
Abstract
Purpose
Analyzing the correlation between patients’ basic information, three-dimensional parameters after calcaneal fractures, and the prognosis of calcaneal fractures.
Methods
A retrospective analysis was conducted on 43 patients with calcaneal fractures who underwent surgical treatment in the Foot and Ankle Surgery, Xi’an Honghui Hospital, from September 2019 to August 2022. Patient demographics including gender and age were collected, as well as the preoperative posterior articular surface collapse area, number of fracture fragments, length, width, height, and volume of the calcaneus obtained from preoperative three-dimensional imaging. Patients were followed up for VAS, AOFAS, and SF-36 scores. Correlation analysis was performed on the obtained data.
Results
All 43 included patients received complete follow-up, including 40 males and 3 females, with an average follow-up time of 35.37 ± 10.73 months, and an average age of 43.98 ± 12.08 years. All patients’ VAS, AOFAS, and SF-36 scores at the last follow-up showed no correlation with patient age, gender, or the area of posterior articular collapse, number of fracture fragments, length, width, height, or volume of the calcaneus.
Conclusions
The prognosis of calcaneal fractures is unrelated to three-dimensional factors such as patient age, gender, length, width, height, volume of the calcaneus, area of the posterior joint, and number of fracture fragments.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Calcaneal fractures account for 2% of all fractures and approximately 60% of all tarsal injuries [1, 2]. The most common cause is falling from a height. Calcaneal fractures may have a negative impact on an individual’s walking and daily activities [3, 4], including long-term pain, decreased functional activities, and heel deformities [5], with severe cases potentially leading to disability [6]. Currently, surgical treatment can restore optimal function and reduce the incidence of post-traumatic arthritis [7]. It effectively alleviates pain, improves foot function, and enhances the quality of life for patients [8].
There are still some controversies regarding the surgical treatment of calcaneal fractures, and open reduction and internal fixation are considered the gold standard for restoring calcaneal morphology and achieving anatomical reduction of the articular surface [9,10,11]. Many researchers have conducted in-depth studies on the imaging factors after calcaneal fracture surgery. Research has found that the clinical outcomes of Sanders IV calcaneal fractures are unrelated to the number of fracture fragments but are associated with the severity of injury to the B\(\:\ddot{o}\)hler angle, Gissane angle, and vertical height [12]. It also emphasizes that the B\(\:\ddot{o}\)hler angle is an important factor influencing prognosis [13]. However, measurements of B\(\:\ddot{o}\)hler angle, Gissane angle, and calcaneal height obtained through X-ray imaging are often influenced by the X-ray projection angle and positioning of the ankle joint, leading to less accurate data [14]. Moreover, fresh calcaneal fractures are acute injuries, and the pain and swelling of the foot during the acute phase can also affect the quality of X-ray images [15]. The advent of computed tomography (CT) and three-dimensional reconstruction techniques has improved the quality of anatomical assessment of calcaneal fractures [16]. Consequently, many researchers have begun three-dimensional measurements of the calcaneus [17]. Research has shown that the postoperative CT scan findings of calcaneal posterior facet step-off are correlated with SF-36 (PCS) scores but not with AOFAS scores [18]. Qiang, M conducted measurements of the area and other three-dimensional parameters of the calcaneal posterior facet and analyzed their correlation with gender [19]. However, there are currently no articles specifically analyzing and reporting on the area of the collapsed portion of the calcaneal posterior facet. Meanwhile, researchers have conducted three-dimensional measurements and correlation analyses of the B\(\:\ddot{o}\)hler angle, Gissane angle, length of the calcaneus, height, and length of the posterior facet in calcaneal fractures [20]. However, during the measurement process, some researchers have pointed out that due to the irregular shape of the calcaneus, using two fixed points to measure its width often leads to certain errors [19].
Therefore, this study improves measurement methods to accurately measure the length, width, and height of the calcaneus by applying distance measurements between surfaces. Simultaneously, we use three-dimensional imaging techniques to measure the area of posterior facet collapse, number of fracture fragments, and volume of the calcaneus. We analyze the most relevant indicators for the prognosis of calcaneal fractures, providing a new perspective for selecting and optimizing clinical treatment plans and assisting clinicians in devising the best surgical approach.
Materials and methods
General information
This study obtained approval from the Ethics Review Committee of Xi’an Honghui Hospital. (No: 202401027). It retrospectively analyzed the clinical and radiological data of patients with calcaneal fractures who underwent surgical treatment in the Foot and Ankle Surgery Department of Honghui Hospital, from September 2019 to August 2022. The collection of follow-up data was conducted with the informed consent of the patients.
Inclusion criteria: (1) Fresh calcaneal fractures with closed epiphyseal lines; (2) Calcaneal fractures treated surgically; (3) SandersII and above unilateral closed calcaneal fractures. Exclusion criteria: (1) Multiple fractures of the foot; (2) Patients with rheumatoid arthritis, talonavicular arthritis, hypertension, diabetes, and other internal medical conditions affecting surgical prognosis; (3) Severe neurovascular injuries in the affected lower limb. All surgeries were performed by the same group of experienced orthopedic surgeons.
Surgical treatment options
Under general anesthesia, a lateral “L”-shaped surgical incision was made on the outer side of the calcaneus, starting from the posterior aspect of the lateral malleolus and extending downward over the base of the fifth metatarsal. The skin and subcutaneous tissue were sequentially incised, the calcaneofibular ligament was dissected, and a whole lateral calcaneal flap was raised, exposing the lateral wall of the calcaneus, the distal tibiofibular joint, and the calcaneocuboid joint. Evidence of posterior facet collapse and comminution was observed. Hematoma, impinged soft tissues, and detached loose cartilage at the fracture ends were cleared, followed by irrigation with saline solution. The subtalar joint surface was reduced under direct visualization, showing a smooth articular surface. Intraoperatively, based on the extent of bone defect, the decision was made whether to implant allograft bone. Intraoperatively, C-arm fluoroscopy was used to obtain lateral and axial views of the calcaneus to assess the reduction of the calcaneus. If satisfactory, the calcaneus was fixed using locking plates and screws. The joint cavity was irrigated, and the surgical incision was closed layer by layer. Sterile gauze and bandages were applied with compression to minimize the occurrence of postoperative complications such as joint swelling and infection.

Preoperative and postoperative X-ray imaging data of the patient. a Preoperative X-ray imaging data of the patient shows evident fracture lines and mild varus deformity. b Postoperative X-ray imaging data of the patient shows good fracture reduction, stable internal fixation, and proper alignment of the calcaneal axis

Preoperative and postoperative CT imaging data of the patient. a Preoperative CT imaging data of the patient shows a lack of smoothness of the subtalar joint surface, with small displaced fracture fragments in the calcaneus, significant height compression of the calcaneus, lateral bulging of the calcaneal outer wall, and increased width of the calcaneus. b Postoperative CT imaging data of the patient shows that the calcaneus is well-reduced and aligned with the subtalar joint surface, with a good match and satisfactory recovery of the calcaneal width
Information and data collection
The basic information of the patients (age, gender) was collected, and during the last follow-up, the Visual Analogue Scale (VAS) [21], American Orthopedic Foot and Ankle Society, (AOFAS) score [22], and the SF-36 Quality of Life Questionnaire were used [23]. Correlation analysis was performed between these variables. We imported the obtained CT imaging data (CT model: Siemens SOMATOM Definition Flash second-generation dual-source CT, slice thickness of 1 mm) into mimics 21.0 software (Materialise’s Mimics Medical 21.0 version), 3-Matic(Materialise’s 3-Matic Medical 13.0 version) for three-dimensional reconstruction. Subsequently, we measured the number of fractured fragments on the articular surface of the calcaneus after calcaneal fracture. Considering the variations in the size of each patient’s calcaneus, which consequently affects the area, volume, length, width, and height of the posterior articular surface, we employed a ratio-based method for more precise measurements. Therefore, we measured the area of posterior calcaneal articular surface collapse/total area of posterior calcaneal articular surface, calcaneal volume/talus volume, calcaneal length/talus length, calcaneal width/talus width, calcaneal height/talus height to obtain complete data.
Description of the operation steps in Mimics software
Firstly, import the complete CT imaging data (in DICOM format) of the included patients one by one into the Mimics 21.0 software. Perform “Advanced Segmentation” by selecting the desired calcaneus and talus, adjust the threshold range to an appropriate level, and obtain complete 3D bone images of the calcaneus and talus (as shown in Fig. 3). Then, export the obtained models of the calcaneus and talus to the 3-Matic 13.0 software and utilize functions such as “Mark”, “Design”, and “Measure” for relevant measurements (as shown in Figs. 4, 5, 6, 7 and 8).

Three-dimensional modeling of the calcaneus and talus depicted

Importing the established model into 3-Matic 13.0 software. a View the volume of the calcaneus in the calcaneus properties of 3-Matic 13.0. b View the volume of the talus in the talus properties of 3-Matic 13.0. c Rotate the calcaneus to the appropriate position to observe the number of fracture fragments on the articular surface after calcaneal fracture

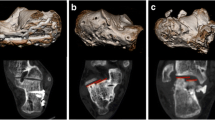
Measurement of the collapsed area and total area of the articular surface. a In 3-Matic 13.0, utilize “Mark” and “Brush Mark” to render the area of the collapsed articular surface after fracture. b Utilize “Mark” and “Brush Mark” to render the total area of the articular surface after fracture

Measurement of the lengths of the calcaneus and talus. a Select three points at the most anterior part of the calcaneal articular surface, use 3-Matic 13.0 to establish a section at the most anterior part of the calcaneal articular surface, then select a point at the most posterior end of the calcaneal tuberosity to establish a plane parallel to the section at the most anterior part of the calcaneal articular surface. bMeasure the distance between the two sections in Figure A as the length of the calcaneus. c The three most convex points were selected in the talus part of the talus articular surface, and the section plane of the talus head was established by using 3-Matic 13.0, and then the point at the end of the posterior process of the talus bone was selected to establish a plane parallel to the section plane of the talus bone. d Measure the distance between the two planes established in Figure C as the length of the talus

Measurement of the width of the calcaneus and talus. a Select three points at the medial aspect of the sustentaculum tali of the calcaneus, use 3-Matic 13.0 to establish a section at the innermost aspect of the sustentaculum tali of the calcaneus, then select a point at the most prominent location of the lateral wall of the calcaneus to establish a plane parallel to the inner section. b Measure the distance between the two planes in Figure A as the width of the calcaneus. c Select three points at the medial tuberosity of the talus, use 3-Matic 13.0 to establish a section at the medial tuberosity of the talus, then use the most lateral point of the lateral tuberosity of the talus to establish a plane parallel to the section at the medial tuberosity of the talus. d Measure the distance between the two planes in Figure C as the width of the talus

Measurement of the height of the calcaneus and talus. a Select two points on the inner and outer sides at the lowest point of the posterior half of the calcaneus, and select one point at the lowest point of the anterior half of the calcaneus. Use 3-Matic 13.0 to establish a section at the lowest end of the calcaneus, and then select the highest point of the calcaneus to establish a plane parallel to the section at the lowest end of the calcaneus. bMeasure the distance between the two planes established in Figure A as the height of the calcaneus. c Two points were selected at the lowest part of the talus and one point at the lowest part of the anterior part of the talus, and one point was selected at the lowest point of the anterior half of the talus, and the section plane at the lowest part of the talus was established by using 3-Matic 13.0, and then the highest point of the talus trochlea was selected by using 3-Matic 13.0 to establish a plane parallel to the section plane at the lowest part of the talus. d Measure the distance between the two planes established in Figure C as the height of the talus
Outcome indicators
Collect basic patient data (age, gender) and radiographic information. Evaluate functional outcomes using VAS, AOFAS, and SF-36 scores at the last follow-up after surgery. Perform correlation analysis to assess the prognostic significance. Visual Analog Scale (VAS) is used to measure pain, with 0 indicating no pain and 100 indicating severe pain. The AOFAS (American Orthopedic Foot and Ankle Society) ankle-hindfoot scoring system has a total score of 100 and includes subjective and objective criteria for evaluating clinical parameters. The score allocation is as follows: pain 40 points, function 50 points, alignment 10 points. The SF-36 Health Survey scores are divided into two major dimensions for statistical analysis: Physical Component Summary (PCS) and Mental Component Summary (MCS).
Statistical methods
SPSS25.0 (IBM, New York, United States) statistical software was used to analyze the data, all data were normally distributed, expressed by mean ± standard deviation (x ± s), and the prognosis was analyzed by t-test, analysis of variance and Pearson correlation coefficient. P < 0.05 was statistically significant.
Results
General condition of the patient
A total of 43 patients were followed up, all of whom completed the follow-up. Among them, there were 40 males and 3 females. The average follow-up time was 35.37 ± 10.73 months, and the average age was 43.97 ± 12.08 years. Outcome measures at the last follow-up for the patients are presented in Table 1. Measurement indicators for the patients are presented in Table 2.
Analysis of various evaluation indicators
This study found that there were no significant correlations (p > 0.05) between the VAS, AOFAS, and SF-36 scores at the final follow-up after calcaneal fractures and the patients’ age, gender, as well as the area of collapse of the posterior joint surface, the number of fracture fragments on the posterior joint surface, and the length, width, height, and volume of the calcaneus. (Refer to Table 3.)
Discussion
The calcaneus, the largest tarsal bone in the human body, plays a crucial role in weight-bearing [24]. An increasing number of researchers have reported on the analysis of the therapeutic efficacy and prognosis correlation of calcaneal fractures. Some researchers have explored the influencing factors of calcaneal fracture prognosis starting from patients’ basic information such as gender and age [17, 25, 26], while others have analyzed the correlation factors of calcaneal fracture prognosis from the perspective of imaging modalities such as X-ray and CT [20, 27, 28]. We conducted our research analysis based on patients’ basic information and three-dimensional data.
There are reports stating that the functional outcomes after calcaneal fractures are unrelated to the patient’s age or gender [25]. In this study, a total of 43 patients were included, and the analysis comparing the prognosis of patients with age and gender also showed no correlation. Patrick and Rammelt, along with others, also pointed out in their articles that increasing patient age does not have a negative impact on the prognosis of calcaneal fractures [17, 29], which remains consistent with our research findings.
This study found that the length, width, height, and volume of the calcaneus were not associated with the VAS, AOFAS, and SF-36 scores at the final follow-up. We believe that since calcaneal fractures are high-energy vertical axial injuries [30], the length of the calcaneus should not significantly change before and after the injury, which is why the length of the calcaneus does not have a significant impact on the prognosis of the fracture. In our study of the width, height, and volume of the calcaneus, we also found no significant correlation with the prognosis of calcaneal fractures. There are very few global reports on research regarding the three-dimensional measurements of the width, height, and volume of the calcaneus. However, some studies have indicated that the recovery of calcaneal morphology can effectively improve the prognosis of calcaneal fractures [31]. During the surgical procedure, we strive to restore the morphology and volume of the calcaneus as much as possible. Additionally, based on the extent of bone defects, we decide intraoperatively whether to implant allogeneic bone to ensure complete restoration of the volume and morphology of the calcaneus. Therefore, we believe that the length, width, height, and volume of the calcaneus may not have a significant impact on the prognosis of the fracture.
Our research results indicate that there is no significant correlation between VAS, AOFAS, and SF-36 scores and the number of fracture fragments on the posterior articular surface of the calcaneus, as well as the area of posterior articular surface collapse. Kim also mentioned in the report that the clinical outcomes of SandersIV calcaneal fractures are not related to the number of fracture fragments [12]. Currently, there is no literature reporting on the impact of the area of posterior articular surface collapse on the prognosis of calcaneal fractures. However, Chaniotakis et al. reported that the quality of reduction and articular congruence after calcaneal fracture surgery directly influence the prognosis of calcaneal fractures [32, 33]. Since all the patients included in our study underwent surgery performed by the same experienced surgeon, efforts were made during the operation to restore the smoothness of the articular surface as much as possible, ensuring congruence with the subtalar joint. Therefore, we have reason to believe that the size of the area of posterior articular surface collapse may not affect the prognosis of calcaneal fractures.
This study has certain limitations: (1) The sample size included in this study is limited, but it fully meets the statistical requirements; (2) During the data measurement process, we still cannot fully accurately reflect the true length, width, and height of the calcaneus. However, compared to previous literature, there has been significant improvement. We no longer use point-to-point measurement methods but instead utilize surface-to-surface measurement methods, which more accurately reflect the length, width, and height of the calcaneus; (3) Due to the many other factors affecting the prognosis of calcaneal fractures, such as smoking, diabetes, anxiety, depression, etc., we will conduct a detailed analysis in our upcoming studies.
Conclusion
The patient’s gender, age, as well as the length, width, height, volume of the calcaneus, and the degree of comminution of the posterior joint do not have an impact on the prognosis of calcaneal fractures.
Data availability
No datasets were generated or analysed during the current study.
References
Molloy AP, Lipscombe SJ. Hindfoot arthrodesis for management of bone loss following calcaneus fractures and nonunions. Foot Ankle Clin. 2011;16(1). https://doi.org/10.1016/j.fcl.2010.12.008. 165 – 79.
Hollawell S. Wound closure technique for lateral extensile approach to intra-articular calcaneal fractures. J Am Podiatr Med Assoc. 2008;98(5):422–5. https://doi.org/10.7547/0980422.
Vicenti G, Carrozzo M, Solarino G, Caizzi G, De Crescenzo A, Portaluri M, Mori CM, Vittore D, Moretti B. Comparison of plate, calcanealplasty and external fixation in the management of calcaneal fractures. Injury, 2019. 50 Suppl 4: pp. S39-S46. https://doi.org/10.1016/j.injury.2019.04.014
Vosoughi AR, Borazjani R, Ghasemi N, Fathi S, Mashhadiagha A, Hoveidaei AH. Different types and epidemiological patterns of calcaneal fractures based on reviewing CT images of 957 fractures. Foot Ankle Surg. 2022;28(1):88–92. https://doi.org/10.1016/j.fas.2021.02.002.
Clare MP, Crawford WS. Managing complications of Calcaneus fractures. Foot Ankle Clin. 2017;22(1):105–16. https://doi.org/10.1016/j.fcl.2016.09.007.
Stephens AR, Grujic L, Post-Traumatic Hindfoot AJ, Orthop Trauma. 2020. 34 Suppl 1: pp. S32-S37. https://doi.org/10.1097/BOT.0000000000001695
Agren PH, Wretenberg P, Sayed-Noor AS. Operative versus nonoperative treatment of displaced intra-articular calcaneal fractures: a prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am. 2013;95(15):1351–7. https://doi.org/10.2106/JBJS.L.00759.
Lewis SR, Pritchard MW, Solomon JL, Griffin XL, Bruce J. Surgical versus non-surgical interventions for displaced intra-articular calcaneal fractures. Cochrane Database Syst Rev. 2023;11(11):CD008628. https://doi.org/10.1002/14651858.CD008628.pub3.
Epstein N, Chandran S, Chou L. Current concepts review: intra-articular fractures of the calcaneus. Foot Ankle Int. 2012;33(1):79–86. https://doi.org/10.3113/FAI.2012.0079.
Paley D, Hall H. Intra-articular fractures of the calcaneus. A critical analysis of results and prognostic factors. J Bone Joint Surg Am. 1993;75(3):342–54. https://doi.org/10.2106/00004623-199303000-00005.
Sanders R, Vaupel ZM, Erdogan M, Downes K. Operative treatment of displaced intraarticular calcaneal fractures: long-term (10–20 years) results in 108 fractures using a prognostic CT classification. J Orthop Trauma. 2014;28(10):551–63. https://doi.org/10.1097/BOT.0000000000000169.
Kim DH, Kim JY, Lee KB. Is subclassification by number of fracture fragments necessary for Sanders Type IV calcaneal fractures? J Am Podiatr Med Assoc. 2023;113(6). https://doi.org/10.7547/21-135.
Basile A. Subjective results after surgical treatment for displaced intra-articular calcaneal fractures. J Foot Ankle Surg. 2012;51(2):182–6. https://doi.org/10.1053/j.jfas.2011.10.042.
Wuest TK. Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg. 1997;5(3):172–81. https://doi.org/10.5435/00124635-199705000-00006.
Sanders R. Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am. 2000;82(2):225–50. https://doi.org/10.2106/00004623-200002000-00009.
Roll C, Schirmbeck J, Müller F, Neumann C, Kinner B. Value of 3D reconstructions of CT scans for Calcaneal Fracture Assessment. Foot Ankle Int. 2016;37(11):1211–7. https://doi.org/10.1177/1071100716660824.
Rammelt S, Zwipp H, Schneiders W, Dürr C. Severity of injury predicts subsequent function in surgically treated displaced intraarticular calcaneal fractures. Clin Orthop Relat Res. 2013;471(9):2885–98. https://doi.org/10.1007/s11999-013-3062-z.
van Hoeve S, de Vos J, Verbruggen JP, Willems P, Meijer K, Poeze M. Gait Analysis and Functional Outcome after Calcaneal fracture. J Bone Joint Surg Am. 2015;97(22):1879–88. https://doi.org/10.2106/JBJS.N.01279.
Qiang M, Chen Y, Zhang K, Li H, Dai H. Measurement of three-dimensional morphological characteristics of the calcaneus using CT image post-processing. J Foot Ankle Res. 2014;7(1):19. https://doi.org/10.1186/1757-1146-7-19.
Qiang M, Chen Y, Jia X, Zhang K, Li H, Jiang Y, Zhang Y. Post-operative radiological predictors of satisfying outcomes occurring after intra-articular calcaneal fractures: a three dimensional CT quantitative evaluation. Int Orthop. 2017;41(9):1945–51. https://doi.org/10.1007/s00264-017-3577-0.
Bodian CA, Freedman G, Hossain S, Eisenkraft JB, Beilin Y. The visual analog scale for pain: clinical significance in postoperative patients. Anesthesiology. 2001;95(6):1356–61. https://doi.org/10.1097/00000542-200112000-00013.
Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994;15(7):349–53. https://doi.org/10.1177/107110079401500701.
Li L, Wang HM, Shen Y, Chinese. SF-36 Health Survey: translation, cultural adaptation, validation, and normalisation. J Epidemiol Community Health. 2003;57(4). https://doi.org/10.1136/jech.57.4.259. 259 – 63.
Hall RL, Shereff MJ, Shereff. Anatomy of the calcaneus. Clin Orthop Relat Res. 1993;29027–35. https://doi.org/10.1097/00003086-199305000-00004.
Simske NM, Hermelin MJ, Vallier HA. Impact of psychosocial and economic factors on functional outcomes after Operative Calcaneus fractures. J Orthop Trauma. 2021;35(11):e423–8. https://doi.org/10.1097/BOT.0000000000002082.
Mitchell MJ, McKinley JC, Robinson CM. The epidemiology of calcaneal fractures. Foot (Edinb). 2009;19(4):197–200. https://doi.org/10.1016/j.foot.2009.05.001.
Su Y, Chen W, Zhang T, Wu X, Wu Z, Zhang Y. Bohler’s angle’s role in assessing the injury severity and functional outcome of internal fixation for displaced intra-articular calcaneal fractures: a retrospective study. BMC Surg. 2013;13:40. https://doi.org/10.1186/1471-2482-13-40.
Maskill JD, Bohay DR, Anderson JG. Calcaneus fractures: a review article. Foot Ankle Clin. 2005;10(3). https://doi.org/10.1016/j.fcl.2005.03.002. 463 – 89, vi.
Pflüger P, Zyskowski M, Greve F, Kirchhoff C, Biberthaler P, Crönlein M. Patient-reported outcome following operative and Conservative Treatment of Calcaneal Fractures: a retrospective analysis of 79 patients at short- to midterm Follow-Up. Front Surg. 2021;8:620964. https://doi.org/10.3389/fsurg.2021.620964.
Bhattacharyya A, Raman R. Mal-United fracture of calcaneum treated with lateral decompression. Mymensingh Med J. 2013;22(1):148–56. https://pubmed.ncbi.nlm.nih.gov/23416823.
Rammelt S, Amlang M, Barthel S, Gavlik JM, Zwipp H. Percutaneous treatment of less severe intraarticular calcaneal fractures. Clin Orthop Relat Res. 2010;468(4). https://doi.org/10.1007/s11999-009-0964-x. 983 – 90.
Badalahu QB, Luo J, Zeng Y, Fu S, Zhang L. Classification of the subtalar articular surface and its matching situation: an anatomical study on Chinese subtalar joint. Surg Radiol Anat. 2020;42(10):1133–9. https://doi.org/10.1007/s00276-020-02444-4.
Chaniotakis C, Genetzakis V, Samartzidis K, Siligardou MR, Stavrakakis I. Percutaneous fixation of displaced intraarticular fractures of the calcaneus. A retrospective case series study and a review of the literature. Injury. 2023;54(10):110966. https://doi.org/10.1016/j.injury.2023.110966.
Funding
This study was supported by the General Project (Social Development Field) of the Science and Technology Department of Shaanxi Province (Grant No. 2023-YBSF-488), Xi’an Health Bureau Scientifc Research Project (Grant No. 2023ms15).
Author information
Authors and Affiliations
Contributions
JunKui Xu designed the study idea for this clinical trial. ShiHang Cao and Peng Li to collect relevant data. Jun Lu and Yi Li to organise and manage data. Meng Lu and ShiHang Cao to analyse data and measure relevant data. Meng Lu wrote the paper. JunKui Xu to review and revise the first draft of the paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of interest
We declare that we have no conflicts of interest.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lu, M., Cao, S., Lu, J. et al. Three dimensional analysis of factors affecting the prognosis of calcaneal fractures. J Orthop Surg Res 19, 473 (2024). https://doi.org/10.1186/s13018-024-04975-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-024-04975-7