat to attachment security posed by the close others’ perceived unreliability [41]. For example, for more anxious persons, the cigarette or any smoking device may become an attachment target itself, or a way to become closer and receive the support of a human attachment target (e.g., that of a romantic partner). Thus, in the present study, we examine if the type of tobacco products can act as a moderator of the relationship between attachment, metacognitions, emotional dysregulation and nicotine addiction, suggesting the possible presence of some individual differences among users of various types of products.
Overview of the present study
Considering the above findings, we aimed to identify how various psychological processes are related to tobacco addiction. Past research indicated that insecure attachment, emotional dysregulation and maladaptive metacognitions were related to smoking behaviors [11,12,13, 26, 42, 43]. However, these studies considered the variables separately and many of them investigated other types of addictions. Although some of the mechanisms related to addiction may be similar regardless of the type of addiction, a more comprehensive view regarding smoking and tobacco addiction is needed to drive the necessary psychotherapeutic interventions. Also, while many studies (including those cited above) took into account multiple risk factors of tobacco addiction, very few considered the protective factors that could reduce addictive behaviors. Psychological capital is a resource that was previously shown to be a protective factor against various types of addiction [35,36,37]. As such, we included it in our model. Third, although individuals use nowadays various smokeless devices and heated tobacco products as alternative to classic cigarettes, there is a scarcity of studies investigating the psychological mechanism that are behind using such products. Testing our proposed model among classic cigarettes, e-cigarettes and heated tobacco cigarettes users provides the opportunity to identify shared risk factors as well as unique manifestations between users of various smoking-related products. For this, we proposed the following hypotheses:
-
(H1)
Insecure attachment (anxious and avoidant) will be positively associated with nicotine dependence.
-
(H2)
Emotional dysregulation and the metacognitions about smoking will mediate the relationship between insecure attachment (anxious and avoidant) and nicotine dependence.
-
(H3)
Psychological capital will be the moderator of the relationship between insecure attachment, emotional dysregulation, metacognitions about smoking and nicotine dependence.
-
(H4)
The relationships between insecure attachment, emotional dysregulation, metacognitions about smoking, psychological capital, and nicotine dependence will be moderated by the type of tobacco products used by the participants.
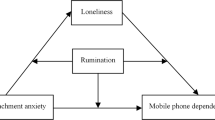
Figure 1 presents the conceptual model tested by this study.

Conceptual model tested in the study
Method
Participants
The participants were gathered by students as a course assignment and consisted of smoking individuals from the general population. Each student had to refer two individuals who use either cigarettes, other alternatives, or a combination of them, and the participants had to complete the questionnaire provided by the researchers. The participants were recruited starting from March to May 2023. This study’s sample consists of 447 participants: 179 men (40%), 267 women, (59.7%) and an individual who didn’t disclose their gender. The mean age for this study’s population is 26.75, with a standard deviation of 9.40 (Min = 18; Max = 64). From the total of participants, 10 (2.2%) had a middle school education level, 200 finished high school (44.7%), 185 (41.4%) had a bachelor’s degree, 46 (10.3%) had a master’s degree, and 6 (1.3%) had a Ph.D. Two hundred eighty-one (62.9%) respondents were born and raised in an urban area, and the rest were born and raised in a rural area. At the time of the study, only 86 (18.3%) respondents lived in a rural area, while the rest had residences in an urban area. The mean for the participants’ years of smoking is 7.85 (SD = 7.6), and from those who declared that they were in a relationship, 129 (28.9%) stated that their partner also smokes. Of the total respondents, 277 (62%) reported that they smoke only classic cigarettes, 39 (8.7%) only e-cigarettes, and 33 (7.4%) only heated tobacco products (HTP), while the rest stated that they use different combinations between the three.
Procedure
To gather the data, the participants completed a web-based survey. The students who gathered the participants received course credits, but the respondents were not rewarded for their involvement. First, the participants could read the scope of the research and then give their informed consent. The participation was voluntary, and the consent for the involvement in the study could have been revoked at any moment without any consequence.
Measures
Sociodemographic data included age, gender, education level, the area they came from and now reside in (rural or urban), relational status and their partners’ smoking habits, years of smoking, and the type of smoking products the respondent uses.
Experiences in close relationships-revised [44] is a 36-item questionnaire that assesses adult attachment. The participants indicated their agreement to each item on a scale ranging from 1-Strongly agree to 7-Strongly disagree. The items are divided into two factors: attachment anxiety (e.g. “My romantic partner makes me doubt myself.”) and attachment avoidance (e.g. “I am nervous when partners get too close to me.”). The internal consistency is 0.91 for attachment anxiety and 0.89 for attachment avoidance. The values of alpha Cronbach are similar to those previously obtained by Marino et al. [30] or Parent et al. [45].
The Compound PsyCap scale [46] is a self-assessing measure of psychological capital. The scale has 12 items (e.g. “I feel confident contributing to discussions about the company’s strategy.”) that are shared among four PsyCap dimensions (hope, optimism, resilience, and self-efficacy), but they also can be used to obtain a total score by computing their answers. The participants can rate each item on a scale ranging from 1 (strongly disagree) to 5 (strongly agree). The internal consistency for this scale is .90, similar to the results found by Turliuc and Candel [32] and Platania and Paolillo [47].
Difficulties in emotion regulation scale [48] is an 18-item self-report measure of emotion regulation difficulties. Each item can be rated on a scale ranging from 1 (almost never) to 5 (almost always), with higher scores reflecting more difficulties in emotion regulation. This scale includes six factors: lack of emotional awareness, lack of emotional clarity, lack of acceptance of one’s emotions when distressed, lack of ability to engage in goal-directed cognition and behavior when distressed, lack of ability to manage one’s impulses when distressed and lack of access to effective strategies for feeling better when distressed. The total score was used for this study. The internal consistency for this scale is 0.91, similar to the one found by Panayiotou et al. [49].
The metacognitions about smoking questionnaire [50] is a self-report measure that aims to evaluate both the positive (cognitive and emotional regulation of smoking) and negative (uncontrollability and cognitive interference) metacognitions about smoking. The 20 items (e.g. “When I get stressed smoking calms me down”, “My smoking is uncontrollable”) of the scale can be scored on a scale ranging from 1 (agree) to 4 (disagree). The internal consistency of the scale is 0.90 for positive metacognitions and 0.89 for negative metacognitions, which is similar or better than the results reported by Nikčević et al. [50] and Poormahdy et al. [51].
Fagerström test for nicotine dependence [52] is a measure developed to assess the addiction to smoking. The 6-item (e.g. “Do you smoke / use e-cigarettes / use heated tobacco products even if you are sick in the bed most of the day?”) instrument aims to investigate the quantity of cigarettes or alternatives consumption, the compulsion to use, and the dependence. The items can be answered by either choosing yes or no or one of the multiple-choice answers, and a higher score will indicate a higher level of dependence. The internal consistency of this scale is 0.67, which is higher than the one reported by Heatherton et al. [52] or by Masiero et al. [11].
Data analyses
As a first step, descriptive statistics and correlations were performed using SPSS 21. In the second step, we computed two separate mediated moderation analyses. Attachment anxiety and attachment avoidance were used, separately, as predictors of nicotine dependence. Emotion dysregulation, positive metacognitions about smoking and negative metacognitions about smoking were used as mediators. Psychological capital was used as a moderator of the direct relationship between the predictors and the outcome, as well as of the relationships between the mediators and the outcome. Model 15 of the PROCESS macro for SPSS [53] was used. As a third and final step, the type of smoking products used by the participants was introduced as a second moderator, for the moderating role of psychological capital. We used model 19 of PROCESS for the analyses.
Results
Preliminary analyses
The descriptive statistics and correlation results are included in Table 1. We found a significant, small and positive correlation between attachment avoidance and nicotine dependence. The link between attachment anxiety and nicotine dependence was not significant. Nicotine dependence correlated significantly with emotion dysregulation and the two types of metacognitions about smoking.
The moderated mediation models
The analyses for the next two models were conducted on the full sample, containing 447 participants. Although attachment anxiety did not correlate significantly with nicotine dependence, we still tested the model containing this predictor, since the possibility of an indirect effect cannot be excluded based on the non-significant correlation. The results show that attachment anxiety is significantly related to emotion dysregulation (b = 0.35, p < .001), positive metacognitions about smoking (b = 0.08, p < .001) and negative metacognitions about smoking (b = 0.05, p = .001). Both positive (b = 0.05, p < .001) and negative metacognitions about smoking (b = 0.14, p = .001) were significantly related to nicotine dependence. However, emotion dysregulation (b = − 0.001, p = .78) and psychological capital (b = − 0.01, p = .19) were not. The direct effect of attachment anxiety was significant and negative only for the individuals with medium psychological capital (b = − 0.01, p = .01). Regardless of the levels of psychological capital, the indirect effects through positive and negative metacognitions about smoking were significant, but those through emotion dysregulation were not.
A second model contained attachment avoidance, which correlated significantly with nicotine dependence. The model shows the positive associations of attachment avoidance with emotion dysregulation (b = 0.22. p < .001), positive (b = 0.03, p = .05), and negative metacognitions about smoking (b = 0.04, p = .01). The direct effect of attachment avoidance on nicotine dependence was not significant at any level of psychological capital. Regardless of the levels of psychological capital, the indirect effect through negative metacognitions about smoking was significant, but the one through emotion dysregulation was not. Psychological capital moderated the indirect effect through positive metacognitions about smoking, which was significant at low (b = 0.002, [0.001; 0.005]) and medium levels of psychological capital (b = 0.001, [0.001; 0.004]), but not at its high levels (b = 0.001, [-0.001; 0.003]).
Adding a second moderator
For the final step of the analysis, we created a new variable using the type of nicotine products the participants used. We took this decision because the number of participants using each type of product, with the exception of classic cigarettes, was low. As such, in the first category – users of classic cigarettes only (CC) – were included 277 participants. In the second category – users of e-cigarettes only or users and e-cigarettes and classic cigarettes (E + CC) – were included 90 participants. In the third category - users of HTP only and users of HTP and classic cigarettes (HTP + CC) – were included 75 participants. Five participants reported using e-cigarettes and HTP and due to their very low number, were excluded from this step. Thus, the analyses for all the following models were conducted on 442 participants.
For the model using attachment anxiety as a predictor, we found that the direct effect on nicotine dependence was significant and negative only for the participants who used classic cigarettes and reported high psychological capital. In terms of indirect effects, emotion dysregulation did not mediate the association between attachment anxiety and nicotine dependence regardless of the product use or level of psychological capital. We found significant and positive indirect effects through positive metacognitions about smoking for the participants in the CC group with low or medium psychological capital, as well as for those in the HTP + CC group with medium psychological capital. We also found significant and positive indirect effects through positive metacognitions about smoking for all the participants in the CC group, for the participants in the E + CC group with low and medium psychological capital, and for the participants from the HTP + CC group with medium psychological capital (see Table 2).
For the model using attachment avoidance as a predictor, the direct effect on nicotine dependence was significant and negative for those in the HTP + CC group with medium or high levels of psychological capital. Again, emotion dysregulation does not mediate the relationship between avoidance and nicotine dependence for any group. The indirect effect through positive metacognitions is significant and positive only for those in the CC group with low and medium levels of psychological capital. The indirect effect through negative metacognitions is significant and positive for the participants in the CC group, for those in the E + CC group with low and medium levels of psychological capital and for those in the HTP + CC group with medium levels of psychological capital (see Table 3).
Discussion
The goal of this study was to investigate the association between insecure attachment, metacognitions, emotional dysregulation, psychological capital and nicotine dependence among the users of various smoking products. Overall, the findings underscore the relative importance of insecure attachment dimensions in predicting nicotine dependence, the mediating role of metacognitions between attachment and nicotine dependence, and the moderating role of psychological capital and the type of smoking product.
In contrast to other studies [11,12,13], the relationship between insecure attachment and nicotine dependence was less clear and less stable among the various types of users of products containing nicotine. When testing the direct correlations, we found a non-significant relationship between anxious attachment and nicotine dependence and a positive, but weak link between avoidant attachment and nicotine dependence. Although unexpected, the results suggest that the hyperactivation strategies used by anxiously attached individuals may not be related to nicotine consumption. On the contrary, avoidant individuals use deactivation, a strategy also called compulsive self-dependence, that aims to reduce pain and frustration. However, it can lead over time to the accumulation of tension that explains the stronger association with attachment substitutes (such as smoking), as a way of calming down. Thus, avoidant individuals resort more easily to substitutes for attachment and to maladaptive coping strategies, including ones that can lead to addiction. In the more complex models, we found that the direct relationship between the insecure attachment and nicotine dependence was, unexpectedly, negative for some participants, depending on their levels of psychological capital and the types of nicotine products they used. Thus, the first hypothesis, proposing a positive link between insecure attachment and nicotine dependence was rejected.
Similar to past studies, both positive and negative metacognitions about smoking significantly mediated the relationships between insecure attachment and nicotine dependence [26, 51, 54], . In addition, the significant indirect effects were positive, thus confirming, at least partially, the second hypothesis. This study confirms that higher levels of insecure attachment can lead to the development of maladaptive cognitions that lead to more negative behaviors [55]. Anxious attachment can guide individuals toward threat monitoring, and can determine them to focus their attention on signals of separation and danger. This can reinforce their positive metacognitions, thus their beliefs that smoking is necessary to regulate their cognitive state [30, 42]. Moreover, when dealing with anxiety inducing situations (such as those created by the belief that the significant others would leave), individuals can use smoking as a way of coping with their anxiety [54]. Anxiously attached individuals can also use negative metacognitions about thought uncontrollability and danger, which leads to a negative mood that is likely to lead to the perseveration of smoking [30, 42]. Finally, it is also worth noting that we found no significant mediation effects for emotional dysregulation, despite its positive and significant correlation with attachment anxiety, avoidance, and nicotine dependence.
The moderating role of psychological capital was supported. Among individuals who use only classic cigarettes and have high levels of psychological capital there was a negative and significant association between anxious attachment and nicotine dependence. Similarly, the link between avoidant attachment and nicotine dependence was negative for those who use HTP and classic cigarettes and report high psychological capital. As for the indirect effects, psychological capital tends to generally attenuate the positive links between insecure attachment and nicotine dependence through positive and negative metacognitions (although not for all the categories of people who smoke). These results show that not all people who experience insecure attachment suffer from similar behavioral and mental health problems. The way individuals deal with their insecure attachment might also depend on their resources and on how they appraise the situations. This study shows that individuals with higher levels of optimism, resilience, self-efficacy, and hope can deal more effectively with the dysfunctional cognitions determined by an insecure attachment style. Moreover, our results confirm previous studies showing that psychological capital and its components are important when dealing with addictions [35, 56,57,58].
Finally, we found different results based on the type of product used by the participants. The unexpected negative links between insecure attachment and nicotine dependence were found only for those who used classic cigarettes, respectively for those who used both HTP and classic cigarettes (and showed elevated levels of psychological capital). Moreover, the protective role of psychological capital seems to be more consistent for those who use alternative products and for dual users who combine alternative smoking products with classic cigarettes. Some previous studies showed that using alternative tobacco products, especially HTP, can lead to a decrease in daily cigarette use and assist in smoking cessation [3, 59]. These users might have more elevated levels of psychological capital that can help them overcome the dangers of their own insecure attachment system and their metacognitions, to regulate better the level of consumption, and take steps in the direction of smoking cessation. For this type of user, the simple fact that they reduce the use of classic cigarettes might reinforce the protective role of psychological capital. Also, earlier research showed that the users of HTP tend to be younger and more educated than the users of classic cigarettes [60]. There is a possibility that the components of psychological capital be more effective for this demographic. However, since the reasons for using e-cigarettes and especially HTP are not sufficiently explored, as well as because the pattern of tobacco use varies greatly based on the motives behind using different products [61, 62], these interpretations must be regarded with caution.
The present study has several important implications. The findings indicate that metacognitions about smoking mediate the relationships between insecure attachment and nicotine dependence. Cognitive-behaviour interventions may be used to modify cognitive biases and dysfunctional beliefs. Also, interventions based on metacognitive therapy [63], which rely on techniques such as detached mindfulness, may prove effective in reducing nicotine dependence, thus leading to smoking cessation [64]. Moreover, our findings indicate that psychological capital is a positive personal resource and an important protective factor against nicotine dependence. It prevents individuals from being affected by distal factors, such as their insecure attachment, and more proximal ones, such as their negative and positive metacognitions about smoking. There is strong support for the usefulness of the interventions targeting psychological capital and its components [65, 66].
Our results can also inform us regarding some prevention measures against smoking. Since we find a significant link between insecure attachment and nicotine dependence, various programs for improving one’s attachment style would be necessary, especially during adolescence. Emotion-focused therapy, which was shown to be efficient when working with adolescents [67,68,69] can be used to help them deal with their attachment insecurities and subsequently reduce the risks of smoking. Fostering psychological capital can also act as a prevention method. Better psychological capital is also related to well-being [32] and previous studies showed that adolescents who smoke report lower levels of well-being compared to those who do not [12]. Thus, improving PsyCap can also improve well-being and by doing so, eliminate some motives behind smoking.
Some limitations must also be noted. First, the study is cross-sectional and cannot infer causality. Moreover, the motives for using alternative smoking products can change over time [70]. As such, longitudinal studies that take into account the potential changes in the smoking behaviors of the participants are needed. Second, due to the low number of participants who used only e-cigarettes or only HTP, we could not create separate categories for them. Putting these participants in the same categories as those who also use classic cigarettes allowed us to achieve sufficient numbers for the analyses, but also led to a decrease in the accuracy of the results. Third, our sample was relatively young and had a high level of education, thus becoming less representative of the entire category of people who smoke. Finally, the sample used in the present study is a convenience one, as such the results cannot be generalized for the entire population.
Conclusion
This study was the first to explore the role of insecure attachment in nicotine dependence in a more diverse sample, as well as its possible mediators and moderators. The results show that insecure attachment is indirectly associated with nicotine dependence mostly through an increase in positive and negative metacognitions about smoking. Higher levels of psychological capital can attenuate these relationships. However, the type of tobacco products used by the participants also played a role, with psychological capital playing a more important role, especially for those who used e-cigarettes and heated tobacco products alongside classic cigarettes. Based on our results, we recommend that the intervention for smoking reduction or cessation target the elimination of dysfunctional beliefs related to the metacognitions about smoking and the improvement of psychological capital.
Data availability
The datasets analyzed in the current study are not publicly available but are available from the corresponding author on request.
Abbreviations
- CC:
-
Classic cigarettes
- MS:
-
Meta-cognitions about smoking
- PsyCap:
-
Psychological capital
- HTP:
-
Heated tobacco products
References
Wise MH, Weierbach F, Cao Y, Phillips K. Tobacco use and attachment style in Appalachia. Issues Ment Health Nurs. 2017;38(7):562–9. https://doi.org/10.1080/01612840.2017.1312651.
Ratajczak A, Jankowski P, Strus P, Feleszko W. Heat not burn tobacco product—A new global trend: impact of heat-not-burn tobacco products on public health, a systematic review. Int J Environ Res Public Health. 2020;17(2):409. https://doi.org/10.3390/ijerph17020409.
Zakiyah N, Purwadi FV, Insani WN, Abdulah R, Puspitasari IM, Barliana MI, et al. Effectiveness and safety profile of alternative tobacco and nicotine products for smoking reduction and cessation: a systematic review. J Multidiscip Healthc. 2021;14:1955–75. https://doi.org/10.2147/jmdh.s319727.
Mahajan SD, Homish GG, Quisenberry A. Multifactorial etiology of adolescent nicotine addiction: a review of the neurobiology of nicotine addiction and its implications for smoking cessation pharmacotherapy. Front Public Health. 2021;9. https://doi.org/10.3389/fpubh.2021.664748.
Lovato C, Watts A, Stead LF. Impact of tobacco advertising and promotion on increasing adolescent smoking behaviours. Cochrane Libr. 2011. https://doi.org/10.1002/14651858.cd003439.pub2.
Lakon CM, Wang C, Butts CT, Jose R, Timberlake DS, Hipp JR. A dynamic model of adolescent friendship networks, parental influences, and smoking. J Youth Adolesc. 2015;44(9):1767–86. https://doi.org/10.1007/s10964-014-0187-7.
Bricker J, Peterson A, Robyn Andersen M, Leroux B, Bharat Rajan K, Sarason I. Close friends’, parents’, and older siblings’ smoking: reevaluating their influence on children’s smoking. Nicotine Tob Res. 2006;8(2):217–26. https://doi.org/10.1080/14622200600576339.
Spada MM, Mohiyeddini C, Wells A. Measuring metacognitions associated with emotional distress: factor structure and predictive validity of the metacognitions questionnaire 30. Pers Individ Dif. 2008;45(3):238–42. https://doi.org/10.1016/j.paid.2008.04.005.
Estevez A, Jauregui P, Lopez-Gonzalez H. Attachment and behavioral addictions in adolescents: the mediating and moderating role of coping strategies. Scand J Psychol. 2019;60(4):348–60. https://doi.org/10.1111/sjop.12547.
Fairbairn CE, Briley DA, Kang D, Fraley RC, Hankin BL, Ariss T. A meta-analysis of longitudinal associations between substance use and interpersonal attachment security. Psychol Bull. 2018;144(5):532–55. https://doi.org/10.1037/bul0000141.
Masiero M, Cutica I, Mazzocco K, Zunino A, Cropley M, Pravettoni G. A comprehensive model of tobacco cigarette smoking in adolescence: the role of attachment style and personality. J Psychol. 2021;155(7):589–605. https://doi.org/10.1080/00223980.2021.1934374.
Habibi M, Hosseini F, Darharaj M, Moghadamzadeh A, Radfar F, Ghaffari Y. Attachment style, perceived loneliness, and psychological well-being in smoking and non-smoking university students. J Psychol. 2018;152(4):226–36. https://doi.org/10.1080/00223980.2018.1446894.
Nakhoul L, Obeid S, Sacre H, Haddad C, Soufia M, Hallit R, et al. Attachment style and addictions (alcohol, cigarette, waterpipe and internet) among Lebanese adolescents: a national study. BMC Psychol. 2020;8(1). https://doi.org/10.1186/s40359-020-00404-6.
Remondi C, Compare A, Tasca GA, Lo Coco G, Chiozza V, Favini A, et al. The effects of attachment, temperament, and self-esteem on technology addiction: a mediation model among young adults. Cyberpsychol Behav Soc Netw. 2022;25(4):258–63. https://doi.org/10.1089/cyber.2021.0237.
Hamonniere T, Varescon I. Metacognitive beliefs in addictive behaviours: a systematic review. Addict Behav. 2018;85:51–63. https://doi.org/10.1016/j.addbeh.2018.05.018.
Spada MM, Nikčević AV, Moneta GB, Wells A. Metacognition as a mediator of the relationship between emotion and smoking dependence. Addict Behav. 2007;32(10):2120–9. https://doi.org/10.1016/j.addbeh.2007.01.012.
Liese BS, Kim HS, Hodgins DC. Insecure attachment and addiction: testing the mediating role of emotion dysregulation in four potentially addictive behaviors. Addict Behav. 2020;107(106432):106432. https://doi.org/10.1016/j.addbeh.2020.106432.
Spada MM, Caselli G, Nikčević AV, Wells A. Metacognition in addictive behaviors. Addict Behav. 2015;44:9–15. https://doi.org/10.1016/j.addbeh.2014.08.002.
Liu L, Xu X, Wu H, Yang Y, Wang L. Associations of psychological capital, demographic and occupational factors with cigarette smoking among Chinese underground coal miners. BMC Public Health. 2015;15(1). https://doi.org/10.1186/s12889-015-1349-6.
Shaver PR, Mikulincer M. Adult attachment strategies and the regulation of emotion. In: Gross JJ, Thomson RA, editors. Handbook of emotion regulation. New Tork: The Guilford Press; 2007. pp. 446–65.
Shaver PR, Mikulincer M, Sahdra B, Gross J. Attachment security as a foundation for kindness toward self and others. In: Brown KW, Leary MR, editors. The Oxford handbook of hypo-egoic phenomena. Oxford: Oxford University Press; 2016. pp. 223–42.
Fairbairn CE, Sayette MA. A social-attributional analysis of alcohol response. Psychol Bull. 2014;140(5):1361–82. https://doi.org/10.1037/a0037563.
Burkett JP, Young LJ. The behavioral, anatomical and pharmacological parallels between social attachment, love and addiction. Psychopharmacology. 2012;224(1):1–26. https://doi.org/10.1007/s00213-012-2794-x.
Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assess. 2004;26(1):41–54. https://doi.org/10.1023/b:joba.0000007455.08539.94.
D’Agostino A, Covanti S, Rossi Monti M, Starcevic V. Reconsidering emotion dysregulation. Psychiatr Q. 2017;88(4):807–25. https://doi.org/10.1007/s11126-017-9499-6.
Alma L, Spada MM, Fernie BA, Yilmaz-Samanci AE, Caselli G, Nikčević AV. Metacognitions in smoking: evidence from a cross-cultural validation of the metacognitions about smoking questionnaire in a Turkish sample. Psychiatry Res. 2018;259:160–8. https://doi.org/10.1016/j.psychres.2017.10.015.
Nikčević AV, Spada MM. Metacognitions across the continuum of smoking dependence. Behav Cogn Psychother. 2008;36(03). https://doi.org/10.1017/s1352465808004293.
Caselli G, Gemelli A, Spada MM. The experimental manipulation of desire thinking in alcohol use disorder. Clin Psychol Psychother. 2017;24(2):569–73. https://doi.org/10.1002/cpp.2038.
Esbjørn BH, Bender PK, Reinholdt-Dunne ML, Munck LA, Ollendick TH. The development of anxiety disorders: considering the contributions of attachment and emotion regulation. Clin Child Fam Psychol Rev. 2012;15(2):129–43. https://doi.org/10.1007/s10567-011-0105-4.
Marino C, Marci T, Ferrante L, Altoè G, Vieno A, Simonelli A, et al. Attachment and problematic Facebook use in adolescents: the mediating role of metacognitions. J Behav Addict. 2019;8(1):63–78. https://doi.org/10.1556/2006.8.2019.07.
Luthans F, Avolio BJ, Walumbwa FO, Li W. The psychological capital of Chinese workers: exploring the relationship with performance. Manag Organ Rev. 2005;1(02):249–71. https://doi.org/10.1111/j.1740-8784.2005.00011.x.
Turliuc MN, Candel OS. The relationship between psychological capital and mental health during the Covid-19 pandemic: a longitudinal mediation model. J Health Psychol. 2022;27(8):1913–25. https://doi.org/10.1177/135910532110127.
Avey JB, Reichard RJ, Luthans F, Mhatre KH. Meta-analysis of the impact of positive psychological capital on employee attitudes, behaviors, and performance. Hum Resour Dev Q. 2011;22(2):127–52. https://doi.org/10.1002/hrdq.20070.
Tugade MM, Fredrickson BL. Resilient individuals use positive emotions to bounce back from negative emotional experiences. J Pers Soc Psychol. 2004;86(2):320–33. https://doi.org/10.1037/0022-3514.86.2.320.
Wang W, Mehmood A, Li P, Yang Z, Niu J, Chu H, et al. Perceived stress and smartphone addiction in medical college students: the mediating role of negative emotions and the moderating role of psychological capital. Front Psychol. 2021;12. https://doi.org/10.3389/fpsyg.2021.660234.
Zeng X, Wei B. The relationship between the psychological capital of male individuals with drug abuse and relapse tendency: a moderated mediation model. Curr Psychol. 2023;42(12):10334–43. https://doi.org/10.1007/s12144-021-02325-y.
Zeng X, Lu M, Chen M. The relationship between family intimacy and relapse tendency among people who use drugs: a moderated mediation model. Subst Abuse Treat Prev Policy. 2021;16(1). https://doi.org/10.1186/s13011-021-00386-7.
Akiyama Y, Sherwood N. Systematic review of biomarker findings from clinical studies of electronic cigarettes and heated tobacco products. Toxicol Rep. 2021;8:282–94. https://doi.org/10.1016/j.toxrep.2021.01.014.
O’Brien D, Long J, Quigley J, Lee C, McCarthy A, Kavanagh P. Association between electronic cigarette use and tobacco cigarette smoking initiation in adolescents: a systematic review and meta-analysis. BMC Public Health. 2021;21(1). https://doi.org/10.1186/s12889-021-10935-1.
Sreeramareddy CT, Shroff SM, Gunjal S. Nicotine dependence and associated factors among persons who use electronic e-cigarettes in Malaysia - an online survey. Subst Abuse Treat Prev Policy. 2023;18(1). https://doi.org/10.1186/s13011-023-00558-7.
Keefer LA, Landau MJ, Rothschild ZK, Sullivan D. Attachment to objects as compensation for close others’ perceived unreliability. J Exp Soc Psychol. 2012;48(4):912–7. https://doi.org/10.1016/j.jesp.2012.02.007.
Nikčević AV, Spada MM. Metacognitions about smoking: a preliminary investigation. Clin Psychol Psychother. 2010;17(6):536–42. https://doi.org/10.1002/cpp.689.
Zvolensky MJ, Bakhshaie J, Shepherd JM, Peraza N, Garey L, Viana AG, et al. Anxiety sensitivity and smoking among spanish-speaking Latinx smokers. Addict Behav. 2019;90:55–61. https://doi.org/10.1016/j.addbeh.2018.10.022.
Fraley RC, Waller NG, Brennan KA. An item response theory analysis of self-report measures of adult attachment. J Pers Soc Psychol. 2000;78(2):350–65. https://doi.org/10.1037/0022-3514.78.2.350.
Parent N, Bond TA, Shapka JD. Smartphones as attachment targets: an attachment theory framework for understanding problematic smartphone use. Curr Psychol. 2023;42(9):7567–78. https://doi.org/10.1007/s12144-021-02092-w.
Lorenz T, Beer C, Pütz J, Heinitz K. Measuring psychological capital: construction and validation of the compound PsyCap scale (CPC-12). PLoS ONE. 2016;11(4):e0152892. https://doi.org/10.1371/journal.pone.0152892.
Platania S, Paolillo A. Validation and measurement invariance of the compound PsyCap scale (CPC-12): a short universal measure of psychological capital. Psicol. 2022;38(1):63–75. https://doi.org/10.6018/analesps.449651.
Victor SE, Klonsky ED. Validation of a brief version of the difficulties in emotion regulation scale (DERS-18) in five samples. J Psychopathol Behav Assess. 2016;38(4):582–9. https://doi.org/10.1007/s10862-016-9547-9.
Panayiotou G, Artemi T-F, Theodorou M, Theodorou C, Neophytou K. Not just for fun: Gambling, substance use, and the transdiagnostic role of emotion regulation. Cogent Psychol. 2023;10(1). https://doi.org/10.1080/23311908.2023.2183677.
Nikčević AV, Caselli G, Wells A, Spada MM. The metacognitions about Smoking Questionnaire: Development and psychometric properties. Addict Behav. 2015;44:102–7. https://doi.org/10.1016/j.addbeh.2014.11.004.
Poormahdy H, Najafi M, Khosravani V. The effects of emotion dysregulation and negative affect on urge to smoke and nicotine dependence: the different roles of metacognitions about smoking. Addict Behav. 2022;124(107108):107108. https://doi.org/10.1016/j.addbeh.2021.107108.
Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom K-O. The Fagerstrom test for nicotine dependence: a revision of the Fagerstrom tolerance questionnaire. Addiction. 1991;86(9):1119–27. https://doi.org/10.1111/j.1360-0443.1991.tb01879.x.
Hayes AF. Introduction to Mediation, Moderation, and conditional process analysis: a regression-based Approach. Guilford Press; 2013.
Izadpanah M, Najafi M, Khosravani V. Anxiety in social interactions and nicotine dependence in nicotine-dependent men: the role of metacognitions about smoking. Addict Behav. 2021;112(106656):106656. https://doi.org/10.1016/j.addbeh.2020.106656.
Myers SG, Wells A. Early trauma, negative affect, and anxious attachment: the role of metacognition. Anxiety Stress Coping. 2015;28(6):634–49. https://doi.org/10.1080/10615806.2015.1009832.
Bradshaw SD, Shumway ST, Wang EW, Harris KS. Addiction and the mediation of hope on craving, readiness, and coping. J Groups Addict Recover. 2014;9(4):294–312. https://doi.org/10.1080/1556035x.2014.969062.
Kelloniemi H, Ek E, Laitinen J. Optimism, dietary habits, body mass index and smoking among young Finnish adults. Appetite. 2005;45(2):169–76. https://doi.org/10.1016/j.appet.2005.05.001.
Hyde J, Hankins M, Deale A, Marteau TM. Interventions to increase self-efficacy in the context of addiction behaviours: a systematic literature review. J Health Psychol. 2008;13(5):607–23. https://doi.org/10.1177/1359105308090933.
Sweet L, Brasky TM, Cooper S, Doogan N, Hinton A, Klein EG, et al. Quitting behaviors among dual cigarette and E-cigarette users and cigarette smokers enrolled in the tobacco user adult cohort. Nicotine Tob Res. 2019;21(3):278–84. https://doi.org/10.1093/ntr/nty222.
Brose LS, McDermott MS, McNeill A. Heated tobacco products and nicotine pouches: A survey of people with experience of smoking and/or vaping in the UK. Int J Environ Res Public Health. 2021;18(16):8852. https://www.mdpi.com/1660-4601/18/16/8852
Kuwabara Y, Kinjo A, Fujii M, Imamoto A, Osaki Y, Jike M, et al. Heat-not-burn tobacco, electronic cigarettes, and combustible cigarette use among Japanese adolescents: a nationwide population survey 2017. BMC Public Health. 2020;20(1). https://doi.org/10.1186/s12889-020-08916-x.
Temourian AA, Song AV, Halliday DM, Gonzalez M, Epperson AE. Why do smokers use e-cigarettes? A study on reasons among dual users. Prev Med Rep. 2022;29(101924):101924. https://doi.org/10.1016/j.pmedr.2022.101924.
Wells A. Metacognitive therapy for anxiety and depression. New York, NY: Guilford; 2011.
Caselli G, Gemelli A, Spada MM, Wells A. Experimental modification of perspective on thoughts and metacognitive beliefs in alcohol use disorder. Psychiatry Res. 2016;244:57–61. https://doi.org/10.1016/j.psychres.2016.07.029.
Dello Russo S, Stoykova P. Psychological capital intervention (PCI): a replication and extension. Hum Resour Dev Q. 2015;26(3):329–47. https://doi.org/10.1002/hrdq.21212.
Lupșa D, Vîrga D, Maricuțoiu LP, Rusu A. Increasing psychological capital: a pre-registered meta‐analysis of controlled interventions. Appl Psychol. 2020;69(4):1506–56. https://doi.org/10.1111/apps.12219.
Robinson AL, Dolhanty J, Greenberg L. Emotion-focused family therapy for eating disorders in children and adolescents. Clin Psychol Psychother. 2015;22(1):75–82. https://doi.org/10.1002/cpp.1861.
Adams CR, Gibbons MM. Counseling adolescents diagnosed with conduct disorder: application of emotion-focused therapy for individuals. J Ment Health Couns. 2019;41(4):283–96. https://meridian.allenpress.com/jmhc/article-abstract/41/4/283/435135/Counseling-Adolescents-Diagnosed-With-Conduct.
Bonnaire C, Liddle H, Har A, Phan O. Searching for change mechanisms in emotion-focused work with adolescents and parents: an example from multidimensional family therapy. Couple Family Psychol. 2020;9(2):100–21. https://psycnet.apa.org/fulltext/2020-30017-001.pdf.
Correa JB, Tully LK, Doran N. Expectancies and reasons for use of e-cigarettes among young adults: a longitudinal analysis. Psychol Addict Behav. 2019;33(8):730–6. https://doi.org/10.1037/adb0000514.
Acknowledgements
Not applicable.
Funding
This study did not obtain any funding.
Author information
Authors and Affiliations
Contributions
Conceptualization, MNT & OSC; methodology, MNT & OSC; formal analysis: OSC; writing—original draft preparation, MNT, OSC & MJ; writing—review and editing, MNT, OSC & MJ. All authors have read and agreed to the current version of the manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations. Informed consent was obtained from all individual participants included in the study. The study protocol was approved by the Ethical Committee of the Faculty of Psychology and Educational Sciences, Alexandru Ioan Cuza University.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Turliuc, M.N., Candel, OS. & Jitaru, M. The relationship between insecure attachment and nicotine dependence among users of classic cigarettes, e-cigarettes, and heated tobacco products: a moderated mediation model. Subst Abuse Treat Prev Policy 19, 43 (2024). https://doi.org/10.1186/s13011-024-00623-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13011-024-00623-9